Embed Size (px)
Citation preview
WHAT YOU KNOW, THOUGHT YOU KNEW, AND EVERYTHING YOU REALLY DIDN’T KNOW
Cystic Fibrosis
Kari Paca BSN, RN, CPNClinical Nurse II
(Cystic Fibrosis Liaison Level 8/9)

Inspiration
One Republic
Overview of Topics
● Pathophysiology of Cystic Fibrosis● Treating CF Pulmonary Exacerbations● Nutrition Basics ● CF Related Diabetes● Isolation and Infection Control for Patients● How to Work With This Challenging Population● The Future of Treatments

Basics of CF
● Average life expectancy currently is 38 years of age● Genetic, autosomal recessive disorder● Dysfunctional CFTR protein that doesn’t allow for
salt and water to cross the epithelial cell membrane correctly○ Thickened secretions in exocrine glands
● Systems affected○ Airways, sinuses, GI and reproductive
● Major Organs○ Lungs and pancreas
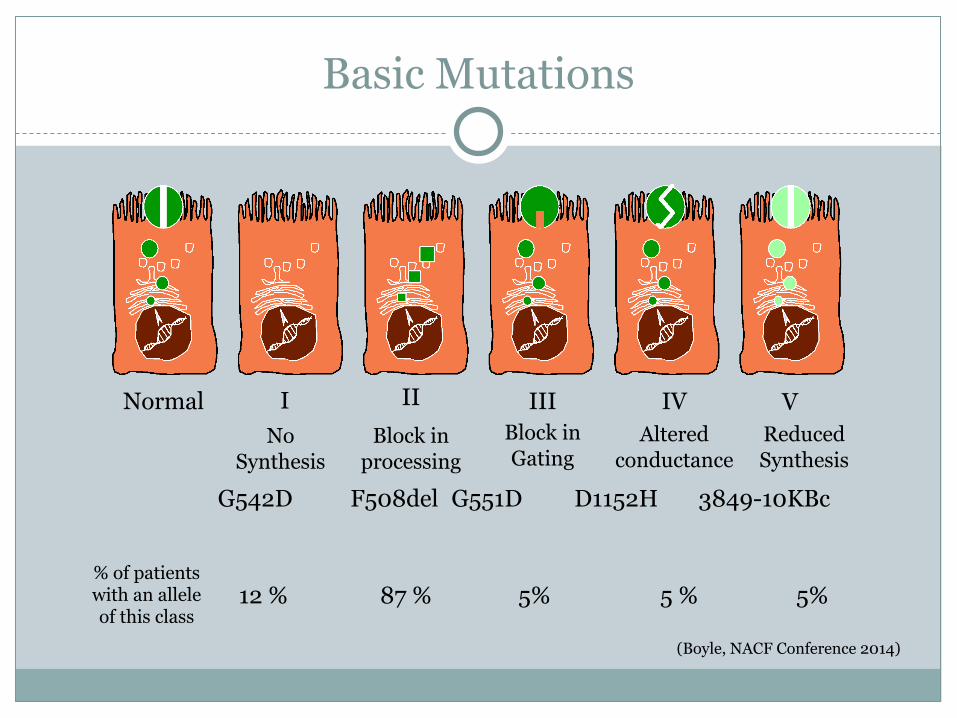
Basic Mutations
Normal I II III IV VNo
SynthesisBlock in
processingBlock in Gating
Altered conductance
Reduced Synthesis
G542D F508del G551D D1152H 3849-10KBc
% of patients with an allele of this class
12 % 87 % 5% 5 % 5%
(Boyle, NACF Conference 2014)

