Embed Size (px)
Citation preview

Daniela Katz M.D.Sharett Institute of Oncology
Chemotherapy

Pareto Principle
• Also known as the 80–20 rule:
80% of the effects come from 20% of the causes.
Example:
“80% of your sales come from 20% of your clients”
“80% of the traffic occurs during 20% of the time”

Objectives

Why is it difficult to develop an effective chemotherapy?
Drug
Host Parasite
No effect Cytotoxic
Bacteria, fungi, protozoa, helminths, viruses vs. cancer cell.
Theory
Paul Ehrlich 1854-1915Nobel Laureate 1908

CHEMOTHERAPY: The basis of anti-cancer chemotherapy and the problem
Qualitative
Quantitative
The goal is to selectively kill malignant cells and spare normal host cells. Selective toxicity is not possible, as malignant cells are derived from the host and the differences between normal and malignant cells are much more subtle. Therefore, successful treatment is with doses and strategies that allow recovery of normal proliferating cells.

• Most chemotherapy drugs are active in cells that are rapidly multiplying – Chemotherapy may not be very active in
indolent or slow growing tumors
• Because of cytotoxic action on rapidly dividing cells they are toxic to normal cells that are actively multiplying– Bone marrow, GI tract, hair follicles are all
rapidly multiplying

Common Toxicities• Thus common toxicity of chemo agents are -
1. Neutropenia, anemia, and thrombocytopenia (collectively called myelosuppression or bone marrow suppression)2. Mucositis, diarrhea (GI toxicity)3. Alopecia4. Sterility/Infertility (especially sterility in males)
• Common Toxicity Criteria Grading System (CTC)–Grade 0 – 4
COST

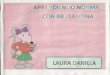
Gompertzian dynamics
Growth fraction (percentage of cells actively dividing)
S
M
G 1
G 2
G 0
A
B
Cnone cycling
cells
Anti-cancer chemotherapy most effect against cells in cell fraction A. Cells in fraction B can re-enter fraction A.
Cell number(tumor size)
Time
1012
109

The Cell Cycle
• G1 phase: cell prepares for DNA synthesis
• S phase: cell generates complete copy of genetic material
• G2 phase: cell prepares for mitosis
• M phase: replicated DNA is condensed and segregated into chromosomes
• G0 phase: resting state

3 x Problem associated with Anti-cancer chemotherapy
Cell No
Tum
ou
rS
ize
(cm
)
Pe rce n
ta ge o
fc
ell in c ycle (A
)
101210910 3 106
2
10
20
Limit of diagnostic procedures.
Exponential growth of a tumour
Cell number(tumor size)
Time
1012
109

Chemotherapy is present in 3 settings:
• Neoadjuvant chemo
• Adjuvant chemo
• Chemo for active disease
Goals of Cancer ChemotherapyCureProlong survivalPalliationRadiosensitive

Summary anti-cancer chemotherapy's
Cytotoxic drugs•Alkylating agentsCyclophosphamide, Busulfan, Carmustin, Chloramabucil, Ifosfamide, lomustine, Melphan, TreosulfanCisplatin, Carboplatin, Oxaliplatin
•Anti-metabolitesMethotrexate, Fluoruracil, Cytarabine, Cladribine, Fludarabine phosphate, Gemcitabine, Mercaptopurine
•Cytotoxic AntibioticsBleomycin, Dactinomycin, Daunorubicin, Doxorubicin, Epirubicin, Idarubicin, Mitomycin
•Plant derivativesEtoposide, Vinblastine, Vincristine
HormoneTamoxifen, Anastrozole, Letrozole
MiscellaneousImatinib, Bortezomib, Bevacizumab, Trastuzumab, Taxol, Cristaspase, Arsenic

