Embed Size (px)
Citation preview
Academy of Acute Care Physical Therapy The Critical Edge www.acutept.org
Updated 2013
Academy of Acute Care Physical TherapyTask Force on Lab Values
2012 Members Roya Ghazinouri, Chair Samidha Deshmukh Sharon Gorman Angela Hauber Mary Krooh Elizabeth Moritz Babette Sanders Darrin Trees
2008 Members Holly McKenzie Dawn Piech Jim Smith
Approved by the Academy of Acute Care
Physical Therapy Board of Directors:
8/2008, 12/2011
LABVALUESINTERPRETATIONRESOURCES
LABVALUESRESOURCES 2013
2 | P a g e
It is the professional responsibility of the physical therapist to interpret available
laboratory values as a component of the examination and evaluation of a patient/client, to
suggest laboratory testing when indicated, and to use lab values to guide the
determination of safe and effective interventions for the patient/client. We, as physical
therapists, act as consultants in the rendering of our professional opinion and bear the
responsibility to advise the referring practitioner about the indications for physical
therapy intervention.
The Academy of Acute Care Physical Therapy created this referenced resource for members to
provide updated information and guide your inquiry into lab value interpretation. In this document
you will find the following:
Acute versus Chronic & Risk versus Benefit Considerations
Sex and Gender Considerations
Race and Culture Considerations
Tips for Collegial Discussions with Healthcare Providers
Peer Reviewed Resources
Websites
Search Engines
Updated Lab Values and Relevant Resources
Pulmonary Function Tests
Anticoagulation for Venous Thromboembolism
Recommended Reading List
Selected full-text articles
o Polich S. Competency based assessment in acute care: theory
behind the practice. Acute Care Perspectives. 2006;15(1):1-6.
o Garritan S, Jones P, Kornberg T, Parkin C. Laboratory values in
the intensive care unit. Acute Care Perspectives. 1995;3(4):7-11.
o Costello E, Elrod C, Tepper S. Clinical decision making in the
acute care environment: a survey of practicing clinicians. J Acute
Care Phys Ther. 2011;2(2):46-54.
DISCLAIMER: The Academy of Acute Care Physical Therapy has provided this information as a
resource to the membership. The Academy will not interpret lab values as this is the
professional responsibility of every clinician.

LABVALUESRESOURCES 2013
3 | P a g e
ACUTE VERSUS CHRONIC CONSIDERATIONS
In addition to reviewing the patient’s lab value and the given reference range, the
therapist should also consider the chronicity of the change in the lab value. Acute
changes, such as those associated with blood loss due to trauma or surgery, may require
the therapist to select a more conservative plan of care. Acute changes in lab values may
have more severe adverse events in patients due to the limited amount of time for the
patient’s system to compensate for this acute change. More chronic changes in lab
values, commonly associated with chronic conditions (e.g., CHF, COPD) or longer term
medical interventions (e.g., chemotherapy, radiation therapy) allow the patient a period of
time for their body to adapt or attempt to adapt to the changes in lab values, which may
allow them to have more resources to deal with potential adverse events caused by
increasing cardiorespiratory demand, mobility, and exercise.
RISK VERSUS BENEFIT CONSIDERATIONS
The fundamental consideration when evaluating lab values to determine appropriate
physical therapy plan of care revolves around the risk to the patient posed by proceeding
with intervention versus the benefits gained by the intervention. The therapist should
carefully consider all the potential adverse events that may present during intervention
based on the lab values out of the reference range, and consider the elevated risk should a
value fall in the critical range. Understanding of the lab test in question and the potential
adverse events is critical to this aspect of patient care. Likewise, the therapist should
consider the potential benefits of increased mobility and exercise that proceeding with the
intervention may provide to the patient. Not only should the immediate risks and benefits
of the therapy session in question be considered, but also the longer term risks and
benefits over the episode of care that may be present. Often it may be that the therapist
will need to consult with other members of the medical team to fully explore the risk
versus benefits of physical therapy intervention, and assist with the development of
facility policies, procedures, and/or protocols to assist in clinical decision making
regarding the use of lab values in determining aggressiveness of physical therapy
intervention.
LABVALUESRESOURCES 2013
4 | P a g e
SEX AND GENDER CONSIDERATIONS
Many lab results will have reference ranges reported as age-specific or sex-specific
values. With regards to interpretation of these reference ranges regarding sex-specific
norms, the therapist needs to consider the patient’s biological sex, gender, and gender
identity to avoid referencing the incorrect ‘normal’ value. A review of the differences of
these terms is provided in Table 1.
Table 1. Definitions pertaining to sex and gender roles.1
Term Definition
Sex Categorical differentiation between men and
women, assigned at birth based on brief visual
examination of external genitalia
Gender Binary social construct involving characteristics
distinguishing men from women
Gender
Identity
Person’s sense of being male or female
Transsexual Outdated term for person who feels they were
assigned the incorrect sex
Transgender Overarching term for persons with various
identities and expressions that are associated with
assignment of incorrect sex
Transition Legal, medical, and surgical processes that a
transsexual person may go through to correct the
incongruence of incorrect sexual assignment
Transwoman A person who identifies as female but was assigned
the male sex
Transman A person who identifies as male but was assigned
the female sex
Individual patients may be in the process of transitioning to their preferred gender
through medical (i.e., hormone replacement therapy), surgical (i.e., gender reassignment
surgery), and/or legal (i.e., amending legal documents to reflect gender identity) means to
correct incongruence of sex. Therapists should determine if patients in transition are
currently under treatment for medical transition, which may occur prior to or in
conjunction with surgical transition, and will be continued after surgical transition. If the
patient is on hormone replacement therapy, you should use the transitioned gender to
determine the reference value. If the patient is not receiving hormone therapy, you
should use their biological sex to determine the reference value. For example, a
transwomen on estrogen replacement therapy should have their lab values compared to
normal values of females due to the effects of estrogen on their physiology, whereas a
transman on testosterone should have their lab values compared to those of males due to
the effects of testosterone on their physiology. The key factor is not whether the medical
record assigns the patient a particular sex nor if the patient has undergone sexual
reassignment surgery, but whether they are taking hormone therapy that will affect their

LABVALUESRESOURCES 2013
5 | P a g e
physiology and lab chemistry. Knowing the medical transition status of a transsexual
person can result in avoidance of misinterpretation of lab values and ensure correct
application of normal reference values consistently.
Reference
1. Polly R, Nicole J. Understanding the transsexual patient: culturally sensitive care
in emergency nursing practice. Adv Emergency Nurs J. 2011;33(1):55-64.

