-
8/10/2019 Damage Control Surgery Ocular Traumatology
(Injury)
1/7
Damage control surgery in ocular traumatology
Ferenc Kuhna,*,#1, Zlatko Slezakbb,#2
aDepartment of Clinical Ophthalmology, University of Alabama at
Birmingham, 1201 11th Avenue South,
Suite 300 Birmingham, AL 35205, USAbDepartment of Ophthalmology,
City Hospital, Varaszin, Croatia
Introduction
Although the eyes represent only 0.1% of the totalbody surface,
they are disproportionally commonlyinvolved in trauma. Part of this
is due to theirvulnerability and the importance of
visionhumansreceive 70%90% of their information about theoutside
world through their eyesbut lifestylechanges (e.g. do-it-yourself
home repairs) alsobring new risks. A good example is warfare
trauma:the proportion of eye involvement among all inju-ries has
shown a steady increase from 1.76% in the
Crimean War (18541856) to 13% in OperationDesert Storm in
1991.2
Instinctively, the ophthalmologist wants torestore the injured
globe to its normal conditionas soon as possible. However, to
achieve the mostoptimal outcome, the treatment must be based on
arational, planned approach. The concept of damagecontrol surgery
means that management of thedeadly triad of coagulopathy, acidosis,
andhypothermia, or other life-threatening conditionstakes
precedence over treatment of the eye injuryin the patient with
polytrauma. This alone mayforce the ophthalmologist to design an
approachin stages, deferring nonemergency interventions.Delayed
surgery also may result from nonrecogni-tion of an eye injury
during the struggle to keep thepatient alive.
Although the concept of damage control surgeryis relatively new,
it has been practiced by ophthal-mologists for decades. While there
is no one-to-oneequivalent to the deadly triad in the eye, a host
of
Injury, Int. J. Care Injured (2004) 35, 690696
KEYWORDS
Damage control surgery;
Ocular traumatology;
Visual rehabilitation
Summary There seems to be no decrease in the incidence of
serious eye injuries.Although recent developments in technology now
allow salvage of eyes that would havebeen lost only a few years
ago, certain rules must be followed to achieve optimaloutcome.
Damage control surgery in ocular traumatology means that the
ophthalmol-ogist understands that eye injuries must be treated only
after life-threatening con-ditions have been properly addressed by
other specialists. Focusing on the injured eye,the ophthalmologist
evaluates the types and severity of the trauma, and designs
amanagement plan. Wounds should be cleaned and closed, infections
treated andprevented, the retina reattached; however, conditions
that do not require immediateintervention are usually better
treated following a few days of delay, during whichintense
corticosteroid therapy is administered. The second, reconstructive
surgery istypically performed 710 days postinjury, when the risk of
intraoperative haemor-rhage is dramatically reduced and the chance
of visual rehabilitation is higher.
2004 Elsevier Ltd. All rights reserved.
*Corresponding author. Tel.: 1-205-558-2588;fax:
1-205-933-1341.
E-mail address:[email protected] (F. Kuhn).#1Executive Vice
President, International Society of Ocular
Trauma; President, American Society of Ocular Trauma;Director of
Clinical Research, Helen Keller Foundation forResearch and
Education; Professor of Ophthalmology, Universityof Pecs,
Hungary.
#2President, Croatian Eye Injury Registry.
00201383/$ see front matter 2004 Elsevier Ltd. All rights
reserved.doi:10.1016/j.injury.2004.03.008
-
8/10/2019 Damage Control Surgery Ocular Traumatology
(Injury)
2/7
other factors makes it necessary to at least consider
planning a staged, rather than an all-in-one
approach, treating certain pathologies early while
deferring surgery for others.
Repair of a seriously injured eye should not be
attempted unless the physician understands the
anatomy, physiology, and pathophysiology of theglobe; can
properly classify the injury; and knows
what unique features each injury type has. Based on
these, a proper management plan is to be developed
and then executed.
Functional anatomy of the human eye
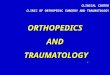
The eye (Fig. 1) has three coats; of these, violation
of the external coat is the most important clinically.