What Happens in the Lungs
● Lack of functioning CFTR● No fluid layer present● Sticky thick mucus that traps white blood cells,
bacteria, fungi, etc. ● Perfect environment for infection● Increased inflammation
● Increased amount of pro-inflammatory cytokines● Studies have shown early inflammation in infant lungs without the onset of
an infection (Courtney et al, 2004)
https://www.nacfconference.org/plen.archive.html
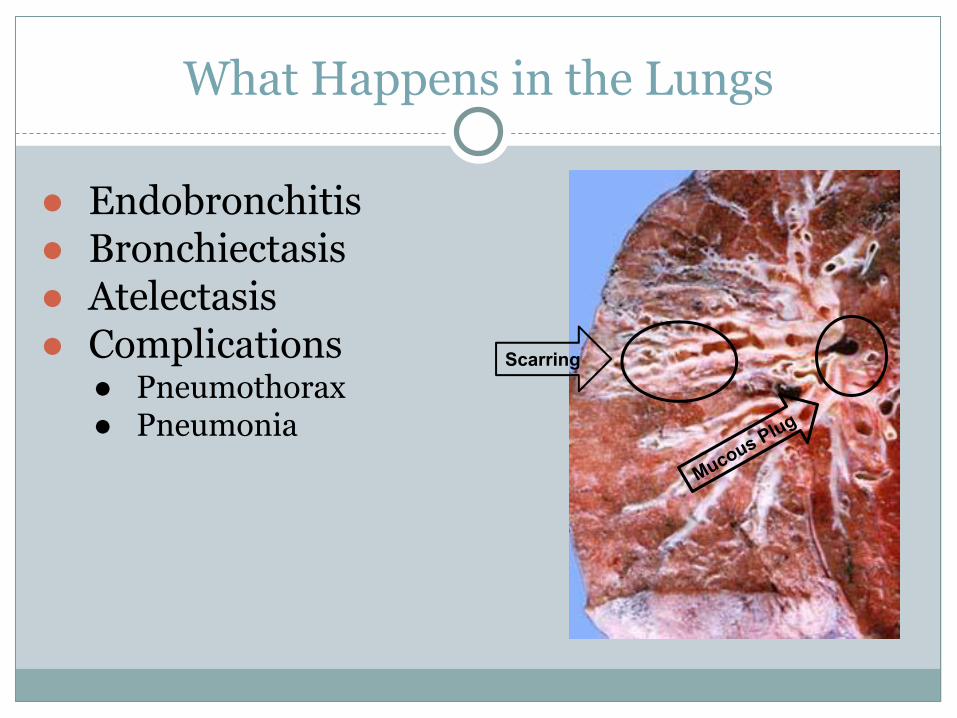
What Happens in the Lungs
● Endobronchitis● Bronchiectasis● Atelectasis● Complications
● Pneumothorax● Pneumonia
Scarring
Mucous Plug

CT Scan 14 Yr old Male
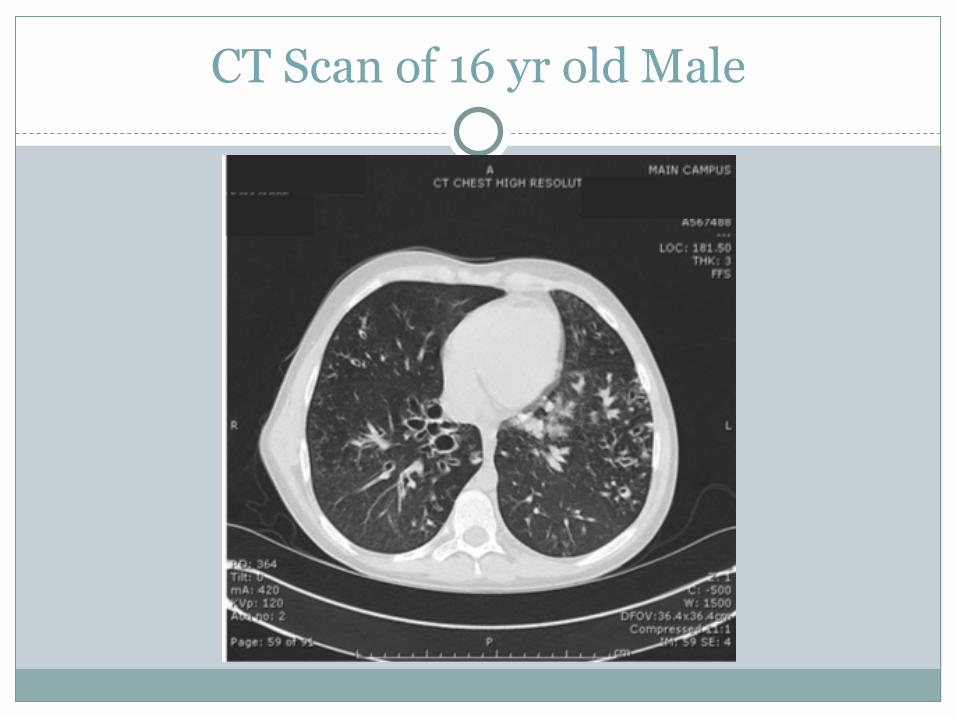
CT Scan of 16 yr old Male

