Embed Size (px)
Citation preview
NOTES, CASES, DACRYOCYSTOGRAPHY USING POLYETHYLENE TUBING J A S W A N T S I N G H P A N N U , M.D.
Port Lauderdale, Florida
Dacryocystography is invaluable in the evaluation of the nasolacrimal duct system, but it is an awkward examination to administrate. The common technique is to inject radiopaque dye in the lower punctum while occluding the upper punctum with a lacrimal probe. The obvious disadvantage is that an assistant has to hold the lacrimal probe while the dye is being injected by the surgeon, also it is difficult to inject dye and get x-ray films
From the Department of Ophthalmology, Evans-ton Hospital, Evanston, Illinois.
Reprint requests to J. S. Pannu, M.D., 4070 West Broward Boulevard, Fort Lauderdale, Florida 33313.
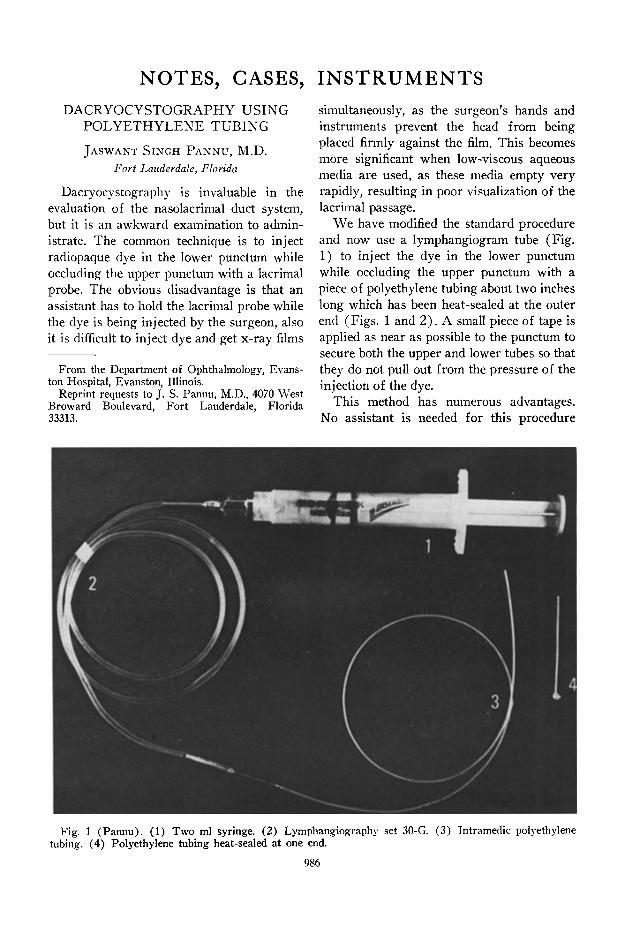
Fig. 1 (Pannu). (1) Two ml syringe. (2) Lymphangiography set 30-G. (3) Intramedic polyethylene tubing. (4) Polyethylene tubing heat-sealed at one end.
INSTRUMENTS simultaneously, as the surgeon's hands and instruments prevent the head from being placed firmly against the film. This becomes more significant when low-viscous aqueous media are used, as these media empty very rapidly, resulting in poor visualization of the lacrimal passage.