The external coat consists of the cornea in the front
and the sclera in the back. The cornea is a trans-
parent tissue of 12 mm in diameter, serving as the
window of the eyeand as its primary refractivepower. The sclera,
covered by the conjunctiva, is a
nontransparent, white tissue, providing much of the
eyes structural support. The transition ringbetween the cornea
and sclera is the limbus.
Themiddle coat, theuvea,has three components.
The most posterior part, the choroid, provides the
blood supply for much of the eye. The tissue anterior
to it, the ciliary body, produces a clear liquid
(aqueous), which is necessary to maintain the in-
traocular pressure (IOP) and the shape/size of the
eye. Extended periods of elevated (glaucoma) or
decreased (hypotony, eventually phthysis (globe
shrinkage)) IOP results in permanent visual loss.
The ciliary body also contains the ciliary muscle,regulating the
refractive power of the lens. The iris
is the foremost portion of the uvea, giving each eye
its characteristic colour, and, acting like a camerasshutter,
regulating the amount of incoming light via
the pupil.
The innermost coat is the retina; some of its
characteristics, such as the inability of its nerve
cells to survive for more than a few minutes if
deprived of the normal blood supply, resemble
those of the brain. Unlike its most external layer
(pigment epithelium), the nine inner layers (neu-
roretina) are transparent. The central part of the
retina, the macula, contains a pinhead-sized area,
the fovea, providing fine detail (reading and colour)
vision. A few millimetres medially is the optic disc
(nerve head), an area of 1.5 mm in diameter, the
gateway where blood vessels and roughly 1 million
nerve fibres, transmitting visual information toward
the occipital cortex, pass through.
The neuroretina must be in contact with the
pigment epithelium and the choroid to function
Figure 1 Cross section of the human eye: (1) cornea, (2) sclera,
(3) lens, (4) vitreous, (5) macula, (6) optic disc, (7)
optic nerve.
Damage control surgery in ocular traumatology 691
-
8/10/2019 Damage Control Surgery Ocular Traumatology
(Injury)
3/7
properly; separation (retinal detachment) results in
first temporary, then, unless reattachment soon
follows, permanent blindness. Depending on the
type of retinal detachment (rhegmatogenous: a
break in the retina allows intravitreal fluid to accu-
mulate under the retina; tractional: scar formation
in front of the retina pulls it off; or haemorrhagic:bleeding
underneath the neuroretina), the time to
lose light perception may vary from weeks to years.
Internally the eye has two compartments. Com-
munication between the anterior chamber and the
almost completely transparent vitreous is normally
limited by the lens; if the lens is missing, serious
complications such as new vessel development are
more likely to develop.
Light from the object, refracted by the cornea
and to a lesser extent by the lens, travels through
the vitreous and forms a sharp image on the
retina. Opacity in the visual pathway, whether by
corneal oedema, blood in the anterior chamber
(hyphaema), or vitreous haemorrhage, reduces
vision by preventing light from reaching the retina.
For a person to have full visual capacity, which
involves true depth perception, both eyes must
have good visual acuity, the size of the retinal
images should be nearly identical, the brain has
to perceive and fuse the two images into a single
one, and movements of the two eyes must be
perfectly co-ordinated.
Pathophysiology of the seriouslyinjured eye
The consequences of a mechanical injury can be
classified as follows:
those occurring at the time of injury (physical:
corneal wound, haemorrhage, retinal tear etc.;
chemical: toxicosis; infection (endophthalmitis);
IOP changes, etc.); and
those occurring later (scarring: ciliary body
detachment, proliferative vitreoretinopathy with
retinal detachment etc.; toxicosis). Many other
tissue pathologies (oedema/dislocation/loss/hypo- or
nonfunction) also have to be expected.
