Embed Size (px)
Citation preview

Darren Urada, Ph.D and Howard Padwa, Ph.D.UCLA Integrated Substance Abuse Programs
CADPAAC / ADP Quarterly Meeting
September 26, 2012
Integration of SUD services with Primary Care

AcknowledgementsUCLA team, past & present: Valerie Antonini, MPH, Aaron Call, Sarah Cousins, MPH, Desiree Crevecoeur-MacPhail, Ph.D., Jia Fan, M.S., Thomas Freese, Ph.D., Rachel Gonzales, Ph.D., Grant Hovik, Adi Jaffe, Ph.D., Adam King, Sherry Larkins, Ph.D., Stella Lee, Allison
Ober, Ph.D., Brandy Oeser, MPH, Alex Olson, Brandy Oeser, MPH, Howard Padwa, Ph.D., Diego Ramirez, Beth Rutkowski, MPH,
Elizabeth Schaper, Suzanne Spear, Ph.D., Cheryl Teruya, Ph.D., Elise Tran, Umme Warda, M.S., Richard Rawson, Ph.D.
Research funded by:California Department of Alcohol and Drug Programs
California Program on Access to CareKern County
The authors’ views and recommendations do not necessarily represent those of the funders, UCLA, or the UCLA Integrated Substance Abuse Programs.

Topics to be covered
• Integration and Health• Integration and costs• Tools & Data: SUD Services, Integration
– FQHC administrative data– Dual Diagnosis in Health Care Settings Instrument– Surveys
• Views from the “other side”: Policies Primary Care Providers want changed to facilitate SUD integration.

Health

Impact of SUD on Health• Substance use contributes to over 70
conditions that require medical care (NCASA 2012)
– Increases risk for chronic disease (cardiovascular, pulmonary, liver) (Stein 1999)
– Increases risk for mental health disorders (CSAT 2007)
– Increases risk for communicable disease (HIV, hepatitis) (Clark 2010)
– Increases risk for serious injury (Vinson 2003)5

Costs
6

Impact of SUD on Healthcare Costs• People with SUD incur
over double the total medical costs of people without SUD (Parthasarathy 2001; Thomas 2005)
• Major cost drivers: ER & inpatient services– Chronic drug use increases
ER utilization by 30% (McGeary & French, 2000)
– SUD pts use ER 3x as often as people without SUD (Parthasarathy 2001)
– Treatment even reduces costs among family members (Weisner et al., 2010)
7

Who Pays for SUD-Related Costs? Medicaid
• 9% of general population has SUD; 13% of disabled Medicaid population has SUD (SAMHSA 2010; Boyd 2010)– Medicaid covers 1/5 of substance-related
hospital stays (Fox 1995)– Medicaid covers over 20% of SUD-related ER
visits (Owens 2010)– Medicaid covers over half of hospital admissions
involving co-occurring SUD and medical conditions (Santora & Hutton, 2008)
• SUD roughly doubles the cost of care for Medicaid enrollees who have co-occurring medical conditions (Boyd 2010)
8

Future Medi-Cal Enrollees Will Need SUD Services
• 147,000-195,000 new Medi-Cal enrollees in 2014 and beyond will need SUD services (TAC & HSRI 2012)
• Early enrollers likely to have higher levels of SUD need
9

Costs• The Lewin Group evaluated the California’s CMSP
Behavioral health pilot project, found “notable progress on improving coordination between primary care and behavioral health, increasing use of appropriate services, and decreasing hospitalizations and emergency room use.”
• Total costs remained about the same.
• As a result, CMSP (administered by Anthem Blue Cross) decided to cover SUD services in all CMSP counties as of January 1, 2012.

Expanding SUD Services Can
Cut Medicaid Costs• Colorado: State invested $2.4 million in SUD services for Medicaid enrollees (Colorado State Auditor, 2010)
• Savings of $3.5 million in ER, hospital, outpatient, pharmacy, mental health, and dental expenses.
• Caveat: Can’t determine causality.