LABVALUESRESOURCES 2013
6 | P a g e
RACE AND CULTURE CONSIDERATIONS
Census 2010 indicated increased minority demographic shifts in the United States.
1
McClatchey noted that “genetic heterogeneity within a population leads to person-to-
person phenotypic differences that can contribute to the variability in laboratory test
results.”2(p101)
In addition, due to culture and food preferences, it is not possible to
determine whether racial differences in laboratory values are genetic or related to lifestyle
alone (e.g., cholesterol).3 Therefore, physical therapists should be mindful of racial
differences in laboratory values and recognize that racial differences are not easily
conclusive because it is often difficult to separate effects of race per se from those of
other factors.
Genetic heterogeneity at the molecular level can lead to differences in the reactivity of a
patient’s DNA, proteins, or cells toward the nucleic acid probes and antibodies that are
used as reagents in many diagnostic tests.2 This type of genetic heterogeneity can result
in false-negative findings. Genetic variability will become an increasing consideration
for development of tests and analyzing test results as the field of clinical laboratory
medicine progresses.
In the United States, African Americans tend to have increased muscle mass and skeletal
structures than their Caucasian counterparts. Therefore, racial differences in serum levels
of creatine kinase and lactate dehydrogenase in adults and in serum alkaline phosphatase
in children are noted. African Americans also tend to have higher serum total protein
levels and higher serum levels of alpha, beta, and gamma globulins, IgG, and IgA than
Caucasians.2
There is a difference in hemoglobin (Hgb) values with African Americans having lower
hemoglobin compared to Caucasians.3 In addition, HgbA1c (A1C) lab values can be
altered in patients with sickle hemoglobin, which is present in 8% of the African
American population.4 Other studies have noted white-black differences in mean
hematocrit (Hct) readings that decreased over time due to quality of care rendered during
the onset of end stage renal disease regardless of socioeconomic status.5
Cultural competence is a non-negotiable skill, subject to rigorous testing similar to any
other core component of the physical therapy profession.6 Leavitt posits “future research
stands to provide a wealth of knowledge on the link between genetics and disparities in
health, but the differences remain to be seen.”7(p109)
Therefore, physical therapists must
consider racial variations in laboratory values in order for culturally competence care.
References
1. US Census Bureau. 2010 census shows America’s diversity. Available at:
http://www.census.gov/newsroom/releases/archives/2010_census/cb11-
cn125.html. Updated August 26, 2011. Accessed October 30, 2011.
2. McClatchey KD. Clinical Laboratory Medicine. 2nd ed. Philadelphia, PA:
Lippincott Williams & Wilkins;2002.

LABVALUESRESOURCES 2013
7 | P a g e
3. Overfield T. Biological Variation in Health and Illness: Race, Age, and Sex
Differences. 2nd ed. Boca Raton, FL:CRC Press;1995.
4. Hart CB. Race differences in long term management of diabetes in an HMO.
Response to Adams et al. Diabetes Care. 2006;29(6):1461.
5. Ward MM. Laboratory abnormalities at the onset of treatment of end-stage renal
disease. Are there racial or socioeconomic disparities in care? Arch Intern Med.
2007;167(10):1083-1091.
6. Purtilo RB. Thirty-First Mary McMillan Lecture: a time to harvest, a time to sow:
ethics for a shifting landscape. Phys Ther. 2000;80(11):1112–1119.
7. Leavitt RL. Cultural Competence: A Lifelong Journey to Cultural Proficiency.
Thorofare, NJ: Slack; 2010.

LABVALUESRESOURCES 2013
8 | P a g e
TIPS FOR COLLEGIAL DISCUSSIONS WITH HEALTHCARE
PROVIDERS
General guidelines
Do your research prior to approaching the healthcare provider.
Give them a copy of the research/evidence and ask to discuss the article
later in the day in a diplomatic way.
Follow up with them and be open minded.
Listen! Then follow up with your point, concern, or idea and cite your
resources.
KISS Principle:1
Keep
It
Short and
Simple
SBAR Communication Technique2
Situation: introduce yourself; succinctly and briefly explain the situation
Background: pertinent patient history; what preceded this point?
Assessment: summarize facts; what is going on in your judgment?
Recommendation: what do you want to happen next; what are you asking for?
References
1. KISS Principle. Wikipedia: the free encyclopedia. Available at:
http://en.wikipedia.org/wiki/KISS_principle. Updated September 27, 2011.
Accessed on September 29, 2011.
2. Institute for Healthcare Improvement: SBAR. Institute for Healthcare
Improvement. Available at:
http://www.ihi.org/knowledge/Pages/Tools/SBARTechniqueforCommunicationA
SituationalBriefingModel.aspx. Accessed on September 29, 2011.

LABVALUESRESOURCES 2013
9 | P a g e
PEER REVIEWED RESOURCES
NOTE: Past Acute Care Perspective and Journal of Acute Care Physical Therapy articles
may be purchased through the Academy of Acute Care Physical Therapy’s website at www.acutept.org/.
1. Hergenroeder A. Implementation of a competency-based assessment for
interpretation of laboratory values. Acute Care Perspectives. 2006;15(1):7-15.
2. Paz JC, West M. Acute Care Handbook for Physical Therapists. 3rd ed. Boston,
MA: Butterworth-Heinemann; 2008.
3. Malone D, Lindsay, K. Physical Therapy in Acute Care: A Clinician's Guide.
Thorofare, NJ: Slack; 2006.
4. Pagana, K, Pagana T. Mosby's Rapid Reference to Diagnostic & Laboratory
Tests. St. Louis, MO: Mosby; 2000.
5. Wallach J. Interpretation of Diagnostic Tests. 9th ed. Philadelphia, PA: Lippincott
Williams & Wilkins; 2011.
6. Fischbach F. Nurses' Quick Reference to Common Laboratory & Diagnostic
Tests. 5thed. Philadelphia, PA: Lippincott, Williams & Wilkins;2010.
7. Stiller K. Safety issues that should be considered when mobilizing critically ill
patients. Crit Care Clin. 2007;23(1):35-53.
8. Irion G. Lab values update. Acute Care Perspectives. 2004;13(1):1,3-5.
9. Garritan S, Jones P, Kornberg T, Parkin C. Laboratory values in the intensive care
unit. Acute Care Perspectives. 1995;3(4):7-11.
10. Deska K, Pagana T. Mosby Diagnostic and Laboratory Test Reference. 10th ed.
St. Louis, MO: Mosby; 2011.
11. Polich S. Competency based assessment in acute care: theory behind the practice.
Acute Care Perspectives. 2006;15(1):1-6.
12. Goodman CC, Boissonnault WG, Fuller KS. Pathology: Implications for the
Physical Therapist. 3rd ed. Philadelphia, PA: Saunders; 2008.
13. Hillegass E. Essentials of Cardiopulmonary Physical Therapy. 3rd ed.
Philadelphia, PA: Saunders; 2010.
14. Polly R, Nicole J. Understanding the transsexual patient: culturally sensitive care
in emergency nursing practice. Adv Emergency Nurs J. 2011;33(1):55-64.
15. Hanekom S, Gosselink R, Dean E, et al. The development of a clinical
management algorithm for early physical activity and mobilization of critically ill
patients: synthesis of evidence and expert opinion and its translation into practice.
Clin Rehabil. 2011;25(9):771-787.
16. Costello E, Elrod C, Tepper S. Clinical decision making in the acute care
environment: a survey of practicing clinicians. J Acute Care Phys Ther.
2011;2(2):46-54.
17. Gorman SL, Wruble Hakim E, Johnson W, et al. Nationwide acute care physical
therapy practice analysis identifies knowledge, skills, and behaviors that reflect
acute care practice. Phys Ther. 2010;90(10):1453–1467.
18. Masley PM, Havrilko C-L, Mahnensmith MR, et al. Physical therapist practice in
the acute care setting: a qualitative study. Phys Ther. 2011;91(6):906-919.
LABVALUESRESOURCES 2013
10 | P a g e
WEBSITES
1. Lab Tests Online: Understanding Your Tests page. American Association for
Clinical Chemistry Web site. Available at:
http://www.labtestsonline.org/understanding/index.htm. Accessed Sept 19, 2011.
Lab values, tests, and interpretation website that you can look up tests by name,
abbreviation, or by diagnosis. Peer-reviewed and non-commercial.
2. Medical Procedures and Tests, MedicineNet.com webpage. Available at:
http://www.medicinenet.com/procedures_and_tests/article.htm. Accessed Sept 19,
2011.
Part of the WebMD network, this page allows you to search for specific
information by test name. Peer and/or medical edited and content is not related to
commercial advertising on the site.
3. Interpretation of Lab Test Profiles page. Ed Uthman’s Web page. Available at:
http://web2.airmail.net/uthman/lab_test.html. Accessed Sept 19, 2011.
Site reference by the College of American Pathologists. Referenced and peer
edited.
4. Academy of Acute Care Physical Therapy website.
Available at: http://www.acutept.org. Accessed Sept 20, 2011.
Access to the peer-reviewed Journal of Acute Care Physical Therapy, practice
resources, and other information pertinent to acute care physical therapy practice.