Finally, certain abnormalities may enhance
the effect or risk of others: for example, vitreous
haemorrhage increases the incidence and
severityof retinal detachment in eyes with open
wound.3
Terminology: the Birmingham Eye
Trauma Terminology system (BETT)
An injury is either open or closed globe. If the
external coat of the eye has no full-thickness
wound, it is a closed globe injury: lamellar (par-
tial-thickness wound) laceration or contusion.
Within the open globe category (full-thickness
corneal and/or scleral wound), the key is to differ-
entiate between ruptures and lacerations. The
underlying cause of rupture is elevated IOP via
energy transfer from a blunt object. Consequently,
the injury occurs by an inside-out mechanism, and
frequently there is tissue prolapse/extrusion. The
wound is not necessarily at the impact site but
commonly at the locus minoris resistentiae. In case
of laceration, a sharp object creates a wound at the
impact site by an outside-in mechanism. The object
enters the interior eye permanently (intraocular
foreign body, IOFB) or temporarily. In the latter
case, if a single (entrance) wound is present, a
penetrating injury is encountered. If an exit wound
is also present, the injury is perforating. A summary
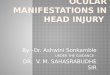
of BETT7 is seen onFig. 2.
Triaging
Eyes with serious injury,6 defined as trauma
resulting in permanent and significant, structural
or functional change to the eye or adnexa, can
be characterised by two important variables:
visual acuity, representing the globes functional
status, and appearance, providing information
albeit unreliableregarding the viability of ana-
tomical reconstruction.Table 1shows a summary
of the possible scenarios based on these two
variables.
Visual acuity allows a rough estimate regarding
functional outcome:
as a general rule, most eyes improve with proper
treatment;
Table 1 The relationship between presenting visual acuity and
the appearance of an injured eye
Appearance Visual acuity
Good Poor
Normal or with minor pathology Common/typical Occasional
Significant pathology Very rare Common/typical
692 F. Kuhn, Z. Slezakb
-
8/10/2019 Damage Control Surgery Ocular Traumatology
(Injury)
4/7
eyes with no light perception initial vision typi-
callyalthough not necessarilyhave poor out-
come;
the worse the initial visual acuity, the worse the
expected outcome;
eyes with good presenting visual acuity uncom-
monly deteriorate.
Based on appearance and evaluation, one of the
following scenarios is possible:
the eye has sustained so severe damage that not
even anatomical reconstruction is possible
(example: large portions of the eyes external
coat and most of its contents are missing);
the eye has sustained so severe damage that even
if anatomical reconstruction is possible, there is
no visual potential (example: loss of the posterior
retina);
the eye shows no or only limited damage yet there
is no visual potential at all or it is extremely
guarded, even with extensive reconstructive
effort (example: severed optic nerve);
the eye has sustained damage that is compatible
with good visual potential if proper reconstruc-
tive surgery is performed (example: vitreous hae-
morrhage and IOFB in retina);
the eye has sustained little damage, requiring no
or only minor surgical intervention and the prog-
nosis is good (example: hyphaema).
Whether and what type of intervention is possible
is determined by the above findings as well as the
patients systemic condition. If at all possible, the
ophthalmologistshould discuss all options with the
patient/family12 and make decisions jointly. The
options are listed inTable 2.
The timing of intervention, as requiredby the concept of damage
control surgery
In eyes with open globe injury, the most immediate
question is the timing of wound closure. An open
wound always risks expulsive haemorrhage, during
which all intraocular contents may be lost and
blindness ensues. The risk depends on patient co-
operation, wound length, and the IOP. Such bleed-
ing is very rare, however, and wound closure is
rarely an emergency indication; usually, the risk
Eye injury
Closed globe Open globe
Rupture
Laceration
Perforating
IOFB
Lamellar
laceration
Contusion
Penetrating
Figure 2 The Birmingham Eye Trauma Terminology system (BETT).
(*) IOFB, intraocular foreign body. The shaded
boxes represent the actual diagnoses used clinically. See the
text for further details.
Damage control surgery in ocular traumatology 693
-
8/10/2019 Damage Control Surgery Ocular Traumatology
(Injury)
5/7
of infection (endophthalmitis) does not measurably
rise if suturing occurs within the first 2414 to 361
hours. Before a decision to perform immediate
wound closure is made, it must be carefullyweighed whether the
proper expertise, experience,
equipment, and operating room personnel are
available.
