Embed Size (px)
Citation preview

J Phys Fitness Sports Med, 10 (2): 85-97 (2021)DOI: 10.7600/jpfsm.10.85
JPFSM: Regular Article
Daily walking habit reduces fasting blood sugar level in newly diagnosed diabetic participants in rural Bangladesh
Subrina Jesmin1,2*, Takeru Shima1,3, Naoto Yamaguchi4, Farzana Sohael2,5, Adil Maqbool6,Arifur Rahman2, Masao Moroi7, Nobutake Shimojo8, Saturo Kawano8, Koichi Watanabe1,
Fumi Takeda1 and Hideaki Soya1
Received: March 14, 2020 / Accepted: August 24, 2020
Abstract Diabetes mellitus, a life-threatening non-communicable disease, is now an epidemic-level problem in developed countries, and also prevalent in developing countries, including Bangladesh. Bangladesh has been facing a significant and growing burden of diabetes mellitus handling in recent decades. In the present study, we investigated whether a daily walking inter-vention could improve the fasting blood sugar level in newly diagnosed diabetes mellitus par-ticipants in rural Bangladesh who were not on medication. A rural population of 1,045 people in Bangladesh were screened for diabetes mellitus. One hundred fifty-six people, including 87 diabetes mellitus participants, went through a 5-month daily walking program (twice daily, 1.5 km walking each time). In our initial screening, the prevalence of newly diagnosed diabetes mellitus cases was 8.5% in the rural population. Mean fasting blood sugar level in these new diabetes mellitus cases was 10.0 ± 0.33 mmol/L. After five months of exercise, both the fast-ing blood sugar and 2h OGTT sugar levels were significantly improved, and no DM (diabetes mellitus) cases were on medication. The current research findings show that a walking program can be a potential lifestyle intervention to combat the diabetes mellitus epidemic in a poor rural context in Bangladesh.Keywords : diabetes, exercise, glycemic parameters, rural population, Bangladesh
Introduction
Diabetes mellitus (DM) is a chronic disease that dis-rupts the regulation of blood sugar either by decreasing insulin secretion or by developing resistance to it1). In-sulin is the primary hormone that regulates blood sugar levels. Beta cells of the pancreas release insulin, which allows the sugar to enter from the bloodstream into other cells by acting on insulin receptors. In broad terms, DM has two main types, DM type 1 and DM type 2. In DM type 1, the beta cells of the pancreas get destroyed as a result of an auto-immune response, and is more com-mon in young adults2). Whereas DM type 2 results from resistance of insulin receptors due to insulin failing to act on these receptors, and mainly affects older people3). DM
has severe complications, including hypertension, car-diovascular disease, stroke, nephropathies, neuropathies, and retinopathies leading to blindness4). It can also cause metabolic disorders like ketoacidosis and hypokalemia, leading to coma and even death5,6). DM is one of the most prevalent diseases of the mod-ern world, and increased to 425 million cases by 2017. It is estimated to rise to 629 million by 20457). According to WHO in 2016, DM was the seventh leading cause of death worldwide8). Currently, 23 million US adults have been diagnosed with diabetes9). Based on 2018 estimates, 34.2 million Americans, or 10.5% of the population, have been living with diabetes10). And, according to the latest statistics from the International Diabetes Federation (IDF), South East-Asia (SEA) Region consisting of India, Sri Lanka, Bangladesh, Bhutan, Mauritius, and the Maldives, had more than 72 million adults with diabetes in 2013, *Correspondence: [email protected]
1 Faculty of Health and Sports Sciences, University of Tsukuba, 1-1-1 Tennodai, Tsukuba, Ibaraki 305-8574, Japan2 Health & Disease Research Centre for Rural Peoples (HDRCRP), Mohammadpur, Dhaka 1207, Bangladesh3 Department of Health and Physical Education, Cooperative Faculty of Education, Gunma University, 4-2 Aramaki-machi,
Maebashi, Gunma 371-8510, Japan4 Ibaraki Prefectural University of Health Sciences, 4669-2 Ami, Ami-machi, Inashiki-gun, Ibaraki 300-0394, Japan5 Department of Gynaecology, Dhaka Medical College, Dhaka 1205, Bangladesh6 Allama Iqbal Medical College, University of Health Sciences (UHS), Lahore 54550, Pakistan7 Faculty of Medicine, Toho University, 5-21-16 Omorinishi, Ota-ku, Tokyo 143-8540, Japan8 Faculty of Medicine, University of Tsukuba, 1-1-1 Tennodai, Tsukuba, Ibaraki 305-8575, Japan
86 JPFSM : Jesmin S, et al.
which is expected to exceed 123 million by 203511). In Bangladesh, although the prevalence of DM type 2 varies from 4.5%-35.0% by area, evidence shows it is increasing in both rural and urban areas12). Where sociodemographic disparities play a significant role in chronic disease han-dling in developing countries, the rural context should be brought into focus for the Bangladeshi community. Positive lifestyle changes (interventions) are recom-mended as one of the most crucial and effective ways to combat diabetes13). As the world continues to progress, new therapeutical ways are being adopted to manage various diseases. As a result, recent studies on managing DM have become more centered on lifestyle interven-tions rather than pharmaceutical approaches14-16). There is emerging evidence that intensive lifestyle interventions can prevent or delay the development of type 2 diabetes17). Even a simple task such as daily walking can not only improve insulin sensitivity, but also improve glycemic control and incidence of obesity, leading to a lower risk of developing DM type 218). In one study, 3,234 individu-als suffering from impaired glucose tolerance (IGT) were assigned three different interventions: standard lifestyle with placebo, intensive program of lifestyle interventions, and current lifestyle with metformin drug. According to a follow-up study 2.8 years later, it was seen that the intensive program of lifestyle interventions reduced the incidence of DM by 58%19). Similarly, 150 min of brisk walking per week can be instrumental in preventing DM type 220). In Bangladesh, a developing country with an enormous DM burden, it is essential to discover an affordable and practical approach to control and even prevent diabetes. In Bangladesh, the estimated overall prevalence of diabe-tes among adults was reported at 9.7% in 201121). There has been a projection that the number of DM cases would
reach 13.7 million by 204522). There is no valid or of-ficial national health insurance system in Bangladesh22). We know the average household spends 7.5% of its total income on health care. However, the poorest 20% of families spend 13.5% of their income on healthcare23). Per capita gross domestic product (so-called GDP) of Bangladesh was estimated to be US$1,677 in 201824). At that time, about one-third (31.5%) of the population of Bangladesh was below the poverty line24). Thus, the self-financing health care expenditure posed a substantial eco-nomic burden on the population, especially the poorest segment. In the present study, we aimed to construct an overall picture and analysis of the current DM situation from na-tionally representative data (Part 1, Fig. 1). This is a sec-ondary analysis of already conducted research. Then we tried to find out the DM prevalence in the population of a specific region in Bangladesh where there has never been any DM screening. And, finally, we implemented lifestyle interventions for diabetic individuals in Bangladesh. The present findings are crucial in the sense that this current study provides the first evidence that even a mild exercise regimen for several months can significantly improve the blood sugar level in new DM cases. We applied an af-fordable exercise regimen that rural people could quickly adopt, especially women. We should mention here, how-ever, that exercise has already been proven to be benefi-cial both for the preventive and therapeutic aspects of DM. But in a developing country, like Bangladesh, where most DM cases are undiagnosed and a lot of disparity exists in the utilization of health care services, the pres-ent findings bear a potential impact for addressing these shortcomings and disparities. The present study was conducted in a rural context where the poverty level, educational level, and health care
Fig. 1 Diagram for study participant screening and selection in Part 1 study.