Chemotherapy Classes• Alkylating agents
– nitrogen mustards– thiotepa, busulfan– nitrosoureas, mitomycin– procarbazine,
dacarbazine• Taxanes
– paclitaxel, docetaxel– nab-paclitaxel
• Topoisomerase II inhibitors– etoposide
• Platinum Complexes– cisplatin, carboplatin– oxaliplatin
• Anthracyclines
– doxorubicin, daunorubicin
– idarubicin, mitoxantrone
• Antimetabolites
– methotrexate
– purine antagonists
– pyrimidine antagonists
• Tubulin interactive agents
– vincristine, vinblastine
• Miscellaneous agents
– bleomycin
– asparaginase
– hydroxyurea

Summary of cytotoxic drug action
PU R IN E SYN THES IS PYR IM ID IN E SYN THE SIS
R IB O NU C LEO TIDE S
PR O TEINS
M IR O TU BU LES EN ZYM ES
D N A
R NA( )transfer, m essenger, ribosom al
D EO XY RIBO N U CLEO TID ES
PENTO STATIN (ct2)
6-M ER CAPTO PUR INE(ct2)6-TH IOG U ANIN E (ct2)
M ETH O TREXATE (ct2 )
C YTARABIN E (ct2)
5-FLU O R OU R ACIL (ct2 )
BLEOM YC IN S (ct3)
D OXO R UBIC IN (ct3)ETO PO SID E (ct4)
D ACTIN OM YCIN (ct3)
V IN C A ALKALO ID S (ct4)TAXANES (ct4)
ALKYLATIN G AG EN TS (ct1)M ITO M YC IN (ct3)C ISPLATIN (ct1)
Inh ib its adenosinedeam inase
Inh ib it pu rine syn thesisInh ib it nucleo tidein te rconversion
Inh ib its pu rine synthesisInh ib its D TM P
Inh ib its D N A po lym eraseInh ib its R N A function
Inh ib its D TM P syn thes is
D am ages D N Aand p revent repa ir
C ross-link D N A
Inh ib its topoisom erase II
Inh ib its topoisom erase II
Inh ib its R N A synthesis
Inh ib its R N A synthesis
In terca la tes in D N A
Inh ib it func tion o f m icro tubes

Alkylating Agents
• Main effect is on DNA synthesis with most cytotoxicity to rapidly proliferating cells

Action of Alkylating drugs- DNA adducts, cell cycle non-specific
A
A
T
T
C
C
G
G
C
C
G
G
Intra-strand linkage
Cross-linkingAldehyde
dehydrogenase

In use in:
BreastSarcomaOvarianTestisCLL
Non-Hodgkin’s LY
PO, IV

Cyclophosphamide and Toxicity
• Myelosuppression– principle dose-limiting toxicity
– primarily leukopenia
• Syndrome of inappropriate antidiuretic hormone
• Alopecia
• Highly emetogenic if 1500 mg/m2

Ifosfamide Toxicity• Hemorrhagic cystitis
– excretion of acrolein into the urinary bladder– greater with bolus regimen– higher after ifosfamide that after equivalent doses of
cyclophosphamide– symptoms of dysuria and urinary frequency– MESNA- sulfhydryl compound binds acrolein– routinely recommended to protect against urothelial
toxicity- Prevention!!!
– treatment of hemorrhagic cystitis requires evacuation of clots and continuous bladder irrigation;

Ifosfamide Toxicity• hematologic toxicity
– leukopenia– the principal dose-limiting toxicity of ifosfamide
• white blood cell nadirs usually occur between days 8 to 13 of the treatment cycle
• recovery will usually be complete by day 17 or 18 of the treatment cycle
• neurotoxicity– chloroacetaldehyde metabolite penetrates the BBB
well after systemic administration– CNS toxicity occurring in 10–40% of the patients
receiving high doses of the drug– Somnolense, mental confusion, cerebellar ataxia,
complex visual hallucinations– methylene blue as an effective treatment for
ifosfamide-induced encephalopathy is controversial

