Embed Size (px)
Citation preview

125© T O U C H B R I E F I N G S 2 0 0 7
a report by
Marcel lo Deraco
Surgical Oncologist, Peritoneal Malignancies Unit, Department of Surgery, National Cancer Institute of Milan
Hyperthermic Oncology
Peritoneal surface malignancy (PSM) is a clinical entity with an
unfavourable prognosis that characterises the evolution of neoplastic
diseases from the abdominal and/or pelvic organs, and could also be the
terminal stage of extra-abdominal tumours.1–3 Examples of diseases that
can spread mainly within the peritoneal cavity include appendiceal
tumours, ovarian cancer, colorectal cancer, abdominal sarcomatosis,
gastric cancer and peritoneal mesothelioma.
Loco-regional therapy is defined as the combination of cytoreductive
surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC).
The rationale of this combined therapy for PSM is based on the fact that
this clinical entity remains confined to the peritoneal cavity for most of its
natural history. This pattern of spread would seem to indicate the
potential usefulness of selectively increasing drug concentration in the
tumour-bearing area by direct IPEC instillation.4
The Rationale for Hyperthermic
Intraperitoneal Chemotherapy
The drug concentration attainable through an IPEC instillation approach
allows the intrinsic or acquired drug resistance to be overcome,
simultaneously minimising the systemic toxicity. Loco-regional drug
delivery under hyperthermia offers several advantages over the same
procedure performed at normal temperature. At 40–42ºC, neoplastic
cells become more chemosensitive due to an increase in the intracellular
concentration of drugs and in their activation process – especially for
alkylating agents – as well as to alterations in the DNA repair process.5,6
Formation of platinum DNA adducts after cisplatin exposure is enhanced
and/or adduct removal is increased in heated cells, resulting in relatively
higher DNA damage.7 Table 1 summarises the most common drug
association used in HIPEC.
Cytoreductive Surgery
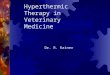
Each procedure that composes the peritonectomy technique to achieve
radical re-section of the tumour (see Figure 1) through CRS has a clearly
defined orderly sequence of surgical manoeuvres. One or more of the
following steps can be performed depending on the extension of primary
surgical staging or disease extension at the time of laparotomy in order
to achieve optimal residual status:
• greater omentectomy, right parietal peritonectomy and right colon
re-section;
• left upper quadrant peritonectomy, splenectomy and left parietal
peritonectomy;
• right upper quadrant peritonectomy and Glissonian’s capsule
re-section;
• lesser omentectomy, cholecystectomy, stripping of omental bursa
and antrectomy;
• pelvic peritonectomy with sigmoid colon re-section with or without
hysterectomy and bilateral salpingo-oophorectomy;
• other intestinal re-section and/or abdominal mass re-section; and
• bowel anastomoses.
Hyperthermic Intraperitoneal Chemotherapy
After CRS, four Tenckhoff catheters are placed in the abdominal cavity.
Two inflow catheters are placed in the right subphrenic cavity and at
deep pelvic level, respectively, and two further catheters are placed in the
left subphrenic cavity and in the superficial pelvic site. These catheters are
connected to a device.
The Device
HIPEC requires the employment of lung–heart machine, which comprises
a roller pump, a thermostat, a heat exchanger and an extra-corporeal
circuit. The perfusate flow is controlled and the heat exchanger adjusts
the temperature of perfusate by circulating water at the desired
temperature in the arterial phase of the circuit. The extra-corporeal circuit
consists of interconnected tubes that have: a) an input section (inflow); b)
an output section (outflow); c) an axis of rapid filling up; d) a central body
connected to a filter; e) a de-flow section; and f) a series of
multiperforated catheters in their extremities. The device should be
approved by CE accreditation. Several centres are currently using the
Performer LRT®.