An equally important question is the timing of
comprehensive reconstruction; this is more urgent
in eyes with open wound: surgery on contused eyes
can often be delayed or may not be necessary at all.
Exceptions include eyes with medically uncontrol-
lable, high IOP due to hyphaema or swollen lens, or
retinal detachment.
In eyes with open globe injury, comprehensive
reconstruction may be performed:
(1) at the time of wound closure;9
(2) early: within thefirst 72 h;5
(3) within thefirst 2 weeks;
(4) several weeks/months postinjury.
Of these four options, the fourth is rarely
employed since the risk of serious complications
due to scarring are significantly higher4 and may
lead to irreparable damage. The second option does
not offer measurable advantages over the third; the
real choice is between performing comprehensive
reconstruction at the time of wound closure versus
at around days 710 postinjury. The following fac-
tors determine the decision-making.
Injury type. Perforating injuries require asearly as possible
vitrectomy to prevent traction
retinal detachment development; this should
be balanced against the risk of exit wound
reopening.
Wound length. Longer wounds require suturing
earlier.
Infection. A crucial factor in damage control sur-
gery: high risk injuries require immediate inter-
vention, even if conditions are otherwise
suboptimal.
The risk of choroidal haemorrhage. The most
crucial factor in damage control surgery: the
earlier the intervention, the higher the risk that
uncontrollable bleeding occurs; delaying the
reconstructive surgery a few days and using heavy
topical, even systemic, corticosteroid therapy
dramatically reduce the risk.
Visibility. For a few days after suturing a central
wound, the cornea is less transparent than at the
time of wound closure; if early need for posterior
segment surgery is expected in such an eye,
immediate reconstruction should be considered.
The presence of choroidal haemorrhage. It can
make posterior segment surgery more difficult; in
Table 2 Management options based on the initial findings
following serious eye injurya
Finding at presentation Option(s)
Eye has no light perception vision Perform anatomical
reconstruction. Function may improve,
but even if it does not, the patient keeps own eye
Leave eye as is, except wound closure. The unreconstructed
eye will probably become phthysical eventually
Remove eye (enucleation). Permanent blindness with
psychological and cosmetical implications results, but
sympathetic ophthalmia (an inflammation following injury
or surgery that threatens the fellow eye) is prevented
Eye has sustained so severe damage that not
even anatomical reconstruction is possible
Enucleation
Eye has sustained so severe damage that
even if anatomical reconstruction is possible,
the eye has no visual potential
Perform anatomical reconstruction
Leave eye as is, except wound closure
Enucleation
Eye has sustained relatively limited anatomical
damage yet there is no visual potential at all
or it is extremely guarded
Perform anatomical reconstruction
Eye has sustained anatomical damage that is
compatible with good visual potential if proper
reconstructive surgery is performed
Perform anatomical reconstruction as necessary
Eye has sustained relatively minor anatomical
damage that requires no or only minor
surgical intervention
Perform anatomical reconstruction if necessary
a The options are listed in the order of preference. See the
text for more details.
694 F. Kuhn, Z. Slezakb
-
8/10/2019 Damage Control Surgery Ocular Traumatology
(Injury)
6/7
such cases, delaying the operation may have more
advantages than early intervention.
Retinal detachment. It is rarely present at the
time of wound closure or the surgeon may not be
aware of its occurrence; if retinal detachment is
known to be present, the surgeon is more
tempted to repair it at the time of wound closure. Posterior
vitreous detachment. Long considered
as a reason to delay the intervention in hopes of
spontaneous hyaloid separation occurring within
a few days postinjury, the condition of the poster-
ior vitreousisnot a proven factor in timing con-
siderations.10
Expertise and equipment. The risk of aggravating
the situation is considerable if surgery is
attempted by an ophthalmologist lacking experi-
ence or equipment; referral is preferred to haste.
