-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
1/14
Endodontic Topics 2002, 2, 89102 Copyright C Blackwell
Munksgaard
Printed in Denmark. All rights reserved ENDODONTIC TOPICS
2002
1601-1538
Technical aspects of treatment in
relation to treatment outcomeLISE-LOTTE KIRKEVANG & PREBEN
HRSTED-BINDSLEV
Apical periodontitis
Apical periodontitis (AP) is an inflammatory processin the
periapical tissues that may occur as a sequel tocaries, trauma or
operative dental procedures whenbacteria have been introduced into
the dental pulp.The relationship between AP and bacteria
infectingthe root canal system is well established (13). Infec-tion
of the coronal pulp may spread apically, usuallycausing necrosis of
pulpal tissues and may reach theapical part of the root canal. The
infection then in-
vades the periapical area resulting in local bone de-struction.
The success of root canal treatment de-pends on several factors:O
elimination of surviving microorganisms in the
root canal;O creation of a tight seal in order to prevent
tissue
fluid from the periapical tissues feeding bacteria, whilst
nonetheless remaining in the root canal,and;
O establishment of an effective blockade of any com-munication
between the oral cavity and the peri-radicular tissue through a
high quality of endodon-tic and coronal restorations (4).
When focusing on the relation between the technical
and the biological aspect of periapical repair,
severalexplanations for slow or absent healing of AP havebeen
pointed out. The low success rates when root-fillings are too short
are probably due to infected pulpremnants or dentin chips in the
apical part of a rootcanal. Overfilling may induce an inflammatory
reac-tion caused by extrusion of the root-filling materialor
infected debris into the periapical area, combined
with physical tissue damage caused by over-instru-mentation.
89
The chronic nature of AP means that patients oftenhave no
subjective symptoms. Given these circum-stances, oral radiography
plays an important role inthe diagnosis and treatment of AP (5).
The presenceof AP is important for tooth survival since caries,
in-cluding pulpitis and AP, has been identified as beingone of the
main reasons for tooth extractions in sev-eral populations (611).
It is important to realize thatthe infection cannot resolve itself,
as the working con-ditions of the immune defence system are
impairedby the localization of the infection inside the root
ca-nal. The goal of contemporary endodontic treatmentis both to
prevent the spreading of the infection, andto create conditions
under which healing can occur,meaning that the tooth can be
preserved. To selectthe best treatment, it is important to gather
infor-mation on different aspects of treatment and relatethis to
the treatment outcome.
General methodologicalconsiderations
Cross-sectional studies are investigations in which in-formation
is collected in a systematic way in a well-de-fined population at a
given point in time. This type of
study can be used to describe disease prevalence, andrelate the
disease to subjects exposure to etiologicagents and pathogenic
factors (12). In the context of
AP, the cross-sectional study could be used to describethe
association between the presence of AP (diseaseprevalence, outcome)
and the quality of endodontic orcoronal restorations (in this
instance, exposure infor-mation). Thecross-sectional study does
notprovide in-formation on the time of event occurrences, but
de-scribes exposure and disease status at the time of the
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
2/14
Kirkevang & Hrsted-Bindslev
investigation. It is therefore not possible in this type ofstudy
to decide whether the exposure preceded the dis-ease or the disease
preceded the exposure. This doesnot, however, preclude the use of
cross-sectional datain the development of a risk assessment model
target-
ing, for example, the periapical status.Since the historic
dimension of the exposure infor-mation retained in the
cross-sectional study is notavailable, it is not possible to
identify why or when arestoration has been made; only that it is
present atthe time of the examination. This means that
thetreatment/disease history is illustrated by proxy vari-ables in
the mouth, e.g. the number and quality ofthe restorations. Another
problem in the cross-sec-tional study design is that only
information on thepresent status of the individual is available,
and sincemany diseases, for example, AP, often take time todevelop
or heal, the exposure information may havebeen too recent to have
had any influence on the de-
velopment of AP. On the other hand, some of theexposure
information accumulates in/around the in-dividual, thereby creating
a picture of both presentand previous exposures.
In the cross-sectional study, it is possible to
identifypotential risk indicators, but longitudinal studies
areneeded to identify a causal direction. The concept ofcauses has
been, and still is, the subject of extensivedebate among
epidemiologists, and a variety of termshave been used. In order to
understand the conceptof causes, it is first necessary to define
what causemeans. Rothman and Greenland define it as:
...an event, condition, or characteristic that pre-ceded the
disease event and without which the diseaseevent either would not
have occurred at all or wouldnot have occurred until some later
time (12) .
This definition describes a cause as a component ofa sufficient
cause in which several causes act togetherat the same time as a
completely causal mechanism.MacMahon and Trichopoulos (13) used the
concept
of direct and indirect causal associations where thecause may be
described as direct or indirect, situatedin a causal web, and the
association with the outcomemight be of varying magnitude. These
definitions ofcause seem to be relevant also to the etiology
thatapplies to most diseases, as only very few diseases, ifany at
all, can be said to be monocausal. Most longi-tudinal studies focus
on one part of the treatment inan attempt to expound the
relationship between thatparticular issue and the treatment
outcome.
90
When looking at the literature, it is essential to real-ize that
the epidemiological and controlled longitudi-nal studies work
together in a kind of symbiosis
where ideas are exchanged to be further elucidated.
History of/criteria for the outcomeof root canal treatment
The diagnosis of AP is predominantly based on devi-ations from
the normal periapical anatomy as display-ed by radiography.
Strindberg (14) presented a fre-quently quoted set of criteria for
classification of en-dodontic treatment results based on
radiographicsigns. He conducted a comprehensive longitudinalstudy
on factors related to the results of pulp therapy,
where a total of 254 patients with 529 root filledteeth were
followed for 210years, and defined theradiographic criteria for
evaluating the result of rootcanal treatment as follows
a success when (a) the contours, width and struc-ture of the
periodontal margin were normal, (b) theperiodontal contours were
widened mainly aroundthe excess filling; a failure when there was
(a) a de-crease in the periradicular rarefaction, (b)
unchangedperi-radicular rarefaction, and (c) an appearance ofnew
rarefaction or an increase in the initial; and asuncertain when (a)
there were ambiguous or technic-ally unsatisfactory control
radiographs which couldnot for some reason be repeated, or (b) the
tooth
was extracted prior to the 3-year follow-up owing tounsuccessful
treatment of another root of the tooth.
These criteria thus divided the cases into successes,failures,
and uncertainties.
The width of the periodontal ligament, the integrityof the
lamina dura and the presence of periapical ra-diolucency have,
since Strindbergs description, beenused in both longitudinal (1521)
and cross-sectional(2233) studies to evaluate the periapical
status.
In 1967, Brynolf (34), in order to disclose to whatextent
histologic changes are reflected in radiographs,compared histologic
and radiographic appearances ofperiapical changes in human autopsy
material from142 individuals. Sections of the apical region from292
upper incisors constituted the material for theinvestigation. She
concluded that differentiation andclassification of the periapical
status were possible inoral radiographs. The study very thoroughly
de-scribed the changes characterising the different levels
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
3/14
Technical aspects
Table1. Brynlofs histological and corresponding roentgenological
main groups (34)
Histological Roentgenological Description
N Ng Normal
M Mg Marginal cases
I Ig Mild, chronic inflammation
Ix Irx Mild, chronic, more active inflammation
II IIg Moderate, chronic inflammation
III IIIg Severe, chronic inflammation
IV Iv g Severe, chronic inflammation with features of
exacerbation
of inflammation and grouped them in seven maingroups
(Table1).