Total number of data = 20039(from whole Bangladesh)
8 Divisions in Bangladesh (BD)
Dhaka Chittagong Rajshahi Rangpur Barishal Khulna Sylhet Mymensingh
Selected Bogura district from Rajshahi division (total number of districts 64 in BD)
Total number of data of Bogra district 1002
After exclusion missing value included statistics in 869 data
Missing value 133 data

87JPFSM : Fasting blood sugar level and mild walking
facilities were notably inferior to an urban setting. Ac-cordingly, the potential significance of this study was to clarify the gravity of the diabetes situation in a rural con-text and how positive lifestyle interventions in poverty-bound healthcare populations with less resources, and who are entirely devoid of the benefits of a health insur-ance system, can help in combating chronic diseases like DM. For this study, we chose mild walking as our life-style intervention, as it is easy to perform and follow up. The rural population in Bangladesh is illiterate to a great extent, so daily supervised walking is a relatively easy way to involve them in a lifestyle intervention.
Materials and Methods
Study procedure. The present study was jointly ap-proved by the Ethics Committee of Bogra Medical Col-lege, Bogra, Bangladesh, and the Health and Disease Research Centre for Rural Peoples (HDRCRP) (ethical number: HDR-BOG-2018), and conforms to the prin-ciples outlined in the Helsinki Declaration. Before enrol-ment in this study, all the study participants gave their written informed consent.
Part 1: Study design. The data was taken from the meta-bolic syndrome and cardiometabolic risk factors survey coordinated by Bogra Medical College with the collabo-ration of HDRCRP Bangladesh. There are several Japa-nese Institutes also involved in this nationally representa-tive study in Bangladesh, including the National Center for Global Health and Medicine (Tokyo), Japan, and the Institute of Clinical Medicine, University of Tsukuba, Japan. The data collection was done in 2012-2013, with adoption of the study protocol, dissemination of some results, and references from past publications25-29). It is a cross-sectional study that was done in Bangladesh, both rural and urban areas, mainly targeting the eight major administrative divisions in Bangladesh (Fig. 1). In Ban-gladesh, there are 64 districts in the eight divisions, and Bogra District belongs to Rajshahi Division. In this study, we present the necessary data on DM prevalence and level of physical inactivity only from Bogra District (Fig. 1). We measured physical activity through the question-naire of the WHO STEPS protocol; and also the criteria of evaluation of physical activity is stated later in this pa-per in the “Definitions” section of Materials and Methods. Although the survey was nationwide, we only presented data for the Bogra district, as part 2 of the study was con-sequently conducted in Bogra. The rationale for choosing the Bogra district is that, according to past findings, it is a very neglected rural region in Bangladesh where women are severely discriminated and healthcare care services are less resourced.
Part 1: Study population. The survey includes 869 Bangladeshi men and women ≥15 years of age25-28,30) and
primary residents of Bangladesh residing in the Bogra district, excluding a military base (e.g., a dormitory), and those who were institutionalized (e.g., hospitals, prisons, nursing homes, and other such institutions). Part 1 study data was taken from a nationally representative survey and shows a similar gender ratio (female:male) (Table 1).
Part 2: Study design. In part 2 of the study, a total of 1,045 rural people in Bangladesh were screened for DM through a mobile satellite camp in five Upazilas of the Bogra district. In Bangladesh, each district is composed of several Upazila (smaller units of a district). We set up a temporary health screening camp with OGTT testing at five convenient places of five Upazila in Bogra (Fig. 3). The five selected sites were conveniently located, with easy access for the study participants. We attempted to catch our target number of study participants from a remote rural context. It was arranged that participants would not need transportation to come to a mobile health camp for DM screening with OGTT. Blood sugar screen-ing was done through a simple ultra-touch pricking method using a sensor. For this study, we took a blood sample of subjects in a fasting condition before having them consume a sugary drink and again getting two blood samples after consumption of the sugar drink. Then we determined a case-control design for 156 out of the 1,045 participants. The 156 participants included 87 DM and 69 non-DM subjects. The 156 participants went through a 5-month daily walking program which was supervised (twice daily, 1.5 km walking each time), including the 87 DM participants screened from a population of 1,045, as already mentioned. The walking program was designed through discussion with study participants (Fig. 3). We included the 69 non-DM participants in the walking intervention. With 80% power (β = 0.20) and a 5% sig-nificance level, the sample was adequate to test the all-inclusive formulated hypothesis.
Part 2: Study participants. House-to-house visits and announcements were made for the recruitment and se-lection of respondents from five different communities (Upazilas) in the Bogra district. The respondents were interviewed and clinically examined for data collection. Blood sampling and related work was done by mobile ex-amination centers for all 1,045 participants. Then 156 of these participants, including 87 newly diagnosed DM sub-jects and 69 non-DM subjects, underwent a 5-month daily walking program, which was supervised (twice daily, 1.5 km walking each time).
Exercise intervention. We conducted a supervised daily walking program for five months, 3 km per day. We di-vided the walkers into a total of nine groups, having al-most 10 participants of newly diagnosed DM cases with 7-8 control participants in each group, and one supervisor from the local community (Fig. 5). The walking program

88 JPFSM : Jesmin S, et al.
Table 1. Sociodemographic characteristics of study participants (Part 1).