LABVALUESRESOURCES 2013
11 | P a g e
SEARCH ENGINES
1. PubMed: A service of the U.S. National Library of Medicine and the National
Institutes of Health.
http://www.ncbi.nlm.nih.gov/pubmed/
2. Hooked on Evidence: APTA’s online database contains current research
evidence on the effectiveness of physical therapy interventions. APTA Members
only service.
http://www.hookedonevidence.org/
3. PEDro: Centre for Evidence-Based Physiotherapy’s website containing clinical
trial literature specific to physical therapy. Supported by numerous international
physical therapy associations.
http://www.pedro.fhs.usyd.edu.au/
4. Open Door: APTA’s research portal gives members free access to full-text
articles in more than 1,200 health care journals and periodicals. APTA Member
Only service.
http://www.apta.org/OpenDoor/
The following are databases on Open Door:
ProQuest Health & Medical Complete and ProQuest Nursing Journals
These databases serve the whole spectrum of users looking for
healthcare information — allied health, medical, and nursing
professionals; planners, administrators, and other researchers in
healthcare business and finance. Searchers have access to more than
1,000 publications in complete text and images. Search both
collections to maximize your results.
Cochrane Library
The Cochrane Library is a collection of databases that contain high-
quality, independent evidence to inform healthcare decision-making.
Cochrane reviews represent a high level of evidence on which to base
clinical treatment decisions. The Cochrane Database of Systematic
Reviews (CDSR) contains the full text of regularly updated systematic
reviews and protocols for reviews of the effects of healthcare. The
Database of Abstracts of Reviews of Effects (DARE) contains
structured abstracts of critical assessments of systematic reviews from
a variety of medical journals. The Cochrane Central Register of
Controlled Trials (CENTRAL) is a database of more than 350,000
abstracts of definitive randomized controlled trials and controlled
clinical trials from around the globe. Search them separately or
combined with the Cumulative Index to Nursing and Allied Health
Literature® (CINAHL®).

LABVALUESRESOURCES 2013
12 | P a g e
Cumulative Index to Nursing and Allied Health Literature®
(CINAHL®)
CINAHL® is the premier database for bibliographic information about
nursing and allied health research literature and topics. It indexes more
than 2,800 journals and other periodicals from the fields of nursing and
17 allied health disciplines. The database contains more than
1,000,000 abstract records dating back to 1982. Search CINAHL®
separately or combined with the Cochrane databases.

LABVALUESRESOURCES 2013
13 | P a g e
UPDATED LAB VALUES AND RELEVANT REFERENCES
These updated values are current as of 2011, and should be referenced as an addendum to
the following article included in this resource:
Garritan S, Jones P, Kornberg T, Parkin C. Laboratory values in the intensive care
unit. Acute Care Perspectives. 1995;3(4):7-11.
Values documented in
article
Updated values References for updated
values Creatinine Phospho - Kinase
(CPK) 25-225microL/L
30-170 U/L Porter RS, ed. The Merck Manual
of Diagnosis and Therapy. 19th
ed. Rahway, NJ: Merck;2011.
CPK-MB begins to rise at 2-4
hours, peaks in 12-24 hours and
returns to normal within 24-48
hours
CPK-MB begins to rise at 4-6
hours, peaks in 12-24 hours and
returns to normal within 48-72
hours
Fischbach F. A Manual of
Laboratory and Diagnostic Tests.
7th ed. Philadelphia, PA:
Lippincott Williams &
Wilkins;2004.
O2 sat: 95%-98% > 94% Porter RS, ed. The Merck Manual
of Diagnosis and Therapy. 19th
ed. Rahway, NJ: Merck;2011.
Partial pressure of oxygen in
arterial blood, PaO2: 80-100mm
Hg
> 80 mm Hg Porter RS, ed. The Merck Manual
of Diagnosis and Therapy. 19th
ed. Rahway, NJ: Merck;2011.
Adult male Red blood cells,
(RBCs): 4.7-5.5 x 104/microL
25-35 mL/kg Porter RS, ed. The Merck Manual
of Diagnosis and Therapy. 19th
ed. Rahway, NJ: Merck;2011.
Adult male hematocrit (Hct): 43-
49%
41-51% Porter RS, ed. The Merck Manual
of Diagnosis and Therapy. 19th
ed. Rahway, NJ: Merck;2011.
Adult male hemoglobin(Hgb):
14.4-16.6 Gm/dL
14-17Gm/dL Porter RS, ed. The Merck Manual
of Diagnosis and Therapy. 19th
ed. Rahway, NJ: Merck;2011.
Adult female white blood cells
(WBCs): 4,500-11,000 cells/mm3
3.9-10.7 x 103 Porter RS, ed. The Merck Manual
of Diagnosis and Therapy. 19th
ed. Rahway, NJ: Merck;2011.
Adult female RBCs: 4.1-4.9 x 104 20-30 mL/kg Porter RS, ed. The Merck Manual
of Diagnosis and Therapy. 19th
ed. Rahway, NJ: Merck;2011.
Adult female Hct: 38-44% 36-47% Porter RS, ed. The Merck Manual
of Diagnosis and Therapy. 19th
ed. Rahway, NJ: Merck;2011.
Adult female Hgb: 14-17 Gm/dL 12-16Gm/dL Porter RS, ed. The Merck Manual
of Diagnosis and Therapy. 19th
ed. Rahway, NJ: Merck;2011.
1. Hct < 25%-No exercise
permitted
1. Hct < 25%: essential
activities of daily living,
assistance as needed for
safety
DeVita, VT, Hellman S,
Rosenberg SA, eds. Cancer:
Principles and Practice of
Oncology. 7th ed. Philadelphia,
PA: Lippincott Williams &
Wilkins;2005.

LABVALUESRESOURCES 2013
14 | P a g e
2. Hct > 25%-Light exercise
permitted†
3. Approximately 30-32%-add
resistive exercise as
permitted†
2. Hct < 25-35%: essential
activities of daily living;
assistance as needed for
safety; light aerobics, light
weights (1-2 lbs) †
3. Hct > 35%, Ambulation and
self care as tolerated;
resistance and aerobic
exercises†
DeVita, VT, Hellman S,
Rosenberg SA, eds. Cancer:
Principles and Practice of
Oncology. 7th ed. Philadelphia,
PA: Lippincott Williams &
Wilkins;2005.
1. Hgb <8- No exercise
permitted
2. Hgb:8-10-light exercise
permitted†
3. Hgb >10-resistive exercise
permitted†
1. Hgb < 8gm/dL: essential
daily activities*
2. Hgb < 8-10gm/dL: Essential
activities of daily living,
assistance as needed for
safety; light aerobics, light
weights (1-2lbs)* †
3. Hgb > 8gm/dL, Ambulation
and self care as tolerated;
resistance exercises*†
DeVita, VT, Hellman S,
Rosenberg SA, eds. Cancer:
Principles and Practice of
Oncology. 7th ed. Philadelphia,
PA: Lippincott Williams &
Wilkins;2005.
1. Platelets (PLT) < 20,000: No
exercise
2. PLT: 20,000-50,000: Light
exercise (No PROM, but
light AROM is permitted)
3. PLT > 50,000: Resistive
AROM is permitted
1. PLT < 10,000 and /or
temperature > 100.5 degrees:
No therapeutic exercise/Hold
therapy
2. PLT: 10,000-20,000:
Therapeutic exercise/bike
without resistance
3. PLT > 20,000: Therapeutic
exercise/bike with or without
resistance
Samuelson K. Standard of care:
hematopoietic stem cell
transplant (HSCT) in-patient
phase. 2010; Brigham and
Women’s Hospital,
Rehabilitation Services.
* Recommendations for transfusion highly influence these recommendations and values,
and vary dependent on the cause of blood loss (e.g., trauma vs. perioperative) and other
comorbidities (e.g., chemotherapy, hypoxia). Interpret these values in conjunction with
the possibility of blood transfusion.
Liumbruno G, Bennardello F, Lattanzio A, Piccoli P, Rossetti G.
Recommendations for the transfusion of red blood cells. Blood Transfus.
2009;7(1):49-64.
† Updated for clarification 3/2013.