The continuous inflammatory process could thusbe classified
radiographically, and this constituted thebasis for development and
application of an ordinalscoring scale in the radiographic
evaluation of AP.
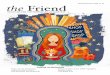
In 1986, rstavik et al. (35) used the results ofBrynolfs study
(34) to develop an index for the regis-tration of AP, the
Periapical Index (PAI). The indexconsists of five categories, each
representing a step onan ordinal scale from sound periapical bone
to severeapical periodontitis. One or two radiographs fromBrynolfs
original material represented each of the
five groups, and these radiographs were used as visualreferences
(Fig. 1).
Before using PAI, a calibration course for the PAIsystem should
be followed. The course involves scor-
Fig.1. The visual references of the periapical index (PAI) (Fig
8.2, rstavik D, Pitt Ford TR eds. Essential EndontologyOxford:
Blackwell Science, 1998; 181).
91
ing of 100 radiographic images of teeth; the group ofteeth
consist of various tooth types, with and withoutroot-fillings. For
each tooth, a true periapical statushas been established by
consensus between five endo-dontists, one dental radiologist, four
general prac-titioners and one dental assistant (35); while
theradiographs and histological correlates of Brynolf(34) may be
viewed as a gold standard, the definedtruth of the 100 teeth may be
viewed as a silverstandard atlas. After scoring 100 teeth in the
calibrat-ing course, the observers results are compared to
thesilver standard atlas.
When a tooth is to be scored, the observer finds the
reference radiograph by visual comparison of whichperiapical
area is most similar to the periapical area ofthe tooth under
evaluation. The corresponding scoreis then assigned to the tooth.
If the tooth is multi-
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
4/14
Kirkevang & Hrsted-Bindslev
rooted, the highest score given to a root should beassigned to
the tooth. The use of visual references inthe PAI de-emphasised the
importance of the ob-server, since no clinical judgement is
permitted in theassessment of AP. This has resulted in a better
repro-
ducibility in the radiographic scoring, and differentstudies may
be more easily compared (35, 36).It can be debated if the PAI
system is valid for can-
ines, premolars and molars, as the histologic materialon which
it was based only included maxillary in-cisors. The anatomic
structures in the jaws vary andmay confound the diagnostic process,
but this prob-lem is the same for all radiographic studies. It
wouldseem reasonable to assume that the radiographic ap-pearance of
AP should be comparable in all teeth.
The PAI has been used in several longitudinal (3741) and
cross-sectional studies (40,4248).
Reliability and reproducibility ofperiapical radiography
In both longitudinal and cross-sectional investi-gations on
endodontic treatment, the assessment oftreatment quality has been
primarily based on radi-ography, and the cross-sectional studies
especiallyoften rely on radiographic images alone.
Obviously, the two-dimensional nature of radio-graphic images
imposes some limitations. Radio-graphs may not reveal minor
occlusal, buccal or oraldefects, which could lead to the amount of
inad-equate coronal restoration required being underesti-mated. In
addition, in multirooted teeth, the lengthof the roots and
root-fillings may not be reproducedcorrectly (49).
When studies have included the lateral seal as oneof the
criteria, there is general agreement that, if a
void is present in the lateral aspect, the root-fillingshould be
categorised as inadequate. However, the
limited reproducibility of the lateral seal as a descrip-tive
parameter for the quality of the root-filling hasbeen demonstrated
in several studies (47,5053).Therefore, Eckerbom & Magnusson
(52) demon-strated that the reproducibility of one orthoradial,
in-traoral radiograph was poor when evaluating the lat-eral seal;
this was probably due to the common occur-rence of oval- and
ribbon-shaped root canals. Theevaluation of the lateral seal of a
root-filling shouldbe evaluated in images with a mesial and/or
distal
92
angulation to get a realistic estimate of the quality ofthe
seal.
The length of the root-filling has proved to be amuch more
reproducible quality parameter than thelateral seal (47, 52, 53),
probably because it is easier
to measure the length of the root-filling than it is todetect
voids.Reit and Hollender (54) noticed that, in radio-
graphic studies, it is difficult to define and maintaincriteria
for the quality of the root-filling and for diag-nosing AP. The
precision of the quality assessment ofthe root-filling has,
therefore, not been convincing,and large inter-examiner variation
has been reported(54, 55).
Concerning the radiographic diagnosis of AP, Gold-man et al.
(56) found that the inter-observer agree-ment in radiographic
assessments of endodontic suc-cess or failure was very poor.
Several attempts havebeen made to minimize the observer
variationthrough calibration (51, 54, 57, 58). Reit (59) evalu-ated
the effect of two calibration programs accord-ing to different
principles. In one of the two pro-grams, the examiners evaluated a
separate radio-graphic sample in which they, through
discussions,exemplified the scoring system that was going to beused
to score the original material. In the other cali-bration program,
the examiners were introduced tothe signal-detection theory. This
theory assumesthat the observer, through a continuum of obser-
vations in his own mind, defines a cut-off point fordisease. The
calibration programs, however, only re-sulted in significant
improvement when diagnosingperiapical destruction of bone
definitely not present.That the effect of observer calibration is
not signifi-cant was also demonstrated in other studies (55, 57).It
was concluded that the benefits of calibration pro-grams seemed to
be limited and suggested that thiscould be due to the complex
structure of the de-cision making process (57).
By statistical evaluation of the scoring performanceof different
methods of evaluation, the PAI scoringsystem produced better
receiver-operating-character-istic (ROC) curves than the
probability assessmentindex (35).
Different methods of recording and maintainingcriteria for AP
and treatment quality, as well as differ-ent thresholds for AP and
treatment quality, indicatethat great caution must be exercised
when resultsfrom different studies are being compared.
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
5/14
Technical aspects
Quality of root-fillings and coronalrestorations
Quality of root-fillings
Longitudinal studies
Information on the quality and prognosis of root ca-nal
treatment has mainly been based on clinicalstudies made in
controlled environments at dentalschools or in specialist clinics.
The results from thesecontrolled, longitudinal studies have shown
successrates up to 96% in establishing periapically sound
con-ditions after endodontic treatment (1417,1921,37,38, 6063).
The longitudinal studies have found that severalfactors may
influence the outcome of the treatment.It has been demonstrated
that the preoperative diag-nosis of the tooth is of importance for
the outcomeof the treatment, but the quality of the endodonticand
the coronal restoration have also been found toinfluence the
treatment outcome (64).
The quality of the root-filling has been evaluated inseveral
studies. The parameters defining the quality ofthe root-filling
differ among investigators, and differ-ent thresholds have been
used when categorisingroot-fillings as adequate or inadequate. In
somestudies, the quality parameters were defined only bythe length
of the root-filling (14, 15, 20, 6062, 65,66). In other studies,
the quality was assessed both inthe lateral and in the apical
aspect (16, 17, 19) (Table2).