BMI: body mass index; SBP: systolic blood pressure; DBP; diastolic blood pressure; HDL: high-density lipoprotein; LDL: low-density lipoprotein; FBS; fasting blood sugar; SE: standard error.
stluseR selbairaV 05.0 ± 2.14 ES ± naem ,)sraey( egA
Gender 3.14 % ,elaM 7.85 % ,elameF
Anthropometric and physical parameters 83.0 ± 9.25 ES ± naem ,)gk( thgieW 20.0 ± 07.1 ES ± naem ,)mc( thgieH
BMI (kg/m2 51.0 ± 5.22 ES ± naem ,) 43.0 ± 8.87 ES ± naem ,)mc( ecnerefmucric tsiaW 76.0 ± 3.211 ES ± naem ,)gHmm( PBS 63.0 ± 4.37 ES ± naem ,)gHmm( PBD
Biochemical parameters 32.2 ± 7.071 ES ± naem ,)ld/gm( loretselohc latoT 00.3 ± 5.131 ES ± naem ,)ld/gm( edirecylgirT
34.0 ± 9.73 ES ± naem ,)ld/gm( loretselohc LDH 20.2 ± 6.901 ES ± naem ,)ld/gm( loretselohc LDL
70.0 ± 58.5 ES ± naem ,)L/lomm( SBFLifestyle factors
30.0 ± 66.1 ES ± naem ,keew/syad gnivres stiurF 60.0 ± 87.4 ES ± naem ,keew/syad gnivres elbategeV
0.44 % ,ytivitca lacisyhp woL 2.65 % ,noitpmusnoc occaboT
Educational level 2.51 % ,noitacude oN 4.7 % ,noitacude yramirP 2.07 % ,noitacude yradnoceS 2.7 % ,noitacude rehgiH
Marital status 7.0 % ,elgniS 1.88 % deirraM 2.11 % ,srehtO
Occupation 9.25 % ,efiW esuoH 9.51 % ,tnemyolpmE-fleS 4.7 % ,boJ tnemnrevoG 2.3 % ,boJ .tvog-noN 6.3 % ,tnedutS 9.1 % ,robal yaD 5.01 % ,remraF 6.4 % ,srehtO
Monthly income (taka) 0.66 % ,00001< 2.23 % ,00002-00001 7.1 % ,00002=>

89JPFSM : Fasting blood sugar level and mild walking
was rated as mild in terms of difficulty level and con-ducted in a calm village environment; yet strictness was maintained in terms of regularity and completion of target walking distance every day. Walking speed was moderate. For DM participants, the adherence rate to this program was very successful; but for the control group who knew they did not have DM, the response and adherence to the walking program was inadequate. In the morning, par-ticipants gathered at a previously designated place, which was different for each of the nine groups, at 6.30 am, and walked 1.5 km together. For the evening walk, partici-pants gathered at 5.30 pm and walked 1.5 km, similar to the morning routine. There were no irregular or dropout cases among DM participants; but there was a dropout rate of more than 20% among the controls.
Part 2: Exclusion criteria. We excluded pregnant wom-en, women with a known illness such as ischemic heart disease (IHD) or chronic illness such as hypothyroidism, and those who were on hormone replacement therapy (HRT).
Study instruments. The study was according to the World Health Organization’s STEPS approach (modified) (https://www.who.int/ncds/surveillance/steps/instrument/en/), according to which risk factor data must be collected stepwise based on a standardized questionnaire covering somatic illnesses, somatic and mental symptoms, demo-graphic characteristics, lifestyle, medications, and neces-sary health behavior (step 1), physical measures (step 2) and biochemical fundamentals such as levels of blood cholesterol and sugar (step 3). Physical activity was mea-sured through the questionnaire of the STEPs protocol. Fruits and vegetables. Survey questions asked about the number of fruits and vegetables consumed by respon-dents and the number of servings of fruits and vegetables consumed on a given day. One standard serving size equaled approximately 80 grams. Servings were measured by showing pictorial cards or measuring cups. Physical activities. We asked respondents the num-ber of days and time spent on vigorous and/or moderate activities at work, travel to and from places, and recre-ational activities. We converted the responses to MET minutes/week. Strenuous exercise, moderate activity, and low physical activity were recorded based on the criteria given in the WHO STEPS Manual20). Tobacco. Information on tobacco was collected for both smoking and smokeless forms. Those who smoked or used smokeless tobacco daily in the past 30 days were considered as ‘current’ user. Daily users were asked about the initiation and duration of use through both age and year(s). The frequency of use of products was also asked. History of raised blood pressure. Questions were asked on the personal history of hypertension, medicine pre-scribed by a doctor, and advice given regarding diet, weight loss, smoking, and nature of physical activity undertaken.
Anthropometric and other variables. Well-trained ex-aminers examined the participants and recorded their an-thropometric measurements. Weight was measured with a balanced calibrated scale to the nearest 0.1 kg. Height was measured with a portable stadiometer to the nearest 0.1cm. After the measurements of height (m2) and weight (kg), the body-mass index (BMI) was calculated, and then the waist circumference was measured to the near-est 0.1cm from the point between the lower border of the rib cage and the iliac crest. Finally, the blood pressure of the individuals was measured with a standard mercury manometer in a sitting position from the right arm. Every individual’s blood pressure (both systolic [SBP] and dia-stolic [DBP]) was measured twice, the first reading after 5 minutes of making the individual comfortable and second reading after an interval of 15 minutes. The mean of these two readings was taken and recorded.
Oral sugar tolerance test and DM diagnosis. The sugar (glucose) tolerance test (GTT), also referred to as the oral sugar tolerance test (OGTT), is a standard method of di-agnosing cases of DM or insulin resistance31). OGTT is a more substantially sensitive indicator of DM than finger prick testing. The study participants came to the mobile health center after an overnight fast of 10-12 hours. For biochemical analysis, including fasting blood sugar, the blood was obtained after 10 to 12 hours of fasting. The blood samples were then centrifuged, and serum was obtained immediately to measure the concentrations of target parameters. We did not conduct the test if the par-ticipants showed signs of illness. And, we did not include any pregnant women. Each study participant was asked to take a sugary drink. We bought a commercial sweet drink having 75 g of sug-ar from a drug store for each subject, and requested that it be consumed within a 5-minute time frame. Their blood sugar level was measured before and at intervals after the sugary drink was taken. In our protocol, further blood samples were then taken after 2 hours (2h) of sugary drink ingestion. Study participants with a fasting blood sugar (FBS) more than 7.0 mmol/L at fasting condition and later confirmed by the 2h blood sugar test (over 11.0 mmol/L) were treated as the DM group. These DM cases were not previously known cases. They knew for the first time that they had DM. They were then recruited to our intervention program. The levels of FBS was measured by a kit (Sugar MR kit; Linear Chemicals SL, Montgat-Barcelona, Spain). Blood sugar was measured by auto-matic biochemical analyzer, not by the manual colorimet-ric method.
Other Biochemical analysis. The separated serum at fasting state, as mentioned above, were immediately run to measure the concentrations of total cholesterol (TC) [Cholesterol MR, Triglycerides MR, Linear Chemicals S.L., Montgat, Barcelona, Spain], triglycerides (TG), and

90 JPFSM : Jesmin S, et al.
HDL [HDL-C with the Determiner-HDL Cholesterol-CROMATEST (Montgat, Barcelona, Spain)]. LDL-C was calculated as TC-HDL-C-VLDL-C; VLDL-C was calculated as 0.456 × total TG concentration expressed in mmol/L32).
