Embed Size (px)
Citation preview

DENTISTRY TODAY...
The journal is indexed with ‘Indian Science Abstract’ (ISA)(Published by National Science Library), www.ebscohost.com, www.indianjournals.com
The journal is printed on ACID FREE paper.
JADCH is available (full text) online:Website- www.adc.org.in/html/viewJournal.php
This journal is an official publication of Ahmedabad Dental Collegeand Hospital, published bi-annually in the month of March andSeptember.
ISSN 0976-2256E-ISSN: 2249-6653
A
Depression, Let's talk
Depression is a common mental disorder that affects people of all ages, from all walks of life, in all countries.
The risk of becoming depressed is increased by poverty, unemployment, life events such as the death of a loved one or a relationship break-up, physical illness and problems caused by alcohol and drug use. Depression causes mental anguish and can impact on people's ability to carry out even the simplest everyday tasks, with sometimes devastating consequences for relationships with family and friends. Untreated depression can prevent people from working and participating in family and community life. At worst, depression can lead to suicide. Depression can be effectively prevented and treated. Treatment usually involves either a talking therapy or antidepressant medication or a combination of these. Overcoming the stigma often associated with depression will lead to more people getting help. Talking with people you trust can be a first step towards recovery from depression.
Editor - in - ChiefDr. Darshana Shah
Co - EditorDr. Harsh Shah
Editorial Board:Dr. Mihir Shah
Dr. Ganesh M
Dr. Monali Chalishazar
Dr. Neha Vyas
Dr. Sonali Mahadevia
Dr. Shraddha Chokshi
Dr. Bhavin Dudhia
Dr. Mahadev Desai
Dr. Darshit Dalal

Contents
Subscription:Rate per issue: ` 400/-, for one year: ` 750/-, for three years: ` 2,000/-Contact: Ahmedabad Dental College & Hospital Vivekanand Society, Bhadaj-Ranchhod Pura Road, Santej, Post: Rancharda, Ta: Kalol, Dist: Gandhinagar, Gujarat, India.
B
EDITORIAL
FROM THE EDITOR'S DESK .......................................................................................................................................................51DR. DARSHANA SHAH
REVIEW ARTICLES
1) STEM CELLS IN ORTHODONTICS: A REVIEW OF LITERATURE..................................................................................52 NEHA SAXENA*, SONALI MAHADEVIA**, NEHA ASSUDANI***
2) LONG TERM SURVIVAL RATES OF SHORT DENTAL IMPLANTS IN PARTIALLY EDENTULOUS PATIENTS – A SYSTEMATIC REVIEW AND META ANALYSIS .............................................................................................................57 SHASHANK CHAUHAN*, DARSHANA SHAH**, CHIRAG CHAUHAN***, MONAL VORA****
ORIGINAL ARTICLE
3) COMPARATIVE EVALUATION OF AMINE FLUORIDE, CALCIUM SODIUM PHOSPHOSILICATE (NOVAMIN), NANO HYDROXY APATITE CONTAINING DENTRIFICES ON ENAMEL MICROHARDNESS: AN IN VITRO STUDY .............65
KUSHANI SHAH*, NEELAM TALSANIA**, SHRADDHA CHOKSHI***, ZARANA SANGHVI****
4) EVALUATION OF ANTIBACTERIAL EFFICACY OF VARIOUS GEL FORMULATIONS WHEN USED AS AN INTRACANAL MEDICAMENT IN PRIMARY MOLARS – AN IN VIVO STUDY.................................................................74
VRUNDA PARIKH*, DHARATI PATEL**, HINAL THAKKAR***, BHUMI SARVAIYA****, KRUNAL CHOKSHI*****
5) KNOWLEDGE, ATTITUDE AND AWARENESS REGARDING INFANT ORAL HEALTH CARE AMONG ..........................................................................................................................81GYNECOLOGIST AND PEDIATRICIANS BIRVA PATEL*, KINJAL ENGINEER**, VASUDHA SODANI***, RAJAL PATHAK****
CASE REPORT
6) RIDGE EXPANSION AND IMMEDIATE IMPLANT PLACEMENT IN POSTERIOR MANDIBLE: A CASE REPORT ........85 SAVAN CHOVATIA*, HITESH SOLANKI**, SACHIN MODI***, SACHIN DALAL****
7) MANAGEMENT OF BUCCALLY PLACED CANINES USING T-LOOP – A CASE REPORT ............................................91 PRIYANKA SHAH*, SONALI MAHADEVIA**, BHAVYA TRIVEDI***, AATMAN JOSHIPURA****
8) PROSTHETIC REHABILITATION OF THE MAXILLARY DEFECT WITH HOLLOW BULB DEFINITIVE OBTURATOR: - A CASE REPORT ............................................................................................................................................................93 HARSHKUMAR SHAH*, MEHUL PATEL**, DARSHANA SHAH***, CHIRAG CHAUHAN****, PARAS DOSHI*****
9) VESTIBULAR INCISION SUBPERIOSTEAL TUNNEL ACCESS (VISTA) WITH PLATELET RICH FIBRIN (PRF) IN THE MANAGEMENT OF MULTIPLE GINGIVAL RECESSION: A CASE REPORT ...........................................99 NAKUL AMETA*, SHIKHA MAVANI**, HARIT SHAH***, ARCHITA KIKANI****
10) FRENECTOMY WITH LATERAL PEDICLE FLAP- A NOVEL FRENECTOMY TECHNIQUE FOR PREVENTION OF SCAR: A CASE REPORT ..........................................................................................................................................103 SHIKHA MAVANI*, NAKUL AMETA**, HARIT SHAH***, ARCHITA KIKANI****, MIHIR SHAH*****

51
Dr. Darshana ShahEditor JADCHEditorial Office:Prof. & Head Dept. of ProsthodonticsAhmedabad Dental College & Hospital,Dist.: Gandhinagar, Gujarat.Email: [email protected]
The Journal of Ahmedabad Dental College and Hospital; 8 (2), September 2017 - February 2018
____From Editor’s desk
Depression Threatens Oral Health
Depression is one of the most prevalent mental health issues and there is significant relationship between depression and oral health, oral health behavior and oral health related quality of life. Physiological consequences of depression may lead to poor oral health due to Xerostomia, Cariogenic diet and Impaired immune functioning contributing to oral infection. Antidepressant medication also causes Hyposalivation and Bruxism.
It is easy to see that the mouth is connected to the rest of the body and vice versa. As a oral health care taker, it is our duty to see the mental well being of each and every patient. So for that, we must take a thorough medical history and perform Intra and Extra Oral Examination which can assist us in delivering the best care to our patient.

Review Article
ABSTRACT
The purpose of this article is to review and update current data of the use of stem cells for dental but specifically orthodontic purpose. Interest regarding stem cell based therapies for the treatment of congenital or acquired craniofacial deformities is rapidly growing. The use of stem cslla in the day to ay treatment modality is not a vision too far. The growing trend in the regeneration of articular disc and TMJ modifications for treatment of arthiritis is also been seen. The concept of harvesting stem cells followed by expansion, differentiation, seeding onto a scaffold and re transplanting them is likely to become a clinical reality. In this review, tries to summarize the translational applications of stem cell therapy in tissue regenerationin the field of orthodontics.
Keywords: Stem cells, orthodontics, articular disc, cleft
Received: 05-07-2017; Review Completed: 16-08-2017; Accepted: 20-11-2017
Neha Saxena*, Sonali Mahadevia**, Neha Assudani***
52
STEM CELLS IN ORTHODONTICS: A REVIEW OF LITERATURE
* PG Student, **Head of the Department, ***Sr Lecturer
ADDRESS FOR AUTHOR CORROSPONDENCE : DR. NEHA SAXENA, TEL: +91 94276 16197
INTRODUCTION:
Orthodontodics and dentofacial orthopectics is comprehensive branch – dealing not just with teeth but craniofacial structures. Stem cell therapy holds a great potential and can bring a revolutionary change in the field of medicine. The knowledge of stem cells and its implications can help the orthodontists to modify their treatment planning and get quintessential results.
WHAT ARE STEM CELLS?
Stem cells are defined as the cells which have the capacity to divide for indefinite periods of time and with the ability to differentiate into a variety of cell types. Stem cells can be classified into three categories: Totipotent, Pluripotent, and Multipotent cells. Totipotent cells have the potential to differentiate into any type of cell in the body and are capable of developing into a complete organism. Pluripotent cells are capable of dividing and differentiating into any type of cell, tissue, or organ. Multipotent cells have more limited capacities than
1do pluripotent cells.
DEPARTMENT OF ORTHODONTICS AND DENTOFACIALORTHOPAEDICSAHMEDABAD DENTAL COLLEGE AND HOSPITAL, TA. KALOL, DIST: GANDHINAGAR, GUJARAT, INDIA.

53
Characteristics of stem cells1:
• They have the ability to generate at least one daughter cell with characteristics of parent cell.
• Multi lineage differentiation from a single cell
• Functional reconstitution of a tissue
The uses of stem cells in orthodontics are:
• Mandibular growth in mandibular hypoplasia using stem cells
• Maxillary expansion
• In cleft palate cleft lip patients
• Repair of alveolar bone
• In orthodontic root resorption of the teeth
• Distraction osteogenisis
• Regeneration and repair of TMJ defects
• Articular disc of TMJ
M A N D I B U L A R G R O W T H I N MANDIBULAR HYPOPLASIA USING STEM CELLS
Mandibular growth deficiency is one of the important aspect considered in orthodontics during the developing ages. Researches have shown that viral vectors carrying vascular endothelial growth factor (rAAV-VEGF) have been shown to stimulate
1mandibular growth in vivo in rats.
A local injection of vector-loaded VEGF into mandibular condyles can modulate mandibular growth. VEGF may stimulate mandibular growth
1through two mechanisms :
(1) Stimulation of endochondral bone growth.
(2) Recruitment of new replicating mesenchymal stem cells, which is correlated to mandibular growth.
MAXILLARY EXPANSION
The maxillary expansion during orthodontic treatment is usually a tough time for the patients since wearing an apparatus during the treatment causes mouth discomfort. Moreover, to prevent relapse after expansion, it is crucial to induce new bone formation and regeneration during retention phase. Bone marrow–derived mesenchymal stem cells were isolated from the femora of rats, and characterized by osteogenic differentiation. Positive contribution to bone formation was
detected with differentiated mesenchymal stem cells that underwent a successful stem cell therapy in the maxillary expansion model in rats. Histomorphometric findings showed an increase in newly formed bone, number of osteoblasts, and
2amount of vascularization.
It has been mentioned that when BMSCs were exposed to continuous mechanical strain (CMS) of 10% at 1 Hz shows that CMS reduced the proliferation of BMSCs and stimulated osteogenic differentiation by activating Runx2, followed by increased alkaline phosphatase (ALP) activity and mRNA expression of osteogenesis-related genes (ALP, col lagen type I and osteocalcin) . Furthermore, the phosphorylation level of extracellular regulated protein kinase (ERK)1/2 increased significantly at the onset of strain. However, the presence of U0126, a selective inhibitor of ERK1/2, blocked the induction of
9Runx2 and subsequent osteogenic events.
IN CLEFT PALATE CLEFT LIP PATIENTS
Cleft palate and cleft lip patients often suffer from social stigma. They are not only hesitant to take treatment but also wish for early and stable results. Various treatment modalities are used by orthodontists. The American Association of Orthopaedic Surgeons suggests that, given the high demand for grafting procedures, the development and supply of “substitutes for conventional bone grafts” should be a priority.
Neha Saxena et. al. : STEM CELLS IN ORTHODONTICS: A REVIEW OF LITERATURE

In a recent study, embryonic stem cells have been differentiated into cartilage cells and implanted on artificially created cranial osseous defects. In comparison to the control group, the group that received the implanted tissue had a significantly
4faster response rate. Furthermore, another study it has been reported that unilateral alveolar cleft, t r ea ted wi th the compos i t e sca ffo ld o f demineralized bone mineral and calcium sulphate (Osteoset) loaded with mesenchymal stem cells (MSCs), showed 34.5% regenerated bone, extending from the cleft walls and bridging the cleft
5after 4 months with presentation of bone integrity.
IN ORTHODONTIC ROOT RESORPTION OF THE TEETH
Dental pulp is the rich source of stem cells. Apical papilla differs from the dental pulp for containing less cellular and vascular components. However, apical papilla stem cells have shown to have both high repair and differentiation potential. Stem cells from apical papilla (SCAP) stem cells for pulp and dentin repair, together with the association between SCAP and periodontal ligament stem cells the tissue repair has become easy. This advancement is also
3known as BIOROOT ENGINEERING.
REPAIR OF ALVEOLAR BONE
Alveolar bone condition is not just important in the prosthodontic field but also in the orthodontic stream. Unwanted alveolar bony defects are often created after orthodontic extractions repair of these defects can be done by stem cell therapy. In a recent study, the tissue repair cells were grafted into the osseous defects of the jaw of 12 patients and the biopsies were and analysed at six and twelve weeks. Reconstruction was completed with an oral implant therapy and was observed for 12 months postoperatively. It was demonstrated clinically, radiographically, and histologically that the stem cell therapy accelerated the regenerative response. There was also significant reduction in the need for
6secondary bone grafting procedures in this group.
DISTRACTION OSTEOGENISIS
Distraction osteogenesis is defined as the surgical approach by which the development of new bone growth in an area subjected to gradual tension and stress occurs by deliberate separation of the fragments by traction. Limitation of the distraction osteogenesis is – Ischemia which can be overcome
by stem cells.
It is suggested that using stem cells in distraction osteogenesis proves to be a potential method to accelerate bone regeneration in the distraction gap and enhance consolidation. In a study, 54 New Zealand white rabbits underwent osteodistraction of the left mandible and were randomly divided into three groups. At the end of the distraction, bone marrow mesenchymal stem cells (BMMSCs) transfected with osterix (OSX), autologous BMMSCs, and physiological saline were injected into the distraction gap in groups A, B, and C, respectively. It was observed that excellent bone callus formation was seen in groups A and B. The group C animals showed poor bone formation in the distracted callus, when compared to groups A and
6B. The bone induced with the mesenchymal cells is stable. The study has compared the ability of MSCs to heal a critical-sized segmental defect and it suggested that bone fill in MSC is is greater and
12better stable.
REGENERATION AND REPAIR OF TMJ DEFECTS
A TMJ defect often perplexes the doctor. The methods used to reconstruct the TMJ include autogenous bone grafting, such as, harvesting from the rib or the use of alloplastic materials which often leads to unwanted adverse effects. The recent advances in stem cell technology assure the construction of a bioengineered TMJ replacement, which is biocompatible and capable of withstanding the physiological loads. Cells sources include
Neha Saxena et. al. : STEM CELLS IN ORTHODONTICS: A REVIEW OF LITERATURE
54

articular cartilage cells, fibroblasts, human umbilical cord matrix cells, and mesenchymal stem cells. In numerous studies, a tissue-engineered mandibular condyle was constructed, with stratified layers of cartilage and bone from a single population of mesenchymal stem cells, which was moulded into the shape of a human cadaver
6mandibular condyle.
ARTICULAR DISC OF TMJ
Articular disc of TMJ is often affected by various degenerative disorders like osteo arthritis. The e f f e c t s o f c h o n d r o g e n i c d i f f e r e n t i a t e d mesenchymal stem cells (MSCs) on cartilage and s u b c h o n d r a l c a n c e l l o u s b o n e i n temporomandibular joint osteoarthritis (TMJOA) is useful to decrease the arthritis. Mesenchymal cells leads to increased mRNA expression of collegan II, a g g e r a n , S o x 9 a n d d e c r e a s e d m a t r i x metalloproteinase 13 (MMP13). Intraarticular injection of MSCs could delay the progression of temporomandibular joint osteoarthritis by
7chondrogenic proliferation.
There have been various studies which describes the ways to increase the proliferation and hence the regeneration of the bone and the articular disc. One such study suggests that culture of hMSCs in 3D collagen matrices under mechanical strain leads to linear 3D type I collagen matrices and subjected to 0%, 10%, or 12% uniaxial cyclic tensile strain at
1Hz for 4 h/day for 7 or 14 days. There is increase in BMP-2 was also observed in hMSCs subjected to 12% strain.8 Other way to increase the cell differenciation and bone formation is use of low-magnitude, high-frequency mechanical vibration stimulations have a favourable influence on osteocytes, osteoblasts and their precursors, thereby enhancing the expression of osteoblastic genes involved in bone format ion and
10remodelling.
Moreover, MSCs exposed to TGF-β1 were loaded into a sponge composed of a hyaluronan derivative (HYAF®-11) for the construction of the cartilage component of the composite graft, and MSCs exposed to osteogenic supplement were loaded into a porous calcium phosphate ceramic component for bone formation. This leads to formation of Type I collagen in the neo-tissue in both sponge and ceramic, and type II collagen in the fibrocartilage, especially the
11pericellular matrix of cells in the sponge.
CONCLUSION
Nowadays stem cell therapy is one of the most upcoming areas of research in craniofacial tissue engineering. It is apparent for the orthodontists to be prepared for paradigm shifts in craniofacial regeneration. It will be really fascinating to see orthodontists using this therapy on a daily basis to treat patients.
REFERENCES:
(1) Role of stem cells in orthodontics - a review Dr. Mohammadi Begum Indian Journal of Medical Research and Pharmaceutical Sciences; Sep 2013
(2) Bone marrow mesenchymal stem cells enhance bone formation in orthodontically expanded maxillae in rats Abdullah Ekizer et al Angle Orthodontist, Vol 85, No 3, 2015
(3) Expanding therapeutic boundaries: Stem cells and tissue engineering Roberto Rocha Dental Press J Orthod 2011 Sept-Oct;16(5):17-9
(4) Stem cells in orthodontics Anirudh Agarwal Stem Cell Research 2016 Volume 7, Issue 1 (Suppl)
(5) Secondary repair of alveolar clefts using h u m a n m e s e n c h y m a l s t e m c e l l s HosseinBehnia et al Volume 108, Issue 2,
August 2009, Pages e1-e6
(6) Reforming craniofacial orthodontics via stem cells Pritam Mohanty, N.K.K. Prasad et al J Int Soc Prev Community Dent. 2015 Jan-Feb; 5(1): 13–18.
(7) K. Chen, C.et a l Effect of in vi t ro chondrogenic differentiation of autologous mesenchymal stem cells on cartilage and subchondral cancellous bone repair in osteoarthritis of temporomandibular joint Int. J. Oral Maxillofac. Surg. 2013; 42: 240–248
(8) Osteogenic Differentiation of Human Mesenchymal Stem Cells in Collagen Matrices: Effect of Uniaxial Cyclic Tensile Strain on Bone Morphogenetic Protein (BMP-2) mRNA ExpressionRuwan D. Sumanasinghe, Susan H. Bernacki, and Elizabeth G. Loboa. Volume: 12 Issue 12: December 18, 2006
Neha Saxena et. al. : STEM CELLS IN ORTHODONTICS: A REVIEW OF LITERATURE
55