Ifosfamide Toxicity• Fanconi syndrome
– impairment of proximal tubule function, including glucose, protein, phosphate, bicarbonate and amino acid transport
– generally irreversible, long-lasting and potentially progressive
– manifested as polyuria, metabolic acidosis, and renal phosphate wasting
• Nausea and vomiting• Alopecia• Cyclophospamide and ifosfamide have little cardiac toxicity at
standard doses– at high doses such as those used for bone marrow
ablation, can cause severe myocarditis, exudative pericarditis, myocardial depression, arrhythmias and congestive heart failure

The PlatinumsIntrastrend DNA adducts
Mg/m2
AUC

Nucleotide excision repair pathwayERCC1

Cisplatin Toxicity• Nephrotoxicity
– dose-limiting toxicity
– renal damage is usually reversible but rarely can be irreversible and require dialysis
– platinum concentrations are higher in the kidney than in the plasma or other tissues
– initiating event is proximal tubular lesion
– secondary events such as disturbances in distal tubular reabsorption, renal vascular resistance, renal blood flow, and glomerular filtration, and polyuria seen 2 to 3 days later
– hypomagnesemia develops in about 75% of patients, beginning 3 to 12 weeks after therapy and persisting for months to years

Cisplatin Nephrotoxicity
• Preventive Measures– aggressive saline hydration (enhance urinary excretion)– lower doses may require less hydration– infuse over 24 hours– avoid other nephrotoxic agents– magnesium supplementation– predisposing factors to developing nephrotoxicity
include age 60 years or older, higher doses, pretreatment GFR < 75 ml/min, cumulative dose, low albumin, single dose compared with daily x 5 administration schedules

Cisplatin Toxicity
• Hematologic toxicity– can affect all 3 blood lineages– minor neutropenia, thrombocytopenia, and ANEMIA– its mild hematologic toxicity has allowed its
combination with highly myelosuppressive chemotherapy
• Ototoxicity– audiograms show bilateral and symmetrical high
frequency hearing loss– usually irreversible– caution with other drugs (aminoglycosides)

Cisplatin Toxicity
• Neurotoxicity– dose-limiting toxicity– most common symptoms are peripheral neuropathy and
hearing loss– first signs are loss of vibration sensation, loss of ankle
jerks and painful paresthesias in hands and feet– proximal progression and deficits in proprioception, light
touch and pain– recovery is typically incomplete
– less common include Lhermitte’s sign (electric shock-like sensation transmitted down the spine upon neck flexion)

Cisplatin Toxicity
• Nausea and vomiting– acute or delayed
– highly emetogenic if use doses than 50 mg/m2
– moderately emetogenic if use doses 50 mg/m2
– severe if not adequately prevented with appropriate medications
– typical anti-emetic regimen• aprepitant 125 mg po day 1 then 80 mg po days 2 – 3
• dexamethasone 12 mg po day 1 then 8 mg po daily x 3 days
• palonosetron 0.25 mg IVP day 1
• metoclopramide 10 mg every 4 hours prn N/V

Carboplatin Toxicity • Moderately emetogenic • Renal impairment is rare
– because it is excreted primarily in the kidneys as an unchanged drug, it is not directly toxic to the renal tubules
• Neurotoxicity is rare• Myelosuppression
– especially THROMBOCYTOPENIA– dose-limiting toxicity
• Hypersensitivity reaction– incidence of hypersensitivity seems to be correlated with
increased number of cycles of carboplatin

Oxaliplatin Toxicity• Gastrointestinal
– Moderate emetogenicity– diarrhea
• Minimal hematologic toxicity– Thrombocytopenia is dose-related (doses > 135 mg/m2)– mild neutropenia– mild anemia
• No nephrotoxicity• Hypersensitivity reaction
– mild– slowing down infusion rate and giving an antihistamine
and/or steroid– desensitization protocol
• Peripheral neuropathy