Definitions. We considered ‘low physical activity’ as achieving less than 5 days a week of any combination of walking and/or moderate- or vigorous-intensity activities, and less than 600 min of physical activity per week. We defined ‘insufficient fruit and vegetable consumption’ as <5 servings of fruit or vegetables a day. ‘Raised blood pressure’ was defined as systolic 140 mmHg or diastolic 90 mmHg or reported treatment for elevated blood pres-sure. Abdominal obesity was considered as waist circum-ference ≥94 cm for men and ≥80 cm for women. For the participants of the medical examination, we computed and made an entry of BMI values as weight divided by the square of height (kg/m2). The study participants were clas-sified as having normal weight (BMI < 25.0), overweight (BMI 25.0-29.9), and obese (BMI ≥ 30.0). We considered high blood pressure as 140/90 mm Hg (systolic/diastolic), high blood cholesterol as ≥240 mg/dL, impaired fasting glucose as 100 mg/dL to 125 mg/dL, and diabetes as ≥126 mg/dL. We considered the current intake of antihyper-tensive medications for high blood pressure and lipid-lowering medications for high blood cholesterol.
Statistical analysis. We used IBM SPSS Statistics 20 for data analysis. We entered data into an excel file and coded the data. Values are expressed as percentages of total re-spondents. Simple bivariate analysis was used to analyze the data. Priority was given to practical benefit and clini-cal significance in interpreting statistically significant data. The differences between participants having normal and DM symptoms, and between pre- and post-exercise intervention, were estimated by t-test for normal data distribution. For skewed continuous variables, the Mann-Whitney test was performed. The data are expressed as mean ± S.E. A p-value < 0.05 is considered as statistically significant. We did not count those participants for data analysis who were irregular in walking and/or did not complete the walking distance with the group.
Results
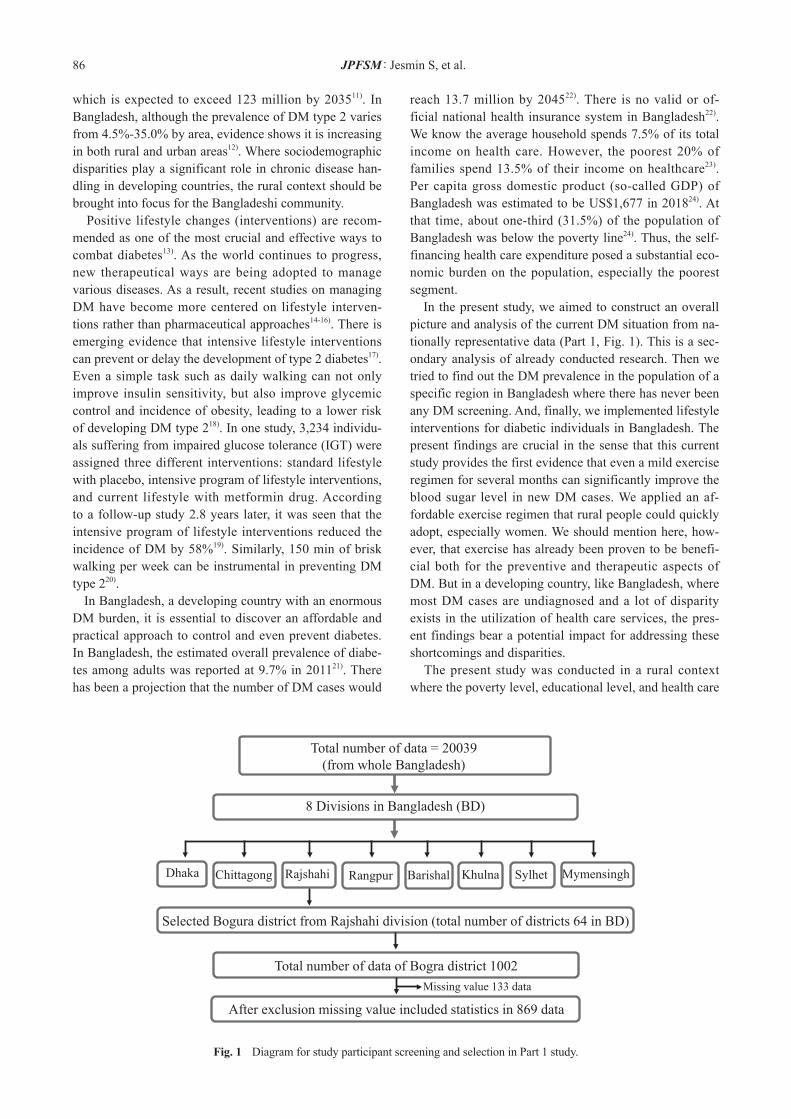
Part 1. In Table 1, we described the sociodemographic parameters of the study participants analyzed in part 1 (869 participants) from a nationwide survey only for the Bogra district (Fig. 1). Female participants were 58.7% (Table 1). The average age was 41 years old, the average BMI was 22.5 kg/m2, and average systolic and diastolic pressure were 112.3 and 73.4, respectively (Table 1). Most of the participants were poor (66%). Fig. 2 empha-sizes physical inactivity and DM prevalence. Physical inactivity was more pronounced among females com-
pared to males, and among urban as compared to those who belong to rural areas (Fig. 2a and 2b). In Fig. 2c, we observed that the prevalence of DM among participants having low physical activity was almost double (11.1%) compared to those with normal physical activity (5.1%). We measured the total DM prevalence, including both known and unknown cases. Similarly, the mean value of FBS was also high among individuals with low physical activity (Fig. 2d).