(9) Osteogenic response of mesenchymal stem cells to continuous mechanical strain is dependent on ERK1/2-Runx2 signaling Peng Zhang Yuqiong Wu Zonglai Jiang et al International Journal Of Molecular Medicine 29: 1083-1089, 2012
(10) Effects of mechanical v ibra t ion on proliferation and osteogenic differentiation of human periodontal ligament stem cells Chunxiang Zhang et al Archives of oral biology 57 (20 12) 1395 – 1407
(11) Tissue-Engineered Fabrication of an Osteochondral Composite Graft Using Rat Bone Marrow-Derived Mesenchymal Stem Cells Jizong Gao et al Tissue Engineering Volume: 7 Issue 4: July 9, 2004
(12) Culture-Expanded, Bone Marrow-Derived Mesenchymal Stem Cells Can Regenerate a Critical-Sized Segmental Bone Defect Sudha Kadiyala et al Tissue Engineering Volume: 3 Issue 2: January 13, 2007
Neha Saxena et. al. : STEM CELLS IN ORTHODONTICS: A REVIEW OF LITERATURE
56

Review Article
ABSTRACT
Aim: The objective of this systematic review was to assess the survival rates of short dental implants (<10 mm) in partially edentulous patients.
Materials and Methods: The literature was searched electronically and 1157 studies were identified and final 8 studies were included based on the inclusion and exclusion criterias in which cumulative implant survival rate and marginal bone loss along with crown-implant ratio was avaluated.
Result: From the 8 studies, the cumulative implant survival rate was the most common parameter assessed, ranging from 92.1% at 1 year to 100% at 2 years. The marginal bone loss in all the studies was 0.03 to 0.75 mm with mean marginal bone loss 0.42 mm.
Conclusion: The best and maximum survival rate of 100% can be attained by using short dental implants of 7 mm with porous sintered surface treated with spherical titanium particles with a delayed loading protocol and by giving a prosthesis of porcelain fused to metal with a minimum marginal bone loss of 0.03 mm.
Keywords: Short dental implants, Dental implants treatment outcomes, Dental implants partially edentulous, Dental implants surface topography, Dental implants survival rate.
Received: 25-07-2017; Review Completed: 01-09-2017; Accepted: 03-11-2017
Shashank Chauhan*, Darshana Shah**, Chirag Chauhan***, Monal Vora****
57
LONG TERM SURVIVAL RATES OF SHORT DENTAL IMPLANTS IN PARTIALLY EDENTULOUS PATIENTS – A SYSTEMATIC REVIEW AND META ANALYSIS
*PG Student, **Professor and Head, ***Professor, **** PG Student
ADDRESS FOR AUTHOR CORROSPONDENCE : DR. SHASHANK CHAUHAN, TEL: +91 9898277072
DEPARTMENT OF PROSTHODONTICS, CROWN AND BRIDGE AND ORAL IMPLANTOLOGY,AHMEDABAD DENTAL COLLEGE AND HOSPITAL, GANDHINAGAR, GUJARAT- 382115
INTRODUCTION:
Short implants are increasingly used for the prosthetic solution of the extremely resorbed
posterior zone of partially and fully edentulous patients. However, there is no consensus in the literature on the definition of a short implant. Sometimes less than 10 mm is considered the
[1]minimal length for predictable success and also
[2]sometimes 10 mm is considered as short. Because an implant can be placed at different levels a short implant has also been defined as an implant with a
[3]designed intra-bony length of 8 mm or less.
When applying 6 and 7 mm implants, short dental implants with press-fit shape and a sintered porous
[4]surface geometry revealed the best performance . Short implants should be considered as an a l te rna t ive t rea tment to advanced bone augmentation surgeries.
The placement of short (≤ 8 mm or < 10 mm) rough-surface implants is not a less efficacious treatment modal i ty compared to the placement of
[5]conventional (≥ 10 mm) rough-surface implants.
In the past short implants have been associated with [6,7]lower survival rates . There are several presumed
reasons for a lower survival rate of short implants in the posterior maxilla or mandible. First, compared
to longer implants with a comparable diameter there is less bone to implant contact when short implants are used, simply because there is less implant surface. Secondly, short implants are mostly placed in the posterior zone where the quality of the alveolar bone is relatively poor, especially in the maxilla (type III or IV, Lekholm & Zarb 1985). Thirdly, often a very outsized crown has to be made to reach occlusion, because of the extensive resorption in the posterior region, which causes a higher (<1 - >2) crown to implant ratio. Crown to implant ratios between 0.5 and 1 were proposed to prevent peri-implant bone stress, crestal bone loss
[8 , 9,10]and eventually implant failure. Some study also states that the crown to implant ratio does not affect
[11]the peri-implant crestal bone loss .
To avoid the use of short implants the extremely resorbed bone can be augmented using a bone grafting technique. This modification in the patient's anatomy makes it possible to insert a longer implant, but an extra surgical intervention also leads to greater patient's morbidity, higher costs and a longer treatment period. Short implants (5-8 mm) are more effective and cause fewer complications than longer implants placed using a more complex technique. Short implants appear to be a better alternative to vertical bone grafting of resorbed mandibles. Complications, especially for

[12]vertical augmentation, are common.
New developments of the different implant systems, especially regarding the surface microtopography and chemistry, has resulted in
[3,4,5,6]higher survival rates of short implants.
The implant surface used to be a smooth turned surface, but now-a-days different techniques e.g. acid etching, grit blasting and titanium plasma spraying, altered the micro-topography of the implant surface by making the surface rougher. Apply ing these t echn iques resu l t s in a tremendously enlarged implant surface. Various developments are been seen on the level of
[13]nanotopography.
To our knowledge, no systematic review with meta-analyses to determine the role of possible predictors has been performed on short (<10 mm) endosseous implants in the partiallyedentulous patients. Hence, the objective of this article was to systematically assess the survival rates of short implants (<10 mm) in partially edentulous patients and to evaluate the sources of heterogeneity between studies by subgroup analyses (viz. length, surface topography, implant location (mandible versus maxilla).
MATERIALS AND METHODS
Sources used:
An electronic search was conducted for articles in English, listed with PubMed, Medline, Embase, Cochrane from January 2000 to March 2016.
The search methodology applied was combination of MeSH terms and keywords like- Short dental implants, Dental implants treatment outcomes, Dental implants partially edentulous, Dental implants surface topography and Dental implants survival rate.
Review articles as well as references from different studies were also used to identify the relevant articles.
Selection of studies:
The review process consists of two phases. In first phase, titles and abstract of the search were initially screened by two authors for relevance and the full text of relevant abstract were obtained and assessed. Any disagreements were solved by discussion or third author suggestion, if needed. The hand search of selected journals as well as search of references of the selected studies were
also done. The articles were obtained after first step of the review process using the following inclusion and exclusion criteria which were screened in second phase and relevant and suitable articles were isolated for further processing and data extraction. Duplicates and articles with insufficient necessary data were excluded by the two authors and any disagreements were resolved by the third author suggestions.
Inclusion Criteria:
1. Study design- Randomized Controlled Trials and Prospective Cohort Study.
2. Partially edentulous patients.
3. Studies with reported implant survival rates as wellas criteria for implant failure.
4. Minimum 1 year follow up time.
5. Implant length- less than 10 mm.
6. Minimum sample size of 10 healthy patients.
7. Posterior maxilla and mandible region
Exclusion criteria:
1. Retrospective studies.
2. Case reports.
3. Reviews.
4. Non-clinical studies.
5. Animal subjects.
6. Augmented region.
7. Grafted sites.
8. Patients with systemic diseases.
Results of the search:
The search from the electronic databases identified a total of 1157 titles of short implants studies, out of which 800 were excluded after discussion. From the 357 titles selected, only 175 abstracts were electable to search for detailed analysis based on inclusion criteria. Among them, 37 articles were selected to full text analysis. Additional searching on their bibliographies provided 3 more studies, with a total of 40 articles in the full text evaluation. Finally, 32 articles were excluded based on the exclusion criteria. This resulted in a final number of 8 publications for the current review.
Data extraction:
Data of the finally included studies were tabulated and the following information were
Shashank Chauhan et. al. : LONG TERM SURVIVAL RATES OF SHORT DENTAL IMPLANTS IN PARTIALLY EDENTULOUS PATIENTS – A SYSTEMATIC REVIEW AND META ANALYSIS
58

extracted. Study, no. of subjects, no of implants, implant length, implant surface, location, prosthesis material, loading protocol, follow up period, drop outs, implant failure, cumulative implant survival, x ray technique, calibration, mean marginal bone loss, crown-implant ratio. The specified values were tabulated and subjected to statistical analysis.
Potentially relevant publication identified from databases (n=1157)
Articles excluded by reading the titles (n=800)
Abstract selected by reading the title (n=357)
Articles excluded by reading the abstracts (n=182)
Abstract searched for detailed evaluation (n=175)
Articles excluded based on inclusion criteria (n=135)
Articles and cited articles included for full text analysis (n=40)
Articles excluded based on the exclusion criteria (n=32)
Articles included in this systematic review (n=8)
Shashank Chauhan et. al. : LONG TERM SURVIVAL RATES OF SHORT DENTAL IMPLANTS IN PARTIALLY EDENTULOUS PATIENTS – A SYSTEMATIC REVIEW AND META ANALYSIS
59

Table 1: Summary of the implant characteristics of the 8 included studies
SR. NO. STUDY YEARTOTAL NOOF SUBJECT
TOTAL NOOF IMPLANTS
IMPLANTLENGTH(mm)
IMPLANTSURFACE
LOCATION PROSTHESISMATERIAL
LOADINGPROTOCOL
FOLLOWUP(YEARS)
DROPOUTS
IMPLANTFAILURE
CUMULATIVEIMPLANTSURVIVAL
1
2
3
4
5
6
7
8
Deporter et al. (14) 2001
2006
2010
2011
2012
2012
2012
2013
24
109
35
46
30
92
80
20
48
262
40
107
60
149
115
46
Tawii et al. (15)
Rossi et al. (16)
De santis et al. (17)
Cannizzaro et al.(18)
Teleman et al. (19)
Telleman et al. (20)
Kim et al. (21)
7 and 9
<10
6
7 and 8.5
6.5
8.5
8.5
7
Porous sinteredimplant treatedwith sphericaltitaniumparticies
Machined-surface
SLActive-modifiedsurfaceimplants
OxidizedSurfaec
Dual etchedcovered withnanoscalecalciumphosphatecrystal
Dual-acidsurface withdeposition ofnonometersized Capparticies
Dual-acidetched surface
Sla sufacetreatment
Posteriormandible
Posteriormandiblemaxilla
Posteriormaxilla
Posteriormandiblemaxilla
Posteriormaxilla
Posteriormandiblemaxilla
Posteriormandiblemaxilla
Posteriormaxilla
Proceiain fusedto metal crowns
Proceiain fusedto metal crowns
Proceiain fusedto goldpailadium alloy
Not reported
Acrylic crownsand metalceramic crowns
Metal-ceramiccrowns
Metal-ceramiccrowns
Not reported
DelayedLoading
Not reported
DelayedLoading
DelayedLoading
Immediate andearly loading
DelayedLoading
DelayedLoading
One and two-stage approach
2
±2
2
3
4
5
1
1
0
Notreported
0
Notreported
0
1
0
Notreported
0
2
2
4
2
9
7
1
100%
95.5%(repported in Tiwii et al.2003)
95%
96.3%
93.3%
Controls 92.1%tests 95.9%
Controls 93.1%tests 94.5%
97.8%
Table 2: Summary of the main methods of implant analysis applied in the 8 included studies
SRNO
REFERANCE IMPLANTLENGTH(mm)
X-RAY TECHNIQUE CALLIBRATION MEAN MARGINAL BONELOSS
CROWN-IMPLANTRATIO RESULTS
CUMULATIONIMPLANTSURVIVAL
FOLLOWUP(YEARS)
1
2
3
4
5
6
7
8
Deporteret al. (14)
Tawil et al. (15)
Rossi et al. (16)
Desantiset al. (17)
Cannizzaro etal. (18)
Tellemanet al. (19)
Tellemanet al. (20)
Kim et al. (21)
7 and 9
<10
6
7 and 8.5
6.5
8.5
8.5
7
CUstomized acrylic resintemplates and standard longcone paralleling technique
Long-cone technique andnon-customized parallelingdevice
Standardized rediographsabtained using individuallyfabricated firm holders
Not reported
Paralleling technique
Paralleling technique and anindividalized holder
Paralleling technique and anindividalized holder
Parallel cone technique
Not reported
Not reported
Not reported
Not reported
K-ray images werecallibrated by the knowndistance of twoconsecutive threads
Callibration based on theknown distance of thethreads. Reliability of theX-ray measures assessedin 30 x-rays of 20 patientsby two examiners(ICC=0.87)
Callibration based on theknown distance of thethreads. Reliability of theX-ray measures assessedin 30 x-rays of 20 patientsby two examiners
Not reported
Mean bone loss of 0.03 mm(baseline and 6 months);bonegain of 0.32 mm (1 to 2 years)
Mean bone loss was 0.74 ±0.65 mm
Mean bone loss of 0.75 ±0.71 mm (insertion to 2 yearfollow up) and 0.43 ± 0.49mm (loading to 2 year follow up)
Mean bone loss of 0.6 ± 0.2mm (rane 0.0-19 mm)
Mean bone loss of 0.37 mm(immediate loading) and 0.31mm (early loading)
Mean bone loss was lessaroaund platform-switched(0.5 ± 0.53 mm) than incontrol implants (0.74+0.61mm)
Mean inter-proximal boneloss were less aroundplatform-switched (0.51 ±0.51 mm) than in controlimplants (0.73± 0.48 mm)
Mean bone loss of 0.04 mm(two stage) and 0.16 mm(one stage)
Not reported
Relatively few C/1 ratioswere ,1 or .2 (16.2%)
C/1 ratio was 1 +-0.2(range 0.7-1.4)
Not reported
Not reported
Not reported
Not reported
Cl ratios > 1.5 displayed-higher pocket depth thanthe group with ratio < 1.5
100%
95.5%
95%
96.3%
93.3%
Control group92.1%Test group95.9%
Control group93.1%Test group94.5%
97.8%
2
±2
2
3
1
1
1
4
Shashank Chauhan et. al. : LONG TERM SURVIVAL RATES OF SHORT DENTAL IMPLANTS IN PARTIALLY EDENTULOUS PATIENTS – A SYSTEMATIC REVIEW AND META ANALYSIS
60

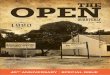
Figure 1: Forest plot of cumulative implant survival rate and subgroup analysis per study design
Study name Cumulative statistics Cumulative event rate (95% CL)
Deporter et al. 2001Tawii et al. 2006Rossi et al. 2010De santis et al. 2011Cannizzaro et al. 2012Telleman et al. 2012Tekkeman et al. 2013Kim et al. 2013
0.0100.0080.0180.0240.0260.0330.0390.0380.038
0.0010.0020.0050.0090.0130.0170.0230.0240.024
0.1480.0280.0650.0570.0510.0620.0640.0610.061
-3.168-7.637-5.841-7.926
-10.145-10.095-11.826-12.795-12-795
0.0020.0000.0000.0000.0000.0000.0000.0000.000
0 / 483 / 3105 / 3509 / 45711 / 51720 / 66627 / 78128 / 827
PointLowerlimit
Upperlimit Z-Value p-Value Total
Relativeweight
Relativeweight
2.8413.0922.6438.4648.0872.8394.47100.00
-1.00 -0.50 0.00 0.50
Fav ours A Fav ours B
1.00
DISCUSSION
The main purpose of this systematic review was to find out the necessary parameters required to evaluate the long-term clinical performance of shortdental implants in partially edentulous patients. Several differences have been found in the definition of short implants in the literature. Finally thedefinition of endosseous dental implant that has a 'designedintrabony length' less than or equal to 10 mm, was selected as a guide to search the articles.
[22]This was given by Renouard et al . From the eight articles selected, the cumulativeimplant survival rate was the most common parameterassessed,
[19]ranging from 92.1% at 1 year to 100% at 2 years [14]
. Data meta-analysis revealed positive effect size to be 0.038 (Z=12.79; p<0.002) at fixed model analysis whichmeans that the provision of short implant in atrophicalveolar ridges appears to be a successful treatment option.
[23]According to Annibali et al. , short
implants are not supposed to be compared with longerimplants placed in the native jawbone. The most suitablecomparison should bebetween short implantsand advanced surgical techniques, which are necessary to place longerimplants in resorbed
[23]posterior jaws . The method of evaluating survival in moststudies is a point of concern because several studiesapply a simple ratio between the number of implantsremoved and the total number of implants placed. Thismethod may mislead since it does not
[24]consider the effects of time .
Recent literature stated that the increased survival rateof short implants to the surface structureis because of thehigher bone-to-implant
[25]contact . All the studies selected in this review, described the type of surface, amongst which
themoderate rough surfaces was selected in most of the cases. The detailing of the implant system also increasesthe reproducibility of the study and allows the comparison of results. Hence it was possible to find out the mostsuccessful surface to be used in
[16]short dental implants .
Based on the clinical performances of conventionalcrown-to-root ratio, those with susceptibility towards harmful lateralocclusal
[26]forces , it was believed that excessive crown-to-implant ratio could be detrimental to long-term implant survival, that too when short implants are
[27]considered . Thehigher the crown, the longer will be thelever arm, and consequently the greater will be the stress inmarginal bone which may lead to an
[27,28, 29]increase in the marginal bone loss . Several [27,28,30]
studies have shownthe absence of an association between crown-to-implant ratio and marginal bone loss, even in cases ofhigh crown-to-
[30]implant ratio of 2.4 . Various reasons behind this fact, include thetreatment of the implant surface and the level in whichthe implant shoulder is placed at the crestal bone.
The second parameter which has been assessed in the selected articlesas an important outcome to measure implant success wasthe mean marginal bone loss. A greatrange of values were noticed with mean marginal boneloss varying from 0.03 to 0.75 mm. Thepossible reason for such variations might be the limits usedas a reference to measure the marginal bone loss or theplacement of the implants in different levels of the crestalbone.
The present systematic review is a basic vision of the vast fieldof research in short dental implants. And therefore it is impossible to guarantee thatall parameters used in the follow-up evaluation
Shashank Chauhan et. al. : LONG TERM SURVIVAL RATES OF SHORT DENTAL IMPLANTS IN PARTIALLY EDENTULOUS PATIENTS – A SYSTEMATIC REVIEW AND META ANALYSIS
61