Expanding SUD Services Can Reduce Medicaid Expenditures• Ohio: Study of Medicaid
enrollees with SUD who received and did not receive services (Gerson 2001)
– 6 months: Enrollees who received SUD treatment incurred half the total Medicaid costs of those who did not get SUD treatment. (caveat: comparison group somewhat self-selected)
– 12 months: Untreated enrollees cost Medicaid 85% more than treated group
12

Expanding SUD Services Can Contain Medicaid Costs
•Washington State: Expanded SUD services for disabled Medicaid population (Wickizer 2012)
– Expenses went up less for those who received SUD treatment than for those who didn’t.
– “Treatment Expansion was “cost neutral”. Estimated cost savings balanced the amount budgeted . . . to expand access to SA treatment”(Wickizer 2012)

Other Cost Studies
• Brief physician advice on SUD leads to $4.30 in savings for every dollar invested (Fleming et al., 2002),
• SBIRT in emergency departments may result in $3.81 in healthcare cost savings for every dollar spent. (Gentilello et al., 2005)

Other Cost Studies
• Compared to drug-free treatment for opioid dependence, buprenorphine reduces costs by 30%. (Baser et al., 2011).
• Compared to oral naltrexone, Vivitrol reduces the cost of inpatient services by 31-38% (Baser et al., 2011, 2011b).
• These studies do not take into account other non-medical savings, such as incarceration. For example for every treatment completer Prop 36 saved California $4 for every $1 spent.

Tools & Data:How do we measure
“Integration”?
http://ahsr.dartmouth.edu/html/ddcat.html

Not with administrative data (yet)California Uniform Data System Data:sparse DOCUMENTATION of services
• In CA FQHCs in 2010, only 0.3% patients had a primary diagnosis of alcohol related disorders.
• Only 0.4% patients were diagnosed with other SUDs (excluding tobacco)
• Similar to national numbers• Usually not reported to CalOMS either.• NOT ACCURATE. Primary diagnosis only
reported. This changed January 2012.Source: http://bphc.hrsa.gov/uds/diagnosesservices.aspx?year=2010&state=CA

Dual Diagnosis Capability in Health Care Settings (DDCHCS) tool
Used to measure Integration / co-occurring capability in health care settings. Requires site visit, interviews, chart review.
For more information see:
http://ahsr.dartmouth.edu/html/ddcat.html

Measuring Integration: Dual Diagnosis Capability in Health
Care Settings (DDCHCS) tool
Scores in 6 California sites ranged from 3.0-3.8 on a 5 point scale, corresponding to “Dual Diagnosis Capable”

21
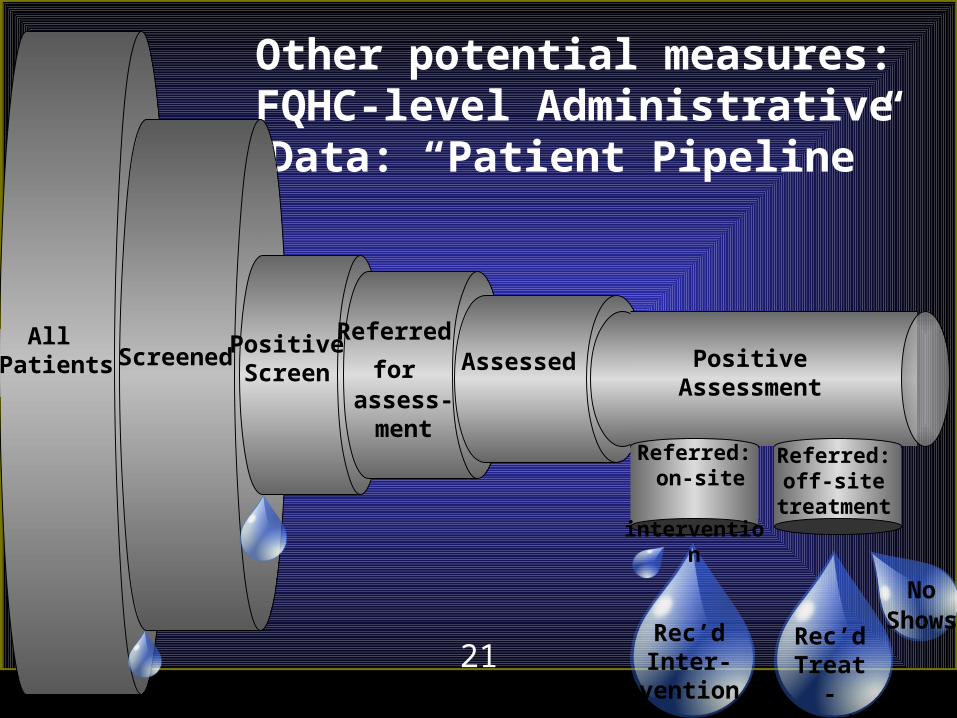
Other potential measures:FQHC-level Administrative Data:
“Patient Pipeline”
All Patients Screened Positive
Screen
Referred for
assess-ment
Assessed PositiveAssessment
Rec’dInter-
vention
Referred: on-site
intervention
Rec’dTreat-ment
Referred: off-site
treatment
No Shows