The working length and the optimal apical limit ofroot canal
obturation has been the subject of on-go-ing discussion for
decades. As a consequence, studies
vary greatly in the categorisation of adequate length.Some
define root-filled teeth, filled flush with apex,as adequate whilst
others view it as inadequate. Somerequire the distance from the
radiographic apex to be2mm, others 3mm. Some accept extrusion ofthe
root-filling if1mm. The actual position of theapical
foramen/foramina has been found to be from0.2 to 3.8mm short of the
radiographic apex (67).Most studies have indicated that the apical
limit ofthe root-filling should be at the apical constriction ofthe
root canal, and that extrusion of root-filling ma-terial into the
periapical tissue should therefore beavoided (6870).
When the technical quality of the root-filling was
93
related to the treatment outcome, the studies demon-strated
success rates of 70100% if the quality wasassessed to be optimal.
If the root-fillings were shortof the apex, a lower success rate of
57%-95% wasfound (Table2). If extrusion of root-filling
material
in the periapical tissue were found, the success ratewas even
lower at 50%-90%. Some studies, however,found no significant
difference between root-fillings
within 2mm from apex and root-fillings that were tooshort (65,
66). It should be noted that the thresholdbetween adequate and
inadequate vary among thestudies and, therefore, the results should
be com-pared with certain reservations.
In a study by Weiger et al. (71), another methodol-ogical and
statistical problem was discussed. In longi-tudinal studies,
success rates have been calculated asthe percentage of successfully
treated teeth followed-up or included in the study. This approach
does notdeal with the problem of the individual time requiredfor
healing/development of AP; in other words, indi-
vidual observation times are not accounted for. Theeffect of
clustering in a sample, e.g. when severalteeth/roots from the same
individual have been in-cluded in the study, may result in under-
or over-esti-mation of the outcome. It was suggested that
theanalysis of event times according to Kaplan & Meier(72)
should be used for estimating prognosis of rootcanal therapy.
Despite the methodological differences, the con-trolled
longitudinal studies suggest that it is possibleto control and
eliminate AP, at least if the treatmentis performed by
highly-skilled personnel or supervisedstudents, probably by
reduction of the more commonreasons for failure, such as poor
aseptic technique, un-detected infected root canals, inadequate
instrumen-tation, and inadequate temporary and permanent
fill-ings.
Cross-sectional studiesCross-sectional studies from different
populationshave, on the other hand, failed to demonstrate thatthe
dental profession in general has succeeded in thecontrol and
elimination of AP (Table 3). On the con-trary, such studies have
revealed a high frequency ofinadequate root-fillings and of AP
associated withroot-filled teeth (22, 24, 27, 28, 30, 4247, 73,
74).
In addition, in the cross-sectional studies, the qual-ity of
root-fillings has been related to the periapical
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
6/14
Kirkevang & Hrsted-Bindslev
status, and again the parameters defining the qualityof the
root-filling differ among investigators, with dif-ferent thresholds
being used when categorising root-fillings as adequate or
inadequate. Some have concen-trated merely on the length of the
root-filling (28,
30), whilst others have used the length of the root-filling and
the lateral seal without combining the two(4244), and some have
used both length and lateralseal and a combination of the two
recordings (22, 24,25, 27, 32, 33, 4547)(Table4).
Despite the differences in populations, diagnosticcriteria and
evaluation methods, most studies findthat the quality of the
endodontic treatment isstrongly related to the periapical status.
In studies ofNorwegian adults, about 30% of the endodontic
res-torations had an inadequate seal, and about 70% ofthese had AP
(42,43). Regarding the length of theroot-filling, studies of
European populations havefound that 15%57% of teeth with adequate
lengthof the root-filling had AP. If the root-filling was tooshort,
15%85% of the teeth had AP, and if the root-filling was too long,
about 52%75% of the teethshowed periapical lesions (Table4).
Due to the methodological variations among thedifferent studies,
it is difficult to directly compare per-
Table 2. Technical quality of root fillings in longitudinal
studies related to the outcome.
Study Cases Adequate Inadequate Adequate Short % Long %lateral
seal lateral seal length % (success %) (succes %)(success %)
(success %) (success %)
Strindberg (14) 774 (roots) 42.4 (90)* 29.1 (90) 28.8 (81)
Grahen & Hansson (15) 1277 (roots) 35.5 (83)* 27 (93) 37.5
(75)
Harty et al. (16) 1139 87.4 (93) 11.6 (65) 48.8 (93) 17.2 (88)
31.9 (87)
Heling & Tamshe (58) 344 (roots) 53 (71) 18 (57) 29 (68)
Heling & Shapira (59) 128 (roots) 36 (80) 52 (82) 12
(73)
Kerekes & Tronstad (17) 501 (roots) 96 (93) 4.9 (28) 62.1
(92) 34.4 (90) 3.5 (67)
Swartz et al. (63) 1770 (roots) 12 (90)** 80.9 (92) 7 (63)
Bystrm et al. (64) 79 14 (100) 48.1 (95) 37.9 (90)
Sjgren et al. (21) 849 (roots) (87) (67)*** (82) (31)*** (94)
(67)*** (68) (65)*** (76) (50)***
Smith et al. (20) 821 613 (87) 116 (76) 92 (75)
Friedman et al. (60) 378 (teeth) 81 (79) 19 (74)****
*filled to apex or 1mm excess**filled flush to apex
***1. parentheses teeth with necrosis/AP, 2. parentheses
previously treated teeth****short and long
94
centages from them. However, the tendency is thesame:
cross-sectional studies on endodontic treat-ment fail to
demonstrate the same high success rateas controlled follow-up
studies. It may be claimedthat, despite the obvious study
differences, various
studies have consistently found that the poor qualityof the
root-fillings is related to AP, makes this findingeven more
evident.
Quality of coronal restorations
In recent years emphasis has also been placed on thequality of
the coronal restoration and its relation tothe periapical status in
root-filled teeth. It has beensuggested that the coronal
restoration, as well as theroot-filling, serve as a barrier against
fluid and bac-terial penetration into the periapical area. The
relationbetween the quality of the coronal restoration and
theperiapical status has been investigated in severalstudies (46,
47, 75, 76). Ray & Trope (75) foundthat the technical quality
of the coronal restoration
was even more important for the periapical statusthan the
quality of the endodontic treatment. Siderav-icius et al. (46)
identified a correlation between thequality of the coronal
restoration and the periapical
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
7/14
Technical aspects
Table3. Studies on endondontic treatment and AP.
