Embed Size (px)
Citation preview

1272
dermatitis of the scalp and dandruff. An alternative to the creambase may be required for delivery of adequate amounts ofketoconazole into the follicles to treat pityrosporal folliculitis, adisorder which responds well to systemic ketoconazole.3Although our study was small and uncontrolled the results are
unequivocal and we conclude that topical ketoconazole is likely tobe an effective therapy for seborrhoeic dermatitis. This is a
considerable advance on treatment with corticosteroids, theultimate effect of which on the face may be worse than the diseasebeing treated.
Department of Dermatology,University of Newcastle upon Tyne,Newcastle upon Tyne NE1 4LP
P. M. FARRSAM SHUSTER
1. Shuster S. The aetiology if dandruff and mode of action of therapeutic agents. Br JDermatol 1984; 111: 235-42.
2. Ford GP, Farr PM, Ive FA, Shuster S. The response of seborrhoeic dermatitis toketoconazole. Br J Dermatol 1984; 111: 603-07.
3. Ford GP, Ive FA, Midgley G. Pityrosporum folliculitis and ketoconazole. Br JDermatol 1982; 107: 691-95.
DANAZOL RAISES ANTITHROMBIN III LEVELS INCASES OF FAMILIAL DEFICIENCY
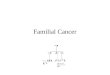
SIR,-Inherited antithrombin III (AT III) deficiency (hereditarythrombophilia) is a rare disorder characterised by recurrent,sometimes fatal, deep-vein thrombosis and pulmonary embolism.The condition is usually treated by long-term anticoagulation.Synthetic androgens such as danazol induce the formation andrelease of other protease inhibitors, including Cl-inhibitorl and&agr;1-antitrypsin2 so we wondered if danazol would correct thebiochemical abnormality in affected members of a family with ATIII deficiency (table, fig 1).Two brothers in this family (II. and 11.2) have been treated with
danazol:Case II.l-56-year-old man with history of pain and stiffness in the left leg(at
age 41); breathlessness, bilateral pleuritic pain, pulmonary emboli, and smallpleural effusions (age 42); and deep venous thrombosis (age 52) after whichlong-term aspirin was prescribed. At the age of 54 his left leg swelledintermittently and he had further pleuritic pain and pulmonary emboli. AT IIIdeficiency was diagnosed and he was anticoagulated with long-term warfarin.Case II.2—His brother presented aged 48 with pleuritic pain and a swollen
right calf. 1 month later the left calf also became swollen and venographyrevealed a DVT. When warfarin was discontinued the leg symptoms recurred.He had a further suspected pulmonary embolism at the age of 55 andmyocardial infarctions (aged 57 and 59).Two sisters have a history of DVT or varicose veins. Two
daughters of patient 11.1 1 and one son of patient IL2 were found tohave AT III deficiency on screening.
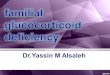
Patients ILl and 11.2 were given danazol in divided doses bymouth up to 600 mg daily. Plasma AT III levels rose (fig 2) as didaI-antitrypsin levels, with no changes in blood urea, electrolytes, orliver function tests. Patient 11.1 took two courses of danazol. The
daily dose was progressively increased: 400 mg daily brought theAT III level (chromogenic) within the normal range and 600 mg
SUMMARY OF PATIENTS WITH AT III DEFICIENCY
*Measured with chromogenic substrate S2238 (’Coa’ test; Kabi) or by radial .
immunodiffusion on Behnngwerke ‘Norpartigen’ plates.
Fig I-Pedigree showing autosomal dominant inheritance of AT IIIdeficiency.
resulted in a further increase. In patient 11.2 the ai-antitrypsinlevels rose from I - 4 g/l before danazol to 2’ 3 g/l, falling to 1’ 7 g/18weeks after the drug had been stopped. In patient II.1, the
a I-antitrypsin increased to 2-2 g/1 during both periods on danazolcompared with levels of 1. 4-1’ 7 g/l off therapy and 1’ 6 g/l betweentreatment periods. The only side-effects were mild headaches in oneman and a sense of wellbeing in the other. Warfarin, which does notaffect AT III levels,3 was continued to keep the prothrombin ratiowithin the therapeutic range but the dose had to be reduced in bothcases to prevent excessive anticoagulation.Anabolic steroids have been reported to produce modest increases
in plasma AT 111.4-6 However danazol has not previously been usedto treat AT III deficiency despite its usefulness in other protease-deficiency states and interest in its possible use to augment factorVIII and factor IX levels. In the two patients described a
therapeutic dose of danazol reversibly corrected the AT III
deficiency without significant side-effects. a. -antitrypsin levels alsorose. For long-term therapy, warfarin is probably the treatment ofchoice. However, danazol may be worth trying when warfarin is
Fig 2-Response of AT III level (chromogenic) to danazol therapy.

