1
CYTOPATHOLOGY OF THE LIVER
23rd Annual Cytology Conference Pittsburgh PA
Gladwyn Leiman
OUTLINE
MICROSCOPY
Normal constituents
HCC and other primary liver tumors
Selected important metastatic tumors
Benign liver lesions
DIDACTICS
Indications, contras & complications
Immunochemistry in liver FNA
BENIGN CONSTITUENTS
Macroscopically: intact formed cores visible
Epithelial cells: - Hepatocytes, single and trabecular
- Bile duct cells
Mesenchymal cells:
- Endothelial lining cells - Macrophages (Kupffer cells)
- Fibroblasts
2
http://www.bioscience.org/2009/v14/af
/3576/fulltext.php?bframe=figures.htm
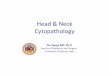
Benign hepatocytes and endothelial cells, trabecular arrangement
Benign liver plates, granular cytoplasm, endothelial cells
3
Benign hepatocytes with pigment
Benign bile duct cells
INDICATIONS AND CONTRA-INDICATIONS
Indication
Solid liver mass or masses
Contraindications Bleeding diathesis
Suspected vascular tumors
Diffuse liver disease eg cirrhosis Relative: Suspected Echinococcus/hydatid
Relative IN SOME CENTERS, Suspected HCC
4
EFFICACY AND SAFETY
Among the safest of all deep organ FNAS
Sensitivity >90% - operator dependent
Specificity ~100% - reader dependent
Hemorrhage 10-20/100,000 often
sub-capsular and contained
FATALITIES: LIVER FNA
21 deaths, 17 hemorrhage using 19 gauge
11 deaths, using 21 gauge or smaller
4 vascular: hemangioma 2, angiosarcoma 2 5 hemorrhage: HCC 2, met ca 3
1 sepsis 1 carcinoid crisis
Smith EH: Radiol 1991; 178:253-258
NEEDLE TRACK SPREAD
All reports show successful resection of NT and subcutaneous deposits
No fatalities in this group, irrespective of gauge
No survival differences with or without NTS
Hemorrhage = 6-31 per 100,000 liver FNA
NTS = 7 per 100,000
Some centers still choose not to sample apparently resectable HCCs pre-operatively
5
RESECTION/TRANSPLANTATION
HCCs found earlier, smaller, greater resectability
Transplantation (Milan criteria): < 3cm or < 5cm
But false positive radiology > micronodular cirrhosis
Gender: M>F, 2:1 - 5:1
Prognosis: dismal unless resectable
FNA: 90+% sensitive ~100% specific
HCC geographic pattern
6
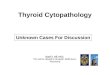
HCC Bare nuclei
HCC Bare nuclei of HCC mimic lymphoma
HCC, geographic pattern and wrapping
7
HCC, endothelial cell wrapping
HCC, bile plugs
HCC, transgressing vessels
8
Pleomorphism and nuclear inclusions
Macronucleoli and endothelial cells
HCC, clear cell variant
9
HCC, clear cell variant
Pleomorphic HCC, multinucleation
IMMUNOCHEMISTRY OLD AND NEW
(AFP) oncofetal antigen (
10
HCC, positive Glypican 3
CHILDREN, ADOLESCENTS, YOUNG ADULTS
Usual HCC Especially with vertical transmission of Hepatitis B virus
Hepatoblastoma USA 0.2/100,000, F,
Fetal, embryonal, macrotrabecular, small cell undifferentiated
Mixed epithelial and mesenchymal, +- teratoid features
Fibrolamellar variant HCC Age 2-35, mean 23, F>M, better prognosis
Large polygonal cells separated by fibrosis
Hepatoblastoma
11
Hepatoblastoma
Hepatoblastoma
Fibrolamellar HCC - LP
12
Fibrolamellar HCC, HP
Fibrolamellar HCC carcinoma
OTHER PRIMARY LIVER TUMORS
Epithelial:
Intrahepatic cholangiocarcinoma
Mesenchymal:
EHEE Epithelioid
hemangio-endothelioma
Angiosarcoma
Kaposis sarcoma
13
14
Full renal glomerulus in liver FNA
Benign ciliated hepatic foregut cyst
15
Benign ciliated hepatic foregut cyst
Degenerated benign ciliated hepatic foregut cyst
Echinococcus granulosus, hydatid cyst,
full scolex
16
E. granulosus, collarette of hooklets
E. granulosus, hydatid hooklets and capsule
17
EMH: megakaryocytes
EMH, section
Benign hemangioma
18
Benign hemangioma
Benign hemangioma
Benign hepatic adenoma:
Young females on OCs
Radiological mass lesion
Liver cells appear normal, lie singly
No bile duct cells
Rare endothelial cells, no wrapping
GPC3 negative
19
Herpes hepatitis?
Pitfall 1
Pitfall 2 GI epithelium
20
Benign biliary cyst, no cytopathology example
LIVER FNA: METASTATIC TUMORS
Far exceed primary tumors in FNA
Any tumor may ultimately involve liver
Often a prior history, diagnosis and slides
Liver mass may be initial manifestation
Sampling liver may be safer than primary
Liver involvement no longer untreatable
Recourse to immunochemistry required
ADENOCARCINOMA
Most common metastatic tumor type in the liver
- Mainly lung & GI colorectal, pancreas
- Breast and gynecologic sites
- Others uncommon - prostate, head & neck
Targeted immunochemistry usually required
Clinical history can save thousands!
Molecular markers increasingly important
21
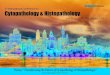
Metastatic mucinous adenocarcinoma
Metastatic pancreatic adenoca, well differentiated
Metastatic colorectal ca, necrosis
22
Metastatic colorectal
carcinoma
Metastatic adenoca, cytoplasmic vacuoles
Metastatic colonic ca, CEA
23
Metastatic duct carcinoma breast Metastatic breast cancer
Cholangiocarcinoma, intrahepatic -Clinical, radiologic, endoscopic data more useful than immunochemistry -Can be very well differentiated, desmoplastic and mucin-producing -Positive for CK7, CEA, MOC31,MUC 4 -Neg TTF1, CK20, p53
SELECTED METASTASES OF NOTE
Neuroendocrine tumors, small cell carcinoma
Squamous cell carcinoma
Melanoma
Gastrointestinal stromal tumor
Non-Hodgkins lymphoma
24
Neuroendocrine tumor, vascular core
Neuroendocrine tumor
Neuroendocrine carcinoma, small cell carcinoma
25
Metastatic squamous cell
carcinoma, necrosis
Metastatic squamous cell carcinoma
Metastatic melanoma, melanotic
26
Melanoma, single cells, INCI
Melanoma, S-100 immunostain
Metastatic GIST
27
Metastatic GIST
Metastatic GIST, c-Kit
Non Hodgkins lymphoma
28
BEST ANTIBODIES IN LIVER FNA
Glypican 3, HepPar1, Arginase (+ve in HCC)
CK 7, CK 20 profile (-ve in HCC)
CDX-2 (+ve in GI primaries)
TTF 1 (+ve for lung adenoca, NETs)
TTF 1 (also +ve in hepatocyte cytoplasm)
CD 56, SYN, CGA (+ve in NETs)
P63, p40 (+ve in squamous-cell ca)
S100, HMB45, MART-1 (+ve in melanoma)
COLLECT MATERIAL FOR MOLECULAR MARKERS !
- lung, colon, melanoma, breast, gastro-esophageal