N Teeth Root-filledindi- Mean N with Root-filled teeth Patient
population
Author Year vidual N teeth teeth AP (%) teeth with AP (%)
(country)
Bergenholtz et al.(101) 1973 240 5472 22.8 6.1 12.7 31.0 Dental
school patients (S)
Hansen & 35 year olds from urbanJohansen (102) 1976 2981 1.5
3.4 46.0 area (N)
General poppulation onlyPetersson et al. premolars were
included(22) 1986 861 4985 5.8* 6.6 3.4 13.0 (S)
Allard & Elderly population fromPalmqvist (23) 1986 183 2567
14.0 9.8 17.6 27.0 rural area (S)
Eckerbom et al. Patients referred for(51) 1987 200 4889 24.4 5.2
13.0 26.4 radiographic survey (S)
Bergstrom et al. Patients visiting their
(25) 1987 250 6593 26.2 3.5 6.5 (root) 28.8 (root) dentist
regularly (S)35 year olds from urban
Eriksen et al. (42) 1988 141 3197 22.7 1.4 3.4 34.0 area (N)
Petersson et al. Patients requiring(26) 1989 567 11497 20.3 8.7
22.2 26.5 substantial dental care (S)
Odesjo et al. (27) 1990 967 17430 18.0 2.9 8.6 24.6 General
population (S)
Eriksen & 50 year-olds from an urbanBjertness (43) 1991 119
2940 24.7 3.5 6.0 36.6 area (N)
66 year-olds from an urbanImfeld (103) 1991 2004 8.0 26.0 31.0
area (CH)
Hlsmann et al.(104) 1991 4845 3.2 60.0 Dental school patients
(D)
De Cleen et al. Patients from oral surgery (28) 1993 184 4196
22.8 6.0 2.3 39.2 (NL)
35 year olds from urbanEriksen et al. (44) 1995 118 3282 27.8
0.6 1.3 38.1 area (N)
Buckley & Patients fromdental schoolSpngberg (33) 1995 208
5272 25.3 4.1 5.5 31.3 (USA)
Dentate old peopleliving atSoikkonen (29) 1995 293 2355 8.0 6.6
21.5 16.0 home (FIN)
Saunders et al. Dental school 20 years-(30) 1997 340 8420 24.8
4.6 5.6 58.1 old (GB)
Patients from private
Weiger et al. (31) 1997 323 7897 24.4 2.7 61.0 surgery 12 years
old (D)Marques et al. 3039 year-olds from an(45) 1998 179 4446 24.8
2.0 1.5 21.7 urban area (P)
Sidaravicius et al. 3544 year-oldsan urban(46) 1999 147 3892
26.5 7.2 15.0 39.4 area (Lith)
De Moor et al. Dental school 18 years(70) 2000 206 4617 22.4 6.6
6.8 40.4 old (B)
Kirkevang et al.(101) 2001 613 15984 28 3.4 4.8 52.2 General
population (DK)
95
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
8/14
Kirkevang & Hrsted-Bindslev
status of root-filled teeth, but not one as pronouncedas Ray
& Trope (75). Kirkevang et al. (47) also foundthat, when the
root-filling and the coronal restoration
were both of high quality, less than one-third of theteeth had
AP, but if both were inadequate, more than
three-quarters of the teeth had AP. If the root-fillingwas
adequate and the coronal restoration was inad-equate, almost half
of the teeth had AP. If, on theother hand, the coronal restoration
was adequate andthe root-filling inadequate, more than two-thirds
had
AP. Tronstad et al. (76) demonstrated that, if theroot-filling
was inadequate, it did not matter whetherthe coronal restoration
was adequate or inadequate;the tooth would still have a poor
prognosis. This wassupported by a study by Ricucci et al. (77)
whichconcluded that the problem of coronal leakage seemsnot to be
of great clinical importance if the instru-mentation and filling of
the root canal was optimised.
The studies indicate that both the quality of theendodontic and
coronal restoration play importantroles in obtaining an efficient
seal of the root canal,even though it is suggested that the quality
of theroot-filling may be the most decisive parameter.
Table 4 Technical quality of root fillings in epidemiological
studies related to the outcome.
Author Year N cases Adequate Inadequate Adequate Short % Long
%roots/ lateral lateral length (success %) (success %)teeth seal %
seal (success %)
(success %) (success %)
Bergenholtz et al. (94) 1973 984R 48.5 51.5 (69) 32 (79) 55.9
(72) 12.1 (63)
Petersson et al. (22) 1986 650T 37.9 (93)* 50.7 11.4 (41)
Eckerbom et al (24) 1987 899R 56.3 43.7 45.7 45.7 9.4
Eriksen et al (42) 1988 79T 68.3 (63) 31.7 (70) 41.0 (86) 43.0
(53) 16.0 (37)
Odesjo et al (27) 1990 1876R 30.2 (78) 69.8 (79) 41.4 (79) 48.5
(85) 10.1 (48)
Eriksen & 1991 141T 73 (73) 27 (29) 32 (77) 48.9 (51) 19.1
(26)
Bjertness (43)
De Cleen et al. (28) 1993 53T 52.8 (43) 43.4 (15) 3.8
(0)Saunders et al. (30) 1997 592T 41.5 (61) 41.5 (45) 17 (43)
Marques et al. (45) 1998 65T 46 (87)** 54 (69)**
Sidaravicius et al. (46) 1999 320T 30.9 (70) 68.8 (63) 33.8 (78)
41.3 (75) 24.7 (30)
De Moor et al. (70) 2000 312T 40.7 (61) 54.2 (25) 2.6 (0)
Kirkevang et al (47) 2000 773T 40.9 (56) 59.1 (42) 60.0 (58)
39.6 (32)***
* No lateral or apical lumen visible.** Adequate lateral and
apical seal
*** Short and long
96
Methods of instrumentation
Instrumentation of the root canal aims to remove allintracanal
soft tissue and to prepare the canal so thatthe canal is aseptic
and a bacteria-tight root-filling can
be made.Numerous instruments and methods have been de- veloped
to attain this objective. Examples includehand instruments of
various metals and design, sonicand ultrasonic instruments, and
engine-driven instru-ments of different design and materials, which
oper-ate with different movements. Each instrument hasto be used in
combination with an irrigation solutionin order to flush tissue
remnants, dentine shavingsand microbiological elements out of the
canal. Appar-ently, no instrument or method for cleaning andshaping
available for the clinician can, in all situations,entirely remove
tissue remnants from the canal lu-mina and debris smeared on the
canal wall (7882).This is not surprising if the often very
irregular canalconfiguration is taken into consideration (Fig.2).
Asan example, the recently introduced Ni-Ti instru-ments may follow
the curvature of the canal more
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
9/14
Technical aspects
precisely than stainless steel instruments but thecleaning
effect is comparable to stainless steel instru-ments (83, 84).
Furthermore, if the cleaning efficacyis measured as reduction of
bacteria in the canal afteruse of either Ni-Ti instruments or
stainless steel in-
struments, no difference has been found (85). Apparently, only
few clinical and radiographicalstudies have evaluated the effect of
specific instru-ments on the outcome of endodontic treatment.
Theproblem may be that among the numerous factorsinvolved, such as
preoperative diagnosis, root canalmorphology, aseptic treatment
regimen, irrigationsolution, quality of root-filling and skill of
the oper-ator, it is rather difficult to single out the effect of
aspecific instrument or a specific cleaning and shapingmethod.
However, the results from a recent retro-spective study is in
accordance with the findings from
various experimental laboratory studies, which gener-ally show
only small differences among currentmethods of instrumentation.