of short implants were included as it requires a detailed description of literature, which is not usual in a systematicreview. Also a specific evaluation regarding the risk ofbias of each selected study was not applied in this review mainly because only few randomized clinical trialswere included and the principal focus of the study wasthe parameters used for the implant assessment, not theresult itself.
CONCLUSION
From the systematic review of available literature following conclusion can be drawn:
1. Marginal Bone loss – The marginal bone loss in all the studies was 0.03 to 0.75 mm with mean marginal bone loss 0.42 mm with the survival rate of 92.1 to 100%.
2. Features related to loading protocol - Short dental implants with delayed loading protocol showed a maximum of survival rate compared to those with early loading protocols.
3. Characteristics of the implants (brands, surface treatment, length, diameter, s h a p e a n d i m p l a n t - a b u t m e n t connection) – Porous sintered implant treated with spherical titanium particles followed by SLA treated implant surface with platform switch connection showed the best survival rate; short
dental implants with length 7 mm to 9 mm resulted in the best outcome.
4. Particularit ies of the prosthesis (material, crown length, C/I ratio) – studies which gave a prosthesis of porcelain fused to metal crowns showed more survival rate of short dental implants compared to the prosthesis of porcelain fused to gold-palladium and metal ceramic crowns; the C/I ratio was found to around 1 to 2 amongst all the studies.
5. Biological parameters (periodontal t i s s u e a n d h y g i e n e c o n d i t i o n assessment) – Professional cleaning, hygiene instructions and recall visit after 4 to 6 months increases the long term survival rate of short dental implants.
After assessment of all the parameters to evaluate the survival rate of short dental implants, we can conclude that the best and maximum survival rate of 100% can be attained by using short dental implants of 7 mm with porous sintered surface treated with spherical titanium particles with a delayed loading protocol and by giving a prosthesis of porcelain fused to metal. The minimum of marginal bone loss of 0.03 mm can be seen with this type of short dental implants and without any complications.
REFERENCES:
1. Morand M. &Irinakis T. The challenge of implant therapy in the posterior maxilla: providing a rationale for the use of short implants. The Journal of Oral Implantology 2007; 33; 257-266.
2. Das Neves F. D., Fones D., Bernardes S.R., do Prado C.J. &Neto A.J. Short implants- An analysis of longitudinal studies. The International Journal of Oral and Maxillofacial Implants 2006; 21; 86-93.
3. Renouard F. &Nisand D. Impact of length and diameter on survival rates. Clinical Oral Implant Research 2006; 17; 35-51.
4. Hagi D., Deporter D. A., Pilliar R. M. &Arenovich T. A targeted review of study outcomes with short (≤7 mm) endosseous dental implants in
part ial ly edentulous patients. Journal of Periodontology 2004; 75; 798-804.
5. Kotsovilis S., Fourmousis I., Karoussis I.K. &Bamia C. A systematic review and meta-analysis on the effect of implant length on the survival of rough-surface dental implants. Journal of Periodontology 2009; 80; 1700-18.
6. Romeo E., Bivio A., Mosca D., Scanferla M., Ghisolfi M. & Storelli S. The use of short dental implants in clinical practice: literature review. Minerva Stomatologica 2010; 59; 23-31.
7. Lee J.H., Frias V., Lee K.W. & Wright R.F. Effect of implant size and shape on implant success rates: A literature review. Journal of Prosthetic Dentistry 2005; 94; 377-381.
8. Haas R., Mensdorff-Pouilly N., Mailath G.
Shashank Chauhan et. al. : LONG TERM SURVIVAL RATES OF SHORT DENTAL IMPLANTS IN PARTIALLY EDENTULOUS PATIENTS – A SYSTEMATIC REVIEW AND META ANALYSIS
62

&Watzek G. Brånemark single tooth implants: A preliminary report of 76 implants. The Journal of Prosthetic Dentistry 1995; 73; 274-79.
9. Rangert B.R., Sullivan R.M. &Jemt T.M. Load factor control for implants in the posterior partially edentulous segment. The International Journal of Oral and Maxillofacial Implants 1997; 12; 360-370.
10. Glantz P.O. &Nilner K. Biomechnical a s p e c t s o f p r o s t h e t i c i m p l a n t - b o r n e reconstructions. Periodontology 1998; 17; 119-24.
11. Blanes. To what extent does the crown-implant ratio affect the survival and complications of implant-supported reconstructions? A systematic review. Clinical Oral Implant Research 2009; 20; 67-72.
12. Esposito M., Grusovin M.G., Rees J., Karasoulos D., Felice P., Alissa R., Worthington H.V. &Coulthard P. Interventions for replacing missing teeth: augmentation procedures of the maxillary sinus. The Cochrane database of systematic reviews 2010; 17; CD008397.
13. Meirelles L., Currie F., Jacobsson M., Albrektsson T. &Wennerberg A. The effect of chemical and nanotopographical modifications on the early stages of osseointegration. The International Journal of Oral & Maxillofacial Implants 2008; 23; 641-647.
14. Deporter D, Pilliar RM, Todescan R, Watson P, Pharoah M. Managing the posterior mandible of partially edentulous patients with short, porous-surfaced dental implants: early data from a clinical trial. Int J Oral Maxillofac Implants 2001; 16; 653-658.
15. Tawil G, Aboujaoude N, Younan R. Influence of prosthetic parameters on the survival and complication rates of short implants. Int J Oral Maxillofac Implants 2006; 21; 275-282.
16. Rossi F, Ricci E, Marchetti C, Lang NP, Botticelli D. Early loading of single crowns supported by 6-mm-long implants with a moderately rough surface: a prospective 2-year follow-up cohort study. Clin Oral Implants Res 2010; 21; 937-943.
17. De Santis D, Cucchi A, Longhi C, Vincenzo B. Short threaded implants with an oxidized surface to restore posterior teeth: 1- to 3-year results of a
prospective study. Int J Oral Maxillofac Implants 2011; 26; 393-403.
18. Cannizzaro G, Felice P, Leone M, Ferri V, Viola P, Esposito M. Immediate versus early loading of 6.5 mm-long flapless-placed single implants: a 4-year after loading report of a split-mouth randomised controlled trial. Eur J Oral Implantol 2012; 5; 111-121.
19. Telleman G, Meijer HJ, Vissink A, Raghoebar GM. Short implants with a nanometer-sized CaP surface provided with either a platform-switched or p la t form-matched abutment connection in the posterior region: a randomized clinical trial. Clin Oral Implants Res 2013; 24; 1316-1324.
20. Telleman G, Raghoebar GM, Vissink A, Meijer HJ. Impact of platform switching on inter-proximal bone levels around short implants in the posterior region; 1-year results from a randomized clinical trial. J Clinic Periodontol 2012; 39; 688-697.
21. Kim YK, Yun PY, Yi YJ, Bae JH, Kim SB, Ahn GJ. One-year prospective study of 7 mm long implants in mandible: installation technique and crown/implant ratio of 1.5 or less. J Oral Implantol 2013; 41; 30-35.
22. Renouard F, Nisand D. Impact of implant length and diameter on survival rates. Clin Oral Implants Res 2006; 17; 35-51.
23. Annibali S1, Cristalli MP, Dell'Aquila D, Bignozzi I, La Monaca G, Pilloni A. Short dental implants: a systematic review. J Dent Res 2012; 91; 25- 32.
24. Chrcanovic BR, Albrektsson T, Wennerberg A. Reasons for failures of oral implants. J Oral Rehabil 2014; 41; 443-476.
25. Telleman G, Raghoebar GM, Vissink A, den Hartog L, Huddleston Slater JJ, Meijer HJ. A systematic review of the prognosis of short (<10 mm) dental implants placed in the partially edentulous patient. J Clinic Periodontol 2011; 38; 667-676.
26. Grossmann Y, Sadan A. The prosthodontic concept of crown-to-root ratio: a review of the literature. J Prosthet Dent 2005; 93; 559-562.
27. Birdi H, Schulte J, Kovacs A, Weed M, Chuang SK. Crown-to-implant ratios of short-
Shashank Chauhan et. al. : LONG TERM SURVIVAL RATES OF SHORT DENTAL IMPLANTS IN PARTIALLY EDENTULOUS PATIENTS – A SYSTEMATIC REVIEW AND META ANALYSIS
63

length implants. J Oral Implantol 2010; 36; 425-433.
28. Blanes RJ. To what extent does the crown-implant ratio affect the survival and complications of implant-supported reconstructions? A systematic review. Clin Oral Implants Res 2009; 20; 67-72.
29. Rangert BR, Sullivan RM, Jemt TM. Load factor control for implants in the posterior partially edentulous segment. Int J Oral Maxillofac Implants 1997; 12; 360-370.
30. Anitua E, Alkhraist MH, Pinas L, Begona L, Orive G. Implant survival and crestal bone loss around extra-short implants supporting a fixed denture: the effect of crown height space, crown-to-implant ratio, and offset placement of the prosthesis. Int J Oral Maxillofac Implants 2014; 29; 682-689.
Shashank Chauhan et. al. : LONG TERM SURVIVAL RATES OF SHORT DENTAL IMPLANTS IN PARTIALLY EDENTULOUS PATIENTS – A SYSTEMATIC REVIEW AND META ANALYSIS
64

ABSTRACT
Aim: To evaluate and compare the microhardness of enamel surface after the application of fluoride, novamin, and hydroxyapatite containing dentifrices. Materials and Methods: Twenty freshly extracted premolars were collected and decoronation of all the teeth was done at cementoenamel junction. The crowns were sectioned mesiodistally into two halves with the help of diamond disc, and then the subsequent forty samples kept in 1% citric acid for the demineralization in an incubator at 350C temperature for 72 hours. The samples were randomly divided into four groups of 10 samples in each group, that is, Group A(Control Group), Group B (sodium fluoride dentifrice), Group C(Novamin dentifrices) and Group D(Hydroxyapatite dentifrices). Groups B, C & D were treated using prepared dentifrices slurries for 3 min daily, twice for 7 days at room temperature. The samples were preserved in artificial saliva in between treatment. The enamel surface microhardness was evaluated using Vickers hardness test at base level, after demineralization, as well as after remineralization. Statistical analysis of surface microhardness obtained at different stages was done by Student's t -test and P < 0.05 was considered statistically significant. Result: Group B C & D showed significant increase in microhardness as compare to Group A. Conclusion: nHAP based dentifrices showed greater increase in microhardness as compare to other groups.
Keywords: Amine fluoride, Demineralization, Dentifrices, Microhardness, Remineralization, Novamin, Nano hydroxyapatite, Artificial saliva, Citric acid.
Received: 02-05-2017; Review Completed: 05-09-2017; Accepted: 08-01-2018
Kushani Shah*, Neelam Talsania**, Shraddha Chokshi***, Zarana Sanghvi****
65
COMPARATIVE EVALUATION OF AMINE FLUORIDE, CALCIUM SODIUM PHOSPHOSILICATE (NOVAMIN), NANO HYDROXY APATITE CONTAINING DENTRIFICES ON ENAMEL MICROHARDNESS: AN IN VITRO STUDY
*PG Student, **PG Student, *** Professor and Head, ****Professor
ADDRESS FOR AUTHOR CORRESPONDENCE : DR. KUSHANI SHAH, TEL: +91 9974528180
DEPARTMENT OF ENDODONTICS, AHMEDABAD DENTAL COLLEGE AND HOSPITAL
Original Article
INTRODUCTION:
Regardless of the age, gender and ethnicity - dental caries, affects a major portion of the world's population. Dental caries is "an infectious microbiological disease of the teeth that results in localized dissolution and destruction of calcified tissues." It is caused due to physiological imbalance between oral microflora and pathological factors. The occurrence of caries is pH dependent. When pH drops below5.5, enamel dissolution starts,
1-2embarking demineralization. Silverstone (1977) defined demineralization as the process of removing minerals, in the form of mineral ions, from dental enamel. Formation of bacterial acids lowers the pH to the point where the hydroxyapatite mineral of enamel dissolves and this mineral loss lead to cavitation in future. The immediate fluid environment involved in demineralization of a tooth is the fluid phase of plaque i.e. 'plaque fluid' and not the saliva. Neutralizing the oral pH opposes the process of demineralization. By definition, remineralization is the process whereby partially demineralized enamel is repaired through the recrystallization of tooth enamel mineral salts. Remineralization represents an important natural mechanism of the oral environment in its defense,
against caries. From a clinical standpoint, remineralization has been associated with the arrest of developing caries and the reversal of clinically diagnosed incipient white spots. Carious lesion r e m i n e r a l i z a t i o n o c c u r s w h e n t h e r e i s supersaturation of saliva with respect to calcium
26phosphate mineral phases.
Numerous mechanisms are available for accelerated remineralization. It involves a delivery
1mechanism of ions to the affected area. Various remineralizing agents like fluoride, potassium nitrate, Casein phosphopeptide stabilized amorphous calcium phosphate, unstabilized ACP, CPP stabilized amorphous calcium phosphate with fluoride are available.
The discovery of remineralizing agents such as fluorides is a boon for the field of dentistry. There are various types of INORGANIC FLUORIDE preparations available such as stannous fluoride, acidulated phosphate fluoride, sodium mono-fluorophosphate and sodium fluoride.1 Muhlemann in h i s s tudy conc luded tha t ORGANIC FLUORIDES such as amino fluoride(organic fluoride) have shown significant superior results than that of inorganic fluorides in decreasing the
3solubility of enamel. The unique position of amine

fluorides is based on their special molecular structure consisting of a hydrophilic (water soluble) and fluoride binding amine group attached to a
4hydrophobic (water insoluble) hydrocarbon chain. Due to their surface activity, amine fluorides are rapidly dispersed in the oral cavity and wet all surfaces , thereby covering teeth with a homogeneous molecular layer and transporting
4fluoride ions to appropriate sites.
Numerous other mechanisms are also available for accelerated remineralization of tooth structure besides fluoride such as bioactive glass, novamin, arginin, nano hydroxyapaptite, theobromine, self-assembling peptides, inotophoresis and sugar alcohol.
Recent ly, b ioact ive g lass mater ia ls and nanohydroxyapatite have been introduced in many fields of dentistry. NovaMin (calcium sodium phosphosilicate bioactive glass.) is a known component made of bioactive glass particulates
6-8with a median size of less than 20 microns.
Nano-hydroxyapatite (n-HAp) is considered one of the most biocompatible and bioactive materials, and has gained wide acceptance in medicine and dentistry in recent years. Synthetic nano-hydroxyapatite (n-HAP) has the same chemical-physical properties as the apatite structure within enamel. These products are envisaged to promote remineralization due to size-specific effects of the apatite nano-particles corresponding to the ultrastructure of the enamel.
● This study sought to test two hypotheses.
1. The first hypothesis was that each of the three d e n t i f r i c e s w o u l d p r o m o t e e n a m e l remineralization that is significantly greater than zero.
2. The second hypothesis was that the three dentifrices differ with respect to post-treatment remineralization. Of special interest was whether the nHAP-based dentifrices promote greater enamel remineralization and enamel microhardness relative to the fluoride dentifrice and novamin based.
Demineralization and remineralization have a crucial impact on the hardness and strength of tooth enamel. Thus, here we have done comparative evaluation of amine fluoride, calcium sodium phosphosilicate (novamin), nanohydroxy apatite
containg dentrifices on enamel microhardness.
MATERIALS AND METHOD
For this prospective study, 20 caries free, freshly extracted premolars were collected. Carious teeth were excluded from samples. The sample size was selected according to systematic random sampling
9method and ISO 24153:2009 standards. Prophylaxis of all the samples were done using ultrasonic scalers and were polished with an abrasive paste (Smile and Shine, ICPA) and brush. Decoronation of all the teeth was done at cementoenamel junction, and the crowns were sectioned mesiodistally into two halves with the help of diamond disc. Then, the subsequent forty samples distributed in four groups by simple randomization, that is, Group A, Group B, Group C and Group D with 10 samples each.
● Group A (Control group)
● Group B (Sodium fluoride dentifrice)
● Group C (Calcium sodium phosphosilicate bioactiveglass dentifrices)
● Group D (Hydroxyapatite dentifrices).
The samples were placed in acrylic resin filled molds facing buccal surface upwards. A Vickers microhardness indenter (fuel instruments and engineer pvt ltd ) used to check the baseline microhardness under the load of 100 g, which was applied for 15 s at three different positions, each was 1 mm apart, and the mean was calculated.Samples were immersed in 1% citric acid (20 ml demineralizing solution) and stored in an incubator at 35°C temperature for 72 h for demineralization. After demineralization, once again, surface microhardness was calculated using the Vickers hardness indenter.
The samples of Group B, Group C and Group D were treated with prepared dentifrices slurries, i.e., Group B with sodium fluoride dentifrice slurry (Amflor™ toothpaste, Group pharmaceuticals) Group C with Calcium sodium phosphosilicate bioactiveglass dentifrices (Novamin) and Group D with Hydroxyapatite dentifrices( Aclaim) using same protocol, that is, 3 min, daily twice for 7 days. The samples were kept in artificial saliva (ICPA, Mumbai, Maharashtra, India) in between treatment. After the t reatment , the enamel surface microhardness in all three groups evaluated with the help of Vickers hardness indenter and a comparative
Kushani Shah et. al. : COMPARATIVE EVALUATION OF AMINE FLUORIDE, CALCIUM SODIUM PHOSPHOSILICATE (NOVAMIN), NANO HYDROXY APATITE CONTAINING DENTRIFICES ON ENAMEL MICROHARDNESS: AN IN VITRO STUDY
66

Vickers hardness values of the samples obtained at the baseline were in the range of 310.40- 328.30 VHN. After demineralization, mean microhardness in Group A decreased to 253.70 VHN, in Group B 274.80 VHN, in Group C 263.80 VHN and in Group D 301.40. After remineralization, mean microhardness in Group B increased to 307.50 VHN ,Group C increased to 316.00 VHN. And Group D increased to 329.80 VHN.
analysis done. Statistical analysis of surface microhardness obtained at different stages done by Student's t-test and P < 0.05 was considered statistically significant.
Kushani Shah et. al. : COMPARATIVE EVALUATION OF AMINE FLUORIDE, CALCIUM SODIUM PHOSPHOSILICATE (NOVAMIN), NANO HYDROXY APATITE CONTAINING DENTRIFICES ON ENAMEL MICROHARDNESS: AN IN VITRO STUDY
67