LABVALUESRESOURCES 2013
15 | P a g e
PULMONARY FUNCTION TESTS
Pulmonary function tests (PFTs): This is a group of tests which help to determine the
presence, nature, and extent of pulmonary dysfunction caused by conditions which cause
obstructive, restrictive, or mixed ventilatory defects. The ventilatory defect resulting from
increase in airway resistance is called an obstructive ventilatory impairment. When
ventilation is disturbed by a limitation in chest wall excursion, the defect is referred to as
a restrictive ventilatory impairment. When ventilation is altered by both increased airway
resistance and limited chest wall excursion, the defect is termed a combined or mixed
defect.
TYPES OF VENTILATORY
IMPAIRMENTS
COMMON EXAMPLES
Obstructive ventilatory impairment Chronic obstructive pulmonary disease (COPD)
Restrictive ventilatory impairment Fibrosis
Mixed ventilatory defect Pulmonary congestion
*Predicted values are based on the individual’s age, gender, ethnicity, height, and body size.
TYPES OF PFTS
TERMS (UNITS) OF
MEASUREMENTS
NORMAL
VALUES
FOR
MALE
(Liters)*
NORMAL
VALUES
FOR
FEMALE
(Liters)*
Airway flow rates:
Measure instantaneous or average
airflow rates during a maximal
forced exhalation to assess airway
patency and resistance
Inspiratory reserve volume (IRV)
Tidal volume (Vt)
Expiratory reserve volume (ERV)
Residual volume (RV)
IRV = 3.3
Vt = 0.5
ERV = 1.0
RV = 1.2
IRV = 1.9
Vt = 0.5
ERV = 0.7
RV = 1.1
Lung volumes and capacities:
Measure the various air-containing
compartments of the lung to assess
hyperinflation or reduction in
volume
Vital capacity (VC)
Inspiratory capacity (IC) = IRV + TV
Functional residual capacity (FRC) =
ERV + RV
Total lung capacity (TLC) = IRV +
ERV + RV
VC = 4.8
IC = 3.8
FRC = 2.2
TLC = 6.0
VC = 3.1
IC = 2.4
FRC = 1.8
TLC = 4.2
Gas exchange:
Measures the rate of gas transfer
across the alveolar capillary
membranes to assess the diffusion
process
Forced vital capacity (FVC)
Forced expiratory volume at the end
of a given time (t) in seconds (FEVt)
FEV1= FEVt at the end of 1
second
FEV2= FEVt at the end of 2
seconds
FEV3= FEVt at the end of 3
seconds
FVC >80% or > 0.80 of Predicted
value*
FEV1, 80%–85% of FVC
FEV2, 90%–94% of FVC
FEV3, 95%–97% of FVC
FEV1/FVC ratio is expressed as a
percentage

LABVALUESRESOURCES 2013
16 | P a g e
Spirograms and Flow Volume Curves: This is a graphical representation of spirometry
data.
FIGURE 1. Spirograms and flow volume curves. (A) Restrictive ventilatory defect. (B)
Normal spirogram. (C) Obstructive ventilatory defect.6
This figure is used with permission and was published in Textbook of Respiratory Medicine, 3rd
edition, Murray JF, Nadel JA, page 805. Copyright Elsevier 2000.
Steps for Spirometry data interpretation:
1. Assess and comment on the quality of test. The American Thoracic Society (ATS)
have published standard guidelines for clinically acceptable spirometry tests for the
purpose of minimizing the variability in the tests and for increasing data accuracy.
These guidelines are used for assessing the quality of a spirometry test.
2. Once the quality of the tests is confirmed, assess FVC, FEV1 and absolute
FEV1/FVC ratio and interpret using the following table:
FVC
FEV1
Absolute ratio
(FEV1/FVC) %
RESULT
Decreased Decreased or normal = or > 70% Restrictive ventilatory impairment
Decreased or normal Decreased < 70% Obstructive ventilatory
impairment
Normal Normal > 70% Normal spirometry

LABVALUESRESOURCES 2013
17 | P a g e
3. Once the type of pulmonary disease is identified severity of disease can be determined
by using the following guidelines:
SEVERITY OF DISEASE ABSOLUTE RATIO (FEV1/FVC)
Normal PFT Outcomes > 100 % of predicted values
Mild Disease 70-100% of predicted values
Moderate Disease 60-70 % of predicted values
Moderately severe Disease 50-60% of predicted values
Severe Disease < 50 % of predicted values
Consideration for Physical Therapy:
PFTs are an important diagnostic tool for identifying and assessing the severity of
pulmonary dysfunctions
Results will facilitate and help guide physical therapy interventions
References
1. Barreiro T. An approach to interpreting spirometry. Am Fam Physician.
2004;69(5):1107-1115.
2. Barrett KE, Barman SM, Boitano S, Brooks HL. Ganong’s Review of Medical
Physiology. 23rd ed. New York, NY:McGraw-Hill Medical;2009.
3. Crapo JD, Glassroth J, Karlinsky JB, King TE. Baum’s Textbook of Pulmonary
Diseases. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2004
4. Fischbach F. A Manual of Laboratory and Diagnostic Tests. 7th ed. Philadelphia,
PA: Lippincott Williams & Wilkins;2004
5. Murray JF, Nadel JA. Textbook of Respiratory Medicine. 3rd ed. Philadelphia,
PA: Saunders;2000:805.
6. Standardization of spirometry-1987 update. Statement of the American Thoracic
Society. Am Rev Respir Dis. 1987;136(5):1285-1298.
7. McCarthy K. Pulmonary Function Testing. Medscape Reference. Available at:
http://emedicine.medscape.com/article/303239-overview. Updated June 7, 2011.
Accessed September 29, 2011.

