Embed Size (px)
Citation preview

Cedrón-Cheng and Ortiz, J Gastroint Dig Syst 2011, S:1 DOI: 10.4172/2161-069X.S1-003
Case Report Open Access
J Gastroint Dig Syst Video Capsule Endoscopy ISSN: 2161-069X JGDS, an open access journal
Hookworm Infestation Diagnosed by Capsule EndoscopyCedrón-Cheng Hugo1* and Ortiz Carlos2
1Gastroenterologist in British American Hospital, Lima, Perú2Gastroenterologist in Peruvian Social Security (ESSALUD) Arequipa, Perú
AbstractHookworm is one of the most common parasites around the world, especially in warm and moist places. Its
diagnosis is based on clinical symptoms of anemia, diarrhea, abdominal pain and weight loss, with the finding of parasites on stool samples. Although hookworm infection is rarely fatal, severe complications could happen due to iron deficiency anemia. Hookworm infestation sometimes is not easy to be detected in stools. We present two patients with different symptoms and negative stool test for Hookworms, both diagnosed on findings of capsule endoscopy.
*Corresponding author: Cedrón-Cheng Hugo, Gastroenterologist in British American Hospital, Lima, Perú, E-mail: [email protected]
Received October 26, 2011; Accepted November 12, 2011; Published November 14, 2011
Citation: Cedrón-Cheng H, Ortiz C (2011) Hookworm Infestation Diagnosed by Capsule Endoscopy. J Gastroint Dig Syst S1:003. doi:10.4172/2161-069X.S1-003
Copyright: © 2011 Hugo CC, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords: Hookworm; Capsule endoscopy
Introduction
Hookworms are estimated to infect more than 740 million people around the world, but most people who are infected are asymptomatic. Hookworm usually lives in the upper part of small bowel. Iron deficiency anemia secondary to loss of iron into the gut is the most significant risk of hookworm. Diarrhea, chronic abdominal pain, anorexia and weight loss are also frequent symptoms seen. The prevalence of infection is as high as 80% in tropical areas within developing countries, and only 20% in drier climates. Definite diagnosis is made by seeing hookworm eggs during stool examination, however sometimes its diagnosis can be missed. We present two cases of Hookworm infestation diagnosed by MiroCam® capsule endoscopy (CE) with negative previous work-up.
Case Report
First case
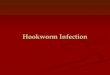
A 31-year-old policeman was seen for 6-month history of iron deficiency anemia, weakness and intermittent hematoquezia. He had recently not traveled. Laboratory tests revealed hemoglobin 6.8g/dL (normal 12.6-16 g/dL), microcitic; white blood cell count and platelets were normal. Upper endoscopy and colonoscopy did not find any significant lesion or site of bleeding that justified anemia. Initial stool tests showed only Blastocytis hominis and no other ova or parasites. He was sent to us to perform capsule endoscopy (CE). MiroCam® CE (Intromedic, South Korea) showed numerous white translucent rounded helminthic parasite attached to the mucosa covering mid and distal jejunum and proximal ileum. Based on the S-shaped appearance the likely diagnosis was Hookworm infestation. We sent special stool examinations that confirmed our impression. Patient was treated with albendazole. He responded completely, after nine months anemia and bleeding have resolved (Figure 1).
Second case
A 41-year-old man from Andean zone with 2-year history of chronic crampy abdominal pain mainly in both flank, intermittent non-bloody diarrhea and progressive weight loss. Pain had no relation to food. Physical examination was normal. Past and family medical history was not significant. Two upper endoscopies and one colonoscopy were normal. Lab results, including multiple stool examinations for parasites and cultures, and contrast enhanced abdominal tomography did not show any significant finding. He was treated like irritable bowel syndrome without improvement for that time. He came to us, and due to persistant symptoms, we suggested a capsule endoscopy rule out inflammatory or neoplasic small bowel
diseases. MiroCam® CE (Intromedic, South Korea) identified several translucent rounded worms in duodenum and jejunum, without any other finding, and hookworm infestation was diagnosed. He was treated with mebendazole. After six months, he gained weight, and diarrhea and abdominal pain disappeared (Figure 2).
Figure 1: Hookworm infestation covering jejunum and ileum.
Figure 2: Hookworm infestation in duodenum and jejunum.
Journal
of G
astro
intestinal & DigestiveSystem
ISSN: 2161-069X
Journal of Gastrointestinal & Digestive System

Citation: Cedrón-Cheng H, Ortiz C (2011) Hookworm Infestation Diagnosed by Capsule Endoscopy. J Gastroint Dig Syst S1:003. doi:10.4172/2161-069X.S1-003
Page 2 of 2
J Gastroint Dig Syst Video Capsule Endoscopy ISSN: 2161-069X JGDS, an open access journal
DiscussionStool should be examined for ova and parasites. However, because
egg laying may be delayed, examination should not be considered a sensitive test for identifying hookworm infection. Stool examinations may need to be repeated.
Small bowel examination is inaccessible to viewing with traditional endoscopy and only a part of it can be evaluated with push enteroscopy or retrograde ileoscopy. Capsule endoscopy is a minimally invasive method that can evaluated entire small bowel, and lead us to decide a follow-up procedure for targeted endoscopic treatment, or for obtaining histopathological diagnosis or for medical treatment. In both cases, capsule endoscopy was performed in order to rule out inflammatory bowel disease or neoplasic diseases, due to iron deficiency anemia or chronic abdominal pain and weight lost, parasites were an important but incidental finding.
Only a few abstract have been written showing a role of capsule
endoscopy in diagnosed parasite infections [1-3]. There is no standardized algorithm for evaluation of patients with iron deficiency anemia or unexplained chronic abdominal pain, but capsule endoscopy should be considered to rule out small bowel disease. Both patients had atypical presentations of hookworm infection and multiple negative stool exams. Capsule endoscopy is an important diagnostic method to evaluate entire small bowel and to exclude also parasites like hookworm specially in patients in tropical areas with previous negative work-up but persistence of symptoms.
References
1. Wu IC, Lu CY, Wu DC (2007) Acute hookworm infection revealed by capsule endoscopy. Endoscopy 39: E306.
2. Chen TH, Chen TY, Shyu LY, Lin CK, Lin CC (2006) Hookworm infestation diagnosed by capsule endoscopy (with video). Gastrointest Endosc 64: 277-278.
3. Morales CP, Ferrer G, Zuckerman MJ (2005) Hookworm detected by capsule endoscopy. Gastrointest Endosc 62: 782-783.
This article was originally published in a special issue, Video Capsule Endoscopy handled by Editor(s). Dr. Sherman M. Chamberlain, GeorgiaHealthServicesUniversity,USA








![Canine zoonoses-iacuc [Read-Only] - NDSU•Dog hookworm larva in the environment penetrate human skin and cause a condition called “cutaneous larval migrans” •The dog hookworm](https://img.pdfslide.us/doc/110x75/604390ee57b3c94fed62be03/canine-zoonoses-iacuc-read-only-ndsu-adog-hookworm-larva-in-the-environment.jpg)