Systemic factors/polytrauma. Any life-threaten-
ing condition takes precedence over the eye
injury; in less serious cases, the decision regard-
ing the most optimal sequence of interventions
should be based on a consultation between the
various specialists.
In summary: the general rule is to delay compre-
hensive reconstruction of the seriously injured eye
for approximately a week. The delay, supported by
the cooling effects of corticosteroid therapy,
brings more favourable conditions, especially by
reducing the haemorrhage risk.
Management: concepts
Below is list of selected principles in the manage-
ment of an injured eye.
Expect a higher tissue prolapse rate with rupture
than with other injury types.
Close the wound before other manipulations are
attempted.
Unless circumferential, large corneal wounds
require interrupted, not running, sutures.
Unless small, corneal wounds should be closed
from the outside in,13 not by division at half
length. Maintenance of the corneal dome shape
is almost as important as the closure being water-
tight and anatomical.
Closure of corneoscleral wounds should start at
the limbus and be completed by closing the
scleral aspect.
Do not excise corneal tissue.
Scleral wounds with posterior extension should
be sutured using theclose-as-you-go method:
conjunctival dissection must not be performed
before the anterior part of the scleral wound is
closed.
Scleral wounds that are very posterior should be
left to heal on their own, rather than attempting
forced closure with the risk of further tissue
extrusion.
Never leave tissue incarcerated in accessible
wounds; the sole exception is the intraoperative
occurrence of an expulsive choroidal haemor-rhage.8
Iris tissue should be repositedexcised only if
necrotic or contaminated. When repositing, pull
the tissue from behindrequires a surgical inci-
sion (paracentesis)do not try to push it in from
the outside.
Ciliary body, choroid, and retina should not be
excised.
Vitreous must always be excised, preferably using
a vitrectomy probe.
Hyphaema is to be evacuated if the IOP cannot be
controlled medically.
Iris tears should be sutured but not until the
posterior segment is meticulously inspected.
It is notalways easy to determine that the lens is
injured;11 if a definite traumatic cataract is pre-
sent, careful early removal allows direct visuali-
sation of the retina, unless vitreous haemorrhage
is present.
It is advisable to delay intraocular lens implanta-
tion until it is determined that there is no serious
posterior segment pathology.
If vitreous removal is performed, all of the vitr-
eous should be excised, including the posterior
hyaloid and the peripheral vitreous. Thick submacular
haemorrhage requires early
removal.
Management: practical issues
Space limitations allow discussing only selected
questions here.
How to suture corneal wounds?
Use a monofilament such as nylon, 100 or 110.
Use sutures with full, not 90%, depth. Fixate the eye with the
forceps over the sclera,
rather than by grabbing corneal tissue.
Suture back to place loose elements.
Plan all suture placements carefully: the sutures
compression effect disappears with removal, but
its slippage effect does not.
How to remove hyphaema?
Always use an infusion: needle held by assistant,
butterfly needle, anterior chamber maintainer,
anterior vitrectomy probe.
Damage control surgery in ocular traumatology 695
-
8/10/2019 Damage Control Surgery Ocular Traumatology
(Injury)
7/7
If the blood is fluid, use one or two paracenteses
for washout.
If the blood is clotted, use forceps or the vitrect-
omy probe.
How to remove an injured lens?
The posterior lens capsule is injured in almost half
of the eyes but this may be impossible to deter-
mine even intraoperatively;11 using the vitrect-
omy probe, rather than traditional cataract
removal techniques, reduces the risk of retinal
complications.
In eyes with high risk for proliferative vitreoreti-
nopathy, posterior capsule removal should be
considered.
How to manage eyes with vitreoushaemorrhage?
Close observation is possible in eyes with contu-
sion; if the haemorrhage organises as determined
by echography or a retinal tear/detachment
develops, vitrectomy is necessary.
In eyes with open globe injury, the risk is too high
to wait for spontaneous blood absorption.
How to treat retinal detachment?
Vitrectomy, rather than traditional surgical
approaches, is preferred; the use of tamponades
should always be considered.