LABVALUESRESOURCES 2013
18 | P a g e
Anticoagulation Therapy for Venous Thromboembolism Medications Alternate
Names
Mode of
Administration
Lab Value
(reference
range)
Therapeutic
Range
When is a
patient safe
to mobilize?
Considerations Precautions
Warfarin Coumadin
Jantoven
Marfarin
Orally (PO)1 INR
(.9-1.1)
2.0-3.0
(achieved in 2-5
days)2
When in
therapeutic range
If not in therapeutic
range, check to see
if the patient is
therapeutic on other
anticoagulants (e.g.
unfractionated
heparin)
Increased risk of bleeding if
supratherapeutic
Unfractionated
Heparin
Subcutaneous
injection
IV infusion
(continuous)2
PTT
(23.8-36.6
seconds)
PTT of 2 to 3 times
the upper limit of
normal;
approximately 60 to
80 seconds or a
weight based
protocol3
When in
therapeutic range
Contact medical
team if specific
PTT goal range is
not documented
Increased risk of bleeding if PTT is
greater than specified therapeutic range
Potential complication: heparin-induced
thrombocytopenia6
Low molecular
weight Heparin
(LMWH)
Enoxaparin
Dalteparin
Tinzeparin
Lovenox
Fragmin
Innohep
Subcutaneous
injection2
Anti-factor Xa can
be measured to
determine
therapeutic range,
but it is not
routinely measured3
Patient considered
therapeutic 3-5
hours after 1st
injection4
3-5 hours after 1st
injection
administered
Potential complication: heparin-induced
thrombocytopenia6
Fondaparinux
Arixtra
Subcutaneous
injection3
Does not require
monitoring3
Peak
anticoagulation:
1.7 hours after 1st
injection5
Once patient has
reached peak
anticoagulation
Commonly used in
patients with
heparin induced
thrombocytopenia7
Contraindicated in patients with severe
renal impairment; cleared renally3

LABVALUESRESOURCES 2013
19 | P a g e
References
1. Warfarin. National Center for Biotechnology Information. U.S. National Library
of Medicine. Available at: www.ncbi.nlm.nih.gov/pubmedhealth/PMH0000634.
Updated September 1, 2008. Accessed September 21, 2011.
2. A Patient’s Guide to Antithrombotic and Thrombolytic Therapy: Comprehensive
Guide .American College of Chest Physicians. Available at:
http://accpstorage.org/newOrganization/patients/AT8/AT8ComprehensiveGuideP
atient.pdf. Accessed September 21, 2011.
3. Partners Handbook: Venous Thromboembolism Guidebook 5th
Edition. Brigham
and Women’s Hospital. Available at:
http://handbook.partners.org/template.aspx?uniqueID=38&pageName=Venous+T
hromboembolism+Guidebook+5th+Edition&level1ID=92. Accessed September
21, 2011.
4. Costello E, Elrod C, Tepper S. Clinical decision making in the acute care
environment: a survey of practicing clinicians. J Acute Care Phys Ther.
2011;2(2):46-54.
5. Bauer K. Therapeutic Use of Fondaparinux. UpToDate. Available at:
http://www.uptodate.com/contents/therapeutic-use-of-fondaparinux. Published
January 31, 2011. Updated May 2011. Accessed September 21, 2011.
6. Coutre S. Heparin-induced Thrombocytopenia. UpToDate. Available at:
http://www.uptodate.com/contents/heparin-
inducedthrombocytopenia?source=search_result&search=heparin&selectedTitle=
6%7E150. Updated June 9, 2011. Accessed September 21, 2011.
7. Kim ESH, Bartholomew JR. Venous thromboembolism. Cleveland Clinic
Foundation. Available at:
http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/cardiolo
gy/venous-thromboembolism/#bib42#bib42. Accessed October 11, 2011.

LABVALUESRESOURCES 2013
20 | P a g e
RECOMMENDED READING
Rothstein JM, Echternach JL, Riddle DL. The Hypothesis-Oriented Algorithm for
Clinicians II (HOAC II): a guide for patient management. Phys Ther.
2003;83(5):455-470.
Atkinson HL, Nixon-Cave K. A tool for clinical reasoning and reflection using
the International Classification of Functioning, Disability and Health (ICF)
framework and patient management model. Phys Ther. 2011;91(3):416-430.
Included in this resource are copies of the following:
Polich S. Competency based assessment in acute care: theory behind the practice.
Acute Care Perspectives. 2006;15(1):1-6.
Garritan S, Jones P, Kornberg T, Parkin C. Laboratory values in the intensive care
unit. Acute Care Perspectives. 1995;3(4):7-11.
NOTE: Updated values as of 2011 to supplement this article are located in
this resource under “Updated Lab Values and Relevant Resources.”
Costello E, Elrod C, Tepper S. Clinical decision making in the acute care
environment: a survey of practicing clinicians. J Acute Care Phys Ther.
2011;2(2):46-54.

Acute Care Perspectives Reprint permission granted courtesy of the Academy of Acute Care Physical Therapy www.acutept.org

Acute Care Perspectives Reprint permission granted courtesy of the Academy of Acute Care Physical Therapy
www.acutept.com
www.acutept.org

Acute Care Perspectives www.acutept.com
Reprint permission granted courtesy of the Academy of Acute Care Physical Therapy

Acute Care Perspectives www.acutept.com
Reprint permission granted courtesy of the Academy of Acute Care Physical Therapy

Acute Care Perspectives Reprint permission granted courtesy of the Academy of Acute Care Physical Therapy www.acutept.com
Academy
Academythe Academy
Academy
Academy membership.

Acute Care Perspectives 95/4/7-11 Reprint permission granted courtesy of the Academy of Acute Care Physical Therapy www.acutept.com

Acute Care Perspectives 95/4/7 11 Reprint permission granted courtesy of the Academy of Acute Care Physical Therapy www.acutept.com
-

Acute Care Perspectives 95/4/711 Reprint permission granted courtesy of the Academy of Acute Care Physical Therapy www.acutept.com

Acute Care Perspectives 95/4/7-11 Reprint permission granted courtesy of the Academy of Acute Care Physical Therapy www.acutept.com
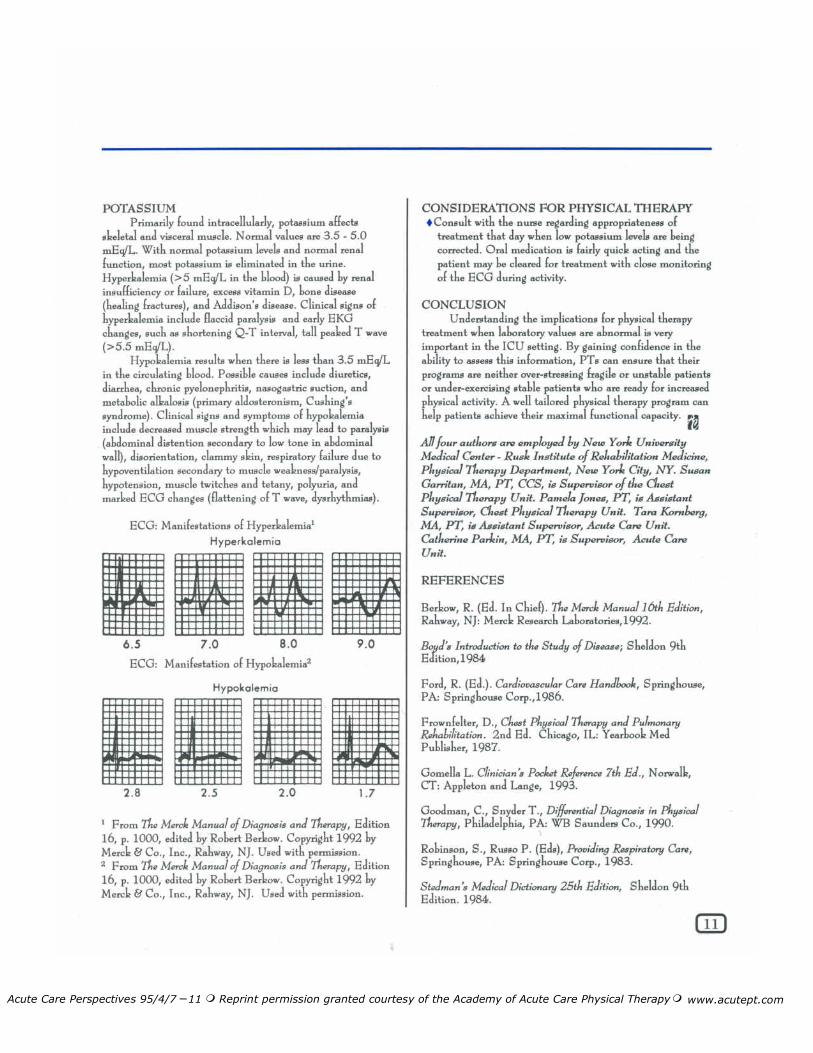
Acute Care Perspectives 95/4/7 -11 Reprint permission granted courtesy of the Academy of Acute Care Physical Therapy www.acutept.com