1273
contraindicated (eg, before major surgery) or to raise AT III levelsbefore surgery or as an adjuvant to anticoagulation where venousthrombosis occurs despite warfarin therapy.Department of Thoracic Medicine,Staffordshire General Infirmary,Stafford ST16 2PA ANDREW J. FAIRFAX
Department of Haematology,Central Pathology Laboratory.Hartshill, Stoke on Trent ROBERT M. IBBOTSON
1. Gelfand JA, Sherins RJ, Alling DW, Frank MA. Treatment of hereditary angioedemawith danazol: Reversal of clinical and biochemical abnormalities. N Engl J Med1976; 295: 1444-48.
2. Gadek JE, Fulmer JD, Gelfand JA, Frank MM, Petty TL, Crystal RG. Danazol-induced augmentation of serum &agr;1-antitrypsin levels in individuals with markeddeficiency of this antiprotease. J Clin Invest 1980; 66: 82-87.
3. Winter JH, Fenech A, Ridley W, Bennett B, Cummmg AM, Mackie M, Douglas AS.Familial antithrombin III deficiency. Quart J Med 1982; 51: 373-95.
4. Walker ID, Davidson JF, Young P, Conkie JA. Effect of anabolic steroids on plasmaantithrombin III, &agr;2-macroglobulin and &agr;1-antitrypsin levels. Thrombosis DiathHaemorrh 1975: 34: 106-14.
5. Fiessinger JN, Alach M. Stanozolol treatment in an AT III deficient patient.Thrombosis Haemostas 1980; 43: 183.
6. Winter JH, Fenech A, Bennett B, Douglas AS. Prophylactic antithrombotic therapywith stanozolol in patients with familial antithrombin III deficiency. Br J Haematol1984; 57: 527-37.
7. Gralnick HR, Rick ME. Danazol increases factor VIII and factor IX in classic
haemophilia and Christmas disease. N Engl J Med 1983; 308: 1393-95.
CHOLECYSTOKININ AND CYSTIC FIBROSIS
SIR,-Dr Cantor and his colleagues (Nov 3, p 1039) suggest ourhypothesis, that the basic defect in cystic fibrosis is due to a
deficiency in proteolytic cleavage of cholecystokinin (CCK)(Sept 8, p 541), implies that CCK-8 is the sole or major biologicallyactive form of CCK in the circulation. Our hypothesis does notimplicate plasma or circulatory levels of CCK. On the contrary, wesuggested that the major routes by which CCK-8 effects exocrinesecretion are neurocrine and paracrine rather than endocrine.CCK is unique among gastroenteropancreatic peptides in having
comparatively high concentrations in both brain and gut.Preprocholecystokinin, the large precursor molecule of CCK, is114 aminoacids long in both tissues. Sequencing ofcDNA clones ofCCK mRNA from brain and gut has established that, although theCCK precursor in both tissues is the same, the distribution of themolecular forms in the two tissues is very different. The precursoris subjected to post-translational cleavage which differs in brain andgut and is thus tissue specific. The smaller forms of CCK producevarious effects, acting either as neurocrine peptides in the brain andautonomic nervous system, or as paracrine peptides in the CCK-containing peptide cells of the gastrointestinal tract. We suggestthat the smaller forms of CCK are normally released either from theCCK peptide cells of the gut or from the autonomic nerve fibresdirectly into the exocrine end organs such as pancreas, gallbladder,salivary glands, trachea, and sweat glands. The CCK binds directlyto cell surface receptors and is then mediated in the exocrine glandcells by calcium and cyclic nucleotides. Tissue-specific cleavage oflarge CCK thus takes place within the brain and autonomic nervesor in the gut cells.We agree that circulating levels of CCK are very low and that
plasma measurements are difficult. The different forms of CCK inthe circulation would be expected to reflect to some degree thoseproduced in all the different tissues. While we acknowledge thatlarge CCK molecules may be as potent as CCK-8 in experimentalsystems, the relevance of this to the in-vivo situation, particularly toa neurocrine mode of transmission, is very questionable.As the production of smaller active forms of CCK which control
exocrine secretion is by post-translational cleavage of largeprecursors in the autonomic nervous system or gut, investigation ofdifferences of such cleavage in cystic fibrosis must be made in thespecific tissues and the hypothesis cannot be refuted bymeasurements in plasma.MRC Clinical and Population Cytogenetics Unit,Western General Hospital,Edinburgh EH42XU
CHRISTINE M. GOSDEN
JOHN R. GOSDEN
1 Gubler U, Chua AO, Hoffman BJ, Collier KJ, Eng J. Cloned cDNA to cholecystokininmRNA predicts an identical preprocholecystokinin in pig brain and gut. Proc NatlAcad Sci USA 1984; 81: 4307-810
GALLSTONES AND CHOLECYSTECTOMY RATES
SiR.—Dr McPherson and his colleagues (Nov 10, p 1092)misrepresent the observations in my study of gallbladder diseaseprevalence and concurrent cholecystectomy rates (Sept 15, p 621).It was not suggested that cholecystectomies are often done in theabsence of gallbladder disease, and this seems very unlikely.However, the overwhelming proportion of gallstones, which arevery common, appeared to be silent and 86% were not treated bysurgery. Cholecystectomy rates in Dundee and Scotland generallyshowed a continuing increase in 1961 to 1978, and the operation wasdone twice as often at the end of this period as at the beginning.Fowkes has demonstrated that cholecystectomy rates in different
parts of Scotland correlated well with local medical resources andwith surgical staffing in particular. The cholecystectomy rate inNorth America is much higher than it is in Britain despite thesimilar prevalence of gallstones.2-s It seems inescapable that
operation numbers are not determined by the frequency with whichgallstones occur in the community, either for Britain and NorthAmerica.