Therefore, Peters et al.(86) did not find differences in treatment
outcomeafter use of two different Ni-Ti rotating systems in astudy
where the same root-filling method was used inboth groups.
Overinstrumentation
Overinstrumentation may happen at any stage of in-strumentation.
Provided aseptic conditions are main-tained, it induces a sterile
trauma to the periapicaltissue and the healing potential is good.
An experi-mental study showed that removal of the entire vitalpulp
and a slight periapical overinstrumentation, fol-
Fig.2. Cleared teeth demonstrating the irregularity of theroot
canal system (courtesy of Dr Chr. Stock).
97
lowed by termination of the root-filling some milli-metres from
the radiographical apex, did not causepersistent inflammation of
the tissue in the residualroot canal or in the periapical tissue
(87). In the apicalpart of the canal, a loosely arranged
granulation tissue
was formed and resorption of the canal walls was after36months
followed by a cell-rich fibrous tissue andapposition of hard tissue
on the walls (Fig.3). How-ever, gross overinstrumentation in vital
and necroticcases, and packing or extrusion of infected
dentindebris and pulp remnants, induces periapical inflam-mation
and may, therefore, be of prognostic import-ance (8890). Thus,
dentin chips have been found inperiapical granulomas from cases of
failed root canaltreatments (91), and Bergenholtz et al. (18) found
a
Fig. 3. Microphotograph of decalcified human root. Sixmonths
previously, the entire pulp was removed, followedby root-filling
about 3mm short of the radiographic apex.A slight accumulation of
lymphocytes is seen adjacent to aplug of dentin particles and
remnants of the root canalsealer (Rf.). The apical part of the pulp
canal is occupiedby a cell rich fibrous connective tissue and a
considerabledeposition of hard tissue is seen onto the canal
walls.
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
10/14
Kirkevang & Hrsted-Bindslev
higher frequency of periapical lesions in roots
withoverinstrumentation in comparison to cases with
nooverinstrumentation.
Overinstrumentation, defined as an excessive re-moval of the
canal wall, may lead to weakening of
the root and lateral perforations, especially in curvedcanals.
Lateral perforations are a negative prognosticfactor, either
because the main canal cannot be instru-mented or because of an
overfilling of the perforation(17, 92).
Methods of root-filling
Like materials and methods for instrumentation, anabundant
number of root-filling methods are avail-able for the clinician.
Numerous laboratory studieshave been performed to demonstrate the
sealabilityof the various obturation methods and to comparethe
different methods(e.g. 93). In the 1990 volumesof two major
endodontic journals, there was aboutone in every four of the
scientific articles were leakagestudies (93).
Dye penetration tests are most commonly used.These tests are
based on the philosophy that the dyemimics in size microorganisms
metabolic products,and either penetrate along the root-filling
materialand the root canal wall or along confluencing voidsin the
filling, reflecting a risk that bacteria may multi-ply in these
lacunae and a periapical inflammation willdevelop or be
maintained.
However, the methodology used in many of thesedye penetration
tests has been questioned (9395).Therefore, it has been claimed
that air entrapped inroot-fillings must be removed by vacuum before
test-ing apical dye penetration in order to get a
reliableimpression of leakage (94). In addition, other
meth-odological problems, such as the pH of the dye and
whether leakage is evaluated in cross-sections of obtu-rated
root canals or in cleared roots or whether dye
penetration should be measured linearly or
spectro-photometrically, have to be considered (93, 96).
Ad-ditional factors are tooth anatomy and root canal
con-figuration, instrumentation, type of sealer and fillingmaterial
and the skill of the operator.
A fundamental question is how well the outcomeof the endodontic
treatment correlates with leakagedemonstrated microscopically in
the laboratory. Oliv-ier and Abbott (97) studied apical dye
penetration in116 extracted teeth root filled more than 6months
98
prior to extraction. Any teeth with canals not filled within
2.0mm of the apical foramen were excludedfrom the study. They found
a significant differencebetween the successful and the unsuccessful
groups,
with a mean percentage linear dye penetration being
greater in the unsuccessful specimens. But apical dyepenetration
was observed in all but one tooth. Thus,the clinical implications
of leakage found in the lab-oratory should be viewed with some
caution. Leakageis only one factor characterizing root-filling
tech-niques.
Guttapercha is part of all contemporary root-fillingmaterials.
Guttapercha is used with a solid core ora softened core technique
and both methods implyadditional use of a sealer.
The cold lateral compaction guttapercha techniquemay be seen as
the classical root-filling methodagainst which other methods are
tested in the labora-tory. The technique or slight variations of
the tech-
Fig.4. Excess of root-filling material following use of thewarm
guttapercha core carrier technique.
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
11/14
Technical aspects
nique has been used in many of the longitudinalstudies on
outcome of endodontic treatments. In or-der to improve the
sealability and to form a morehomogeneous root-filling, several
techniques usingsoftened guttapercha have been developed. The
warm
vertical technique was first introduced by Schilder(98) and has
gained wide acceptance. Later manyvariations of this technique have
been introduced. Aguttapercha-condensing instrument may be
heatedoutside the canal, or the guttapercha may be intro-duced in
the canal after being heated. In some ofthese systems the
temperature of the guttapercha orcondenser rises to about 200c
which decreases toabout 70c when introduced in the canal. In a
labora-tory setting, this temperature increases the
surfacetemperature of the root more than 10C which isconsidered
harmful to the periodontal membrane andmay cause external
resorptions (99). Thus, an animalstudy showed external root
resorption after thermo-mechanical compaction of guttapercha
(100).
The advocates of the various warm techniques claimto make
root-fillings in three dimensions, but due tothe pressure applied
to achieve this, surplus of ma-terial is a common finding (Fig.4),
the effect of whichhas been addressed above. In the clinic, the
relativeperformance of any of these plasticized techniques
incomparison to the cold lateral condensation tech-nique has not
been shown. Even root-fillings with asingle point technique and
sealer, which in several invitro studies have shown substantial
leakage and
which in general has been abandoned by endodonticspecialists,
has not shown inferior results in the clinic(62).
It can thus be concluded that, even though there isno doubt that
sealability is of great importance, asdemonstrated in longitudinal
studies, the importanceof differences in microsealability as found
in the lab-oratory should not be over-emphasized. It must
berealised that the outcome of endodontic treatment
depends on a multitude of factors, and no method offilling can
boast superior clinical documentation.
Concluding remarks
Despite the differences in defining the radiographicquality
parameters of the root-filling, the rather lowreproducibility for
some of them and the differencein thresholds used to categorise
root-fillings as ade-quate or inadequate, the studies have
demonstrated
99
that there is an association between the quality of
theroot-filling and the periapical status. All studies haveagreed
that AP is more frequent in teeth with inad-equate root-fillings
than in teeth with adequate root-fillings. Furthermore, studies
have indicated that the
quality of the coronal restoration may be related tothe outcome
of root canal treatment.Longitudinal studies have demonstrated that
it is
possible to control and cure AP. Ideally, this wouldbe reflected
in cross-sectional studies of general popu-lations. This is not the
case, however. On the con-trary, it seems that the present methods
of performingroot canal therapy is not ideal when performed
ingeneral practice. General dentists do not succeed inpreventing or
curing AP as demonstrated by thecross-sectional studies on
periapical and endodonticstatus that demonstrate high rates of AP
in root-filledteeth. It is therefore essential that efforts should
bemade to optimise the treatment of teeth with pulpalor periapical
infection, and that endodontic treatmentstrategies should be
brought into focus in the plan-ning of future under- and
postgraduate education.Several technical aspects of treatment are
not easilytraceable in radiographs and do not lend themselveseasily
to cross-sectional or epidemiological investi-gations. While
specific methods of instrumentationand filling have been ardently
promoted, based onlaboratory studies of efficacy, few if any
clinical dataare available in support of superiority.