Part 2. DM screening and case-control comparison. Among 1,045 participants, the newly diagnosed prevalence of DM was 8.5%, as revealed through the OGTT test in the rural mobile camp setting (Fig. 3). Following DM screen-ing, we made a case-control analysis of 156 participants, including 87 DM cases, and these participants later un-derwent a five-month daily walking intervention. The primary demographics of these 87 DM participants are described in Table 2. The mean age of the DM participants was 43.0 ± 1.1 years. There was no significant difference in age be-tween DM and control participants (Table 2). The mean weight and height of DM participants were 54.7 kg and 150.6 cm, respectively, which made the mean body mass index (BMI) to be 24.1 kg/m2 (Table 2). Only waist cir-cumference was significantly different between DM and control groups (p < 0.001). Among biochemical param-eters investigated here, plasma FBS, 2hOGTT, HDL, and LDL levels were significantly different between DM and control groups (Table 2). If we look at the education level, secondary and higher education level was lower in DM participants in comparison to control participants (p = 0.062). Most of the DM participants were married (97.7%). Among DM participants, the majority of the par-ticipants were Muslims by religion (77.9%), while the rest are Hindus (22.1%) (Table 2). Among DM participants, 83.5% were housewives while others were self-employed (9.4%), doing non-govt. jobs (4.7%), day labors (1.2%) and students (1.2%). There was not a remarkable differ-ence in the occupational status between DM and control participants (Table 2). When we did financial stratifica-tion analysis for study participants, the DM group seemed to have a better economic condition than the control group (Table 2) (p = 0.034). Results from walking intervention. We presented the data only on DM participants after five months of walk-ing intervention who were newly diagnosed as DM cases. More than 80% of DM participants had significant improvement in their blood sugar levels both from the fasting state level and 2h OGTT level. The five months of mild walking significantly improved the high levels of FBS from the baseline 10.0 ± 0.3 mmol/L to 6.9 ± 0.2 mmol/L at the end of 5 months (Fig. 4a; p < 0.001), 2h OGTT level from 13.0 ± 0.5 mmol/L to 8.9 ± 0.6 mmol/L (Fig. 4b; p < 0.001), waist circumference was also im-
91JPFSM : Fasting blood sugar level and mild walking
Fig. 2 Bangladeshi physical activity and its relationship to the prevalence of diabetes and mean levels of FBS. (a) Gender difference on physical activity, male: n = 359; female: n = 510. (b) Regional deference on physical activity, rural: n = 182; urban: n = 687. (c) Prevalence of diabetes, and (d) mean levels of FBS with physical activity, low physical activity, n = 382; normal physical activity, n = 487.
Figure 2
a b
CCCC
c d
Fig. 3 Diagram for study participant screening and selection in Part 2 study.
Total number of data participants=1045 (from Bogra district)
5 study areas at Upazila level under Bogra district
Bogra Sadar Sherpur Dhunat Shibganj Gabtali
Newly diagnosed prevalence of DM was 8.5% among 1045 (N=89)
Next analysis: DM subjects 87 + Control 69 (case-control design) Missing value 2 data
N=202 N=220 N=211 N=212 N=200
These 156 participants underwent walking intervention

92 JPFSM : Jesmin S, et al.
Table 2. Sociodemographic analysis as a baseline between the control and diabetes groups (Part 2).
BMI: body mass index; SBP: systolic blood pressure; DBP; diastolic blood pressure; HDL: high-density lipoprotein; LDL: low-density lipoprotein; FBS; fasting blood sugar; OGTT: oral glucose tolerance test; SE: standard error.
eulav-P setebaiD lortnoC selbairaV 563.0 31.1 ± 0.34 34.1 ± 3.14 ES ± naem ,)sraey( egA
Gender (Male vs Female; 10.3% vs 89.7%) 426.0 2.9 6.11 % ,elaM
8.09 4.88 % ,elameFAnthropometric and physical parameters
871.0 20.1 ± 7.45 32.1 ± 6.25 ES ± naem ,)gk( thgieW 406.0 15.0 ± 6.051 07.0 ± 2.051 ES ± naem ,)mc( thgieH
BMI (kg/m2 360.0 34.0 ± 0.42 64.0 ± 8.22 ES ± naem ,)Waist circumference (cm), mean ± SE 82.8 ± 1.66 90.8 ± 0.59 <0.001
113.0 68.1 ± 5.711 06.2 ± 9.021 ES ± naem ,)gHmm( PBS 599.0 90.1 ± 1.08 34.1 ± 1.08 ES ± naem ,)gHmm( PBD
Biochemical parameters Total cholesterol (mg/dl), mean ± SE 159.5 ± 3.73 164.3 ± 3.54 0.384 Triglyceride (mg/dl), mean ± SE 121.9 ± 7.93 123.8 ± 8.98 0.884 HDL cholesterol (mg/dl), mean ± SE 45.0 ± 1.17 36.0 ± 0.58 <0.001 LDL cholesterol (mg/dl), mean ± SE 90.1 ± 3.68 103.6 ± 3.46 0.013
100.0< 33.0 ± 0.01 01.0 ± 57.5 ES ± naem ,)L/lomm( SBF 100.0< 64.0 ± 0.31 23.0 ± 4.7 ES ± naem ,)L/lomm( TTGO
Lifestyle factors Fruits serving days/week, mean ± SE 1.49 ± 0.16 1.27 ± 0.16 0.323 Vegetable serving days/week, mean ± SE 3.27 ± 0.19 2.96 ± 0.17 0.206
779.0 7.15 0.25 % ,ytivitca ytisnetni-suorogiV 100.0< 9.55 9.03 % ,noitpmusnoc occaboT
753.0 1.66 9.95 % ,ytivitca lacisyhp woLEducational level
260.0 7.83 4.03 % ,noitacude oN 0.23 8.81 % ,noitacude yramirP 7.22 7.73 % ,noitacude yradnoceS
7.6 0.31 % ,noitacude rehgiHMarital status
072.0 2.1 8.5 % ,elgniS 7.79 8.29 % ,deirraM
2.1 4.1 % ,srehtOOccupation
956.0 5.38 7.97 % ,efiW esuoH 4.9 2.7 % ,tnemyolpmE-fleS 7.4 8.5 % ,boJ .tvog noN 2.1 9.2 % ,tnedutS 2.1 3.4 % ,robal yaD
Monthly Income (Tk.) 430.0 4.45 9.37 % ,00001<
9.23 7.12 % ,00002-00001 7.21 3.4 % ,00002=>
Religion 623.0 9.77 0.17 % ,milsuM
1.22 0.92 % ,udniH

93JPFSM : Fasting blood sugar level and mild walking
Discussion
In the first part of this study, we demonstrated the phys-ical inactivity and DM state from a nationwide analysis in Bangladesh, displaying the data of the Bogra district. Here we showed that the population with high physical activity has a lower prevalence of DM compared to the people with low physical activity. Later, through the DM screening in five Upazila, in a Bogra district rural con-text, we found 8.5% prevalence of newly diagnosed DM who did not know that they had DM. Furthermore, we
proved from 90.8 ± 0.6 cm to 81.8 ± 1.1 cm (Fig. 4c; p < 0.001). However, there was no significant change in cho-lesterol levels, triglyceride levels, LDL-C levels, and BMI of the participants (Figs. 4e-4h). At the end of the five-month daily exercise intervention, the HDL-C levels had increased from 36.0 ± 0.6 mg/dl to 49.0 ± 0.9 mg/dl (Fig. 4d; p < 0.001), and DBP levels decreased from 80.1 ± 1.1 mmHg to 74.5 ±1.8 mmHg with exercise intervention (Fig. 4j; p = 0.01). In contrast, SBP levels only decreased from 117.5 ± 1.9 mmHg to 114.6 ± 3.0 mmHg, showing no significant change (Fig. 4i; p = 0.41).