Acute Care Perspectives 95/4/7 -11 Reprint permission granted courtesy of the Academy of Acute Care Physical Therapy www.acutept.com
Academy of Acute Care PhysicalTherapy
Academy of Acute Care PhysicalTherapy
Academy

Summer 2011 ● Volume 2 ● Number 2JACPT
46
Clinical Decision Making in
the Acute Care Environment:
A Survey of Practicing
Clinicians
Ellen Costello, PT, PhD is Assistant
Professor, Program in Physical Therapy
at the George Washington University
900 23rd St, 6155, NW, Washington,
DC 20037 (Correspondence Address)
Dr. Elrod, PT, PhD is an Associate
Professor, Program in Physical
Therapy, Marymount University, 2807
North Glebe Rd, Arlington, VA 22207
Dr. Tepper, PT, PhD is President of
Rehab Essentials, Monkton, MD 21111
Ellen Costello, Cathy Elrod, Steven Tepper
ABSTRACT
Purpose: To investigate current practice trends in the acute care setting
using a case-based clinical decision-making survey to clarify when exercise
or ADL training would be contraindicated.
Methods: Acute care and cardiovascular and pulmonary section members
participated in an 8-question clinical decision-making survey. Choices
included decisions “to treat” or “not to treat” based on information
provided. Additional comments were analyzed. Demographic information
was also collected.
Results: 356 PTs responded to the survey (18% response rate). Number of
correct responses was calculated per case. Responses were also analyzed
by educational training and years of experience. Respondents chose the
optimal treatment choice more than 80% of the time in five of eight cases.
Mean scores ranged from 4.85 for bachelors-trained therapists with less
experience, to 6.76 for doctorally-trained therapists with greater experience.
A two-way ANOVA indicated a significant main effect for educational
training and years of experience and also a significant interaction (p=.017).
Incorrect responses in one of the eight cases appeared to be related to
therapists using outdated information or institutional guidelines.
Conclusions: Section members appear to be utilizing current evidence
to support their clinical decision making process. Respondents with more
experience, and those who continued their professional education were
more likely to choose the optimal treatment strategy.
Key Words: acute care, clinical decision making, exercise, clinical
experience
RESEARCH
REPORT© 2011 All rights reserved. Reproduction in whole or in part by permission only.Academy of Acute Care Physical Therapy

Summer 2011 ● Volume 2 ● Number 2 JACPT47
Clinical Decision Making in the Acute Care Environment: A Survey of Practicing Clinicians
A primary purpose of physical
therapist practice is to enhance human
performance as it relates to movement
and health. Physical therapists analyze
impairments, identify deficits in activities
and participation and provide safe,
effective, and efficient interventions in
order to restore patient/client function.1
As a complex interaction of systems
permits a patient/client to perform
activities of daily living (ADL), physical
therapists draw upon multiple domains
of knowledge when examining the
client’s ability to pursue and perform
goal-directed and personally desired
tasks.
A challenge for physical therapists is to
accurately synthesize and interpret the
diverse data surrounding the client’s
presentation to determine whether
participation in therapeutic exercise
or functional tasks would potentially
result in harm. During the evaluative
process, various factors influence the
therapist’s clinical reasoning. These
factors include the clinical setting and
available resources, the patient’s age,
medical diagnosis, signs and symptoms,
and health beliefs, and the therapist’s
knowledge, expertise, values, and use
of evidence and established guidelines.2,
3 A variety of formal guidelines are
available to assist physical therapists
in determining when formal exercise
testing would be contraindicated or
when a graded exercise test should
be terminated.4, 5 However, guidelines
to address absolute or relative
contraindications for participating in
activities of daily living or therapeutic
exercise as part of a physical therapy
plan of care are often inferred or
nonexistent.
PURPOSE
The purpose of this study was to
determine factors related to the ability
of clinicians to choose the optimal
course of action when presented with
scenarios that might require withholding
or terminating therapeutic intervention.
Clinicians were asked whether they
would treat or not treat a patient, or
whether they would terminate the
physical therapy session based on a
given patient case scenario. Additional
comments were solicited to clarify
the basis for the clinical decision.
Results may provide insight into current
clinical practice and highlight the use
of published guidelines or institutional
practices as part of the clinical decision
making process.
METHODS
Participants
Part ic ipants were a sample of
convenience of all individuals who
were physical therapists and current
members of the Cardiovascular and
Pulmonary (n = 947)6 or Acute Care
Sections (n = 1980)7 of the American
Physical Therapy Association (APTA) in
the Spring of 2010. These two groups
were chosen as they were considered to
have a range of clinical experience in the
evaluation and treatment of individuals
with medical conditions that a physical
therapist might encounter in the acute
care environment. An invitation to
complete the online survey was sent
via email to the listserv subscribers of
the aforementioned section members
asking for their participation in an online
survey. Not all section members are
listserv subscribers; hence the total
number of online surveys distributed
was approximately 2,000. A follow-up
reminder was emailed one week later
to optimize the return rate.
Development of the survey
A physical therapist with greater than 30
years of clinical and academic experience
in cardiovascular and pulmonary physical
therapy developed the survey to address
the following: 1) the dearth of clinical
practice guidelines regarding exercise
and functional training in the acute care
environment, and 2) to identify the
role if any, institutional practices and
guidelines contribute to the decision
making process when physical therapists
choose a particular course of action.
This researcher used current literature
to develop eight clinically-based
patient case scenarios that required
the respondent to make a decision
regarding the course of patient care.
Cases ranged from the treatment
of an individual following a total hip
replacement who was diagnosed with
a deep venous thrombosis, to a patient
following a Q wave MI who presented
with pedal edema, jugular venous
distention (JVD) and crackles. The
survey asked the respondents whether
they would either “treat” or “not treat”
the patient, or “terminate treatment”
or “continue treatment” based on
information provided. Respondents
were asked to keep in mind that they
would be providing usual care for this
scenario rather than making clinical
decisions based on outliers. Specifically,
the survey stated, “Keep in mind that
this is related to 80% of your patients
with this scenario and try not to think
of specific outliers. You are asked to
perform usual care for this patient
type.”
Additionally, demographic information
was collected to determine the
respondent’s educational training and
years practicing physical therapy. All
survey responses were anonymous
with no identifiable information. The
protocol for this study was reviewed
by the Institutional Review Board. A
full description of the survey questions
is found in Table 1 along with the
rationale and supporting literature for
the authors’ management choice.
DATA COLLECTION
A mixed methods design was used to
analyze this eight-question survey. In five
of the eight clinical scenarios presented,
the survey asked respondents whether
they would “treat this patient” or
“not treat this patient.” In three of
the eight clinical scenarios, the survey
asked the respondents whether they
would “continue the treatment in this
patient” or “terminate the treatment
in this patient.” Each survey question
also contained a comment section for
qualitative remarks.
DATA ANALYSIS
The data were analyzed using SPSS
Version 17.0 (SPSS Inc., Chicago,
IL). Descriptive statistics were used
to summarize the demographic
variables of the respondents, as well
as the percentage of participants who
chose the correct course of patient
Academy