22
(Yet) Another Measure: Staff Perceptions & Attitudes
SurveysAdapted from surveys developed by the Integrated
Behavioral Health Project (http://www.ibhp.org/)
Multiple versions used:• Behavioral Healthcare Provider Satisfaction Survey• Primary Care Provider Satisfaction Survey• Primary Care Provider Satisfaction Survey - Non
PCP Staff

3.0
3.5
4.0
4.5
5.0
Sati sfi ed w/medical staff abil ity to address MH/SUD
pati ent needs*
Primary Care staff value MH/SUD services*
Communicati on between medical, MH/SUD staff is
good*
Selected Survey Results
Mental Health/SUD Staff Med Ast, Line Staff Primary Care Providers
StronglyAgree
Uncertain

Bigger Picture: Survey of County SUD Administrators
Not Engaged in Initiatives
44%
Planning Initiatives
16%
Engaged in Initiatives
12%
Initial Communi-
cation21%
Learning about
Integration7%
County Participation in SUD-PC Integration Initiatives (n=43)County Participation in SUD-PC Integration Initiatives (n=43)
2010: SUD/primary care integration was in its infancy.
2012 survey is on its way!!
2010: SUD/primary care integration was in its infancy.
2012 survey is on its way!!

Incoming Data:UCLA’s FQHC Study
(funded by the California Program on Access to Care)
• Case studies to assess SUD service delivery and integration in California FQHCs.
• 18 FQHCs invited to participate via survey.
– 14 responded so far (78%).
• Interviews, focus groups currently in progress
• Targeted a few counties with known integration efforts (more integrated than the rest of the state)

FQHC Survey
Web-based survey included questions on:
• FQHC SUD practices
• Integration between SUD services and primary care, MH, and HIV/AIDS services,
• How services are funded, recorded in electronic records, and delivered.
• Policy recommendations.

Findings• Screening: 57% screened all patients for SUD
• Electronic Health records (EHR). 43% do not have an EHR that integrates physical health and MH/SUD records.
• Evidence-based treatment practices: Most common behavioral practices include motivational interviewing, cognitive behavioral therapy, and social skills building (all 50%).

Findings (cont’d)• Medication assisted treatment: 21% reported
prescribing Buprenorphine “sometimes”; none routinely. Even lower percentages were reported for intramuscular naltrexone (Vivitrol).
• Reimbursement: Mixture of FQHC prospective payment system rate (57%), other county sources (36%), grant funding (36%), self-payment, and services provided without any reimbursement.

Findings (cont’d)
• Integration: Though we targeted “high integration” counties, only 43% indicated “Close Collaboration” between SUD and primary care. By contrast, for Mental Health, it was 71%.
• SUD services were well integrated with mental health.
• SUD services were not as well integrated with HIV/AIDS services as with other primary care services.