340
310
280
2501 2 3
GROUP AGROUP BGROUP CGROUP D
1. BASELINE 2. AFTER DEMINERALIZATION 3. AFTER REMINERALIZATION
DISCUSSION Ear ly enamel ca r ies can histologically be described as a subsurface carious lesion of enamel. Prominent feature being a subsurface demineralized zone with intact and unscathed enamel surface. Even though surface is intact, the mineral content is deficient. Hence, there is a lower microhardness of early enamel caries as
15opposed to sound enamel. The battle to keep teeth strong and healthy is dependent upon the ratio between demineralization and remineralization. It i s o b s e r v e d t h a t t h e b a l a n c e b e t w e e n demineralization and remineralization influences dental caries initiation and reversal.
This balance is dependent on factors such as presence of calcium, phosphate, and fluoride in
10saliva, as well as pH of saliva.
During demineralization, Ca2+, OH−, PO42−, F−, CO3−, Na+ and Mg2+ get displaced from the enamel surface to the exterior. More the acidic environment, greater is the outward flow of ions. However, mineral content of surface is higher than
15the body of the lesion. The demineralization process can be stopped by creating an environment conducive for remineralization by various remineralizing agents. The process of restoring lost mineral ions to the tooth structure and strengthening
16the lattice work is known as remineralization. Remineralization of enamel occurs when the
14alkaline pH increases.
Different fluoride combinations may show different results in prevention of caries. Dentifrices and mouthwashes are very popular in the world. The use of dentifrices as therapeutic agents is well accepted
17in dentistry. Chaudhary et al. in their study observed that dentifrices can help enamel against erosion and caries by increasing the enamel
21microhardness with remineralizing effect.
Here we have used amine fluoride which is organic fluoride which has showed promising results in
studies done by Sh et al. who has evaluated effect of amine fluoride and sodium fluoride mouthwashes on enamel microhardness and they concluded that amine fluoride increased enamel microhardness
22more than sodium fluoride. Galuscan et al. in their study observed that amine fluoride helps to promote the remineralization of initial lesions by releasing high quantities of fluoride molecules during the
23acid attack.
Chronic exposure to low levels of fluoride can cause gastrointestinal, urogenital, and respiratory problems in normal individuals. On the other hand, the prevalence of dental fluorosis has increased noticeably in non-fluoridated areas and to a lesser extent in optimally fluoridated areas. Moreover, fluoride ions alone cannot completely remineralize carious lesions. Formation of each fluorapatite molecule requires calcium and phosphate in addition to fluoride ions. Thus, it is imperative to find an efficient, safe alternative to fluoride to completely prevent caries and remineralize the
27incipient enamel lesions.
NovaMin comes in contact with saliva or any aqueous media, its active ingredient, inorganic chemical calcium sodium phosphor silicate, binds to the tooth surface in order to initiate the remineralization process on the tooth enamel. This is performed by providing silica, calcium, phosphorous and sodium ions to the tooth
11-12structure.
Synthetic NHA has the same physicochemical properties as those of apatite in the enamel. It shows strong affinity to the tooth and can strongly adsorb on enamel surfaces. nanoHA has the potential to directly fill up defects and micropores on demineralized teeth. Once, nano-HA penetrates the enamel pores, nano-HA will act as a template in the precipitation process and will continuously attract a large amount of Ca2+ and PO3− 4 to the enamel surface to fill the vacant positions of the enamel calcium crystals. This in turn will promote crystal integrity and growth.
White et al. in their study evaluated different methods for enamel demineralization and remineralization such as direct methods and indirect methods. In the present study, indirect method, i.e., microhardness measurement method is used because it can measure changes in the physical parameters such as surface structural
Kushani Shah et. al. : COMPARATIVE EVALUATION OF AMINE FLUORIDE, CALCIUM SODIUM PHOSPHOSILICATE (NOVAMIN), NANO HYDROXY APATITE CONTAINING DENTRIFICES ON ENAMEL MICROHARDNESS: AN IN VITRO STUDY
68

strength, and also it is simple, fast and least destructive method to determine demineralization
18-19and remineralization.
There are different types of microhardness tests which include Knoop, Vickers, and Brinnel. Darshan and Shashikiran in their study observed that even small changes can be detected easily, by the square shape indent obtained after Vickers hardness test. Hence, in the current study, Vickers hardness test was selected for investigation over
20Knoop and Brinnel test.
The results of the current study showed significant increase in mean microhardness after Nano hydroxyapatite (Aclaim) remineralization than amine sodium fluoride (Amflor) remineralization and Calcium sodium phosphosilicate glass (Novamin) and it was statistically significant. These results are in accordance with study done in 2007 by K. OHTA et al who has observed that mineral density to demineralized surface can be increased by treatment with nano HAP. In 2013 Shreya S et al observed HAP showed definite potential as an effective remineralizing agent when compared to p o t a s s i u m n i t r a t e a n d s o d i u m
25monofluorophosphate.
In these study significant increase in mean microhardness was greater in novamin group as compared to the fluoride group. These results are in accordance with study done in In 2012 M. Vahid et al in their study observed that NovaMin dentifrice
appears to have a greater effect on remineralization of carious-like lesions when compared to that of fluoride containing dentifrice in permanent teeth.24 in 2010 sharma N et al has observed that Comparison of the potassium nitrate and stannous fluoride formulations, the dentifrice containing NovaMin provided more substantial and significant
28improvements in enamel microhardness.
CONCLUSION:
Demineralization of the tooth is a condition that is affected by diet, bacteria and limited use of protective agents found in fluoride, salivary buffers and an t imic rob ia l agen t s . Wi th c l ea re r understanding of the implementation of these effective agents and new technologies accessible to dentists, we can create a more favorable relationship in which remineralization occurs more often than demineralization.
Under the limitation of this study we can conclude that NOVAMIN (calcium sodium phosphosilicate bioactive glass.) and aclaim tooth paste (Nano hydroxyapatite crystals) were more effective in restoring enamel microhardness than fluoride contaiong tooth paste (Amflor). And between NOVAMIN (calcium sodium phosphosilicate bioactive glass.) and aclaim tooth paste (Nano hydroxyapatite crystals) aclaims tootpaste shows more effctive results.
REFERENCES:
1. Patil N, Choudhari S, Kulkarni S, Joshi SR. Comparative evaluation of remineralizing potential of three agents on artificially demineralized human enamel: An in vitro study. J Conserv Dent 2013;16:116-20.
2. Lata S, Varghese NO, Varughese JM. Remineralization potential of fluoride and amorphous calcium phosphate-casein phospho peptide on enamel lesions: An in vitro comparative evaluation. J Conserv Dent 2010;13:42-6.
3. Muhlemann HR, Schmid H, Konig KG. Enamel solubility reduction studies with inorganic and organic fluoride. Helv odontol Acta 1957;1:233-7.
4. Buchalla W, Attin T, Schulte-Mönting J, Hellwig E: Fluoride uptake, retention, and remineralization efficacy of a highly concentrated fluoride solution
on enamel lesions in situ. J Dent Res 81 (2002), 329–333.
5. Sargod SS, Bhat SS, Hegde S, Karunakaran R. Remineralization potential using calcium sucrose phosphate (EnaFix) on artificial carious lesion: A polaroid microscopic study. Indian J Appl Res 2015;5:421-3.
6. La Torre G, Greenspan DC. The role of ionic release from Novamin (Calcium Sodium Phosphocilicate) in yubule occlusion: an exploratory invitro study using radio-labeled isotopes. J Clin Dent. 2010;21(3):72-6.
7. Burwell A, Jennings D, Muscle D, Greenspan DC. NovaMin and dentine hypersensitivity-invitro evidence of efficacy. J Clin Dent. 2010;21(3):66-71.
8. Cochrane NJ, Saranathan S, Cai F, Cross Kj,
Kushani Shah et. al. : COMPARATIVE EVALUATION OF AMINE FLUORIDE, CALCIUM SODIUM PHOSPHOSILICATE (NOVAMIN), NANO HYDROXY APATITE CONTAINING DENTRIFICES ON ENAMEL MICROHARDNESS: AN IN VITRO STUDY
69

Reynolds EC. Enamel subsurface lesion remineralization with casein phosphopeptide stabilized solution of calcium, phosphate and fluoride. Caries Res. 2008;42(2):88-97.
9. Random Sampling and Randomization Procedures; 2009. Available from: Aoba T. Solubility properties of human tooth mineral and h t t p : / / w w w. i s o . o r g / i s o / i s o _ c a t a l o g u e / catalogue_tc/catalogue_detail.htm?csnumber=42039. [Last cited on 2015 Sep 08].
10. Aoba T. Solubility properties of human tooth mineral and pathogenesis of dental caries. Oral dis 2004;10:249-57
11. Manton DJ, Walker GD, Cai F, Cochrane NJ, Shen P, Reynolds EC. Remineralization of enamel subsurface lesions in situ by the use of three commercially available sugar-free gums. Int J Paediatr Dent. 2008 Jul;18(4):284-90.
12. Lata S, Varghese NO, Varoughese JM. Remineralization potential of fluoride and a m o r p h o u s c a l c i u m p h o s p h a t e - c a s e i n phosphopeptide on enamel lesions. An invitro comparative evaluation. J Conserv Dent. 2010 Jan;13(1):42-6.
13. Ten Cate JM. Fluorides in caries prevention and control: Empiricism or science. Caries Res 2004;38:254-7.
14. Arnold WH, Haase A, Hacklaender J, Gintner Z, Bánóczy J, Gaengler P. Effect of pH of amine fluoride containing toothpastes on enamel remineralization in vitro. BMC Oral Health 2007;7:14
15. Lata S, Varghese NO, Varughese JM. Remineralization potential of fluoride and amorphous calcium phosphate-casein phospho peptide on enamel lesions: An in vitro comparative evaluation. J Conserv Dent 2010;13:42-6
16. Pradeep K, rao PK. Remineralizing agents in thnoninvasive treatment of early carious lesions. Int J Dent case 2011;2:73-84
17. Zero DT. Dentifrices, mouthwashes, and remineralization/caries arrestment strategies. BMC Oral Health 2006;6 Suppl 1:S9
18. White DJ, Fal ler RV, Bowman WD. Demineralization and remineralization evaluation techniques – Added considerations. J Dent Res 1992;71:929-33
19. Jabbarifar SE, Salavati S, Akhavan A, Khosravi K, Tavakoli N, Nilchian F. Effect of fluoridated dentifrices on surface microhardness of the enamel of deciduous teeth. Dent Res J (Isfahan) 2011;8:113-7
20. Darshan HE, Shashikiran ND. The effect of McInnes solution on enamel and the effect of tooth mousse on bleached enamel: An in vitro study. J Conserv Dent 2008;11:86-91.
21. Chaudhary A, Ingle NA, Kaur N, Rahul G. Effect of fluoridated dentifrices on microhardness of enamel surface: In vitro study. J Adv Oral Res 2013;4:11-6.
22. Sh P, Raghu R, Shetty A, Gautham P, Reddy S, Srinivasan R. Effect of organic versus inorganic fluoride on enamel microhardness: An in vitro study. J Conserv Dent 2013;16:203-7
23. Galuscan A, Podariu AC, Jumanca D. The decreasing of carious index by using toothpaste based on amine fluoride. Oral Health Dent Man Black Sea countries 2003;1:42-6
24. M. Vahid Golpayegani1~, A. Sohrabi2, M. Biria1,3, G. Ansari. Remineralization Effect of Topical NovaMin Versus Sodium Fluoride (1.1%) on Caries-Like Lesions in Permanent Teeth. Journal of Dentistry, Tehran University of Medical Sciences, Tehran, Iran (2012; Vol. 9, No.1)
25. Shreya S, Ramesh K, Ramreddy Y, Karunakar S (2013) Comparative Evaluation of Hydroxyapatite, P o t a s s i u m N i t r a t e a n d S o d i u m Monofluorophosphate as in Office Desensitising Agents–A Double Blinded Randomized Controlled Clinical Trial. Oral Hyg Health 1: 104
26. Silverstone L.M.Remineralization Phenomena. Caries Res. 1977: 11 (Suppl 1): 59-84
27. Haghgoo R, Mehran M, Ahmadvand M, Ahmadvand MJ. Remineralization effect of eggshell versus nano-hydroxyapatite on caries-like lesions in permanent teeth (in vitro). J Int Oral Health 2016;8(4):435-439
28. Sharma N, Roy S, Kakar A, Greenspan DC, Scott R A clinical study comparing oral formulations containing 7.5% calcium sodium phosphosilicate (NovaMin), 5% potassium nitrate, and 0.4% stannous fluoride for the management of dentin hypersensitivity. The Journal of Clinical Dentistry [01 Jan 2010, 21(3):88-92].
Kushani Shah et. al. : COMPARATIVE EVALUATION OF AMINE FLUORIDE, CALCIUM SODIUM PHOSPHOSILICATE (NOVAMIN), NANO HYDROXY APATITE CONTAINING DENTRIFICES ON ENAMEL MICROHARDNESS: AN IN VITRO STUDY
70

SINGLE ROOTED NATURAL PREMOLARS
DECORONATED CROWNS
DEMARCATION LINE FOR DECORONATION
MESIO-DISTAL SECTION OF CROWN
Kushani Shah et. al. : COMPARATIVE EVALUATION OF AMINE FLUORIDE, CALCIUM SODIUM PHOSPHOSILICATE (NOVAMIN), NANO HYDROXY APATITE CONTAINING DENTRIFICES ON ENAMEL MICROHARDNESS: AN IN VITRO STUDY
71

SAMPLE EMBEDDED ACRYLIC BLOCKS SAMPLES IMMESED IN 1%CITRIC ACID
MICROHARDNESS TESTING 4 GROUPS
Kushani Shah et. al. : COMPARATIVE EVALUATION OF AMINE FLUORIDE, CALCIUM SODIUM PHOSPHOSILICATE (NOVAMIN), NANO HYDROXY APATITE CONTAINING DENTRIFICES ON ENAMEL MICROHARDNESS: AN IN VITRO STUDY
72

SAMPLES EMBEDDED IN THE REMINERALIZING SOLUTION
ARTIFICIAL SALIVA
Kushani Shah et. al. : COMPARATIVE EVALUATION OF AMINE FLUORIDE, CALCIUM SODIUM PHOSPHOSILICATE (NOVAMIN), NANO HYDROXY APATITE CONTAINING DENTRIFICES ON ENAMEL MICROHARDNESS: AN IN VITRO STUDY
73

ABSTRACT
Introduction: The success of root canal treatment is mainly based on the complete eradication of microorganisms by instrumentation and disinfection protocols followed during the procedure. Due to anatomical complexities like lateral canals, achieving long term success would be difficult because these areas have limited access to instruments and irrigants. Hence, application of intracanal medicament has been considered as an important step to reduce the persistent bacterial load inside the root canal. Since the routine intracanal solutions have the limited time for action so gels were used in the study to increase the time of action and reduce the bacterial load. Aims and Objectives: To evaluate antibacterial efficacy of various gel formulations when used as an intracanal medicament in primary molars. Material and Method: Carious primary molars with adequate coronal tooth structure were selected and randomly allotted to 4 different groups- 2% Metronidazole gel (Positive control), 2% Chlorhexidine gel, 2% Povidone-iodine gel and no medication group (Negative control).Selected tooth was anaesthetized and isolated using rubber dam. Access opening was done and canals were negotiated and biomechanical preparation was done using K-files upto #35 with frequent irrigation in between with normal saline. Pre-operative sample was taken using a paper point (#30) and was transported to lab in vial containing brain-heart infusion broth. Intracanal medicament was placed using a syringe in all the canals. Cotton pellet was placed on top of it and temporary restoration was placed. Bacterial culture of the sample was done on blood agar and colony forming units were counted. Patients were recalled after 3 days and second sample was taken immediately after removing the temporary restoration and cotton pellet using paper points and was sent for culture. Root canals were irrigated, obturated and teeth were restored with permanent restorative material. Results: Percentage reduction of colony forming units was calculated. Results were obtained and statistical analysis was performed using one-way ANOVA and Tukey's post-hoc test. Betadine group showed the best result among all four groups. Conclusion: On comparing the mean of pre-operative and post-operative CFUs, it was concluded that metronidazole, betadine and chlorhexidine showed a significant difference while no medication group showed non-significant difference.
Keywords: Intracanal medicament, gels, pulpectomy
Received: 04-05-2017; Review Completed: 16-08-2017; Accepted: 30-01-2018
Vrunda Parikh*, Dharati Patel**, Hinal Thakkar***, Bhumi Sarvaiya ****, Krunal Chokshi *****
74
EVALUATION OF ANTIBACTERIAL EFFICACY OF VARIOUS GEL FORMULATIONS WHEN USED AS AN INTRACANAL MEDICAMENT IN PRIMARY MOLARS – AN IN VIVO STUDY
*PG Student, **PG Student, *** PG Student, ****Reader, *****Sr Lecturer
ADDRESS FOR AUTHOR CORROSPONDENCE : DR. VRUNDA PARIKH, TEL: +91 9714964499
DEPARTMENT OF PEDODONTICS AND PREVENTIVE DENTISTRY, AHMEDABAD DENTAL COLLEGE AND HOSPITAL
Original Article
INTRODUCTION:
Achieving predictable long-term success of root canal treatment requires effective debridement and disinfection of the root canal system.1 Chemico-mechanical instrumentation removes the majority of infecting bacteria, together with necrotic pulp
2debris. However, this is not always achieved completely because of anatomical complexity and the limitation in accessing the canal system by instruments and irrigants. The remaining bacteria may multiply during the period between appointments, often reaching the same level that it was at the start of the previous session, in cases where the canal is not dressed with a disinfectant
3between visits. Residual bacteria in obturated
4canals may be denied access to nutrients and die , or they may survive and ultimately proliferate. Persistent endodontic infection may be attributed to the retention of microorganisms in dentinal
5tubules. Inter-appointment intracanal medication
has been unequivocally shown to contribute to favourable outcomes when treating endodontic infections. It was observed that when no intracanal medicament was used between the appointments pathogenic microorganisms increased in number, so the need for intracanal medicaments seems to be
6apparent.
Two percent chlorhexidine gluconate has been used as an irrigant and intracanal medicament in endodontics. Chlorhexidine is a bis-biguanide that acts by adsorbing onto the cel l wal l of microorganisms resulting in leakage of intracellular components. Chlorhexidine has a broad spectrum antimicrobial activity, targeting both gram-positive
7and gram-negative microbes and is biocompatible. Metronidazole is a nitroimidazole compound that exhibits a broad spectrum of activity against protozoa and anaerobic bacteria. Metronidazole readily permeates bacterial cell membranes and

binds to DNA, disrupting its helical structure and leads to very rapid cell death. It has been shown to have excellent activity against anaerobes isolated from odontogenic abscesses but has no activity against aerobes.8 Povidone-iodine which is used widely as a topical agent, is an iodophore in which iodine is linked to povidone, a dextran-like molecule. Povidone-iodine appears to be active against all microorganisms, including gram-positive and gram-negative, spores, mycobacteria,
9fungi, viruses and protozoa.
Root canals in primary teeth relatively very thin and ribbon shaped, with large number of lateral canals. So, placing a gel based intracanal medicament will increase the duration of action of the drug by producing a sustained-release type of action. Hence, this study is aimed to assess the efficacy of chlorhexidine gel, metronidazole gel and povidone-iodine gel as asintracanal medicament against E. faecalis in endodontically infected human primary molars.
Materials and Methods
80 patients with necrotic or infected pulp as diagnosed clinically and radiographically who had come to the O. P. D. of Department of Pedodontics and Preventive Dentistry and who required endodontic treatment for the same. Ethical approval was obtained from ethical committee of Ahmedabad Dental College and Hospital.
Inclusion criteria
• Patient with non-contributary medical history
• Tooth without any previous restoration
• Tooth with infected or with necrotic pulp as diagnosed clinically or radiographically
• Tooth with 2/3rd root length
• Tooth with adequate coronal structure for proper isolation, temporarization and restoration
Exclusion criteria
• Patient with any systemic condition
• Patient with acute periapical abscess
• Retreatment cases
Study Design
Written consent was obtained from parents of all the participants after explaining the intention of the study. Participants with carious primary molars
with adequate coronal tooth structure were selected and randomly allotted to 4 different groups.
Group I: 2% Metronidazole gel (Positive control)
Group II: 2% Chlorhexidine gel
Group III: 2% Betadine gel
Group IV: No medication placed (Negative control)
Selected tooth was anaesthetized and isolated using rubber dam. Access opening was done and canals were negotiated. Working length was obtained and confirmed by using a radiograph. Biomechanical preparation was done using K-files upto #35 with frequent irrigation in between with normal saline. Pre-operative sample was then taken using paper points (#30) and were placed in a vial containing brain-heart infusion broth and was transported to the laboratory. 0.1 ml of randomly chosen intracanal medicament was placed in each canal. Cotton pellet was placed on top of it and temporary restoration was placed on top of the cotton pellet.
Bacterial culture
Chocolate agar plates were pre-dried in an incubator for 15-30 minutes and inoculated by streaking. A sterile wire loop of 0.01 ml was dipped into vial containing the sample and was used to inoculate on chocolate agar. Then streaking was carried out. The same procedure was done for all
samples. The plates were then incubated at 37 C̊ for 24 hours and number of colony forming units (CFU) were counted in each sample.
Post-operative sample
Patient were recalled after 3 days and post-operative sample was taken using paper points (#30), immediately after removing temporary restoration and cotton pellet. The sample was sent to the laboratory in vials containing brain-heart infusion broth and were cultured in similar manner. The number of colony forming units in post-operative sample were counted.
After taking the post-operative sample, root canals were irrigated, dried and obturated using suitable obturating material. All the teeth were then restored with stainless steel crowns.
Antibacterial efficacy
Percentage reduction of colony forming units was calculated and results were obtained.
Vrunda Parikh et. al. : EVALUATION OF ANTIBACTERIAL EFFICACY OF VARIOUS GEL FORMULATIONS WHEN USED AS AN INTRACANAL MEDICAMENT IN PRIMARY MOLARS – AN IN VIVO STUDY
75