The Perfusate
The perfusate, which is the liquid filling the circuit, could be of various
types: peritoneal dialysis solution;8 physiological solution;9 or a
composition of Normosol solution R pH 7.4 associated with Haemagel (in
the proportion 2:1).10 The recommended type of perfusate is isotonic salt
solutions and dextrose solutions.11
Modalities of Execution
The available modalities of execution are open, closed abdominal or semi-
closed techniques.12–15 In the closed technique, the skin of the abdominal
wall is temporarily closed with a running suture and the Tenckhoff
catheters are connected to the circuit in order to initiate the HIPEC.16 In
the open modality, also known as the Coliseum technique,17 the
abdomen is covered with a plastic sheet and drug vapour is evacuated to
protect the operating room personnel. The catheters are connected to
the extra-corporeal circuit and the pre-heated polysaline perfusate
containing the drug combination is instilled in the peritoneal cavity using
the heart–lung pump at a mean flow of 600–800ml/min for 60–90
minutes in order to achieve an intra-abdominal temperature of 42.5ºC.
State of the Art – Indications and Results of the Treatment
Table 2 provides information regarding the indications of CRS and HIPEC.
Cytoreductive Surgery and Intraperitoneal Hyperthermic Perfusion
Deraco_edit.qxp 17/7/07 12:15 Page 125
DOI: 10.17925/EOH.2007.0.1.125

126 E U R O P E A N O N C O L O G I C A L D I S E A S E 2 0 0 7
Hyperthermic Oncology
Colorectal Carcinoma
In 2004, colorectal cancer was the second most common form of cancer
(381,000 cases) and the second most common cause of death due to
cancer (203,700 deaths) in Europe. At initial diagnosis of colon cancer,
the peritoneal surface is tumorous in 10–15% of patients. The
peritoneal surface is the second most common site for cancer recurrence
after so-called curative colorectal cancer re-sections, occurring in as
many as 50% of patients.
Recent advances in the systemic treatment of advanced and/or metastic
colorectal cancer – with the introduction of oxaliplatin/irinotecan
associated or not with biological therapies – have allowed the
achievement of median survival of up to 20 months.18 However, these
favourable results should not be expected for patients with peritoneal
carcinomatosis, as this subset of patients represents a minority of
the population deemed as advanced and/or metastatic cases in the
main studies.
A systematic review of relevant studies on CRS with early peri-operative
IPEC before March 2006 has recently been published.19 Two randomised
controlled trials, one comparative study, one multi-institutional registry
study and the 10 most recent case-series studies were evaluated. The
median survival of patients treated by CRS associated with early peri-
operative IPEC varied from 13 to 29 months, and five-year survival rates
ranged from 11 to 19%. Patients who received complete cytoreduction
benefited most, with median survival varying from 28 to 60 months and
five-year survival ranging from 22 to 49%. The overall morbidity rate
varied from 23 to 44% and the mortality rate ranged from 0 to 12%. The
authors concluded that the current evidence suggests that CRS combined
with peri-operative IPEC is associated with improved survival compared
with systemic chemotherapy for peritoneal carcinomatosis from
colorectal carcinoma.
Gastric Cancer
In 2004, gastric cancer was the fifth most common form of cancer
(171,000 cases) and the third most common cause of death due to
cancer (137,000 deaths) in Europe. A meta-analysis has recently been
conducted involving 10 randomised controlled trials in which patients
with gastric cancer were randomly assigned to receive surgery combined
with IPEC versus surgery without IPEC.20 A significant improvement in
survival was associated with HIPEC alone (hazard ratio (HR) 0.60; 95%
confidence interval (CI) 0.43–0.83; p=0.002) or HIPEC combined with
early post-operative IPEC (HR 0.45; 95% CI 0.29–0.68; p=0.0002). The
authors concluded that HIPEC with or without early post-operative IPEC
after re-section of advanced gastric primary cancer is associated with an
improved overall survival.