Fig. 4 Effects of exercise intervention on biochemical and anthropometric param-eters. (a) Mean levels of FBS, (b) sugar tolerance 2h OGTT, (c) mean levels of waist circumference, (d) mean levels of HDL-C, (e) total cholesterol level, (f) triglyceride levels, (g) LDL-C levels, (h) BMI levels, (i) SBP levels, and (j) DBP levels at baseline and after exercise intervention. Data are expressed as mean ± S.E., n = 87 (DM only).
Figure 4Figure 4
Figure 4
Figure 4
Figure 4Figure 4
Figure 4
94 JPFSM : Jesmin S, et al.
found that a five-month daily walking program improved FBS levels and sugar (glucose) tolerance, and lowered HDL-C levels in newly diagnosed diabetic population in rural Bangladesh who were not on medication. To our knowledge, this is the first study to explore the associa-tion between FBS levels and mild daily exercise in newly diagnosed diabetic patients in Bangladesh. Lifestyle changes are being adopted for treating non-communicable diseases such as DM18-20). Notably, a large number of studies reported that exercise has beneficial effects on managing DM18-20). The current study showed that a population with high physical activity has a lower prevalence of DM and mean levels of FBS compared to people with low physical activity (Fig. 2c and 2d); thus, physical inactivity is a significant contributing factor in a DM population. Also, we found gender-based and urban-rural differences in weekly physical activity (Fig. 2a and 2b) from a nationally representative analysis. These find-ings imply that the female population and the urban popu-lation are at risk of developing DM in Bangladesh. The prevalence of DM is much higher in South Asians compared to other developing and developed countries in regards to not only prevalence, but also DM-associated complications. Even mortality rates are higher among South Asians33). One of the major factors of these com-plications is the late diagnosis and inadequate follow-up. Due to unawareness of DM among the public, people are usually diagnosed as DM only when they experience a hyperglycemic crisis or ketoacidosis. The diagnostic rate of pre-diabetic people is low in South Asia. In diagnosis, most of the cases are diagnosed as people with DM type 1,
and usually appear at an early age with symptoms of poly-uria, polydipsia, and diabetic ketoacidosis. In diagnostic tests, FBS, OGTT, and random plasma sugar levels are checked; and for confirmation, HbA1C levels are checked. According to the American Diabetic Association (ADA), initially, the suspected person should be tested with the FBS and OGTT tests. If these tests come out positive, then HbA1c should be done twice as a confirmation test. The criteria of HbA1C (twice > 6.5%) and have FBS more than 126 mg/dl determined whether or not a subject was considered as DM34). The population in rural Bangladesh investigated in the current study was poor. Most of them did not have ad-equate access to healthcare facilities, which are mainly urban-based in Bangladesh. The rationale for choosing the rural context in this study was due to several sociode-mographic factors including poverty, lack of awareness on health, lack of health insurance system, less-resourced healthcare facilities, lack of health care professionals, gender inequity, and transportation barriers. There are very few OGTT facilities in remote rural Bangladesh. Thus, the present study conducted a series of mobile health camps with instant measurement of biochemical parameters. In Bangladesh, even in the urban context, the cost and facilities to perform HbA1C level measurements are limited, warranting future studies to be conducted exploiting this sensitive technology for the diagnosis of DM. Another vital issue to be mentioned here is a higher level of cooperation of female DM participants in the Part 2 study, as well as in the intervention. It was easy to
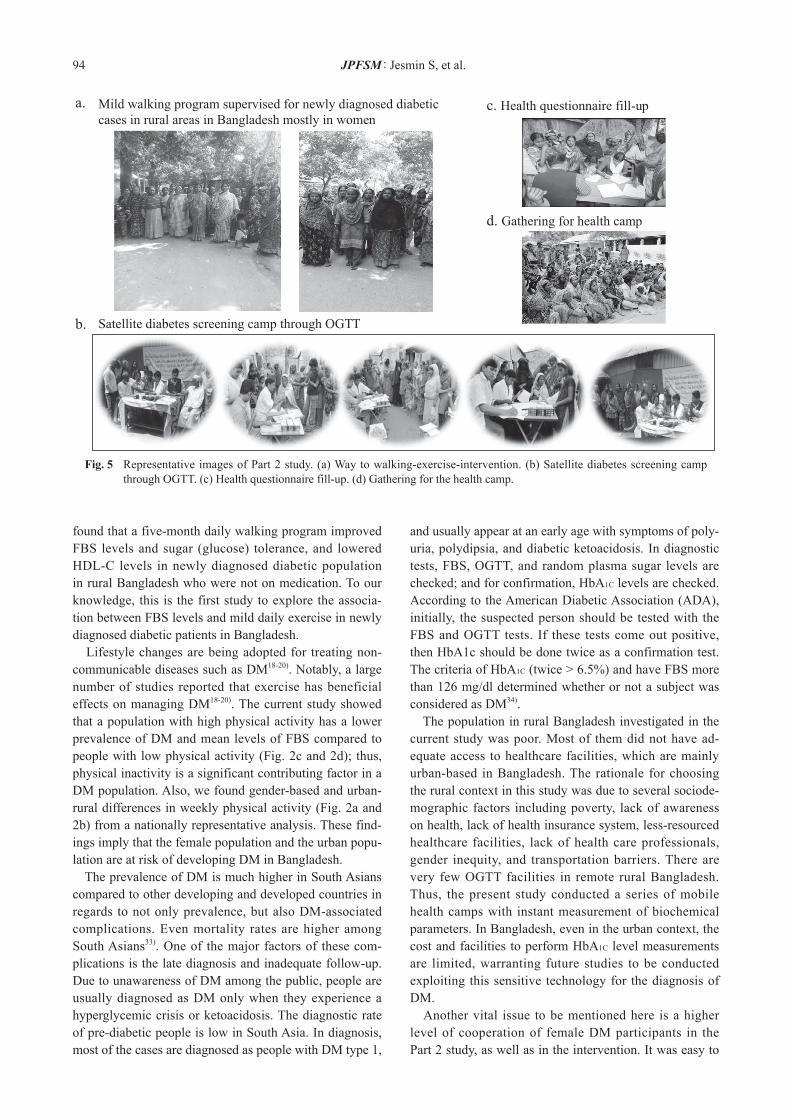
Fig. 5 Representative images of Part 2 study. (a) Way to walking-exercise-intervention. (b) Satellite diabetes screening camp through OGTT. (c) Health questionnaire fill-up. (d) Gathering for the health camp.
a.
b.