Well-designedand targeted clinical studies are needed for
assessmentof clinical performance.
References1. Kakehashi S, Stanley HR, Fitzgerald RJ. The effects
of sur-
gical exposures of dental pulps in germ-free and conven-tional
laboratory rats. Oral Surg Oral Med Oral Pathol,1965: 20:
340349.
2. Sundqvist G. Bacteriological studies of necrotic pulps.
Thesis. Ume, Sweden 1976.3. Mller JR, Fabricius L, Dahlen G,
hman AE, HeydenG. Influence on periapical tissues of indigenous
oral bac-teria and necrotic pulp tissues in monkeys. Scand J
DentRes, 1981: 89: 475484.
4. Sundqvist G, Figdor D. Endodontic treatment of
apicalperiodontitis. In: Essential Endodontology(Ed. rstavik,
D,Pitt Ford, TR). Blackwell Science Ltd, 1998: pp 242269.
5. Hummonen S, rstavik D. Radiological aspects of
apicalperiodontitis. Endodontic Topics, 2002: 1: 325.
6. Eckerbom M, Magnusson T, Martinsson T. Reasons forand
incidence of tooth mortality in a Swedish population.Endod Dent
Traumatol, 1992: 8: 230234.
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
12/14
Kirkevang & Hrsted-Bindslev
7. Morita M, Kimura T, Kanegae M, Ishikawa A, WatanabeT. Reasons
for extraction of permanent teeth in Japan.Community Dent Oral
Epidemiol, 1994: 22: 303306.
8. Angelillo IF, Nobile CG, Pavia M. Survey of reasons
forextraction of permanent teeth in Italy. Community DentOral
Epidemiol, 1998: 24: 336340.
9. Haddad I, Haddadin K, Jebrin S. Maani M, Yassin O.
Reasons for extractions of permanent teeth in Jordan. IntDent J,
1999: 49: 343436.
10. Trovik TA, Klock KS, Haugejorden O. Trends in reasonsfor
tooth extractions in Norway from. To 1998 ActaOdontol Scand, 1968:
58: 8996.
11. Chestnutt IG, Binnie VI, Taylor MM. Reasons for
toothextractions in Scotland. J Dent, 2000: 28: 295297.
12. Rothman KJ, Greenland S. Causation and causal inference.In:
Modern Epidemiology (Ed. by by Rothman, KJ,Greenland, S).
Lippincott Raven, 1998: pp 728.
13. MacMahon B, Trichopoulos D. Concepts of cause.
In:Epidemiology. Principles and Methods(Ed. by by MacMa-hon, B,
Trichopoulos, D). Little, Brown, 2nd edn., 1996:pp 1926.
14. Strindberg LZ. The dependence of the results of pulp
ther-apy on certain factors. An analytic study based on
radio-graphic and clinical follow-up examinations. Thesis.
ActaOdontol Scand., 1956: 14 (Suppl 21).
15. Grahnen H, Hansson L. The prognosis of pulp and rootcanal
therapy. A clinical and radiolographic follow-up ex-amination.
Odontol Revy, 1961: 12: 146165.
16. Harty FJ, Parkins BJ, Wengraf AM. Success rates in rootcanal
therapy. A retrospective study of conventional cases.Br Dent J,
1970: 128: 6570.
17. Kerekes K, Tronstad L. Long-term results of
endodontictreatment performed with a standardized technique. J
En-dod, 1979: 5: 8390.
18. Bergenholtz G, Lekholm U, Milthon R, Engstrm B. In-fluence
of apical overinstrumentation and overfilling on re-treated root
canals. J Endod, 1979: 5: 310314.
19. Sjgren U, Hgglund B, Sundqvist G, Wing K. Factorsaffecting
the long-term results of endodontic treatment. JEndod, 1990: 16:
498504.
20. Smith CS, Setchell DJ, Harty FJ. Factors influencing
thesuccess of conventional root canal therapy-a
five-yearretrospective study. Int Endod J, 1993: 26: 321333.
21. Sjgren U, Figdor D, Persson S, Sundqvist G. Influenceof
infection at the time of root filling on the outcome ofendodontic
treatment of teeth with apical periodontitis.Int Endod J, 1997: 30:
297306.
22. Petersson K, Petersson A, Olsson B, Hkansson J,Wennberg A.
Technical quality of root fillings in an adultSwedish population.
Endod Dent Traumatol, 1986: 2: 99102.
23. Allard U, Palmqvist S. A radiographic survey of
periapicalconditions in elderly people in a Swedish country
popula-tion. Endod Dent Traumatol, 1986: 2: 103108.
24. Eckerbom M, Andersson JE, Magnusson T. Frequencyand
technical standard of endodontic treatment in a Swed-ish
population. Endod Dent Traumatol, 1987: 3: 245248.
25. Bergstrm J, Eliasson S, Ahlberg KF. Periapical status
insubjects with regular dental care habits. Community DentOral
Epidemiol, 1987: 15: 236239.
100
26. Petersson K, Lewin B, Hkansson J, Olsson B, WennbergA.
Endodontic status and suggested treatment in a popula-tion
requiring substantial dental care. Endod DentTraumatol, 1989: 5:
153158.
27. desj B, Hellden L, Salonen L, Langeland K. Prevalenceof
previous endodontic treat-ment, technical standard andoccurrence of
periapical lesions in a randomly selected
adult, general population. Endod Dent Traumatol., 1990:6.
2265272.
28. De Cleen MJH, Schuurs AHB, Wesselink PR, Wu MK.Periapical
status and prevalence of endodontic treatmentin an adult Dutch
population. Int Endod J, 1993: 26: 112119.
29. Soikkonen KT. Endodontically treated teeth and
periapicalfindings in the elderly. Int Endod J, 1995: 28:
200203.
30. Saunders WP, Saunders EM, Sadiq J, Cruickshank E. Tech-nical
standard of root canal treatment in an adult
Scottishsub-population. Br Dent J, 1997: 182: 382386.
31. Weiger R, Hitzler S, Hermle G, Lst C. Periapical
status,quality of root canal fillings and estimated
endodontictreatment needs in an urban German population. EndodDent
Traumatol, 1997: 13: 6974.
32. Bergenholtz G, Malmcrona E, Milthon R. Endodontiskbehandling
och periapikalstatus. I. Rntgenologiskunderskning av frekvensen
endodontiskt behandladetnder och frekvensen periapikala
destruktioner. Tandlk-artidningen, 1973: 2: 2001 Bergenholtz G,
MalmcronaE, Milthon R. Endodontisk behandling och
periapikal-status. II. Rntgenologisk bedmning av
rotfyllningenskvalitet stlld i relation till frekomst av
periapikala de-struktioner. Tandlkartidningen 1973; 5: 269279.