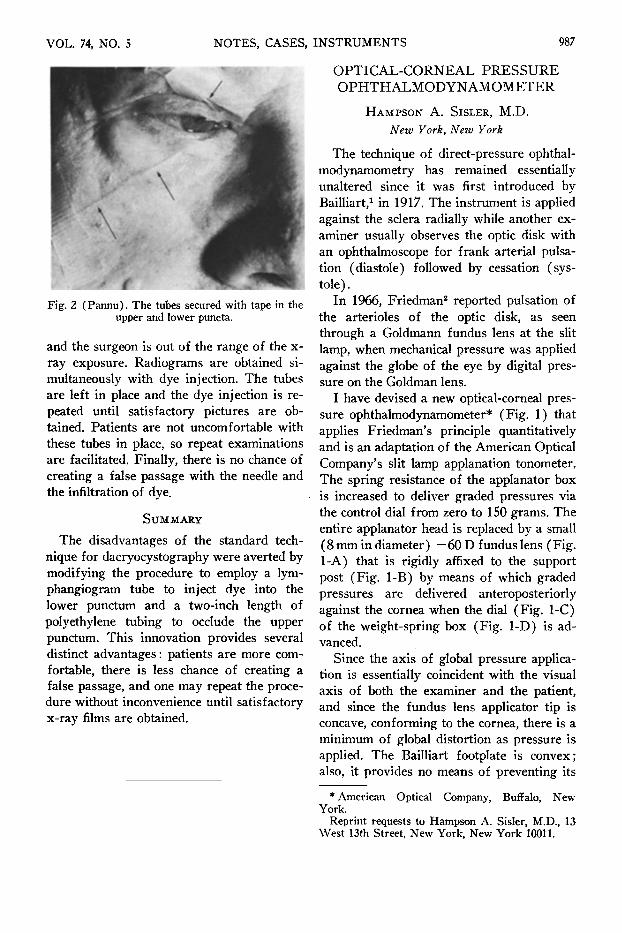
W e have modified the standard procedure and now use a lymphangiogram tube (Fig. 1) to inject the dye in the lower punctum while occluding the upper punctum with a piece of polyethylene tubing about two inches long which has been heat-sealed at the outer end (Figs . 1 and 2 ) . A small piece of tape is applied as near as possible to the punctum to secure both the upper and lower tubes so that they do not pull out from the pressure of the injection of the dye.
This method has numerous advantages. No assistant is needed for this procedure
986
VOL. 74, NO. 5 NOTES, CASES, INSTRUMENTS 987
Fig. 2 (Pannu). The tubes secured with tape in the upper and lower puncta.
and the surgeon is out of the range of the x-ray exposure. Radiograms are obtained simultaneously with dye injection. The tubes are left in place and the dye injection is repeated until satisfactory pictures are obtained. Patients are not uncomfortable with these tubes in place, so repeat examinations are facilitated. Finally, there is no chance of creating a false passage with the needle and the infiltration of dye.
SUMMARY
The disadvantages of the standard technique for dacryocystography were averted by modifying the procedure to employ a lym-phangiogram tube to inject dye into the lower punctum and a two-inch length of polyethylene tubing to occlude the upper punctum. This innovation provides several distinct advantages : patients are more comfortable, there is less chance of creating a false passage, and one may repeat the procedure without inconvenience until satisfactory x-ray films are obtained.
OPTICAL-CORNEAL PRESSURE OPHTHALMODYNAMOMETER
HAMPSON A. SISLER, M.D.
New York, New York
The technique of direct-pressure ophthal-modynamometry has remained essentially unaltered since it was first introduced by Bailliart,1 in 1917. The instrument is applied against the sciera radially while another examiner usually observes the optic disk with an ophthalmoscope for frank arterial pulsation (diastole) followed by cessation (systole).
In 1966, Friedman2 reported pulsation of the arterioles of the optic disk, as seen through a Goldmann fundus lens at the slit lamp, when mechanical pressure was applied against the globe of the eye by digital pressure on the Goldman lens.
I have devised a new optical-corneal pressure ophthalmodynamometer* (Fig. 1) that applies Friedman's principle quantitatively and is an adaptation of the American Optical Company's slit lamp applanation tonometer. The spring resistance of the applanator box is increased to deliver graded pressures via the control dial from zero to 150 grams. The entire applanator head is replaced by a small (8 mm in diameter) —60 D fundus lens (Fig. 1-A) that is rigidly affixed to the support post (Fig. 1-B) by means of which graded pressures are delivered anteroposteriorly against the cornea when the dial (Fig. 1-C) of the weight-spring box (Fig. 1-D) is advanced.
Since the axis of global pressure application is essentially coincident with the visual axis of both the examiner and the patient, and since the fundus lens applicator tip is concave, conforming to the cornea, there is a minimum of global distortion as pressure is applied. The Bailliart footplate is convex; also, it provides no means of preventing its
* American Optical Company, Buffalo, New York.
Reprint requests to Hampson A. Sisler, M.D., 13 West 13th Street, New York, New York 10011.





