Antibacterial efficacy = (CFU preop*-CFU postop**)
CFU preopx 100
Figure 1: Sample collection
Figure 3: Placing sample in Brain Heart Infusion Broth
*CFU preop = CFU in pre-operative sample
**CFU postop = CFU in post-operative sample
Statistical analysis
The data was analysed by SPSS 20.0 software using one way analysis of variance (ANOVA), Students paired “t” test and Tukey's (P < 0.05) test. Since there are four groups, the ANOVA was used to find the significance, the multiple comparison test and pair wise comparison was done using the TUKEY post hoc test. Students paired “t” test was used for a comparison of mean between two samples of four groups.
Figure 2: Medication placement
Figure 4: E. faecalisgrowth seen on Chocolate Agar
76
Vrunda Parikh et. al. : EVALUATION OF ANTIBACTERIAL EFFICACY OF VARIOUS GEL FORMULATIONS WHEN USED AS AN INTRACANAL MEDICAMENT IN PRIMARY MOLARS – AN IN VIVO STUDY

Results:
The results obtained after evaluating the antibacterial efcacy between all four groups – Metronidazole, Chlorhexidine, Betadine and No medication are shown table I and chart I.
77
Vrunda Parikh et. al. : EVALUATION OF ANTIBACTERIAL EFFICACY OF VARIOUS GEL FORMULATIONS WHEN USED AS AN INTRACANAL MEDICAMENT IN PRIMARY MOLARS – AN IN VIVO STUDY

78
Vrunda Parikh et. al. : EVALUATION OF ANTIBACTERIAL EFFICACY OF VARIOUS GEL FORMULATIONS WHEN USED AS AN INTRACANAL MEDICAMENT IN PRIMARY MOLARS – AN IN VIVO STUDY

The results showed that the percentage reduction in bacterial count was highest in betadine group and was lowest in no medication group. One way ANOVA test was applied for the comparison of mean of each group. The value was found to be p <0.001, which was statistically significant. On comparing the mean of pre-operative and post-o p e r a t i v e C F U s , i t w a s o b s e r v e d t h a t metronidazole, betadine and chlorhexidine showed a significant difference while no medication showed non-significant difference. In intergroup comparison, it was seen that all the three medicament showed significant difference when compared with no medication group. However, there was no significant difference when the medication groups were compared with each other.
DiscussionIn the current study, 80 abscessed primary
molars were selected which required two visit pulpectomy. Literature suggests two visit pulpectomy for abscessed cases as it provides sufficient time for the abscess to drain. The inter-appointment gap was kept to be three days as it is the usual amount of time taken by most of the practitioners and it also provides enough time for the intracanal medicament to act.
In the present study, all the pulpectomies were carried under rubber dam isolation so as to have a properly isolated field. Ahmad IA in an article in 2005 suggested that failure to use rubber dam has been shown to influence the choice of root canal irrigant, has a negative impact on treatment outcome and places the patient at risk of swallowing
10or aspirating materials and instruments.E. faecalisis one of most common micro-
organism which causes failure of endodontic treatment. Hancock HH and colleagues performed a study in 2001 to determine the composition of the microbial flora present in teeth after the failure of root canal therapy in North American population and concluded that out of the total sample almost 30% of the teeth had a positive culture for E.
11faecalis. In the present study, the only irrigant that was used was normal saline as it has minimal antibacterial properties. Use of any other endodontic irrigant would have caused a bias as it would have its own bacteriocidal properties which
would alter the original results. All the three medicaments that were used were in gel form to increase the retaintivity of the medication. Bhangadia MB and colleagues in a study in 2014 compared the efficacy of metronidazole gel versus metronidazole solution against E. faecalis in
12abscessed primary molars. The results of the study concluded that metronidazole gel was more effective metronidazole solution against E.faecalis.
2% chlorhexidine gel was found to be 87.17% effective while 2% metronidazole was found to 92% effective and 2% betadine was found to be 97.25% effective against in this E. faecalisstudy which is in contrast to a study done by Krithidatta J and colleagues in 2007 in which they concluded that 2% chlorhexidine gel was 100% effective while 2% metronidazole gel was 86.5% effective against Efficacy of betadine 13E. faecalis.was compared with commonly used intracanal medicament to justify its use for a two visit pulpectomy. In a study done by Kandaswamy D and associates in 2010 antimicrobial activity of 2% chlorhexidine gel, propolis, juice, Morindacitrifolia2% povidone-iodine and calcium hydroxide on E. faecalis was investigated and the results showed that 2% chlorhexidine was 100% effective while 2% povidone iodine was 87% effective followed by propolis (71%), juice (69%) and Morindacitrifoliacalcium hydroxide (55%).14
Sterile paper points were used to take sample from the root canals of the selected teeth as they could reach the complete length of the canal and absorb enough fluid from the canals for culture.
Pre-sterilised sealed vials of brain heart infusion broth were used as transport medium as it allows growth of and can also be used Enterococcias a culture medium for the same if no other medium is available. The time lapse after the placement of sample in broth would not alter the count of Enterococci.
Chocolate agar was used as a culture medium for . In a study done by Gunn BA E. faecalisin 1984, he concluded that chocolate agar can be used as a differential medium for gram-positive cocci including streptococci, staphylococci and enterococci.5
79
Vrunda Parikh et. al. : EVALUATION OF ANTIBACTERIAL EFFICACY OF VARIOUS GEL FORMULATIONS WHEN USED AS AN INTRACANAL MEDICAMENT IN PRIMARY MOLARS – AN IN VIVO STUDY

ConclusionIntracanal medicaments and their use in permament teeth has been widely demonstrated and studied, but its use and efficacy in primary teeth has not been properly evaluated. Metronidazole, chlorhexidine and betadine have been used as irrigants for decades but using them in gel form would increase its substantivity and retaintivity. In this study, it was found that the bacterial count reduced upto 97.25% in betadine group followed by metronidazole group (92%) and chlorhexidine group (87.17%). The percentage reduction in count in no E. faecalismedication group was only 20% inspite of all patients being on systemic medication which makes it all the more necessary to use an inter-appointment
medicament in case of abscessed molars.Betadine group showed highest percentage reduction of CFUs among all the four groups.No medication group showed the least percentage reduction of CFUs of On comparing the mean of pre-E. faecalis.operative and post-operative CFUs, it was observed that metronidazole, betadine and chlorhexidine showed a significant difference while no medication group showed non-significant difference.In intergroup comparison, it was seen that all the three medicament showed significant difference when compared with no medication group.However, evidence for the medicaments is still insufficient for primary teeth. Further similar multicentric studies need to be carried out.
REFERENCES:
1. Lee Y, Han SH, Hong SH, Lee JK, Ji H, Kum KY. Ant imicrobial eff icacy of a polymeric chlorhexidine release device using in vitro model of Enterococcus faecalis dentinal tubule infection. J Endod. 2008;34(7):855-8.
2. Manzur A, Gonzalez AM, Pozos A, Herzog DS, Friernam S. Bacterial quantification in teeth with apical periodontitis related to instrumentation and different intracanal medications: a randomized clinical trial. J Endod. 2007;33(2):66-70
3. Bystorm A, Sundqvist G. Bacterial evaluation of the e ff icacy of mechanica l root canal instrumentation in endodontic therapy. Scand J Dent Res. 1981;89(4):321-8.
4. Peters LB, Wesenlink PR, Moorer WR. The fate and role of bacteria left in root dentinal tubules. IntEndod J. 1995;28(2):95-9.
5. Safavi KE, Spanberg SW, Langeland K. Root canal dentinal tubule disinfection. J Endod. 1990;16(5):207-10.
6. Sjogren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. IntEndod J. 1997;30(5):297-306.
7. Yesiloy C, Whitaker E, Cleveland D, Phillips E, Trope M. Antimicrobial and toxic effects of established and potential root canal irrigants. J Endod. 1995;21(10):513-5.
8. Roche Y, Yoshimori RN. In vitro activity of spiramycin and metronidazole alone or in
combination against clinical isolates from odontogenic abscesses. J AntimicrobChemother. 1997;40(3):353-77.
9. Cherry M, Daly CG, Mitchell D. Effect of rinsing with povidone iodine on bacteraemia due to scaling: a randomized controlled trial. J ClinPerio. 2007;34(2):148-55.
10. Ahmad IA. Rubber dam usage for endodontic t r e a t m e n t : a r e v i e w . I n t E n d o d J . 2009;42(11):963-72
11. Hancock HH, Sigurdsson A, Trope M, Moiseiwitsch J. Bacteria isolated after unsuccessful endodontic treatment in North American population. Oral Surg Oral Med Oral Pathol Oral RadiolEndod. 2001;91(5).579-86.
12. Bhangadia MB, Nandlal B, Vijaykumar GS, Kulkarni PK, Shanbhog R. Clinical evaluation of sustained-release metronidazole gel versus metronidazole solution as an intracanal medicament in abscessed primary molars. Eur Arch Paediatr Dent. 2014;15(1):19-26.
13. Krithikadatta J, Indira R, Dorothykalyani AL. Disinfection of dentinal tubules with 2% chlorhexidine, 2% metronidazole, bioactive glass when compared with calcium hydroxide as i n t r a c a n a l m e d i c a m e n t s . J E n d o d . 2007;33(12):1473-6.
14. Kandaswamy D, Venkateshbabu N, Gogulnath D, Kindo AJ. Dentinal tubule disinfection with 2% chlorhexidine gel, propolis, morindacitrifolia juice, 2% povidone iodine, and calcium hydroxide. IntEndod J. 2010;43(5): 419–23.
80
Vrunda Parikh et. al. : EVALUATION OF ANTIBACTERIAL EFFICACY OF VARIOUS GEL FORMULATIONS WHEN USED AS AN INTRACANAL MEDICAMENT IN PRIMARY MOLARS – AN IN VIVO STUDY

ABSTRACT
Introduction: Gynecologist and Pediatricians are the first to observe any dental disease in the child as they are usually approached by the parents for any illness. Many pediatric oral diseases are preventable if they are recognized and preventive care is encouraged and refer to the pediatric dentist whenever necessary. The lack of parental education in the prenatal period and the neglect of oral health care in infancy can have deleterious effect as during this period foundation of permanent dentition is laid. Hence appropriate knowledge of gynecologist and pediatricians regarding infant oral health care can lead to early diagnosis, timely referral and proper management of the same. Aim: To evaluate the knowledge, attitude, awareness and practices regarding infant oral health care among gynecologist and pediatricians in Ahmedabad city regarding. Materials and Method: A cross sectional survey was undertaken among 140 gynecologist and pediatricians of Ahmedabad city. A self-administered questionnaire was personally handed over to the gynecologist and the pediatricians and collected on the same day. The data was collected and statistically analyzed. Results: The study revealed that majority of gynecologist and pediatricians need to have more knowledge regarding infant oral health care. Conclusion: As health care professionals, responsible for the overall health of children, knowledge regarding oral health is important for both gynecologist and pediatricians so that they could early diagnose and refer these patients to the pedodontist in order to avoid further spread of the disease and prevent its future complications.
Keywords: Infant oral health care, knowledge, awareness, gynecologist, pediatricians.
Received: 05-04-2017; Review Completed: 23-08-2017; Accepted: 25-01-2018
Birva Patel*, Kinjal Engineer**, Vasudha Sodani ***, Rajal Pathak****
81
KNOWLEDGE, ATTITUDE AND AWARENESS REGARDING INFANT ORAL HEALTH CARE AMONG GYNECOLOGIST AND PEDIATRICIANS
*PG Student, **PG Student, *** Reader, ****Reader
ADDRESS FOR AUTHOR CORROSPONDENCE : DR. BIRVA PATEL, TEL: +91 9825100530
DEPARTMENT OF PEDODONTICS AND PREVENTIVE DENTISTRY, AHMEDABAD DENTAL COLLEGE AND HOSPITAL
Original Article
INTRODUCTION:
Oral health is considered to be a vital part of general health and since decades, the outlook to treat oral disease has been, correcting the destruction and then start prevention. So, for good oral health guidelines recommend to put more emphasis on early professional intervention and primary
1prevention.
Although the AAPD calls for every child to have a dental visit by the time the first primary tooth erupts and to have access to preventive dental care throughout childhood, the reality is different,
2especially for children in low-income families. Gynecologistsand Pediatricians are the first to observe any dental disease in the child as they are
3usually approached by the parents for any illness. Many pediatric oral diseases are preventable if they recognize and encourage preventive care and refer patients to pediatric dentist whenever necessary. Unfortunately, medical professional's knowledge and inclination to practice preventive dentistry has been shown to be lacking. In fact, the incidence of permanent tooth dental caries has declined consistently over the last three decades than that of the primary tooth caries. So, it remains to be seen
whether the medical community can effect the change in that pattern.
Hence appropriate knowledge of gynecologists and pediatricians regarding infant oral health care can lead to early diagnosis, timely referral and proper management of the same.
MATERIALS AND METHOD
A cross sectional survey was undertaken among 140 gynecologist and pediatricians of Ahmedabad city through random sampling. A self-administered questionnaire was personally handed over to all of them and collected on the same day. It comprised a series of questions pertaining to personal and

demographic characteristics and infant oral health care. The data was collected and statistically analyzed.
RESULTS
The scores obtained were stored in an excel spread sheet (Microsoft, Inc., Redmond, Wash) and statistical analysis was carried out using statistical package for social sciences (SPSS). Pearson's Chi Square test was used.
95.7% of the practitioners were aware of, the first baby tooth appears the child's mouth at the age of 6 month. 74.3% of the practitioners didn't know that tooth decay is caused by bacteria that is transmitted by sharing utensils. 60% reported that disease of primary teeth can affect the permanent teeth. 31.4% of the practitioners didn't know that bacteria that cause tooth decay get transmitted from mother to child. Most of the practitioners (54.3%) were aware about the ill effects of prolonged breast feeding/bottle feeding on oral health of infants. Half of the practitioners (54.3%) knew that health of the kid's mouth effects its appearance in future. Only 37.1% of practitionars knew that oral health of the mother influences the infants oral health.
97.1% of the practitioners knew that brushing your baby's teeth is important for oral health. 60% of the practitioners believed that parents should take their baby to dentist as soon as first tooth erupts for preventive dental health examination and 61.4% agree that effective cleaning of teeth can be achieved by 3-4 years old child. 51.4% of them disagreed that infants mouth prior to tooth eruption, needs to be clean. Most of them agreed that parents should be educated to reduce the frequency of sucrose consumption by their child, especially in between meals.
Birva Patel et. al. : KNOWLEDGE, ATTITUDE AND AWARENESS REGARDING INFANT ORAL HEALTH CARE AMONG GYNECOLOGIST AND PEDIATRICIANS
82

Majority (92.9%) of them agreed that balance diet is essential for the healthy growth of a baby's teeth. and 57.1% disagreed with weaning from a baby bottle to a sipping cup should be plan when the baby is 6-month-old. 61.4% disagreed that night time bottle/at will breast feeding can cause tooth decay. 62.9% of the practitioners agreed that child's teeth should be cleaned as soon as the teeth erupts and 67.1% reported that fluoride in tooth paste is important for preventing tooth decay.
Birva Patel et. al. : KNOWLEDGE, ATTITUDE AND AWARENESS REGARDING INFANT ORAL HEALTH CARE AMONG GYNECOLOGIST AND PEDIATRICIANS
83

REFERENCES:
1. General Accounting Office. Oral health: dental disease is a chronic problem among low-income populations. Available at: url: http:// www.gao.gov. Accessed on May 19, 2010.
2. American Academy of Pediatric Dentistry reference manual 2009-2010. Pediatr Dent 2009; 31:1-302.
3. U S p r e v e n t i v e s e r v i c e s t a s k f o r c e recommendation. Am J Prev Med 2004; 26:326-9.
4. American academy of pediatric dentistry clinical affairs committee. American academy on pediatric dentistry counsil on clinical affairs. Guideline on periodicity of examination, preventive dental services, anticipatory guidance/counseling and oral treatment for infants, children and adolescents. Pediatr Dent 2008-2009; 30 suppl 7:112-8.
5. Marcelo B, Jenny A, Gustavo T and Luciana O. Impact of dental caries on preschool children's quality of life: an update.Braz Oral Res 2012;26(1):103-7.
6. Faizal C, Kottayi S, Vaibhav K. Knowledge, Attitude and Practices of Pediatricians regarding prevention of Dental Caries. Health Scie 2013;2(2):1-10.
7. Sham S, sundeep K, Vidya S, Chinchu M. Knowledge, Attitude and Practices among Pediatricians on early childhood caries and infant oral health care in Mangaluru. Ind J Appli Res 2016;6(6):368-71.
8. MD Indira et al. Knowledge, Attitude and Practice toward Infant Oral Healthcare among the Pediatricians of Mysore: A Questionnaire survey. Int J clin Ped dent 2015;8(3):211-4.
9. Seema Lochib, KR Indushekar, Bhavna G, Neha SH, Divesh S. Knowledge, Attitude and Practices of Pediatricians in Faridabad towards infant oral health care. Univ res j dent 2014;4(2):97-100.
10. Feldens CA, Rodrigues PH, Gislaine A, Marcia R, Benjamin W. Feeding frequency in infancy and dental caries in childhood: a prospective cohort study. Int Dent J 2017.
11. Murthy GA, Mohandas U. The Knowledge, Attitude and Practice in Prevention of Dental Caries amongst Pediatricians in Banglore: A cross – Sectional study. J Indian Soc Pedod Prevent Dent 2010;2(28):100-3.
12. Damle SG et al. Transmission of mutans streptococci in mother-child pairs. Indian J Med Res 2016;144(2):264-70.
Birva Patel et. al. : KNOWLEDGE, ATTITUDE AND AWARENESS REGARDING INFANT ORAL HEALTH CARE AMONG GYNECOLOGIST AND PEDIATRICIANS
84