Cross-sectional studies of gallstones disease have yieldedcontradictory and unreliable results, almost certainly because of theproblems of studying small numbers of patients in differentlocalities.4,6 As yet this technique can provide no information aboutchanging patterns of disease or treatment though it may do in thefuture with the advent of ultrasonography.The case may be stated simply: a lot of people have cholelithiasis,
most gallstones do not matter, and the rate at which subjects withgallstones are investigated, diagnosed, and treated is remarkablyvariable.
Department of Medicine,Bishop Auckland General Hospital,Bishop Auckland,Co Durham DL14 6AD M. C. BATESON
1. Fowkes FGR. Cholecystectomy and surgical resources in Scotland. Health Bull 1980;(May): 126-32.
2. Lieber MM. The incidence of gallstones and their correlation with other diseases. AnnSurg 1952; 135: 394-405.
3. Ludlow AI. Autopsy incidence of cholelithiasis. Am J Med Sci 1937; 193: 481-82.4. Watkinson G. The autopsy incidence of gallstones in England and Scotland. In:
Proceedings of the 3rd World Congress of Gastroenterology (Tokyo, 1966).5. Bateson MC, Bouchier IAD. Prevalence of gallstones in Dundee. a necropsy study Br
Med J 1975; iv: 427-29.6. Barker DJP, Gardner MJ, Power C, Hutt MSR. Prevalence of gallstones at necropsy in
nine British towns: a collaborative study. Br Med J 1979; ii: 1389-92.
131I-MIBG AND MEDULLARY CARCINOMA OFTHE THYROID
SIR,-As your Oct 20 editorial notes, the 1-w-iodobenzylguan-idine (13 11-MIBG) scan has proved useful in the detection andtreatment of metastatic phaeochromocytoma. Scintigraphic imagingof other neoplasms of neuroectodermal origin, including neuro-blastomal and carcinoid tumours2 has also been described and131 I-MIBG may be of value in the investigation and management ofthese conditions. We can confirm the report of Endo and colleagues3 3that 131 I-MIBG is taken up by medullary carcinoma of the thyroid.A 61-year-old woman from a kindred with multiple endocrine
neoplasia type IIa presented with severe hypertension (240/180mm Hg). Plasma noradrenaline and adrenaline were raised (31- 5and 14-5 5 nmol/1, respectively) and a computerised tomographicscan of the abdomen demonstrated bilateral adrenal tumours.
Medullary carcinoma of the thyroid was suggested by theconcentration of calcitonin in peripheral venous plasma, which was1280 ng/1 (normal 10-45); concentrations in the left superior andinferior thyroid veins were 3800 and 4580 ng/1, respectively.The patient’s abdomen, chest, and neck were scanned 24-120 h
after intravenous injection of 20 MBq (0-5 mCi) 131I_MIBG.Uptake of iodide by the thyroid was prevented with oral potassiumiodide 60 mg twice daily for the duration of the study. Radioactivitywas concentrated over both adrenals (figure) and over the left side ofthe neck, the lesion/background count density ratio increasing overthe first 48 h. The mean count density ratio (lesion/background) inthe neck was 2, whereas in the adrenal area the ratio was about 5.The best images of the thyroid area were obtained at 96 h. Thepresence of a solid left-sided thyroid tumour was subsequently