Ovarian Cancer
Ovarian cancer – with an incidence of 44,000 cases a year in Europe in
2004 – remains the most lethal of all gynaecological malignancies, being
responsible for about 50% of all deaths from female genital tract
cancer.21 A recent systematic review of 14 studies published in the English
literature evaluating the effects of CRS+HIPEC in patients with ovarian
cancer has been carried out.22 Seven studies showed that patients with
complete cytoreduction had the greatest benefit. Median overall survival
for primary and recurrent disease ranged from 22 to 54 months, and
median disease-free survival from 10 to 26 months. The rates of
significant morbidity associated with this combined treatment were low,
ranging from 5 to 36%. The median mortality was 3% (range 0–10%).
Cytoreductive surgery combined with heated IPEC is a treatment option
for patients with ovarian cancer that is worthy of further investigation.
The Italian Society of Integrated Loco-regional Therapy (SITILO) is
conducting a prospective multicentre randomised study to test the
effectiveness of secondary CRS associated with HIPEC in patients with
epithelial ovarian cancer as second-line therapy.
Appendiceal Mucinous Tumours and
Pseudomyxoma Peritonei
A recent published systematic review reported on five observational
studies with relatively large series (n≥100) in patients affected by
pseudomyxoma peritonei (PMP). The median survival after the treatment
CRS+HIPEC ranged from 51 to 156 months. One-, two-, three- and five-
year survival rates varied from 80 to 100%, 76 to 96%, 59 to 96% and
52 to 96%, respectively. Overall morbidity rate varied from 33 to 56%,
and overall mortality rates ranged from 0 to 18%. In summary, some
promising long-term results were observed compared with historical
controls. Due to the rarity of this disease, a well designed, prospective,
multi-institutional study would be meaningful.23
Peritoneal Mesothelioma
According to an epidemiological study conducted in six western
European countries, projections for the period 1995–2029 suggest that
the number of men dying from mesothelioma each year will almost
Table 1: Drugs Schedule for Hyperthermic Intraperitoneal Chemotherapy
Author/Year Drug Dosage Drug Dose Duration of the IndicationPerfusion
Rossi et al. 200226 Cisplatin 43mg/l of perfusate Adriamycin 15.25mg/l of perfusate 90 min Ovarian cancer and
peritoneal mesothelioma
Fujimoto et al. 199327 Cisplatin 25.0mg/m2/l of Mitomycin C 3.3gm/m2/l of perfusate 60 min Pseudomyxoma peritonei
perfusate Colorectal cancer
Elias et al. 200228 Oxaliplatin 460mg/m2 in 2l/m2 30 min Colorectal cancer
of perfusate
De Bree et. al 200329 Docetaxel 75mg/m2 Ovarian cancer
HIPEC = hyperthermic intraperitoneal chemotherapy.
Table 2: Indications of Cytoreductive Surgery and HyperthermicIntraperitoneal Chemotherapy
Resectable PC from ovarian cancer after first-line chemotherapy*
Peritoneal mesothelioma30,31
Resectable PC from colorectal cancer32–36
Mucinous tumour from the appendix with Pseudomyxoma peritonei37,38
Carcinoma of the appendix with resectable PC39
Gastric cancer with resectable PC40–43
PC = peritoneal carcinomatosis. * Under phase III investigation.
Deraco_edit.qxp 17/7/07 12:16 Page 126

A4 adv Performer.ai 4/14/2006 4:37:20 PMRand_Bio_ad.qxp 9/7/07 02:29 Page 128

128 E U R O P E A N O N C O L O G I C A L D I S E A S E 2 0 0 7
Hyperthermic Oncology
double over the next 20 years, with a total of about a quarter of a million
deaths over the next 35 years. This projection has been attributed to the
wide use of asbestos in western Europe until 1980; substantial quantities
are still used in several European countries.24 Although these projections
were calculated for the pleural form of mesothelioma, a similar increase
in mortality due to the peritoneal form of the disease could be expected
in the next few years.
A recent systematic review evaluated the current evidence for CRS and
peri-operative IPEC for diffuse malignant peritoneal mesothelioma
(PSM).25 Seven observational studies were available for assessment; these
demonstrated an improved overall survival compared with historical
controls using systemic chemotherapy and palliative surgery. The median
survival ranged from 34 to 92 months. One-, three- and five-year survival
varied from 60 to 88%, 43% to 65% and 29% to 59%, respectively.