33. Buckley M, Spngberg LSW. The prevalence and technicalquality
of endodontic treatment in an American subpopu-lation. Oral Surg
Oral Med Oral Pathol, 1995: 79: 92100.
34. Brynolf I. A histological and roentgenological study of
theperiapical region of human upper incisors. Thesis. OdontolRev,
1967: 18 (Suppl 1)1.
35. rstavik D, Kerekes K, Eriksen HM. The periapical index:a
scoring system for radio-graphic assessment of apical
peri-odontitis. Endod Dent Traumatol, 1986: 2: 2034.
36. rstavik D. Reliability of the periapical index scoring
sys-tem. Scand J Dent Res, 1988: 96: 108111.
37. rstavik D, Hrsted-Bindslev P. A comparison of endo-dontic
treatment results at two dental schools. Int Endod
J, 1993: 26: 348354.38. rstavik D. Time-course and risk analyses
of the develop-
ment and healing of chronic apical periodontitis in man.Int
Endod J, 1996: 29: 2006
39. Valderhaug J, Jokstad A, Ambjornsen E, Norheim PW.
As-sessment of the periapical and clinical status of
crownedteethover 25 years. J Dent, 1997: 25: 97105.
40. Trope M, Delano EO, rstavik D. Endodontic treatmentof teeth
with apical perio-dontitis: single vs. multivisittreatment. J
Endod, 1999: 25: 345350.
41. Waltimo TM, Boiesen J, Eriksen HM, rstavik D.
Clinicalperformance of 3 endodontic sealers. Oral Surg Oral MedOral
Pathol Oral Radiol Endod, 2001: 92: 8992.
42. Eriksen HM, Bjertness E, rstavik D. Prevalence and qual-ity
of endodontic treatment in an urban adult populationin Norway.
Endod Dent Traumatol, 1988: 4: 122126.
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
13/14
Technical aspects
43. Eriksen HM, Bjertness E. Prevalence of apical peri-odontitis
and results of endodontic treatment in middle-aged adults in
Norway. Endod Dent Traumatol, 1991: 7:1 4.
44. Eriksen HM, Berset GP, Hansen BF, Bjertness E. Changesin
endodontic status among 35-Year-Olds Oslo. NorwayInt Endod J 1995,
197393: 28: 129132.
45. Marques MD, Moreira B, Eriksen HM. Prevalence of api-cal
periodontitis and results of endodontic treatment in anadult,
Portuguese population. Int Endod J, 1998: 31:161165.
46. Sidaravicius B, Aleksejuniene J, Eriksen HM.
Endodontictreatment and prevalence of apical periodontitis in an
adultpopulation of Vilnius. Lithuania Endod Dent Traumatol,1999:
15: 210215.
47. Kirkevang L-L, rstavik D, Hrsted-Bindslev P, WenzelA.
Periapical status and quality of root fillings and
coronalrestorations in a Danish population. Int Endod J, 2000:33:
509515.
49. White SC, Pharoah MJ. Intraoral radiographic examina-tions.
In: Oral Radiology. Principles and Interpretation
(Ed. by by White, SC, Pharoah, MJ), 4th edn. Mosby1999.
50. Molven O. The frequency, technical standard and resultsof
endodontic therapy. Thesis. Bergen, Norway 1974.
51. Eckerbom M, Andersson JE, Magnusson T.
Interobservervariations in radiographic examination of endodontic
vari-ables. Endod Dent Traumatol, 1986: 2: 243246.
52. Eckerbom M, Magnusson T. Evaluation of technical qual-ity of
endodontic treatment reliability of intraoral radio-graphs. Endod
Dent Traumatol, 1997: 13: 259264.
53. Helminen SE, Vehkalahti M, Kerosuo E, Murtomaa H.Quality
evaluation of process of root canal treatments per-formed on young
adults in Finnish public oral health ser-vice. J Dent, 2000: 28:
227230.
54. Reit C, Hollender L. Radiographic evaluation of endodon-tic
therapy and the influence of observer variation. ScandJ Dent Res,
1983: 91: 205212.
55. Lambrianidis T. Observer variations in radiographic
evalu-ation of endodontic therapy. Endod Dent Traumatol,1985: 1:
235241.
56. Goldman M, Pearson AH, Darzenta N. Endodontic suc-cess-Whos
reading the radio-graph? Oral Surg, 1972: 33:432437.
57. Reit C, Grndahl H-G. Application of statistical
decisiontheory to radiographic dia-gnosis of endodontically
treatedteeth. Scand J Dent Res, 1983: 91: 213218.
58. Halse A, Molven O. A strategy for the diagnosis of
peri-apical pathosis. J Endod, 1986: 12: 2002 Hansen BF,
Johansen JR. Oral roentgenologic findings in a Norwegianurban
population. Oral Surg Oral Medical Oral Pathol1976; 41: 261626.
58. Heling B, Tamshe A. Evaluation of the success of
endo-dontically treated teeth. Oral Surg, 1970: 30: 533536.
59. Heling B, Shapira J. Roentgenologic and clinical evalu-ation
of endodontically treated teeth, with or withoutnegative culture.
Quintessence Int, 1978: 11: 7984.
59. Reit C. On decision making in endodontics. Thesis. Gte-borg,
Sweden 1986.
60. Friedman S, Lst C, Zarrabian M, Trope M. Evaluation
ofsuccess and failure after endodontic therapy using a glassionomer
cement sealer. J Endod, 1995: 21: 384390.
101
61. Caliskan MK, Sen BH. Endodontic treatment of teeth
withapical periodontitis using calcium hydroide: a long-termstudy.
Endod Dent Traumatol, 1996: 12: 215221.
62. Friedman S. Treatment outcome and prognosis of endo-dontic
therapy. In: Essential Endodontology (Ed. by by Drstavik, T R Pitt
Ford). Blackwell Science Ltd, 1998: pp367401.
63. Ricucci D. Apical limit of root canal instrumentation
andobturation, part 1. Literature review. Int Endod J, 1998:31:
384393.
63. Swartz DB, Skidmore AE, Griffin JA. Twenty years of
en-dodontic success and failure. J Endod, 1983: 9: 198202.
64. Bystrm A, Happonen R-P, Sjgren U, Sundquist G.Healing of
periapical lesions of pulpless teeth after endo-dontic treatment
with controlled asepsis. Endod DentTraumatol, 1987: 3: 25863.
64. Nygaard-stby B. ber die Gewebsvernderungen im api-kalen
Paradentium des Menschen nach verschiedenartigenEingriffen in den
Wurzelkanlen. Eine klinische rntgenol-ogische und
histo-patologische Studie. Skrifter utgitt avDet Norske
Videnskaps-Akademi i Oslo., 1939: 1223.
65. Ketterl W. Kriterien fr den Erfolg der Vitalextirpation.DDZ,
1965: 20: 2005
66. Hrsted P. Studies on the root filling cement bi-oxol.
Aclinical, roentgenological and histological investigation.