Summer 2011 ● Volume 2 ● Number 2JACPT 48
management. Responses were coded
as either a “correct” or “incorrect” for
each case scenario and a total score per
respondent was calculated. A correct
decision for 3 of the cases was to “treat”
or “continue to treat” the patient. A
correct decision for 5 of the cases was
to “not treat” or “terminate treatment”
for this patient. The range of scores was
zero to eight; zero indicated that the
respondent did not choose a correct
response for any of the cases and eight
reflected that the respondent chose
the correct response for all eight of
the cases.
Survey responses were analyzed by
educational training and years of clinical
experience. Years of clinical experience
were collapsed into 3 groups (1-10, 11-
20, and > 21 years of practice) in order
to increase the cell size and facilitate
data analysis. A two-way ANOVA (3
x 3 design) was used to evaluate the
effects of type of educational training
analyzed as bachelor, masters, or
doctoral (including post-professional)
trained physical therapist and years of
clinical experience divided as described
above.8 Type of training and years
of clinical experience were classified
as independent variables and the
respondent’s total number of correct
responses was the dependent variable.
The Levene’s test was used to assess
the homogeneity of variance across all
groups prior to conducting the two-
way ANOVA.9 Additional comments
provided by the respondents were also
analyzed. Statements were reviewed
for patterns of meaning. Comments
were coded by two researchers using
the open coding method described
by Patton.10 Each coding schema was
operationally defined. Axial coding
then allowed for easier identification
of key words and phrases associated
with emerging themes. Themes were
developed and agreed upon by all three
investigators.
RESULTS
Three hundred and sixty-five individuals
responded to the survey. Based on the
inclusion and exclusion criteria, nine
respondents were excluded from data
analysis as they were physical therapists
assistants. A return rate of 17.8% was
calculated based on the total number
of respondents meeting the inclusion
criteria (n = 356) and the total number
of potential email listserv subscribers
(n = 2,000). Thirty-three percent of
the respondents were trained at the
bachelor’s level, 34% at the master’s
level and 33% described themselves
as trained at the doctoral level, which
included both professional and post-
professional DPT degrees. Thirty-eight
percent of survey respondents had been
practicing between one and 10 years;
30% between 11 and 20 years; and
32% over 21 years. Table 2 summarizes
the respondents’ type of educational
training and years of clinical experience
in addition to the average correct score
per group.
Frequency responses for each case
scenario were calculated and coded
as either correct (1) or incorrect (0).
Percent correct responses ranged
from 57.3% for Case 5 to 94.4% for
Case 8. Correct frequency responses
for all respondents per case are found
in Table 1. Respondents chose the
correct management decision greater
than 80% of the time in five out of
the eight cases. Correct frequency
responses by educational training and
grouped years of clinical practice are
found in crosstab format in Table 3.
The mean score ranged from 4.85 for
bachelors-trained physical therapists
with 1-10 years of clinical experience
to 6.76 for doctorally-trained physical
therapists with greater than 21 years
of clinical experience.
The Levene’s test for homogeneity of
variance found no significant difference
among the 9 groups (F=1.572, df=8,
p=.134).9 The results of the two-way
ANOVA indicated a significant main
effect for both educational training and
grouped years of clinical experience,
in addition to a significant interaction
between educational training and years
of clinical experience (p=.017) (see
Table 4). When both main effects
and interaction effects are significant
and the interaction is disordinal in
nature, Portney & Watkins8 suggest
that only the interaction effect should
be interpreted, therefore pairwise
comparisons of the main effects were
not conducted.
DISCUSSION
Educational Training and Years of
Clinical Experience
Our results indicated that respondents
with more years of clinical experience
coupled with an advanced degree were
more accurate in choosing the optimal
treatment strategy compared with less
experienced clinicians with baccalaureate
training. Although evidence to support
experience alone as a reliable criterion
for identifying expertise is lacking,
clinical experience is one component
that separates a novice from a master
clinician.11-14 Clinical decision-making
skills evolve over time as the physical
therapist gains more experience and has
more opportunities for observation of
expert clinicians, reflection on practice
decisions, and acquisition of knowledge
through continuing education.15-17
Although the bachelors-trained physical
therapists with less clinical experience
had the lowest mean score, one
must interpret these results with
caution as this group reflects only 7
respondents, less than 2% of the total
respondents. However, our results
support the importance of continuing
one’s professional education and the
importance of clinical experience, as
the groups with master’s or doctoral
level of training and those with greater
than 10 years of experience had higher
overall mean scores (Table 2).
The Cases
More than 80% of respondents chose
the correct management decision in five
of the eight clinical cases, suggesting that
the clinicians were aware of and utilizing
current evidence in their decision making
process. In three of the case scenarios
fewer than 80% of respondents chose
the correct response (cases 1, 4, and
5). Further analysis of the cases and
the respondents’ additional comments
helped to elucidate the therapists’
decision-making processes (see Table
5). In Case 1, the patient is being treated
for a recently diagnosed DVT with
Lovenox™, a low molecular weight
Clinical Decision Making in the Acute Care Environment: A Survey of Practicing Clinicians
Summer 2011 ● Volume 2 ● Number 2 JACPT49
heparin (LMWH) 2 days post-total hip
arthroplasty (THA). Although current
evidence supports early mobilization and
the use of compression stockings,18-21
almost 40% of the respondents
chose not to treat the patient. The
respondents were generally concerned
about the timeframe of administration
of the anticoagulant agent. Sixteen
respondents who chose not to treat
and additional respondents who chose
to treat commented that they would
only initiate treatment if Lovenox™
had been administered at least 24 hours
earlier. However, peak anticoagulation
has been noted 3-5 hours from
Lovenox™ administration.22, 23 Twelve
respondents stated they would check
the Prothrombin Time (PT) or Activated
Partial Thromboplastin time (aPTT) or
International Normalized Ratio (INR)
first before initiating treatment. These
guidelines pertain to Coumadin or
unfractionated heparin use rather
Clinical Decision Making in the Acute Care Environment: A Survey of Practicing Clinicians
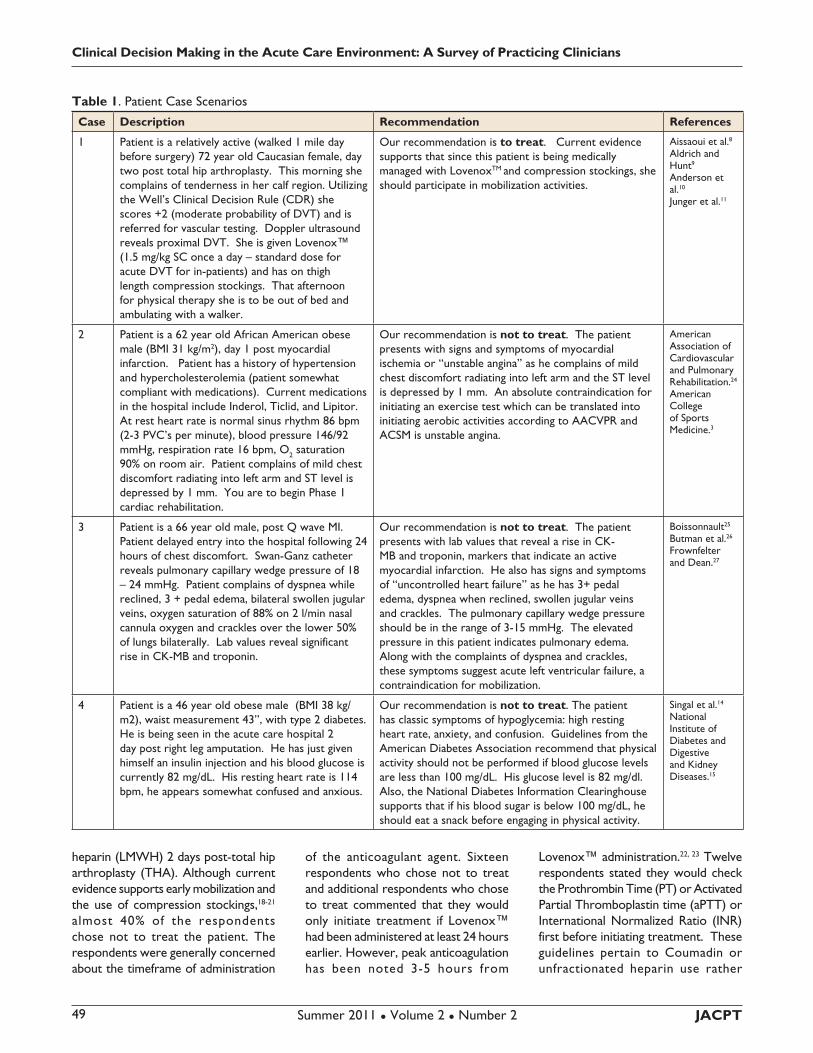
Table 1. Patient Case Scenarios
Case Description Recommendation References
1 Patient is a relatively active (walked 1 mile day
before surgery) 72 year old Caucasian female, day
two post total hip arthroplasty. This morning she
complains of tenderness in her calf region. Utilizing
the Well’s Clinical Decision Rule (CDR) she
scores +2 (moderate probability of DVT) and is
referred for vascular testing. Doppler ultrasound
reveals proximal DVT. She is given Lovenox™
(1.5 mg/kg SC once a day – standard dose for
acute DVT for in-patients) and has on thigh
length compression stockings. That afternoon
for physical therapy she is to be out of bed and
ambulating with a walker.
Our recommendation is to treat. Current evidence
supports that since this patient is being medically
managed with LovenoxTM and compression stockings, she
should participate in mobilization activities.
Aissaoui et al.8 Aldrich and Hunt9 Anderson et al.10
Junger et al.11
2 Patient is a 62 year old African American obese
male (BMI 31 kg/m2), day 1 post myocardial
infarction. Patient has a history of hypertension
and hypercholesterolemia (patient somewhat
compliant with medications). Current medications
in the hospital include Inderol, Ticlid, and Lipitor.
At rest heart rate is normal sinus rhythm 86 bpm
(2-3 PVC’s per minute), blood pressure 146/92
mmHg, respiration rate 16 bpm, O2 saturation
90% on room air. Patient complains of mild chest
discomfort radiating into left arm and ST level is
depressed by 1 mm. You are to begin Phase 1
cardiac rehabilitation.
Our recommendation is not to treat. The patient
presents with signs and symptoms of myocardial
ischemia or “unstable angina” as he complains of mild
chest discomfort radiating into left arm and the ST level
is depressed by 1 mm. An absolute contraindication for
initiating an exercise test which can be translated into
initiating aerobic activities according to AACVPR and
ACSM is unstable angina.
American Association of Cardiovascular and Pulmonary Rehabilitation.24
American College of Sports Medicine.3
3 Patient is a 66 year old male, post Q wave MI.
Patient delayed entry into the hospital following 24
hours of chest discomfort. Swan-Ganz catheter
reveals pulmonary capillary wedge pressure of 18
– 24 mmHg. Patient complains of dyspnea while
reclined, 3 + pedal edema, bilateral swollen jugular
veins, oxygen saturation of 88% on 2 l/min nasal
cannula oxygen and crackles over the lower 50%
of lungs bilaterally. Lab values reveal significant
rise in CK-MB and troponin.
Our recommendation is not to treat. The patient
presents with lab values that reveal a rise in CK-
MB and troponin, markers that indicate an active
myocardial infarction. He also has signs and symptoms
of “uncontrolled heart failure” as he has 3+ pedal
edema, dyspnea when reclined, swollen jugular veins
and crackles. The pulmonary capillary wedge pressure
should be in the range of 3-15 mmHg. The elevated
pressure in this patient indicates pulmonary edema.
Along with the complaints of dyspnea and crackles,
these symptoms suggest acute left ventricular failure, a
contraindication for mobilization.
Boissonnault25
Butman et al.26
Frownfelter and Dean.27
4 Patient is a 46 year old obese male (BMI 38 kg/
m2), waist measurement 43”, with type 2 diabetes.
He is being seen in the acute care hospital 2
day post right leg amputation. He has just given
himself an insulin injection and his blood glucose is
currently 82 mg/dL. His resting heart rate is 114
bpm, he appears somewhat confused and anxious.
Our recommendation is not to treat. The patient
has classic symptoms of hypoglycemia: high resting
heart rate, anxiety, and confusion. Guidelines from the
American Diabetes Association recommend that physical
activity should not be performed if blood glucose levels
are less than 100 mg/dL. His glucose level is 82 mg/dl.
Also, the National Diabetes Information Clearinghouse
supports that if his blood sugar is below 100 mg/dL, he
should eat a snack before engaging in physical activity.
Singal et al.14
National Institute of Diabetes and Digestive and Kidney Diseases.15