Clinical characteristics of oxaliplatin neurotoxicity
Acute symptoms Chronic symptoms
• Common (90% of patients)• Transient, short lived• Dysesthesias and paresthesias• Manifesting as stiffness of the
hands or feet, inability to release grip, and sometimes affecting the legs or causing contractions of the jaw
• Distal extremeties, perioral, oral, and pharyngolaryngeal
• 10% to 15% moderate neuropathy after a cumulative dose of 780 to 850 mg/m2
• Does not seem to be schedule-dependent
• Dysesthesias and paresthesias persisting between cycles
• Progressively evolving to functional impairment: difficulties in activities requiring fine sensorimotor coordination, sensory ataxia
• Tends to improve/recover after treatment is stopped
• Spares motor neurons (like cisplatin)
Prevention: Stop and Go Strategy, Ca and Mg infusions (may compromise efficacy), Gloves avoid cold

Comparison of Platinum Toxicity
Table 5. Comparative adverse effect profiles of platinum drugs
Adverse effect cisplatin carboplatin oxaliplatin
Nephrotoxicity ++ + -
Gastrointestinal toxicity
+ + +
Peripheral neurotoxicity
+++ - ++
Ototoxicity + - -
Hematologic toxicity + ++ +
Hypersensitivity - + -

Anthracyclines

Cytotoxic antibiotics Doxorubicin, Dactinomycin, Etoposide (VA)
D ouble stranded D N A
D ouble stranded D N A break
N on-c leavab le com p lexTrans ien t c leavab lecom plex P ersis tan t c leavab le
com plex
Topo isom erase II
DR
UG
S trand passing, ro ta tionb reak resea ling
Administered i.v.Acute lymphocytic leukemiaAcute granulocytic leukemia

Cardiotoxicity
Red Devil
aLOPECIA
NauseaMyelosupression
Mucositis

palmar-plantar erythrodysesthesia, or hand-foot syndrome

Chemotherapy- induced mucositis

Plant alkaloids (vincristine & vinblastine, Taxol)
Steady state
Polym erization blocked by vincristine & vinblastine
Polym erization stabilized by Taxol
Tub lindim er
Assem bly
C ontinued d isassem bly
S table m icro tubu le
D rug
D isassem bly
Resistance due to multidrug resistance,altered tublin moleculesAdministered I.v.Childhood leukemia's, Hodgkin'sand non-Hodgkin's lymphoma, testicular,ovarian carcinomas and brain tumours
Vincristine & vinblastine
Resistancealtered tublin molecules
Administered i.v.Metastatic ovarian and breast cancer
Taxol

Antimetabolites

5-Fluorouracil
• Fluoropyrimidine analogue= 5-FU

N
N N
N
HO
HO HO
HO
O
O O
O
O
O O
O
O
O O
O
F
F
HN
HN HNCH 3
HN
Inhib ites Thymidilate synthasevia com plexing w ith Tetrahydrofolate
Thym idilate synthaseTetrahydrofolate
P
P P
P
5-F luorouracilF luorouracil-Deoxy Urid ine
+
Thym idinePhosphorylase
D eoxyuridy lic acid D eoxythym idylic acid
Anti-metabolites (5-Fluorouracil)
ResistanceDecreased levels of thymidine phosphorylaseor affinity for 5FU
Administered parentallyBreast, ovarian, prostate,pancreatic, hepatic carcinomas

Indications
• Breast
• Colorectal
• Head and Neck
• Hepatoma
Leucovorin=Folinic Acid Stabilizes TS-FdUMP complex (GI tract)

Contraindications
• Myocardial infraction previous 6m

Toxicity
• Mucositis (Dose limiting toxicity for infusional)• Diarrhea (Dose limiting toxicity for infusional)• Myelosupression (Dose limiting toxicity for bolus)• Hand and foot syndrome (more with infusional)• Hyperpigmentation of the infused vein• Metallic taste during infusion• Cardiac symptoms+ ECG changes• Neurotoxicity- somnolence, cerebellar ataxia…
Extreme toxicity DPD deficiency??