Acta Odont Scand, 1972: 30: 187199.67. Weiger R, Axmann-Krcmar
D, Lst C. Prognosis of con-
ventional root canal treatment reconsidered. Endod
DentTraumatol, 1998: 14: 1 9.
68. Kaplan EL, Meier P. Nonparametric estimation from
in-complete observations. J Am Stat Ass, 1958: 53: 457481.
69. Bergenholtz G, Lekholm U, Milthon R, Heden G, desjB, Engstrm
B. Retreatment of endodontic fillings. Scand
J Dent Res, 1979: 87: 217224.70. De Moor RJG, Hommez GMG, De
Boever JG, Delme
KIM, Martens GEI. Periapical health related to the qualityof
root canal treatment in a Belgian population. Int EndodJ, 2000: 33:
113120.
71. Ray HA, Trope M. Periapical status of endodonticallytreated
teeth in relation to the technical quality of the rootfilling and
the coronal restoration. Int Endod J, 1995: 28:1218.
72. Tronstad L, Asbjrnsen K, Dving L, Pedersen I, EriksenHM.
Influence of coronal restorations on the periapicalhealth of
endodontically treated teeth. Endod Dent Trau-Matol, 2000: 16:
218221.
73. Ricucci D, Grndahl K, Bergenholtz G. Periapical statusof
root-filled teeth exposed to the oral environment by lossof
restoration or caries. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod, 2000: 90: 354359.74. .Turek T, Langeland K. A
light microscopic study of theefficacy of the telescopic and the
Giromatic preparation ofroot canals. J Endod., 1982: 8: 437443.
75. Langeland K, Liao KKS, Pascon EA. Work-saving devicesin
endodontics: Efficacy of sonic and ultrasonic tech-niques. J Endod,
1985: 11: 499510.
76. Sen BH, Wesselink PR, Trkn M. The smear layer: a phe-nomenon
in root canal therapy. Int Endod J, 1995: 28:141148.
77. Heard F, Walton RE. Scanning electron microscope
studycomparing four root canal preparation techniques in
smallcurved canals. Int Endod J, 1997: 30: 323331.
-
8/6/2019 ,DanaInfo=Www.blackwell Synergy.com%2Bj.1601
1546.2002.20106
14/14
Kirkevang & Hrsted-Bindslev
78. Peters OA, Laib A, Ghring TN, Barbakow F. Changesin root
canal geometry after preparation assessed by high-resolution
computed tomography. J Endod, 2001: 27: 16.
79. Schfer E, Zapke K. Effizienz maschineller
Wurzelkanal-aufbereitungssysteme im Vergleich zur manuellen
Instru-mentierung. Quintessenz, 2000: 51: 115124.
80. Gluskin AH, Brown DC, Buchanan LS. A
reconstructedcomputerized tomographic comparison of Ni-Ti
rotaryGTTM files versus traditional instruments in canals shapedby
novice operators. Int Endod J, 2002: 34: 476484.
81. Dalton BC, rstavik D, Phillips C, Pettiette M, Trope
M.Bacterial reduction with nickel-titanium rotary instrumen-tation.
J Endod, 1998: 24: 763767.
82. Peters CI, Barbakow F, Peters OA. Rotary root canal
prep-aration. Preliminary retrospective analysis of 268
clinicalcases and 661 roots. Munich: European Soc Endodontol
Ab-stract No O: 36: 13.
83. Hrsted P, Nygaard-stby B. Tissue formation in the rootcanal
after total pulpectomy and partial root filling. OralSurg Oral Med
Oral Pathol, 1978: 46: 2003
84. Seltzer S, Soltanoff W, Sinai I, Goldenberg A, Bender
IB.Biologic aspects of endodontics. Part III. Periapical
tissuereactions to root canal instrumentation. Oral Surg OralMed
Oral Pathol, 1968: 26: 694705.
85. Nygaard-stby B, Hjortdal O. Tissue formation in theroot
canal following pulp removal. Scand J Dent Res,1971: 79:
333349.
86. Holland R, De Souza V, Nery MJ, de Mello W, BernabePFE,
Otoboni Filho JA. Tissue reactions following apicalplugging of the
root canal with infected dentin chips. OralSurg Oral Med Oral
Pathol, 1990: 49: 366369.
87. Yusuf H. The significance of the presence of foreign
ma-terial periapically as a cause of failure of root treatment.Oral
Surg Oral Med Oral Pathol, 1982: 54: 566574.
88. Ingle JI, Beveridge EE, Glick DH, Weichman JA.
Modernendodontic therapy. In: Ingle, JI, Bakland, LK ., eds.
En-dodontics, 4th edn. Baltimore: Williams & Wilkins., 1994:p
152.
89. Wu M-K, Wesselink PR. Endodontic leakage studies
re-considered. part I. Methodology, application and rel-evance. Int
Endod J, 1993: 26: 3743.
102
90. Goldman M, Simmonds S, Rush R. The usefulness of
dyepenetration studies re-examined Oral Surg Oral MedicalOral
Pathol. 1989: 67: 327332.
91. Spangberg LSW, Achierno TV, Cha B. Influence of en-trapped
air on the accuracy of leakage studies using dyepenetration
methods. J Endod, 1989: 15: 548551.
92. Tamse A, Katz A, Kablan F. Comparison of apical leakage
shown by four different dyes with two evaluating methods.Int
Endod J, 1998: 31: 333337.
93. Oliver CM, Abbott PV. Correlation between clinical suc-cess
and apical dye penetration. Int Endod J, 2001: 34:637644.
94. .Schilder H. Filling root canals in three dimensions.
DentClin N Am., 1967: 723.
95. Silver GK, Love RM, Purton DG. Comparison of two ver-tical
condensation obturation techniques: Touch n Heatmodified and System
B. Int Endod J, 1999: 32: 287295.
96. Saunders EM. In vivo findings associated with heat
gener-ation during thermomechanical compaction of gutta-per-cha.
Part II. Histological response to temperature elev-ation on the
external surface of the root. Int Endod J,
1990: 23: 268274.97. Bergenholtz G, Malmcrona E, Milthon R.
Endodontisk
behandling och periapikalstatus. II. Rogntgenologisk be-domning
av roftyllningens kvalitet stalld i relation till fore-komst av
periapikala destruktioner. Tandlakartidningen,1973; 5: 267279.
98. Hansen BF, Johansen JR. Oral roentgenologic findings ina
Norwegian urban population. Oral Surg Oral Med OralPathol, 1976;
41: 261626
99. Imfeld TN. Prevalence and quality of endodontic treat-ment
in an elderly urban population of Switzerland. J En-dod, 1991; 17:
604607
100. Hulsmann M, Lorch V, Franz B. Untersuchung zur Hau-figkeit
und Qualitat von Wurzelfullungen: eine Auswer-
tung von Orthopantomogrammen. Dtsch Zahnartzl Z,1991; 46:
296299.
101.Kirkevang LL, Horsted-Bindslev P, Orstavik D, Wenzel
A.Frequency and distribution of endodontically treated teethand
apical periodontitis in an urban Danish population. IntEndod J,
2001; 34: 198205