RIDGE EXPANSION AND IMMEDIATE IMPLANT PLACEMENT IN POSTERIOR MANDIBLE: A CASE REPORT
Savan Chovatia*, Hitesh Solanki**, Sachin Modi***, Sachin Dalal****
85
ADDRESS FOR AUTHOR CORROSPONDENCE : DR. SAVAN CHOVATIA, TEL: +91 9510733357
ABSTRACT
Endosseous dental implants may require bone augmentation before implant placement. Herein is described an approach to edentulous ridge expansion with the use of oscillating saw and immediate placement of implants. This may allow for a shortened treatment time and the elimination of donor-site morbidity. One case with single edentulous posterior region is reported. This technique uses an oscillating saw to cut the crestal and proximal facial cortices. Space is then created with osteotomes to widen the split ridge. This technique allows for expansion of narrow, anatomically limiting, atrophic ridges, creating space for immediate implant placement. The facial and lingual cortices provide support with vital osteocytes for osteogenesis. The implants were restored to a functional and esthetic outcome.
Keywords: Dental implant, Horizontal ridge augmentation, Ridge split, Ridge expansion
Received: 03-05-2017; Review Completed: 11-09-2017; Accepted: 26-12-2017
*PG Student, **PG Student, ***Sr Lecturer, ****Professor
A Case Report
DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY AHMEDABAD DENTAL COLLEGE AND HOSPITAL
INTRODUCTION:
Edentul ism is an incapaci ta t ing and i r r e t r i evab le cond i t i on wh ich can l ead unswervingly to functional limitation, physical, psychological and social handicap. Maintenance of bone after tooth loss to improve retention, function, and performance of the restoration is a challenging task. The existence of a thin edentulous ridge signies a clinical situation that is more complex for the placement of endosseous implants. Dental rehabilitation of the edentulous ridges with oral implants has become a routine treatment modality in the last few decades with consistent long term
1results.
One of the most common condi t ions encountered in implant dentistry is the presence of decient bone quantity to allow for the appropriate implant placement according to standard protocols. The atrophic edentulous ridges present an inimitable challenge to the implant surgeon. It has come to light that for a completely functional and esthetic restoration, a comprehensive hard and soft tissue harmony has to be achieved before and after implant placement. The present perspective is to
1place an implant in a prosthetically driven position.
Various techniques for augmentation of the ridges have been addressed in the past which includes: onlay bone grafts harvested from the hip, maxillary tuberosity, symphysis of the chin, mandibular ramus and external oblique ridge. All these methods have their own shortcomings, the most important being the inevitability of a second
surgical site for procuring the graft. Hence various alternative procedures were developed to minimize this morbidity. Splitting and expanding the edentulous ridge for bone augmentation and implant placement is considered as an innovative technique as it avoids the need for a second surgical site which further reduces the ailment of the
1patient.
This ridge split technique was developed by 2 3Simionet al. and Scipioni et al. in the early 1990s. 2
Simion et al. aimed at creating a ''self-space making defect'' by splitting the atrophic crests in two parts with a longitudinal greenstick fracture displacing the vestibular cortical bone both in maxilla or mandible to create a gap, which was used to contain the inserted implants. The maxillary bone owing to the thinner cortical plates and softer medullary bone compared to that of the mandible is a good candidate for performing a ridge spilt procedure. In this procedure, the corticotomies can be performed using variousinstruments like beaver blade, razor-sharp chisel, round bur, ssure bur, diamond disk, reciprocal saw, piezoelectric device, or laser (erbium: yttrium–aluminumgarnet, erbium, chromium-doped: yttrium-scandium-gallium-
4garnet.
This case report throws light on the use of a consistent technique for horizontal ridge augmentation namely the oscillating saw assisted ridge splitting followed by successful implant placement with subsequent prosthetic rehabilitation in the mandibular posterior edentulous area.

CASE REPORT
The present case report is about a 23 year old female patient reported with chief complaint was missing teeth in lower right region of the jaw. She requested fixed prosthesis, preferably an implant-supported one. The medical/social and family history was noncontributory. Patient gave history of caries associated with lower right mandibular first molar which had been extracted three years ago.
Intra oral clinical examination revealed that the patient had missing lower right mandibular first molar (Figure 1). There was decient ridge width Cone beam computed tomography was performed to evaluate the bone quality and quantity. Pre-operative CBCT images revealed a horizontal ridge width of about 3.3mm and vertical height of 16.3
Figure 1. Pre-operative atrophic edentulous ridge in relation to mandibular right first mo.
Figure 2. Pre-operative CBCT showing deficient horizontal bone.
mm in relation to right lower first molar (Figure 2). CBCT revealed inadequate buccolingual dimension of bone at the crest for implant placement. There was adequate cortical and cancellous bone to allow ridge expansion.
The treatment plan was decided to perform ridge splitting for horizontal ridge augmentation and Implant placement in relation to mandibular right first molar. The facial painting was done with providone iodine and draping was done. The surgical site was anesthetized using 2 % lignocaine HCl with adrenaline (1:80,000). A mid-crestal incision was given in the region of the molar and a vertical releasing incision was placed anteriorly to reect a full thickness mucoperiosteal ap (Figure 3). Periosteal releasing incisions were given in order to relieve the tension on the aps while suturing. The pre-operative horizontal ridge width measured was around 3 mm. A longitudinal mid-crestal osteotomy was performed using the oscillating saw in a side to side cutting motion. Two vertical bone incisions were made, one at the mesial and other at the distal aspect at least 2–3 mm from adjacent root (Figure 4). The osteotomy site was expanded usingosteotome. The osteotome is tapped and controlled lateral force should begin to be used to mobilize the buccal plate. (Figure 5). After the cortical plate had been separated a pilot drill 2.3 mm in diameter was used to prepare the osteotomy for the final length of the implant to be placed. A 3.75 mm diameter and 10 mm length implant was immediately placed within the bony envelope (Figure 6). The site was grafted with irradiated allogenic cortical particulates (Sybograf plus) (Figure 7). This was followed by the placement of collagen membrane in order to prevent the epithelial down growth and as a means to provide space for bone regeneration (Figure 8). After achieving primary closure of the aps the site was sutured tension free with interrupted sutures using vicryl 3-0 suture material (Figure 9). Post-operative instructions were given and the analgesics (combination of paracetamol-500 mg and diclofenac-50 mg thrice daily for 3 days) and antibiotics (amoxicillin 500 mg thrice daily for 5 days) were prescribed. Healing was uneventful and within normal limits.
Savan Chovatia et. al. : RIDGE EXPANSION AND IMMEDIATE IMPLANT PLACEMENT IN POSTERIOR MANDIBLE: A CASE REPORT
86

Figure 3. Minimal flap reflection to maintain periosteal attachment in apicalregion.
Figure 4. One horizontal and two vertical cuts are made on buccal plate with oscillating saw.
Figure 7. Bone graft placed in the gap between the implant and buccal plate.
Figure 8. Collagen membrane is placed over the implant and bone graft.
Savan Chovatia et. al. : RIDGE EXPANSION AND IMMEDIATE IMPLANT PLACEMENT IN POSTERIOR MANDIBLE: A CASE REPORT
87

Figure 11. Definitive PFM prosthesis.
Figure 12. Final prosthesis.
The implants were allowed to osseointegrate for 4 months after which the site was exposed to place the healing caps to obtain the soft tissue contour around them. After 15 days the nal impression was made followed by the placement of ceramic fused to metal xed implant supported prosthesis which was checked for its precise t(Figure 11,12). Patient was kept under regular follow-up with 3 months visit after placement of nal prosthesis. The nal radiograph taken after a period of 10 months showed no signicant bone loss around the implant (Figure 14).
Figure 13. Post op radiograph after 4 months of implant placement.
Savan Chovatia et. al. : RIDGE EXPANSION AND IMMEDIATE IMPLANT PLACEMENT IN POSTERIOR MANDIBLE: A CASE REPORT
88

Figure 14. Post op radiograph after 10 months shows minimal crestal resorption.
DISCUSSION
Bone loss is an ongoing process following tooth loss affecting the mandible four times more than the
5maxilla. The loss of tooth structure causes impaired mastication, functional and sensory deciencies of the oral mucosa, musculature and salivary glands. Apart from this it also affects the general health and
6quality of life of the patient. Hence accurate restoration of the lost tooth structure is of prime importance. The four main surgical approaches for the augmentation of atrophic ridges includes guided bone regeneration, bone grafting, expansion and distraction techniques and a combination of these
7methods.
Ridge split technique essentially reconstructs the alveolar bone by creating a green stick fracture which is a reliable and relatively non-invasive procedure. It principally consists of splitting the vestibular and buccal cortical tables while
7displacing the vestibular cortical bone. Simion et
2 3al. and Scipioni et al. introduced this technique by aiming at creating a self-space making defect with the help of chisels which prevented the membrane from collapsing into the defect from which the
2osteogenic cells can be recruited. The advantage of this ridge split technique is that the expansion created heals with rapid vascularization and bone remodeling in a manner similar to that occurring in
8fractures. But the limitation of this technique is its inability to create bone vertically and the pre-requisite that there should be cancellous bone present between the buccal and lingual plates to allow separation.
Significant advantages of ridge expansion rather than Onlay grafting include simultaneous implant placement and grafting, lower cost, lower possibility of cross-infection from graft materials and lower morbidity. This technique has greater predictability, since the grafted area is essentially a five-wall bony defect, with excellent blood supply. This technique is only suitable for enhancing ridge width. There must be adequate available bone height for implant placement, and no vertical bone defect should be present. A minimum of 3 mm of bone width, including at least 1 mm of cancellous bone is desired to insert a bone chisel between cortical plates and consequently expanding the cortical bones. The thinner cortical plates and softer medullary bone make the maxillary ridge easier to expand. The risk of malfracture of the osteotomized segment is high in the mandible due to thicker
10cortical plates.
Several modifications of the ridge splitting technique have been described. Ridge splitting is accomplished either with the use of osteotomes and chisels, or with the use of special equipment such as burs, micro-saws and horizontal spreaders. Compared to the osteotome technique, the use of spreaders provides better control of the amount of the expansion achieved, prevents excessive forces
11, 12, 13and patient discomfort produced by malleting. On the other hand, the osteotome technique eliminates the need for special equipment. Strong evidence for the effectiveness and the predictability of the ridge splitting technique is available in the literature. Clinical trials have reported success rates ranging from 98 to 100%. The survival rates of implants immediately placed in expanded sites ranged from 91% to 97.3%, while the success rates
3, 6, 14, 15, 16varied from 86.2% to 98.8%. Complications during the surgical procedure are very rare - fracture of the buccal bone plate being reported as a major complication of the technique49. Controlled force application and gradual expansion could prevent
4 , 1 1 malfractures . In addi t ion, a thorough preoperative evaluation is very important. The thickness of the cortical plates and the amount of the intervening cancellous bone must be carefully assessed preoperatively by dental CT scans. Last but not least, fabrication of radiographic/surgical guide can prevent improper implant placement and angulation.
Savan Chovatia et. al. : RIDGE EXPANSION AND IMMEDIATE IMPLANT PLACEMENT IN POSTERIOR MANDIBLE: A CASE REPORT
89

REFERENCES:
1. B. Tarun Kumar, M. G. Triveni, V. Priyadharshini, D. S. Mehta. Staged Ridge Split Procedure in the Management of Horizontal Ridge Deciency Utilizing Piezosurgery. J. Maxillofac. Oral Surg. 2015 DOI 10.1007/s12663-015-0790-5.
2. Simion M, Baldoni M, Zaffe D. Jawbone enlargement using immediate implant placement associated with a split-crest technique and guided tissue regeneration. Int J Periodontics Restor 1992. 12:462–473.
3. ScipioniA, Bruschi GB, Calesini G. The edentulous ridge expansion technique: a ve- year study. Int J Periodontics Restor 1994. 14:451–459.
4. Sohn DS, Lee HJ, Heo JU, Moon JW, Park IS, Romanos GE. Immediate and delayed lateral ridge expansion technique in the atrophic posterior mandibular ridge. J Oral MaxillofacSurg2010. 68:2283–2290.
5. Emami E, De Souza RF, Kabawat M, Feine JS (2013) The impact of edentulism on oral and general health. Int J Dent. doi: 10.1155/ 2013/498305.
6. Bravi F, Bruschi GB, Ferrini F (2007) A 10-year multicenter retrospective clinical study of 1,715 implants placed with the edentulous ridge expansion technique. Int J Periodontics Restor Dent 27:557–565 9.
7. Anitua E, Begon ˜a L, Orive G (2012) Controlled ridge expansion using a two-stage split-crest technique with ultrasonic bone surgery. Implant Dent 21:163–170.
8. Coatoam GW, Mariotti A (2003) The segmental
ridge-split procedure. J Periodontol 74:757–770.
9. Abadzhiev M (2009) Alternative sinus lift techniques—literature review. J Int Med Assoc Bulgaria 15:23–27. doi:10.5272/jimab. 1522009_23.
10. Hollinger J, Wong ME. The integrated processes of hard tissue regeneration with special emphasis on fracture healing. Oral Surg Oral Med Oral Pathol Oral RadiolEndod. 1996;82(6):594–606.
11. Siddiqui AA, Sosovicka M. Lateral bone condensing and expansion for placement of endosseous dental implants: a new technique. J Oral Implantol, 2006; 32(2):87-94. 44.
12. Nishioka RS, Souza FA. Bone spreader technique: a preliminary 3-year study. J Oral Implantol, 2009; 35:289-294.
13. Peñarrocha M, Pérez H, Garciá A, Guarinos J. Benign paroxysmal posi t ional ver t igo as a complication of osteotome expansion of the maxillary alveolar ridge. J Oral MaxillofacSurg, 2001; 59:106-107.
14. Sethi A, Kaus T. Maxillary ridge expansion with simultaneous implant placement: 5-year results of an ongoing clinical study. Int J Oral Maxillofac Implants, 2000; 15:491-499.
15. Engelke WG, Diederichs CG, Jacobs HG, Deckwer I. Alveolar reconstruction with splitting osteotomy and microfixation of implants. Int J Oral Maxillofac Implants, 1997; 12:310-318.
16. Chiapasco M, Ferrini F, Casentini P, Accardi S, Zaniboni M. Dental implants placed in expanded narrow edentulous ridges with the Extension Crest device. A 1-3-yearmulticenter follow-up study. Clin Oral Implants Res, 2006; 17(3):265-272.
The grafting procedure done in the present case is an interpositional or ''sandwich'' grafting which is based on the theory that bone placed between 2 pieces of pedicled bone with internal cancellous bone will undergo rapid and complete healing and
8graft incorporation. In the present case there was excellent bone formation after 4 months re-entry into the grafted site with no complications.
CONCLUSION
In this report, there was 3-4 mm of bone crestally, which did not allow implant placement with conventional technique. There was sufficient trabecular bone with cortical bone on either side. This was an ideal case for ridge splitting with bone expansion.
Learning Points
1. Use of ridge splitting technique offers great advantage of placing dental implant at same surgical appointment in ≥3 mm of bone width
2. Bone expansion allows condensation of softer bone quality to more condensed variety apical and lateral to prepared osteotomy
3. Since no drilling is required to prepare implant osteotomy. It prevents loss of patient bone associated with drilling
4. Bone expansion also helps to reduce any labial undercutand allows more favorable axial loading
5. Combined flap on labial side maintains integrity of labial bone by preserving intact periosteum over cortical bone.
Savan Chovatia et. al. : RIDGE EXPANSION AND IMMEDIATE IMPLANT PLACEMENT IN POSTERIOR MANDIBLE: A CASE REPORT
90