Methotrexate

Anti-metabolites (methotrexate)
FF (glu)n
(glu)n
(glu)n
(G lu) (glu)n(glu)nF H 2 F H 4
F H 4
DTMP DUMPThym idyla tesynthase
D ihydro fo la tereduc tase
D ihydro fo la tereduc taseMethotrexate
Methotrexate
O ne-ca rbon U n it
C ellB lood
Polyglutam ates are retained in the cell
DTMP=Deoxythymidylic Acid
DUM P=Deoxyuridylic Acid
Cancer cells have higher rates of g lutamation enzym es levels
ResistanceDecreased transport into cellsDecreased affinity of DHF reductaseIncrease levels of DHF reductase
Administered orally or i.v.Non-Hodgkin’s lymphomaBurkitt’s lymphomaChildhood acute lymphoblastic leukemia

Indications
• Breast
• Head and neck
• Osteosarcoma
• High dose MTX 1-12 grams/m2
Leucovorin rescues the toxic effects of MTX and also may impair antitumor effect.

Contraindications
• Abnormal renal function• Third space fluid (ascites, effusions)- MTX
half life is prolonged.
• How is MTX given:• Hydrate the patient• Bicarbonate for a PH >7• Monitor MTX levels (<50nM)

Toxicity
• Myelosupression DLT
• Mucositis DLT (3-7d after MTX therapy)
• Nephrotoxicity (intratubular precepitation of MTX+direct tubular effect)
• Transient elevation of LFTs with HD MTX (12-24h)
• Pneumonitis
• Radiation recall skin reaction

Combination therapy
Knowledge of the pharmacokinetics of each cytotoxic agent is less important than knowing the maximal dose and the duration of that drug can be administrated before adverse side effects become unacceptable
Individual drugs must be active against the tumour
Drugs must have different modes of action• Minimize drug resistance• Hit cancer cells in different parts of cell cycle
Drugs must have limited overlapping toxicity
Individuals should be optimally scheduled
EtoposideBleomycin
CisplatinCurative therapy testicular cancer (BEP)
Renal & hepatic FunctionBone Marrow reserveImmune statusPrevious Treatments
Likely natural History of TumorPatients Wishes to undergo treatmentPatients Physical & emotional ToleranceLong term gains & Risks

כמו לפני בודקים ?'מה
•. כמותרפי טיפול כל לפני דם ספירת בודקיםתסיות <• 100000דרישות8.5המוגלובין <•לבנה • PMN > 1500ספירה
, פינוי קראטינין בודקים מהטיפולים חלקקראטינין.
. לב אקו

Secondary Leukemias
• Leukemias secondary to chemotherapy agents have poor prognosis.
• Secondary to alkylating agents– Most often occur after 5 – 7 years
– Often have MDS preceding leukemia
– Frequently FAB class M1 or M2
– Alterations of chromosomes 5 and/or 7 in 60% – 90% cases
• Secondary to topo II inhibitors:– Diagnosed 2 -3 yrs after tx
– Most often FAB class M4 or M5
– Frequent translocation of chromosome 11 (11q23) t(11;19)(q23;p13)

Chemotherapy Toxicity
• Neurologic– CNS: cytarabine, methotrexate, ifosfamide
– Peripheral: paclitaxel, oxaliplatin, vincristine
• Gastrointestinal– Nausea and vomiting: cisplatin, doxorubicin, cyclophosphamide
– Mucositis: methotrexate, melphalan, etoposide, 5-FU
• Pulmonary– Methotrexate, bleomycin
• Cardiovascular– Anthracyclines

Chemotherapy Toxicity
• Hepatic– busulfan
• Metabolic– Ifosfamide, cisplatin
• Renal– Hemorrhagic cystitis: cyclophosphamide, ifosfamide
– Renal failure: cisplatin
• Dermatologic– Hand-foot syndrome: 5-FU, capecitabine, cytarabine
• Immune System– Immunosuppression: fludarabine, cyclophosphamide, steroids
– Hypersensitivity: paclitaxel, asparaginase, bleomycin

Miscellaneous Toxicity
• Etoposide– Hypotension, flushing (infusion-related)
• Irinotecan– Acute and delayed diarrhea (SN-38 metabolite)