Chest X-Ray Same 16 Yr old Male

Chest CT 6 Yr old Female
CF Exacerbations
● Common Bacteria● Staph Aureus
● MRSA/MSSA● Psuedomonas Aeruginosis● B. Cepacia (several strains)
● Fungus● Aspergillus
● Viruses● H. Flu● RSV
● MAC ● Mycobacterium Avium Complex

Treatments
● Typical stay is 10-14 days (YIKES)● Main focus=airway clearance.
● Increased to 3-4 times per day ● Vest, IPV, EzPap
● Antibiotics● Nebulizers
● Hypertonic Saline, Toby, Pulmozyme, Cayston● Exercise● Monitoring PFTS
● Want FEV1 to be very close, if not back to baseline
GI Tract and Cystic Fibrosis
● Abnormal CFTR protein affects:● Pancreas● Liver● Intestines
● Complications● Malabsorption● Impaired glucose tolerance● CFRD
Nutrition
● Significantly higher caloric needs● Children age 4-6 need 2,000-2,800 cal/day● Teens need 3,000-5,000 cal/day
● Malnutrition is associated with higher morbidity and mortality rates in individuals with CF (Davies et al, 2002)
● High Fat/ High Protein foods ● Does not mean just sugar
● Salt supplementation (usually younger kids)● BMI and lung function are highly correlated● Enzymes before meals, snacks, overnight feeds
CFRD
● Not DM Type I or II● Has components of both● Don’t make enough● Insulin resistance
● Most common comorbidity related to CF● About 16% of CFers have it● Gradual process ● Treatment
● +/- insulin● Not a limit on calories, still watch sugar● Blood sugar monitoring● OGTT
● Annual starting at age of 10 or earlier if suspected CFRD

What to Monitor
● Taking enzymes (time sensitive)● Blood sugar checks● Bowel Movements
● Are they having them?● Are they “normal”?● Distension or tenderness
● Supplements● New Process● Considered a snack for enzyme requirement
Infection Control and Isolation
● CF Glove and Gown● Least limiting● To protect them● Go anywhere with mask (including the fitness center)● Can be in teen lounge as long as no other CFer is in it
Infection Control and Isolation
● CF Droplet● Limiting ● Cannot go outside room to common areas● Can go directly outside wearing mask● Need to wear gown, glove, and mask for PFT● Specific signs for MRSA and B. Cepacia

Infection Control and Isolation
● Droplet● Trumps CF Droplet● When a pt has a virus● Cannot go outside of room period● Wears gown, glove, and mask to PFTs
Ask Your ISS for the in-room Signs!
Strategies to Work With Challenging Patients
● Long stays = more stress● BE A PRIMARY!!● Get Child Life Specialists involved
● Behavioral contract● Psych consults● Make a written schedule of their day with them● Make sure they have the new hospital handbook● Make sure the medical team knows if they always want
bedside rounding...even on the weekend● Meal cards for after hours
What is to Come of CF Treatment
● No Cure● New medications on the horizon
● Ivacaftor● Lumicaftor
● Investigating gene therapy● Incorporating Psychologists in care ● New methods to make it easier to take
respiratory equipment everywhere ● Increased rates of survival post lung-
transplant● 50% are alive at 5 years.
Thank-You!
● CF Team (outpatient) x76181● E-mail me: [email protected]● www.cff.org ● https://www.nacfconference.org/

Citations
● Boyle, M. (Director) (2014, October 8). Scaling the Mountain: The Journey to Delivering Transformational CF Therapeutics.. North American Cystic Fibrosis Conference. Lecture conducted from Cystic Fibrosis Foundation, Atlanta.
● Courtney, J., Ennis, M., & Elborn, J. (2004). Cytokines and inflammatory mediators in cystic fibrosis. Journal of Cystic Fibrosis, 3(4), 223-231. Retrieved March 13, 2015, from EbscoHost.
● Davies, P., Erskine, J., Hambidge, K., & Accurso, F. (2002). Longitudinal investigation of energy expenditure in infants with cystic fibrosis. European Journal of Clinical Nutrition, 56(10), 940-946. Retrieved March 13, 2015, from Academic Publishing Group.
● WWW.CFF.ORG












![Cystic Fibrosis 2[1]](https://img.pdfslide.us/doc/110x75/577daca71a28ab223f8e2cc3/cystic-fibrosis-21.jpg)