MANAGEMENT OF BUCCALLY PLACED CANINES USING T-LOOP – A CASE REPORT
Priyanka Shah*, Sonali Mahadevia**, Bhavya Trivedi***, Aatman joshipura ****
91
ADDRESS FOR AUTHOR CORROSPONDENCE : DR. PRIYANKA SHAH , TEL: +91 9712144042
ABSTRACT
Ectopic eruption of canine or buccally placed canine is frequently found in general population. Cause can be genetic or environmental. Diagnosis and timely management of highly placed canine is must by orthodontist. This article is about a case of 12 year old male patient with buccally placed permanent maxillary canines bilaterally. Extraction is carried out for managing severe crowding and get canines into the arch. Extrusion and retraction of canine is done by segmental T-loop on both sides in maxilla.
Received: 22-02-2017; Review Completed: 30-08-2017; Accepted: 19-01-2018
*PG Student, **Head of the Department, ***Professor, ****Reader
A Case Report
DEPARTMENT ORTHODONTICS AND DENTOFACIAL ORTHOPEDICS DEPARTMENT, AHMEDABAD DENTAL COLLEGE AND HOSPITAL.
INTRODUCTION:
Canine being a corner tooth of arch plays an important role esthetically as well functionally. Ectopic buccal eruption of maxillary canine is one of the most frequently encountered condition in orthodontics.
The prevalence of maxillary permanent canine impaction or ectopic eruption in general population
1,2is 1-2%.
There is wide range of systemic and local etiology for such ectopic eruption. Also environmental factor may affect during long and tortuous course of canine eruption path.
Canine impactions are found to occur in families, suggesting a genetic or familial pattern of
3inheritance. Peck and peck suggested it to be a multi-factorial genetic inheritance.
CASE REPORT
DIAGNOSIS
A 12 year old male patient came with chief complain of irregularity in upper front teeth. After clinical examination it was found that maxillary canines were buccally placed bilaterally with class II molar relation on both sides. Also crowding was present in lower arch with a midline shift of 2mm on left side. Overjet of 3mm and overbite of 5mm was seen. No mandibular shift was noted on closure. No relevant medical history was found. Radiographic examination showed class I skeletal pattern and horizontal growth pattern.
TREATMENT OBJECTIVES AND PLAN
Treatment objectives were to achieve well aligned upper and lower arches with class I molar and canine relation, to obtain normal overjet and overbite with ideal incisor inclination. To get buccally placed maxillary canines into arch extraction of upper first premolars was planned on
Figure 1: (a)Pre-treatment Extra-oral photos
Figure 1: (b)Pre-treatment Intra-oral photos

both sides and in lower arch extraction of second premolars bilaterally was decided for relieving crowding and midline shift correction.
TREATMENT PROGRESS
Treatment plan includes extraction of 14, 24, 35 & 45. Treatment was started with extraction of upper first premolars. Both upper first molars were banded and canines were bonded. Segmental T-loop for extrusion and retraction of both right and left canines was given. Patient was recalled after every 5 weeks for follow up. After achieving canine in arch fixed appliance treatment was initiated in both upper and lower arches.
Full arch upper and lower bonding was done using 0.022” slot edgewise bracket. Lower second premolars were extracted bilaterally to relieve crowding and correct molar relation. Thus leveling and alignment of both arches is done.
DISCUSSION
After extraction space closure is done either by sliding mechanics or frictionless mechanics i.e with loop.
Various loops are used for retraction purpose like T-loop, opus loop, tear drop shape loop, etc. Loop mechanics is friction free and thus by maintaining
Figure 2: Segmental T-loop
Figure 3: Post T-loop result
Figure 4: Intra-oral photographs after alignment of canine
moment to force ratio we can get pure translation movement of tooth.
T-loop was given by Charles Burstone in 1962. It can be used for segmental tooth retraction or en-masse retraction during space closure. Desired tooth movement can be achieved by changing position of loop or changing preactivation bends. Desired movement is achieved by controlling moment to force ratio.
T-loop is constructed using 0.017” x 0.025” Titanium molybdenum alloy (TMA) wire. Advantage of TMA over stainless steel are low modulus of elasticity, low force and high range of action. T-loop with standard dimensions was made
4with pre activation bend.
CONCLUSION
T-loop is versatile loop which can be used for differential anchorage control for various tooth movement like segmental retraction, en-masse retraction, extrusion or intrusion. Sometimes it requires multidisciplinary approach. If proper diagnosis and biomechanics is used, the goal is not difficult to achieve.
REFERENCES:
1. Bedoya MM, Park JH. A review of the diagnosis and management of impacted maxillary canines. The Journal of the American Dental Association. 2009 Dec 31;140(12):1485-93.
2. Fleming PS, Scott P, Heidari N, DiBiase AT. Influence of radiographic position of ectopic canines on the duration of orthodontic treatment. The Angle orthodontist. 2009 May;79(3):442-6.
3. Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. The Angle orthodontist. 1994 Aug;64(4):250-6.
4. Kuhlberg AJ, Burstone CJ. T-loop position and anchorage control. American journal of orthodontics and dentofacial orthopedics. 1997 Jul 31;112(1):12-8.
Pryanka Shah et. al. : MANAGEMENT OF BUCCALLY PLACED CANINES USING T-LOOP – A CASE REPORT
92

PROSTHETIC REHABILITATION OF THE MAXILLARY DEFECT WITH HOLLOW BULB DEFINITIVE OBTURATOR: - A CASE REPORTHarshkumar Shah*, Mehul Patel**, Darshana Shah***, Chirag Chauhan****, Paras Doshi*****
93
ADDRESS FOR AUTHOR CORROSPONDENCE : DR. HARSHKUMAR SHAH, TEL: +91 9712137652
ABSTRACT
The presence of a large palatal or maxillary defect after partial or total maxillectomy for tumor, trauma or congenital deformation poses a challenge to prosthodontists. Diseases like carcinomas can cause significant effects on human beings like psychological, functional and surgical and can influence the overall quality of life. It is the responsibility of the Prosthodontist to restore the lost esthetics, function and speech. While we strive to achieve the above, it has to be borne in mind that the proposed prosthesis should be simple to handle, easy to maintain, biocompatible, light in weight and convenient for future adjustments. This clinical case report describes the rehabilitation of a patient with a maxillary defect using a single-piece hollow bulb obturator, replacing the missing teeth. For that primary and final impressions, jaw relation, articulation and mounting, teeth set up and curing of the hollow bulb obturator was done by lost salt technique.
Key Words: Definitive obturator, hollow bulb, single-piece, maxillectomy; maxillofacial defects; obturator.
Received: 08-06-2017; Review Completed: 23-08-2017; Accepted: 29-11-2017
*PG Student, **PG Student, ***Head of the Department, ****Professor
A Case Report
DEPARTMENT OF PROSTHODONTICS AND CROWN AND BRIDGE AHMEDABAD DENTAL COLLEGE AND HOSPITAL
INTRODUCTION:
Maxillofacial defects are caused by trauma, tumor or congenital deformations. Severe deficiencies in appearance, pronunciation and swallowing occur when maxillofacial defects cause oral–nasal
transport. These severe malfunctions may
1 ultimately result in psychological problems. Since the 1940s, prosthodontists have tried to help these patients by separating the oral and the nasal cavity using obturator prostheses to improve deglutition,
2 articulation, pronunciation and facial appearance. The absence of teeth, and the size and configuration of the maxillary defect, may influence the masticatory function of patients wearing an obturator prosthesis and may lead to a poor rehabilitation outcome. Restoring function, speech and esthetics is a challenging task when the defect presented is large. Treatment becomes even more difficult when the problem is associated with restricted mouth opening caused by radiation
3,4 therapy. The present article is a case report explaining the rehabilitation of a patient who had undergone partial maxillectomy of the left side maxilla.
Case Report
75 years old male patient reported to the department of prosthodontics in Ahmedabad dental college and hospital with the chief complaint of the difficulty in the chewing, drinking, deglutition and speaking.
Patient was relatively asymptomatic before 2 years
then he was experienced pain in upper left back teeth region and went to the civil hospital, Ahmedabad for the same. extraction of the 26 were done under local anesthesia. After 20 days of extraction he was experienced, water coming from the nose and he was diagnosed as the oro-antral fistula with osteomylitis in relation to upper left back region. He had undergone the partial maxillectomy surgery under general anesthesia before 2 years with the radiotherapy.
Examination
Intra oral examination revealed the class II Armani's maxillectomy defect. (Figure 1) With the present t e e t h a r e a s f o l l o w : 18,16,15,14,13,12,38,37,36,35,34,33,42,43,44,47,48. There were acrylic prostheses in relation to 34, 33,32,31,41,42,43,44.
Treatment Plan
A definitive obturator, replacing missing teeth would be fabricated, to restore patient's functional demand.
Procedure for Definitive Obturator
A maxillary defect was blocked using gauze pack, which was socked in betadine solution. Maxillary and mandibular primary impressions were taken with stock metal t ray using irreversible hydrocolloid (Zermack tropicalgin alginate powder) (Figure 2a & 2b). The maxillary and

mandibular primary models were fabricated by using the type III dental stone (apexion gold stone) (Figure 3a & 3b). The special tray was fabricated and the border moulding was done by low fusing green stick compound (DPI) (Figure 4). The final impression was taken with the help of light body elastomeric impression material (DPI photosil) (Figure 5). Pick up impression was taken with the help of irreversible impression material (Figure 6). The master model was prepared using type III dental stone (Figure 7). The permanent record base with occlusal wax rim was fabricated. The jaw relation was recorded and the articulation and mounting was done in mean value articulator. (Figure 8 & 9). Teeth set up was carried out by using acry pan teeth set and final trial was done. (Figure 10a & 10b). The routine wax up, flasking and dewaxing procedures were carried out (Figure 11 & 12). At the time of heat cure acrylic resin (Pyrex Fship) packing the salt was incorporated at the defect area to reduce the weight of the prosthesis. And short duration curing cycle was completed. After retrieval from the curing unit finishing and polishing was carried out. The salt was removed by making the escape hole over the bulb. (Figure 13a, 13b, 13c) The escape holes were closed with the help of cold cure acrylic resin. The occlusal adjustment was carried out and the final prosthesis was delivered to the patient. (Figure 14, 15, 16a &16b)
Discussion
With any size of palatal perforation, retention as it applies to conventional complete denture prosthesis is impossible. Therefore, the contours of the defect must be used to maximize the retention, stability
5and support. since the lateral portion of the obturator exhibits the greatest degree of movement, retention can be improved by appropriate obturator-
6 tissue contact superolaterally. Many authors have insisted that the obturator for a large defect should
7 be routinely made hollow to reduce the weight. Most clinicians agree that the obturator should be hollow and lightweight, but there is some controversy concerning whether the superior surface can be left open or should be closed. Clinicians who prefer the closed top concluded that if the obturator is left open, nasal secretions
8, 9, 10 accumulate leading to odor and added weight.
Conclusion
The patient with maxillectomy defect has greater problems in speech and mastication than the conventional maxillary removable partial or complete denture. Sound prosthodontic principles of using bony undercuts, achieving maximum tissue coverage without overextension, and placing the dentition in harmony with the functional tissues are paramount for prosthetic success when treating these patients.
References
1) Philip Worthington, Craniomaxillofacial rehabilitation in oncology patients. In: Branemark, Oliviera. Craniofacial Prostheses. Quintessence Publishing Co Inc: 1997. p 86. Bhat V. A close-up on obturators using magnets: Part II. J Indian Prosthodont Soc 2006; 6: 148-153.
2) Wang RR. Sectional prosthesis for total maxillectomy patients: a clinical report. J Prosthet Dent 1997; 78(3): 241–244.
3) Sato Y, Minagi S, Akagawa Y et al. An evaluation of chewing function of complete denture wearers. J Prosthet Dent 1989; 62(1): 50–53.
4) Koyama S, Sasaki K, Inai T et al. Effects of defect configuration, size, and remaining teeth on masticatory function in post-maxillectomy patients. J Oral Rehabil 2005; 32(9): 635–641.
5) Desjardins, R. P. Obturator prosthesis design for acquired maxillary defects. J Prosthet Dent 1978; 39: 424-435
6) Brown K. E. Peripheral consideration in improving obturator retention. J Prosthet Dent 1968; 20:176-181
7) Rhonda F. Jacob, Clinical management of the edentulous maxillectomy patient. In: Taylor TD. Clinical maxillofacial prosthetics. Quintessence Publishing Co Inc: 2000. p 100, 96, 102.
8) Chalian VA, Barnett MO. A new technique for constructing a one- piece hollow obturator after partial maxillectomy. J Prosthet Dent 1972; 28:448-53.
9) Varoujan A. Chalian, Joe B. Drane, and S. Miles Standish, Intraoral Prosthetics. In:
Harshkumar Shah et. al. : PROSTHETIC REHABILITATION OF THE MAXILLARY DEFECT WITH HOLLOW BULB DEFINITIVE OBTURATOR: - A CASE REPORT
94

Chal ian VA, Drane JB, Standish M. Maxillofacial Prosthetics: Multidisciplinary Practice. The Williams and Wilkins Co: 1971. p 133-48
10) Thomas A. Curtis and John Beumer III, Restoration of acquired hard palate defects: etiology, disability, and rehabilitation. In: Beumer, Curtis, Firtell. Maxillofacial rehabilitation: prosthodontic and surgical considerations. The C.V. Mosby Company: 1979. p 218.
Figure 1: Armani's class II maxillary defect.
Figure 2a: Maxillary primary impression.
Figure 2b: Mandibular primary impression.
Figure 3a: Maxillary primary cast.
Figure 3b: Mandibular primary cast.
Harshkumar Shah et. al. : PROSTHETIC REHABILITATION OF THE MAXILLARY DEFECT WITH HOLLOW BULB DEFINITIVE OBTURATOR: - A CASE REPORT
95

Figure 4: Maxillary border moulding.
Figure 5: Maxillary final impression.
Figure 6: Maxillary pick up impression with irreversible hydrocolloid.
Figure 7: Maxillary master cast.
Figure 8: Jaw relation record.
Harshkumar Shah et. al. : PROSTHETIC REHABILITATION OF THE MAXILLARY DEFECT WITH HOLLOW BULB DEFINITIVE OBTURATOR: - A CASE REPORT
96

Figure 9: Articulation and mounting on mean value articulator.
Figure 10a: Teeth set up on mean value articulator.
Figure 10b: Final trial.
Figure 11: Flasking procedure.
Figure 12: After dewaxing procedure.
Figure 13a: Maxillary obturator with hollow bulb.
Harshkumar Shah et. al. : PROSTHETIC REHABILITATION OF THE MAXILLARY DEFECT WITH HOLLOW BULB DEFINITIVE OBTURATOR: - A CASE REPORT
97

Figure 13b: Escape holes for salt removal.
Figure 13c
Figure 14: Maxillary obturator placed in patient's mouth.
Figure 15: After occlusal adjustment
Figure 16a: Before the treatment
Figure 16b: After the treatment
Harshkumar Shah et. al. : PROSTHETIC REHABILITATION OF THE MAXILLARY DEFECT WITH HOLLOW BULB DEFINITIVE OBTURATOR: - A CASE REPORT
98

VESTIBULAR INCISION SUBPERIOSTEAL TUNNEL ACCESS (VISTA) WITH PLATELET RICH FIBRIN (PRF) IN THE MANAGEMENT OF MULTIPLE GINGIVAL RECESSION: A CASE REPORTNakul Ameta*, **, Harit Shah***, Archita Kikani****Shikha Mavani
99
ADDRESS FOR AUTHOR CORROSPONDENCE : DR. NAKUL AMETA, TEL: +91 9773220467
ABSTRACT
Gingival recession is clinically manifested by an apical displacement of the gingival tissues, leading to root surface exposure. It is a concern for both patients and clinician for several reasons such as root hypersensitivity, erosion, root caries, and esthetics. Recently, new techniques have been suggested for the surgical treatment of multiple adjacent recession type defects. The current case series introduce a novel, minimally invasive approach applicable for both isolated recession defects as well as multiple contiguous defects in the maxillary anterior region. This case series describes the use of the vestibular incision subperiosteal tunnel access (VISTA) technique in combination with platelet-rich fibrin (PRF) membrane for treating multiple gingival recession defects.
Key Words: Platelet rich fibrin, gingival recession, vestibular incision subperiosteal tunnel access technique.(VISTA)
Received: 11-05-2017; Review Completed: 20-07-2017; Accepted: 05-12-2017
*PG Student,, **PG Student,, ***PG Student,, ****Professor
A Case Report
DEPARTMENT OF PERIODONTOLOGY AND ORAL IMPLANTOLOGY AHMEDABAD DENTAL COLLEGE AND HOSPITAL
INTRODUCTION:
Gingival recession is defined as apical migration of gingival margin beyond the cementoenamel
[1]junction (CEJ) . Patients with gingival recessions often seek treatment because of impaired aesthetics, increased sensitivity and fear of losing teeth. In the cases of multiple adjacent gingival recessions, patients request that treatment is done in a single stage. The surgical treatment of such recessions requires a larger volume of donor connective tissue. This tissue is taken from the palate which greatly increases the difficulty and the probability of complications throughout the surgery and even
[ 2 ]afterwards . In order to minimize these disadvantages, the method of GTR (guided tissue
[3]regeneration) with biodegradable and non-biodegradable membranes and biologically active substances such as acellular dermal matrix allograft (ADM), enamel matrix derivate (EMD), platelet-
[4] rich plasma (PRP), platelet-rich fibrin (PRF) and more.
The platelet-rich fibrin (PRF) was first introduced for the first time by Choukroun et al. in 2001 and is regarded as a second generation platelet concentrate. This autogenous biomaterial slowly releases growth factors which lasts for at least 7-28
[5-9]days .
Platelet rich fibrin (PRF) a second generation platelet concentrate, has been used extensively in combination with bone graft materials for periodontal regeneration, ridge augmentation, sinus lift procedures for implant placement and for
coverage of gingival recession defects in the form of [10].a membrane It has become a focus of current
studies because of its potential to accelerate healing.
What is also important is that the resulting from the patient clot contains no chemical or biological additives while it has a solid structure and can easily be used to prepare strong, elastic fibrin membrane. Many publications with promising results appeared in the past few years about the treatment of gingival recessions with PRF.
In 2011 Zadeh H H modified the tunnel technique offering the so-called VISTA (Vestibular Incision subperiosteal Tunnel Access) technique for the treatment of multiple adjacent gingival recessions in the front part of the maxilla. The purpose of this case report is to evaluate clinically, the efficacy of the novel and minimally invasive VISTA in combination with PRF in the treatment of gingival recession defects.
2. Materials and Methods:
The clinical study was conducted at the Department of Periodontology and Implantology in the month of February. A 37 year old female patient came with chief complain of sensitivity and unfair esthetics due to exposed roots. On examination there were multiple Miller's class 1 and 2 gingival recession in maxillary anterior teeth in first quadrant. The surgical treatment was done using the VISTA technique with PRF. The affected and treated teeth were maxillary central, lateral and canine in first quadrant. The results were monitored for three months postoperatively.
Nakul Ameta*, Krishna Doshi**, Harit Shah***, Archita Kikani****

2. Surgical Technique:
The VISTA technique is essentially a modification of the double-layer tunneling technique that requires a single incision serving in the creation of the subperiosteal tunnel flap and an opening for the graft. Our modified technique is as follows: after the application of adequate local anesthesia, the affected by the recession teeth are cleaned, smoothed and polished with machinery tools.
A vertical incision is made on the mucous membrane and the periosteum with a scalpel. The incision is 8-10mm long, beginning from the mobile mucosa and reaching the apical end of the keratinized gingiva – Figure 1a. A small subperiosteal elevator is inserted through the incision and is used to free the subperiosteal tunnel flap. The flap includes the tissues of the mobile and immobile mucosa in the area of the affected teeth and about 1 cm distally and medially from them. A scalpel is used to make intrasulcular incisions covering up to a third of the papilla width medially and distally.
Pre-operative view
Figure 1a
Instruments for tunneling plastic are used through the vertical incision to free the mucosa and the periosteum around the affected by the gingival recessions teeth. This is continues at the base of the gingival papillae without affecting their entirety. The mucosa and the periosteum, below adjacent unaffected teeth laterally and medially from the affected ones, are freed using the method described below – Figure 2 a-b
The previously prepared platelet-rich fibrin membranes --Figure 3 a are inserted through the entrance vertical incision – Figure 3 b. With a ½ needle and biodegradable thread 0000 the vertical incision is stitched.
Figure 2 a
Figure 2 b
Nakul Ameta et. al. : VESTIBULAR INCISION SUBPERIOSTEAL TUNNEL ACCESS (VISTA) WITH PLATELET RICH FIBRIN (PRF) IN THE MANAGEMENT OF MULTIPLE GINGIVAL RECESSION: A CASE REPORT
100