Peri-operative morbidity varied from 25 to 40% and mortality ranged
from 0 to 8%.
Conclusion
Loco-regional treatment for PSM is attracting increasing interest from the
scientific community. The procedure is time- and labour-consuming: the
mean duration of the procedure, according to the National Cancer
Institute of Milan experience, is nine hours; average duration of
hospitalisation is 23 days; and mean cost is €30,000. The institution of a
programme in PSM requires not only highly specialised human resources
but also complex technological facilities. At least 130 active centres in
western Europe have already set up such a programme for PSM.
However, each centre is able to perform no more than 50–60 procedures
per year due to its complexity.
Considering the projected constant increase of the prevalence of diseases
treatable by the procedure, more centres should be activated. In this
sense the establishment of clear policy and scientific guidelines is
mandatory in order to allow clinicians to perform CRS+HIPEC safely,
minimising treatment-related morbidity and mortality and maximising
results in terms of survival and quality of life. ■
Consensus Statement on Peritoneal Surface Malignancies
An International Workshop on Peritoneal Surface Malignancies took
place in Milan in December 2006. On this occasion, a panel of experts in
loco-regional therapy achieved an agreement pertaining to conceptual
and technical aspects regarding the methodology and indications of local
regional treatment of PSM. They also managed to establish general
treatment guidelines and investigational future prospects of main
peritoneal surface malignancies. More randomised data for each disease
are necessary to confirm the efficacy of this complex approach. On the
other hand, studies on biological markers with prognostic value should
also be conducted to improve the indications of the procedure. For more
information visit: www.peritonealworkshop2006.it and www.sitilo.org
Figure 1: The Various Phases of Cytoreductive Surgery – thePeritonectomy Procedure
Spleen and omentum
Stomach andlesser omentum
Rectum signoidcolon and pelvicperitoneum
Right colon andparictal peritoneum
1. Deraco M, Santoro N, Carraro O, et al., Tumori,1999;85(1):1–5.
2. Sugarbaker PH, Ann Med, 2004;36(1):9–22.3. Sugarbaker PH, Oncology (Huntingt), 2004;18(1):51–9.4. Markman M, Kelsen D, J Cancer Res Clin Oncol,
1992;118:547–50.5. Engelhardt R, Recent Results Cancer Res, 1987;104:136–203.6. Teicher BA, Kowal CD, Kennedy KA, Sartorelli AC, Cancer Res,
1981;41:1096–9.7. Hettinga JVE, Lemstra W, Meijer C, et al., Br J Cancer, 1997;75:
1735–43.8. Stephens AD, Alderman R, Chang D, et al., Ann Surg Oncol,
1999;6(8):790–96.9. Salle B, Gilly FN, Carry PY, et al., J Gynecol Obstet Biol Reprod
(Paris), 1993;22:369–71.10. Deraco M, Vaglini M, Santinami M, et al., Argomenti di
Oncologia, 1995;16:149–59.11. www.peritonealworkshop2006.com12. Kusamura S, Deraco M, Baratti D, et al., J Exp Clin Cancer Res,
2003;22(4):207–12.13. Glehen O, Osinsky D, Cotte E, et al., Ann Surg Oncol,
2003;10(8):863–9.14. De Simone M, Barone R, Vaira M, et al., J Surg Oncol,
2003;82(2):138–40.15. Stephens AD, Alderman R, Chang D, et al., Ann Surg Oncol,
1999;6(8):790–96.16. Vaglini M, Deraco M, Santinami M, et al., Argomenti di
Oncologia, 1995;16:161–7.17. Stephens AD, Alderman R, Chang D, et al., Ann Surg Oncol,
1999;6(8):790–96.18. Kelly H, Goldberg RM, SJ Clin Oncol, 2005;23(20):4553–60.