Findings (cont’d)
• Separation from primary care. Only one FQHC had primary care, SUD services in the same building.
• Delays. No FQHCs reported providing SUD services on the same day as a primary care referral. Most (71%) typically delivered it more than 7 days from referral.
• Training. 78% agreed that additional SUD-related training would be helpful for their clinic staff

Policy Recommendations from Survey
• Expand workforce who can bill for SUD services. In particular add MFTs. Currently only Licensed Clinical Social Workers (LCSWs) and psychologists can bill for behavioral health. “We do not have enough LCSW providers to be able to go into all the community health centers as we would like.”
– This would require legislation and a Medicaid waiver from the federal government.
– Same would apply for SUD counselors.

• Allow same-day billing for two services.
“It would be very helpful if we could bill for mental health and physical health visits on the same day. The current restriction impedes access for our patients.”
Would allow “warm hand-offs” between primary care and SUD or MH. Otherwise they tend to become “no shows”.
• 28 states currently allow same-day billing, but California does not.
Policy Recommendations from Survey

Policy Recommendations from Survey
• Stabilize funding.
“Our integrated effort . . . is funded wholly by grants and MHSA, making it feel precarious and temporary by comparison with other primary care services.”
“allow for reimbursement of case management services. Currently, important roles such as a navigator and peer partner, must be funded by grants, but in the long term these roles must be funded through FQHC or Medi-Cal reimbursement.”

So what’s stopping us?Primary barrier seems to be concern over additional State general fund expenditures. For example, AB 1785 (Lowenthal) would have added MFTs as reimbursable providers and passed 17-0 out of the Assembly Health Committee, but it is currently held under submission by Assembly Appropriations Committee
Translation: probably dead, due to concerns over costs.
How about a pilot project, like CMSP and other states?

ReferencesBaser, O., Chalk, M., Fiellin, D.A. & Gastfriend, D.R. (2011). Cost and utilization outcomes of opioid-dependence treatments.
American Journal of Managed Care,17(8), S235-S248.
Baser, O., Chalk, M., Rawson, R., & Gastfriend, D.R. (2011b). Alcohol dependence treatment: comprehensive healthcare costs, utilization outcomes, and pharmacotherapy persistence. American Journal of Managed Care, 17(8),S222-S234.
Boyd, C., et al. (2010). Clarifying Multimorbidity Patterns to Improve Targeting and Delivery of Clinical Services for Medicaid Populations: Faces of Medicaid Data Brief. Center for Health Care Strategies.
Center for Substance Abuse Treatment (CSAT) (2007). The Epidemiology of Co-Occurring Substance Use and Mental Disorders.
Clark, R.E. et al. (2010). Substance Abuse and Healthcare Costs Knowledge Asset. Web site created by the Robert Wood Johnson Foundation’s Substance Abuse Poliyc Research Program. http://saprp.org/knowledgeassets/knowledge_detail.cfm?KAID=21
Colorado State Auditor. (2010). Medicaid Outpatient Substance Abuse Treatment Benefit. Department of Health Care Policy and Financing Performance Audit. Retrieved from: http://www.leg.state.co.us/OSA/coauditor1.nsf/All/80EE029745B4C589872577F30060F888/$FILE/2079SubstanceAbuseFinalReport12132010.pdf .
Estee, S., Wickizer, T., He, L., Shah, M.F., & Mancuso, D. (2010). Evaluation of the Washington State Screening, Brief Intervention, and Referral to Treatment Project: cost outcomes for Medicaid patients screened in hospital emergency departments. Medical Care, 48(1), 18-24.
Fleming, M.F., Mundt, M.P., French, M.T., Manwell, L.B., Stauffacher, E.A., & Barry, K.L. (2002). Brief physician advice for problem drinkers: long-term efficacy and benefit-cost analysis. Alcoholism: Clinical and Experimental Research, 26(1), 36-43.
Fox, K., et al. (1995). Estimating the costs of substance abuse to the Medicaid Hospital Care Program. American Journal of Public Health. 85(1):48-54.
Gentilello, L.M., Ebel, B.E., Wickizer, T.M., Salkever, D.S., Rivara, F.P. (2005). Alcohol interventions for trauma patients treated in emergency departments and hospitals: a cost benefit analysis. Annals of Surgery, 24(4), 541-550.
Gerson, L.W., Boex, J., Hua, K., Liebelt, R.A., Zumbar, W.R., Bush, D., & Givens C. (2001). Medical care use by treated and untreated substance abusing Medicaid patients. Journal of Substance Abuse Treatment, 20(2), 115-120.