Figure 3 a
Figure 3 b
Single horizontal sutures are made 2-3 millimeters below the gingival margin in the area of the affected teeth. They are knotted in a way that the knots can be fixed to the coronary surface of the corresponding tooth – Figure 3 b. The place where the knots (sutures) are fixed is defined in advance by the affected teeth and the occlusion type. The knots are fixed to the vestibular or lingual tooth surfaces with light curing liquid composite resin
Post operative 3 months follow up
Postoperative Care: Postoperatively patient was assigned therapy with NSAIDs for 3 days and mouth rinsing with 0,12% solution of chlorhexidine one minute three times a day for 14 days. The application of cold compresses in the surgery area and mushy-liquid diet for the first seven days were recommended. Checkup examination was done on the first day after the surgery, and the threads were removed on the 14th day after. Patient was given instructions about the technique of personal hygiene and to avoid brushing the treated teeth for the next 14 days.
3. Results: The results demonstrated 100% root coverage in this case at 3 month.
4. Discussion: Earlier periodontal therapy was limited to eliminate and to avoid disease by maintenance of a functional healthy dentition and supporting hard and soft tissues. However, more recently periodontal therapy is increasingly directed at esthetic outcomes for patients. Patients have become more conscious of dental esthetics and are demanding precision treatment for exposed root
[11]surfaces
In order to minimize the surgical procedures and optimize the aesthetic results all adjacent gingival recessions should be treated in a single treatment stage. This can be achieved by making use of different surgical techniques, but most commonly different modifications of the tunneling technique are used. One important feature that makes the VISTA technique stand out of the rest is the difference in the approach used in the formation of the tunnel flap. In the VISTA technique there is a wide dissection of the soft tissues in order to eliminate possible pull. This allows for a maximal move of the tissues over the cementoenamel junction (CEJ) while the stitching technique effectively prevents possible apical movement of the marginal gingiva during the initial healing period. The elimination of the pull on the gingival tissues is essential in achieving good final results when treating gingival recessions. Preserving the entirety of the interdental papillae by avoiding their dissection ensures stability and fine local blood supply to the soft tissues. The stable fixation of the gingival tissues accounts for the lowering of their micro movement during the healing stage which is a great step ahead of the other techniques. In this study we use platelet-rich fibrin membrane in
Nakul Ameta et. al. : VESTIBULAR INCISION SUBPERIOSTEAL TUNNEL ACCESS (VISTA) WITH PLATELET RICH FIBRIN (PRF) IN THE MANAGEMENT OF MULTIPLE GINGIVAL RECESSION: A CASE REPORT
101

combination with the VISTA technique. The usage of this autogenous biological material eliminates completely the danger of adverse reactions to foreign (non-autogenous) materials. We used PRF membrane prepared in our own way from two A-PRF clots. The forming of the PRF membrane using our method aims to increase the concentration and the distribution of the platelets and leukocytes in the final membrane.
5. Conclusions
Based on the results from this clinical study we can conclude that the VISTA technique in combination with platelet-rich fibrin membrane can successfully be used as a treatment method for multiple gingival recessions of Miller's Class I and Class II. Additional clinical studies with a longer monitoring period and larger number of patients are need for better assessment of the VISTA technique with PRF for the treatment of these recessions.
REFERENCES
1. Chambrone L, Sukekava F, Araujo MG, Pustiglioni FE, Chambrone LA, Lima LA. Root coverage procedures for the treatment of localised recession-type defects. Cochrane Database Syst Rev. 2009; (2):CD007161.
2. Dridi SM,Chousterman M,Danan M,Gaudy JF. Heamorrhagic risk when harvesting palatal connective tissue grafts: a reality? J Perio.2008; 5(4):231-240
3. Tinti C, Vincenzi G. The treatment of gingival recession with guided tissue regeneration procedure by means of Gore-Tex membranes. (La regenerazione guidata dei tessuti con Gore-Tex: nuove prospettive?) Quintessence Int. 1990;6: 465-468.(45-49).
4. Anilkumar K, Geetha A, Umasudhakar et al.Platelet-rich fibrin:A novel root coverage approach.Journal of Indian Society of Periodontology 2009; 13 (1), 50-54.
5. Choukroun J, Adda F, Schoeffer C, Vervelle A. PRF: an opportunityin perio-implantology (in French). Implantodontie 2001; 42:55- 62.
6. Dohan DM, Choukroun J, Diss A, et al. Platelet-rich fibrin (PRF):a second-generation p l a t e l e t c o n c e n t r a t e : P a r t I . Technologicalconcepts and evolution. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:37-44.
7. Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJ, Mouhyi J, Gogly B. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part III: leucocyte activation: a new feature for platelet concentrates? Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:51-5.
8. Dohan Ehrenfest DM, Rasmusson L, Albrektsson T. Classification of platelet concentrates: from pure platelet-rich plasma (PPRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol 2009;27:158-67.
9. Dohan Ehrenfest DM, de Peppo GM, Doglioli P, Sammartino G. Slow release of growth factors and thrombospondin-1 in Choukroun's platelet-rich fibrin (PRF): a gold standard to achieve for all surgical platelet concentrates technologies. Growth Factors 2009;27:63-9
10. Dohan Ehrenfest DM. How to optimize the preparation of leukocyte-and platelet-rich fibrin (LPRF, Choukroun's technique) clots and membranes: Introducing the PRF Box. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010; 110:275-278.
11. Anilkumar K. platelet-rich-fibrin: A novel root coverage approach: case report JISP. 2009; 13:50-54.
Nakul Ameta et. al. : VESTIBULAR INCISION SUBPERIOSTEAL TUNNEL ACCESS (VISTA) WITH PLATELET RICH FIBRIN (PRF) IN THE MANAGEMENT OF MULTIPLE GINGIVAL RECESSION: A CASE REPORT
102

FRENECTOMY WITH LATERAL PEDICLE FLAP-A NOVEL FRENECTOMY TECHNIQUE FOR PREVENTION OF SCAR: A CASE REPORTShikha Mavani*, **, Harit Shah***, Archita Kikani****, Mihir Shah*****Nakul Ameta
103
ADDRESS FOR AUTHOR CORROSPONDENCE : DR. SHIKHA MAVANI, TEL: +91 9924461675
ABSTRACT
An aberrant frenum is postulated to create functional and aesthetic problems. Archer's 'classical frenectomy' is an extensive procedure including the excision of fibers, interdental papilla, and exposure of alveolar bone up to the palatine papilla. The resultant delayed healing, loss of interdental papilla, and abnormal scar led towards the conservative approaches like Edward's frenectomy, frenum relocation by Z-plasty and free gingival graft; with their technical and aesthetic limitations. A better approach to make a primary closure in midline and to avoid anesthetic scar by creating a zone of attached gingiva, frenectomy is assisted with lateral pedicle graft. The interdental papilla is left surgically undisturbed and healing takes place by primary intention. This article is a case report of frenectomy with laterally displaced flap.
Key Words: Aberrant frenum, frenectomy, lateral pedicle graft
Received: 21-06-2017; Review Completed: 13-09-2017; Accepted: 11-12-2017
*PG Student, **PG Student, ***PG Student, ****Professor
A Case Report
DEPARTMENT OF PERIODONTOLOGY AND ORAL IMPLANTOLOGY AHMEDABAD DENTAL COLLEGE AND HOSPITAL
INTRODUCTION:
A frenum is an anatomic structure formed by a fold of mucous membrane and connective tissue, sometimes muscle fibers. The superior labial frenum is triangular in shape and attaches the lip to the alveolar mucosa and/or gingiva. It extends over the alveolar process in infants and forms a raphe that reaches the palatal papilla. Through the growth of alveolar process as the teeth erupt, this attachment gene ra l ly changes to a s sume the adu l t
[1]configuration . Taylor has observed that a midline diastema is normal in about 98% children between six and seven years of age, but the incidence
.[2]decreases to only 7% in persons 12-18 yrs old
This high coronal attachment is generally associated with a hypertrophy of the frenum. Depending upon the extension of attachment of
[3]fibers, frena have been classified as:
1. Mucosal – when the frenal fibers are attached up to mucogingival junction;
2. Gingival – when fibers are inserted within attached gingiva;
3. Papillary – when fibers are extending into interdental papilla; and
4. Papilla penetrating – when the frenal fibers cross the alveolar process and extend up to palatine papilla.
Clinically, papillary and papilla penetrating frena are considered as pathological and have been found to be associated with loss of papilla,
recession, diastema, difficulty in brushing, alignment of teeth, and psychological disturbances to individual
.[4,5]
Abnormal or aberrant frena are detected visually by applying tension over it to see the movement of papillary tip or blanch produced due to ischemia of the region. Miller has
[6]
recommended that the frenum should be characterized as pathogenic when it is unusually wide or there is no apparent zone of attached gingiva along the midline or the interdental papilla shifts when the frenum is extended.
[7]
In such cases, it is necessary to perform a frenectomy for aesthetic, psychological, and functional reasons. There are numerous surgical techniques for the removal of labial frenum. In the “classical frenectomy” by Archer and
[8]
Kruger, the frenum, interdental tissue, and [9]
palatine papilla are completely excised leading to exposure of underlying alveolar bone and thus leading to scarring. Though this technique resulted into an anesthetic scar, but this approach was advocated to assure removal of muscle fibers, supposedly connecting the orbicularis oris with the palatine papilla. It was thought that if this was not done, the diastema would reopen.
Edwards method consisted of three procedures:[10]
1. Apically repositioning of the frenum (with denudation of alveolar bone),
Shikha Mavani*, Dipen Barot**, Harit Shah***, Archita Kikani****

2. Destruction of the trans-septal fibers between the approximating central incisors,
3. Gingivoplasty of any excess labial and/or palatal tissue in the interdental area.
One of the salient aspects of Edward's technique was the aesthetic maintenance of the interdental papilla. But the healed scar in the midline appeared anesthetic to the subjects.
Coleton and Lawrence have used free gingival [11] [12]
graft combined with frenectomy. This procedure avoids the scar, but a mismatched gingival color in midline and need of a second surgical site to achieve donor tissue complicate the technique.
Miller has presented a surgical technique combining the frenectomy with a laterally positioned pedicle graft. Closure across the midline by laterally positioned gingiva and healing by primary intention resulted in aesthetically acceptable attached gingiva across the midline. No attempt was made to dissect the trans-septal fibers and hence, interdental papi l la remained undisturbed. Aesthetically and functionally better results were obtained
MATERIALS AND METHODOLOGY :
A 19 year old female, referred from the department of orthodontics for frenectomy. The chief complaint was spacing between the front teeth. On general examination the patient was apparently healthy. On clinical examination, aberrant frenum was detected.It was found that patient had a type III frenal attachment. Tension test was positive and hence frenectomy procedure was planned. Written informed consent was obtained from the patient before the surgical procedure.
Figure 1: Preoperative view showing midline diastema and type III frenal attachment
Surgical Technique :
After local anesthesia, using 2% lignocaine with I;80000 adrenalin, primary incision was given at the base of the papilla and extended to the depth of vestibule to separate the frenum from underlying alveolar mucosa. Any remnant of frenal tissue in the mid line was excised. A vertical incision parallel to the primary incision was given on the mesial side of lateral incisor, 2-3mm apical to marginal gingiva, up to vestibular depth. The gingiva and alveolar mucosa in between these two incisions were undermined by partial dissection to raise the flap. A horizontal incision was made connecting the coronal ends of the two vertical incisions . Flap was raised, mobilized mesially and sutured to obtain primary closure with 4-0 vicryl interrupted suture across the midline. No attempt was made to dissect trans-septal fibers between approximating central incisors. Gingivoplasty of any excess labial and/or palatal tissue in the interdental area was done, preserving the integrity of the interdental papilla. The surgical area was dressed with COE PAK. Dressing and the sutures were removed one week later. A healing zone of attached gingiva was clearly visible with no loss of interdental papilla
Figure 2:Resected frenum site
Shikha Mavani et. al. : FRENECTOMY WITH LATERAL PEDICLE FLAP-A NOVEL FRENECTOMY TECHNIQUE FOR PREVENTION OF SCAR: A CASE REPORT
104

Figure 3:Vertical incision mesial to lateral incisor and undermining of the pedicle
Figure 4:Displacement and suturing of the pedicle at midline
Figure 5:Application of Coe –Pak
Post op care:
Patient was instructed not to have hot and spicy foods after the surgical procedure. Antibiotics and analgesics were prescribed for 3 days. Patient was advised to report for next appointment 1 week after surgery for review
Figure 6:post operative view at 1 week
Figure 7: post operative view at 1month
Figure 8:post operative view at 3 months
RESULTS
The outcome of this surgical procedure shows this technique produced a pleasing aesthetic result. Scar formation in the midline could be avoided. On healing, a wider zone of attached gingiva was obtained. It was color matched with adjacent tissue. Healing was obtained by primary intention. No loss of interdental papil la was observed. No complication was noted during healing period. Patient's compliance was also very good.
Shikha Mavani et. al. : FRENECTOMY WITH LATERAL PEDICLE FLAP-A NOVEL FRENECTOMY TECHNIQUE FOR PREVENTION OF SCAR: A CASE REPORT
105

Discussion
In the era of periodontal plastic surgery, more conservative and precise techniques are being adopted to create more functional and esthetic results. The technique for management of aberrant frenum has undergone changes from Archer's and 8
Kruger's “classical techniques” of total frenectomy 9
to Edward's10 more conservative approach. Recent techniques added frenal relocation by Z-plasty , 15
frenectomy with soft-tissue graft and Laser11, 12 13, 14
applications to avoid typical diamond shaped scar and facilitate healing. A frenum is evaluated in relation to vestibular depth, zone of attached gingiva, interdental papilla and diastema. A zone of attached gingiva is considered to prevent recession and it also gives an aesthetically pleasant appearance. Miller's technique combined with a laterally positioned pedicle graft was attempted in
7
this case. This technique offers two distinct advantages. First, on healing there is a continuous band of gingiva across the midline rather than
unesthetic scar. The second advantage is that trans-septal fibres are not disrupted surgically, to avoid any trauma to interdental papilla. This prevents loss of interdental papilla.
CONCLUSION
The present study describes the surgical technique combining frenectomy with a lateral pedicle graft. This method has certain distinct advantages e.g.-
1. Healing takes place by primary intention
2. A zone of attached gingiva, matching with adjacent tissue, forms in midline which is pleasing to the individual
3. No unesthetic scar formation
4. No recession of interdental papilla occurs because the transseptal fibers are not severed out
The attached gingiva in midline may have a bracing effect which helps in prevention of orthodontic relapse
REFERENCES
1. Henry SW, Levin MP, Tsaknis PJ. Histological features of superior labial frenum. J Periodontol. 1976;47:25–8.
2. Taylor JE. Clinical observation relating to the normal and abnormal frenum labii superioris. Am J Orthod Oral Surg. 1939;25:646.
3. Placek M, Miroslavs, Mrklas L. Significance of the labial frenal attachment in periodontal disease in man. Part 1; Classification and epidemiology of the labial frenum attachment. J Periodontol. 1974;45:891–4.
4. Dewel BF. The labial frenum, midline diastema and palatine papilla: A clinical analysis. Dent Clin North Am. 1966:175–84.
5. Díaz-Pizán ME, Lagravère MO, Villena R. Midline diastema and frenum morphology in the primary dentition. J Dent Child (Chic) 2006;26:11–4.
6. Gottsegen R. Frenum position and vestibule depth in relation to gingival health. Oral Surg. 1954;7:1069–72.
7. Miller PD., Jr The frenectomy combined with a laterally positioned pedicle graft; functional and aesthetic consideration. J Periodontol. 1985;56:102–6.
8. Archer WH, editor. 3rd ed. Philedelphia: W B Saunders Co; 1961. Oral surgery - a step by step atlas of operative techniques; p. 192.
9. Kruger GO, editor. 2nd ed. St. Louis: The C.V. Mosby Co; 1964. Oral surgery; p. 146.
10. Edwards JG. The diastema, the frenum, the frenectomy: A clinical study. Am J Ortho. 1977;71:489–508.
11. Colten SM. Mucogingival surgical procedures employed in re-establishing the integrity of the gingival unit (III): The frenectomy and the free m u c o s a l g r a f t . Q u i n t e s s e n c e I n t . 1977;8:53–61.
12. Lawrence GB, Fowler EB, Moore EA, Murray DJ. The free gingival graft combined with the frenectomy: A clinical review. Gen Dent. 1999;47:514–8.
13. Coluzzi DJ. Fundamentals of dental laser, science and instruments. Dent Clin North Am. 2004;48:751–70.
14. Gontizo F, Navarro RS, Haypek P, Ciamponi AL, Haddad AS. The application of diode and Er;YAG lasers in labial frenectomy in infant patients. J Dent Child. 2005;72:10–5.
15. Tait CH. Median frenum of upper lip and its influence on spacing of upper central incisor teeth. N Z Dent J. 1929;25:116.
Shikha Mavani et. al. : FRENECTOMY WITH LATERAL PEDICLE FLAP-A NOVEL FRENECTOMY TECHNIQUE FOR PREVENTION OF SCAR: A CASE REPORT
106

107
DEPARTMENT OF PERIODONTICS:Dr. Sarat ChandranDr. Neeraj DeshpandaDr. Vasumati Patel
DEPARTMENT OF CONSERVATIVE DENTISTRY:Dr. Sonali Kapoor
DEPARTMENT OF PROSTHODONTICS:Dr. Rajesh SeturamanDr. Saumil MathurDr. Keval Shah
DEPARTMENT OF ORAL MEDICINE & RADIOLOGY:Dr. F. R. KarjodkarDr. Jigna ShahDr. Chandrmani Mori
DEPARTMENT OF ORAL PATHOLOGY:Dr. Vandana ShahDr. Madhusudan AstekarDr. Dharmesh Vasavada
DEPARTMENT OF ORTHODONTIA:Dr. A. F. BhatiaDr. N. Daruwala
DEPARTMENT OF ORAL SURGERY:Dr. Bhagvandas RaiDr. Anisha MehtaDr. Kiran Desai
DEPARTMENT OF PEDODONTICS:Dr. Bhavna DaveDr. Anshula DeshpandeDr. Dinesh Rao
DEPARTMENT OF PUBLIC HEALTH DENTISTRY:Dr. Nisarg ChaudharyDr. Rahul PatelDr. Suyog Savant

108
ETHICS COMMITTEE
CHAIRPERSONDr. Chetana DesaiProfessorDept of PharmacologyBJMC, Ahmedabad.
DEPUTY CHAIRPERSONDr. Mahadev DesaiProfessor & Head,Dept of General Medicine, ADCH.
MEMBER SECRETARYDr. Harsh ShahReaderDepartment of Public Health Dentistry, ADCH.
COMMITTEE MEMBERSDr. Darshana ShahProfessor & H.O.DDept of Prosthodontics & Crown & Bridge, ADCH
Dr. Dolly PatelProfessor & H.O.DOrthodontics & Dentofacial Orthopedics, GDCH.
Dr. Alok ThakkarMedico Legal AdvisorDEPUTY CHAIRPERSON
Dr. G. C. PatelStatistician
Dr. Dilip ZaveriDirectorBiocare Research (India) Pvt. Ltd.Paldi, Ahmedabad.
COMMUNITY REPRESENTATIVE / SOCIAL WORKERMr. Darshak Shah
Dr. Janki VasantNGO. Samvedna