Summary
Seriously injured eyes have a much better chance of
improving than only a few years agoif all appro-
priate guidelines of damage control surgery are
followed. For the ophthalmologist, damage control
surgery has two aspects. First, treatment of the
ocular trauma may have to be delayed due to the
patients systemic condition; second, because the
risk of iatrogenic damage or the chance of subopti-
mal treatment is higher if the intervention is not
delayed for a few days. The goal is to restore eye-
sight, or at least preserve the eyeball, not simply to
fight the tissue damage caused by the trauma. Most
commonly, the initial surgery is restricted to wound
toilette and closure, and the comprehensive recon-
structive operation is performed 710 days post-
injury, following intensive corticosteroid therapy to
reduce the risk of haemorrhage and increase visi-
bility. The concept of damage control surgery also
implies that referral is preferred if not all conditionscan be
met to perform optimal surgery.
References
1. Barr C. Prognostic factors in corneoscleral lacerations.
Arch
Ophthalmol 1983;101:91924.
2. Biehl J, Biehl JW, Valdez J, et al. Penetrating eye injury
in
war. Mil Med 1999;164:7804.
3. Cleary P, Ryan S. Histology of wound, vitreous, and retina
in
experimental posterior penetrating eye injury in the rhesus
monkey. Am J Ophthalmol 1979;882:22131.
4. Cleary PE, Ryan SJ. Vitrectomy in penetrating eye injury.
Arch Ophthalmol 1981;99:28792.5. Coleman D. Early vitrectomy in
the management of the
severely traumatized eye. Am J Ophthalmol 1982;93:
54351.
6. Kuhn F, Mester V, Berta A, Morris R. Epidemiology of
serious
ocular trauma: the United States Eye Injury Registry (USEIR)
and the Hungarian Eye Injury Registry (HEIR). Ophthalmo-
loge 1998;95:33243.
7. Kuhn F, Morris R, Witherspoon CD, et al. A standardized
classification of ocular trauma terminology. Graefes Arch
Clin Exp Ophthalmol 1996;234:399403.
8. Kuhn F, Morris R, Mester V, Witherspoon CD. Management of
intraoperative expulsive choroidal haemorrhage during
anterior segment surgery. In: Stirpe M, editor. Anterior
and posterior segment surgery: mutual problems and
common interests. New York: Ophthalmic CommunicationsSociety;
1998. p. 191203.
9. Lemmen K, Heimann K. Fruh-Vitrektomie mit primarer
Silikonolinjektion bei schwerstverletzten Augen. Klin Mon-
atsbl Augenheilk 1988;193:594601.
10. Mester V, Kuhn F. Ferrous intraocular foreign bodies
retained in the posterior segment: management options
and results. Int Ophthalmol 2000;22:35562.
11. Mester V, Kuhn F. Lens. In: Kuhn F, Pieramici D,
editors.
Ocular trauma: principles and practice. New York: Thieme;
2002. p. 18096.
12. Morris R, Kuhn F, Witherspoon CD, Stevens D. Counseling
the
patient and the family. In: Kuhn F, Pieramici D, editors.
Ocular trauma: principles and practice. New York: Thieme;
2002. p. 226.
13. Rowsey J, Hays J. Refractive reconstruction for acute
eyeinjuries. Ophthalmic Surg 1984;15:56974.
14. Thompson W, Rubsamen P, Flynn H, Schiffman J, Cousins S.
Endophthalmitis after penetrating trauma. Risk factors
and visual acuity outcomes. Ophthalmology 1995;102:
1696701.
696 F. Kuhn, Z. Slezakb















![[Forensics] traumatology 2.ppt](https://img.pdfslide.us/doc/110x75/55ce4f98bb61eb46528b47b2/forensics-traumatology-2ppt.jpg)









![[Forensics] traumatology 1](https://img.pdfslide.us/doc/110x75/55c475bdbb61ebbc228b45ab/forensics-traumatology-1.jpg)