c. Health questionnaire fill-up
d. Gathering for health camp
Mild walking program supervised for newly diagnosed diabetic
cases in rural areas in Bangladesh mostly in women
Satellite diabetes screening camp through OGTT

95JPFSM : Fasting blood sugar level and mild walking
glycemic levels in Bangladesh. Additionally, we did not have a non-intervention group in the study design for validating the walking intervention. Although we conducted the study in rural Bangladesh, our goal is to decrease the rise in diabetes prevalence in all of South Asia37). The existing pieces of evidence, sur-veys, and statistics point out that the incidence of diabetes is much higher in South Asian regions in comparison to developed and other developing countries. Such a high incidence causes a substantial health, social and financial burden, at present and for the future, for people in South Asia37). In South Asia, morbidity and premature and early mortality result from inadequate healthcare facilities for early detection, diagnosis, and initiation of therapy, with suboptimal management concerning diabetes and its associated complications and morbidities11). There are enough possibilities and hope on the primary prevention of diabetes through early lifestyle intervention and raising the awareness and perception of diabetes both in the pub-lic and with healthcare providers11). The future calls and agendas on the urgent need for concerted efforts by both public and private sectors to adopt and implement nation-wide programs focused on the prevention, management, cure, follow up and surveillance of DM and associated consequences.
Conclusion The current study clarified that the population with high physical activity has a lower prevalence of DM compared to people with low physical activity, and further five months daily walking program improves FBS levels and sugar tolerance in newly diagnosed diabetic populations in rural Bangladesh without medication. These findings imply that physical inactivity might be a potential con-tributing factor to the development of DM in Bangladesh, and mild exercise intervention has the potential to combat the DM epidemic in rural Bangladesh. This evidence can be a cornerstone for other South Asian rural contexts.
Acknowledgments
This study is supported by a research grant from Naito Memo-rial Foundation (Tokyo, Japan) and in part by a Grant-in-Aid for Scientific Research (Kiban C) from the Ministry of Education, Culture, Sports, Science, and Technology of Japan and Japan Society for the promotion of Science.
Financial Disclosure
There is no specific funding source to be mentioned.
Conflict of Interests
The authors declare that they have no conflict of interests.
convince female DM participants to participate in DM screening, as well as enroll in the intervention program. Undoubtedly, conducting the supervised walking inter-vention with a female supervisor dramatically helped in including more female participants in the Part 2 study. Furthermore, even when a male population in a rural con-text somehow has access to healthcare facilities, women groups, especially the married women in rural areas, are still mostly devoid of healthcare access, suffering higher levels of illness and health discomforts. Thus, the present study, mainly Part 2, has focused on female DM partici-pants who were active involved in the exercise interven-tion. The exercise intervention used in the current study was 3 km daily (1.5 km twice a day) walking for five months. This walking exercise represents about 3 METs35); and the average person can do this level of exercise easily with-out discomfort. In the current study, we found that such mild exercise improved FBS levels, sugar tolerance, waist circumference, and HDL-C levels (Fig. 2a-d). Although a previous study showed that above moderate-intensity exercise yielded beneficial effects for managing DM36), the current study provides the possibility that even mild exercise has a beneficial impact on DM. We have already found that a 10-week walking exercise intervention im-proved low-HDL-C levels in rural Bangladeshi women30); but that study could not see an improvement in FBS levels. The current study clarified that a long-term mild exercise intervention improved not only HDL-C levels, but also sugar tolerance in rural Bangladeshi. However, the current long-term exercise program did not visibly improve the cholesterol levels, triglyceride levels, LDL-C levels, and BMI of the participants. Thus, we need to investigate a longer duration of the exercise program in future studies. Besides, we cannot conclude that the ob-served effects on blood sugar following five months of mild walking are solely attributed to exercise activity, as we could not present the post-exercise effects of blood sugar levels in the control group. The sample size for the control group was not adequate for the presentation here when we excluded the missing values. Also, the drop out rate was significant, and there was an irregularity in the walking program. The analysis with a small size in the control group showed that there was a declining trend in blood sugar level after exercise, even though it was not statistically significant. Future studies should address these issues using a good study design. Besides, the limitations mentioned above, the present study has other limitations. The efficacy of this lifestyle intervention is limited to a specific remote rural region in Bangladesh, and may not represent the whole country contextually. A comparison of the current study design replicated in an urban context may provide additional unique insights for formulating affordable public health policy in Bangladesh. A similar study could also be con-ducted in the DM population that doesn’t have controlled

96 JPFSM : Jesmin S, et al.
References
1) Kharroubi AT and Darwish HM. 2015. Diabetes mellitus: the epidemic of the century. World J Diabetes 6: 850-867.
2) Craig ME, Hattersley A and Donaghue KC. 2009. Definition, epidemiology and classification of diabetes in children and adolescents. Pediatr Diabetes 10: 3-12.
3) Goyal R and Jialal I. 2019. Diabetes Mellitus Type 2 - Stat Pearls. Indian Dermatol Online J 10: 272-278.
4) Papatheodorou K, Banach M, Bekiari E, Rizzo M and Ed-monds M. 2018. Complications of diabetes 2017. J Diabetes Res 2018: 3086167.
5) Nickerson HD and Dutta S. 2012. Diabetic complications: current challenges and opportunities. J Cardiovasc Transl Res 5: 375-379.
6) Papatheodorou K, Papanas N, Banach M, Papazoglou D and Edmonds M. 2016. Complications of diabetes 2016. J Diabe-tes Res 2016: 6989453.
7) Cho NH, Shaw JE, Karuranga S, Huang Y, da Rocha Fer-nandes JD, Ohlrogge AW and Malanda B. 2018. IDF Diabe-tes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract 138: 271-281.
8) Diabetes. https://www.who.int/news-room/fact-sheets/detail/diabetes
9) National diabetes statistics report. 2010. CDC. Atlanta, GA: US Department of Health and Human Services. https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statis-tics-report.pdf
10) Statistics about diabetes. American Diabetes Association. https://www.diabetes.org/resources/statistics/statistics-about-diabetes
11) Ramachandran A, Snehalatha C and Wan Ma RC. 2014. Dia-betes in South-East Asia: an update. Diabetes Res Clin Pract 103: 231-237.
12) Biswas T, Islam A, Rawal LB and Islam MS. 2016. Increas-ing prevalence of diabetes in Bangladesh: a scoping review. Public Health 138: 4-11.
13) Marín-Peñalver JJ, Martín-Timón I, Sevillano-Collantes C and del Cañizo-Gómez FJ. 2016. Update on the treatment of type 2 diabetes mellitus. World J Diabetes 7: 354-395.