References (continued)The Lewin Group (2011). Evaluation of the CMSP Behavioral Health Pilot Project Final Report. Retrieved from
http://www.cmspcounties.org/pdf_files/CMSPBHPPFINALRPT021711.pdf
Linkins, K.W., et al. (2008). Frequent Users of Health Services Initiative: Final Evaluation Report. Prepared for the California Endowment and the California Healthcare Foundation.
Mancuso, D., Nordlund, D.J., & Felver, B.E.M. (2009). DASA Treatment Expansion: Spring 2009 Update. Olympia, WA: Washington State Department of Social and Health Services. Retrieved from: http://www.dshs.wa.gov/pdf/ms/rda/research/4/75.pdf
McGeary, K.A. & French, M. (2000). Illicit drug use and emergency department utilization. Health Services Research, 35(1), 153-169.
National Center on Addiction and Substance Abuse (NCASA) (2012). Addiction Medicine: Closing the Gap between Science and Practice.
Owens, P.L., et al. (2010) Mental Health and Substance Abuse-Related Emergency Department Visits Among Adults, 2007. Agency for Healthcare Research and Quality.
Parthasarathy, S., Mertens, J., Moore, C., Weisner, C.(2003). Utilization and Cost Impact of Integrating Substance Abuse Treatment and Primary Care. Medical Care, 41(3), 357-367.
Stein, M.D. (1999). Medical Consequences of Substance Abuse. Psychiatric Clinics of North America. 22(2), 351-370.
Substance Abuse and Mental Health Administration (SAMHSA) (2010). Results from the 2009 National Survey on Drug Use and Health.
Technical Assistance Collaborative (TAC) & Human Services Research Institute (HSRI) (2012) California Mental Health and Substance Use System Needs Assessment: Final Report. Submitted to California Department of Healthcare Services.
Thomas, M.R., et al. (2005). Prevalence of psychiatric disorders and costs of care among adult enrollees in a Medicaid HMO. Psychiatric Services, 56(11), 1394-1401.
Vinson, D.C., et al. (2003). A population-based case-crossover and the case-control study of alcohol and the risk of injury. Journal of Studies on Alcohol and Drugs, 64(3), 358-366.
Weisner C, Parthasarathy S, Moore C, Mertens JR. (2010). Individuals receiving addiction treatment: are medical costs of their family members reduced? Addiction. 05(7):1226-34.
Wickizer, T.M., et al. (2012) Evaluation of an innovative Medicaid health policy initiative to expand substance abuse treatment in Washington State. Medical Care Research and Review, 69(5):540-559.

One last plug: Integration Learning Collaborative
• Interactive forum where county administrators and other key stakeholders collaborate to identify successful models of integration and solutions to challenges. See:
http://www.uclaisap.org/Affordable-Care-Act/html/learning-collaborative
• These slides will be available shortly at this website.








![First Total Synthesis of (±)-Strychnine via a [4+2]- Cycloaddition/Rearrangement Cascade Hongjun Zhang, Jutatip Boonsombat, and Albert Padwa* Org. Lett](https://img.pdfslide.us/doc/110x75/56649d9e5503460f94a87dda/first-total-synthesis-of-strychnine-via-a-42-cycloadditionrearrangement.jpg)





