Review.19. Yan TD, Black D, Savady R, Sugarbaker PH, J Clin Oncol,
2006;24(24):4011–19. Review.20. Yan TD, Black D, Sugarbaker PH, Zhu J, et al., ANZ J Surg,
2007;77(Suppl. 1):A49.21. Pisani P, Parkin DM, Bray F, Ferlay J, Int J Cancer,
1999;83(1):18–29.22. Bijelic L, Jonson A, Sugarbaker P, Ann Oncol, 2007.23. Yan TD, Black D, Savady R, Sugarbaker PH, Ann Surg Oncol,
2007;14(2):484–92. Epub 2006 Oct 12. Review.24. Peto J, Decarli A, La Vecchia C, et al., Br J Cancer,
1999;79(3–4):666–72.25. Yan TD, Welch L, Black D, Sugarbaker PH, Ann Oncol,
2007;18(5):827–34.26. Rossi CR, Foletto M, Mocellin S, et al., Cancer,
2002:15(94):492–9.27. Fujimoto S, Takahashi M, Kobayashi K, et al., Surg Today,
1993;23(12):1094–8.28. Elias D, Bonnay M, Puizillou JM, et al., Ann Oncol,
2002;13(2):267–72.29. de Bree E, Rosing H, Beijnen JH, et al., Anticancer Drugs,
2003;14(2):103–10.30. Deraco M, De Simone M, Rossi CR, et al., J Exp Clin Cancer Res,
2003;22(4):41–5.31. Deraco M, Casali P, Inglese MG, et al., J Surg Oncol,
2003;83(3):147–53.32. Glehen O, Gilly FN, Sugarbaker PH, Scand J Surg,
2003;92:178–9.33. Cavaliere F, Perri P, Rossi CR, et al., J Exp Clin Cancer Res,
;22(4):29–3334. Glehen O, Kwiatkowski F, Sugarbaker PH, et al., CJ Clin Oncol,
2004;22(16):3284–92.35. Elias D, Blot F, El Otmany A, et al., Cancer, 2001;92:71–6.36. Verwaal VJ, van Ruth S, de Bree E, et al., J Clin Onc,
2003;21(20):3737–43.37. Deraco M, Baratti D, Inglese MG, et al., Ann Surg Oncol,
2004;11(4):393–8.38. Deraco M, De Simone M, Rossi CR, et al., J Exp Clin Cancer Res,
2003;22(4):35–9.39. Mohamed F, Gething S, Haiba M, et al., J Surg Oncol,
2004;86(1):10–15.40. Sugarbaker PH, Yu W, Yonemura Y, Semin Surg Oncol,
2003;21(4):233–48.41. Yu W, Whang I, Chung HY, et al., World J Surg,
2001;25(8):985–90.42. Bozzetti F, Vaglini M, Deraco M, Tumori, 1998;84(4):483–8.43. Akiyama H, Yamaoka H, Tanaka K, et al.,
Hepatogastroenterology, 1998;45(24):2079–86.
Deraco_edit.qxp 17/7/07 12:18 Page 128

July 25-28, 2007 - Foz do Iguazu, Brazil
Organisers : J. Goldman, G. Daley, C. Jamieson, J. Melo, N. Nardi, P. Quesenberry, L. Silla, D. Tabak, I. Weissman, M. Zago
ESH-SOCIEDADE BRASILEIRA DE HEMATOLOGIA E HEMOTERAPIA-COLEGIA BRASILEIRO DE HEMATOLOGIA CONFERENCE :
MOLECULAR CHARACTERISTICS OF NORMAL AND LEUKEMIA STEM CELLS
September 10-11, 2007 - Mumbai, India
Chairs : F. Cavalli, J. Goldman
Host chair : S. Advani, Scientific organiser : T. Mughal
ESO-ESH-INCTR FIRST GLOBAL CANCER INITIATIVE :LEUKAEMIAS
ESH_ad.qxp 9/7/07 02:27 Page 125