14) Wing RR, Bolin P, Brancati FL, Bray GA, Clark JM, Coday M, Crow RS, Curtis JM, Egan CM, Espeland MA, Evans M, Foreyt JP, Ghazarian S, Gregg EW, Harrison B, Hazuda HP, Hill JO, Horton ES, Hubbard VS and Jakicic JM. et al. 2013. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med 369: 145-154.
15) Research Group LA, Wadden TA, West DS, Delahanty L, Jakicic J, Rejeski J, Williamson D, Berkowitz RI, Kelley
DE, Tomchee C, Hill JO and Kumanyika S. 2006. The Look AHEAD study: a description of the lifestyle intervention and the evidence supporting it. Obesity (Silver Spring) 14: 737-752.
16) Wadden TA, Webb VL, Moran CH and Bailer BA. 2012. Lifestyle modification for obesity: new developments in diet, physical activity, and behavior therapy. Circulation 125: 1157-1170.
17) Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA and Nathan DM; Diabetes Prevention Program Research Group. 2002. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 346: 393-403.
18) Colberg SR, Sigal RJ, Fernhall B, Regensteiner JG, Blissmer BJ, Rubin RR, Chasan-Taber L, Albright AL and Braun B; American College of Sports Medicine; American Diabetes Association. 2010. Exercise and type 2 diabetes: the Ameri-can College of Sports Medicine and the American Diabetes Association: joint position statement. Diabetes Care 33: e147-e167.
19) Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA and Nathan DM; Diabetes Prevention Program Research Group. 2002. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 346: 393-403.
20) Hamasaki H. 2016. Daily physical activity and type 2 diabe-tes: a review. World J Diabetes 7: 243-251.
21) Akter S, Rahman MM, Abe SK and Sultana P. 2014. Preva-lence of diabetes and prediabetes and their risk factors among Bangladeshi adults: a nationwide survey. Bull World Health Organ 92: 204-213.
22) Afroz A, Alam K, Ali L, Karim A, Alramadan MJ, Habib SH, Magliano DJ and Billah B. 2019. Type 2 diabetes mellitus in Bangladesh: a prevalence based cost-of-illness study. BMC Health Serv Res 19: 601.
23) World Health Organization. 2015. Bangladesh health system review. Manila: WHO Regional Office for the Western Pa-cific.
24) Bangladesh Bureau of Statistics (BBS), Ministry of Planning. 2018. National accounts statistic. Asian Development Bank, Poverty in Bangladesh. 2017.
25) Jesmin S, Islam AMS, Akter S, Islam MM, Sultana SN, Ya-maguchi N, Okazaki O, Moroi M, Hiroe M, Kimura S, Wata-nabe T, Saturo K and Mizutani T. 2013. Metabolic syndrome among pre and post-menopausal rural women in Bangladesh: result from a population based-study. BMC Res Notes 6: 157.
26) Jesmin S, Akter S, Rahman MM, Islam MM, Islam AM, Sul-tana SN, Mowa CN, Yamaguchi N, Okazaki O, Satoru K, Kimura S, Hiroe M, Mizutani T and Moroi M. 2013. Disrup-tion of components of vascular endothelial growth factor an-giogenic signalling system in metabolic syndrome. Findings from a study conducted in rural Bangladeshi women. Thromb Haemost 109: 696-705.
27) Jesmin S, Islam MR, Islam AM, Mia MS, Sultana SN, Zae-di S, Yamaguchi N, Iwashima Y, Hiroe M and Watanabe T. 2012. Comprehensive assessment of metabolic syndrome among rural Bangladeshi women. BMC Public Health 12: 49.
28) Akter S, Jesmin S, Islam MM, Sultana SN, Okazaki O, Hi-roe M, Moroi M and Mizutani T. 2012. Association of age at menarche with metabolic syndrome and its components in rural Bangladeshi women. Nutr Metab (Lond) 9: 99.
Informed Consent
All study participants provided written informed consent.
Author Contributions
SJ designed and executed the study. SJ also drafted the manu-script. TS, NY, FS, AM, AR, MM, NS, SK, KW, FT, and HS assisted in sample collection and analysis. SJ and TS supervised this manuscript preparation and provided critical editing.

97JPFSM : Fasting blood sugar level and mild walking
29) Akter S, Jesmin S, Rahman MM, Islam MM, Khatun MT, Yamaguchi N, Akashi H and Mizutani T. 2013. Higher gra-vidity and parity are associated with increased prevalence of metabolic syndrome among rural Bangladeshi women. PLoS One 8: e68319.
30) Jesmin S, Sohael F, Rahman MA, Maqbool A, Islam MM, Shima T, Shimojo N, Moroi M, Yamaguchi N, Watanabe K, Takeda F and Soya H. 2020. Short-term lifestyle interven-tion program through daily walking improves circulatory low HDL level in rural Bangladeshi women. J Phys Fitness Sports Med 9: 181-190.
31) Oral Sugar Tolerance Test. https://www.diabetes.co.uk/oral-sugar-tolerance-test.html
32) Friedewald WT, Levy RI and Fredrickson DS. 1972. Estima-tion of the concentration of low-density lipoprotein cholester-ol in plasma, without use of the preparative ultracentrifuge. Clin Chem 18: 499-502.
33) Shah A and Kanaya AM. 2014. Diabetes and associated com-
plications in the South Asian population. Curr Cardiol Rep 16: 476.
34) American Diabetes Association. 2018. 2. Classification and diagnosis of diabetes: standards of medical care in diabe-tes-2018. Diabetes Care 41(Suppl 1): S13-S27.
35) Ainsworth BE, Haskell WL, Herrmann SD, Meckes N, Bas-sett DR Jr, Tudor-Locke C, Greer JL, Vezina J, Whitt-Glover MC and Leon AS. 2011. 2011 compendium of physical ac-tivities: a second update of codes and MET values. Med Sci Sports Exerc 43: 1575-1581.
36) Kodama S, Tanaka S, Saito K, Shu M, Sone Y, Onitake F, Suzuki E, Shimano H, Yamamoto S, Kondo K, Ohashi Y, Ya-mada N and Sone H. 2007. Effect of aerobic exercise train-ing on serum levels of high-density lipoprotein cholesterol: a meta-analysis. Arch Intern Med 167: 999-1008.
37) Waisundara VY and Shiomi N. 2017. Diabetes mellitus in South Asia. Diabetes and Its Complications. doi: 10.5772/intechopen.76391.
![Fasting and Power [Draft]imranhosein.org/inhmedia/books/fasting&power-new.pdf · Fasting in Islam – its basic objective 21 Fasting and internal spiritual power 26 Religion and the](https://img.pdfslide.us/doc/110x75/5ed9610cf59b0f56f45f61bd/fasting-and-power-draft-amppower-newpdf-fasting-in-islam-a-its-basic-objective.jpg)