Summer 2011 ● Volume 2 ● Number 2JACPT 50
than Lovenox™. Routine coagulation
tests such as (PT/INR) or (aPTT) are
insensitive measures of Lovenox™
activity and thus would not be utilized
to measure its anticoagulant effect.
The only reliable way to monitor
LMWH is an expensive test that is not
utilized clinically unless the patient has a
history of significant renal impairment.22
Lovenox™ is considered therapeutic
once administered at the appropriate
dose. Furthermore, all of the randomized
controlled clinical trials examining
mobilization following diagnosis of
DVT and administration of Lovenox™
did not require a post-injection delay
before initiating activity.18-21 Thus,
some respondents are likely making
clinical decisions based on institutional
guidelines or they are not taking into
account the specific anticoagulant used
in the decision making process.
Case 4 involves a 46-year-old obese
patient with Type 2 DM, who is 2 days
post-right leg amputation. Following
insulin injection his blood glucose is
82mg/dL. He is confused with a HR
of 114. The literature suggests that
persons with diabetes should not
perform activity if exhibiting signs of
hypoglycemia or if the blood glucose
level is less than 100 mg/dL;24, 25 however
almost 40% of respondents chose
the incorrect response. Analysis of
additional comments suggests that
the therapists were aware that the
glucose levels were low and that this
warranted their close attention. Hence,
the intervention most frequently cited
was low-level bedside activity with
close monitoring of vital signs (n=24).
Other additional comments noted the
need to provide a snack and recheck
the blood sugar before proceeding
with treatment. One person noted
his institutional guidelines for exercise
and blood glucose was 70-110 mg/dL
and thus would have proceeded with
treatment. Respondents clearly were
addressing the low glucose levels in their
decision making process, but used these
values as only one piece of information
as they made their clinical decisions to
treat or not treat the patient.
Case 5 involved a 58-year-old woman
with leukemia awaiting a bone
marrow transplant. The patient was
Clinical Decision Making in the Acute Care Environment: A Survey of Practicing Clinicians
Case Description Recommendation References
5 Patient is a 58 year old female who is receiving a
bone marrow transplant following the diagnosis of
leukemia. Prior to the transplant the physicians
are inducing immunosuppression and trying to
kill off neoplastic cells in her bloodstream and
bone marrow. Her lab values reveal white blood
cell count of 2,200/mm3, Hemoglobin of 7.4 g/
dl, HCT 21%, platelets 3,200/mm3. Physiological
measurements reveal resting heart rate of 114
bpm, blood pressure 114/64 mmHg, oxygen
saturation 92% (on room air), respiratory rate of
16 bpm.
Our recommendation is to treat. While many of the
laboratory values (platelets, hemoglobin, HCT, WBC’s)
are below what is often thought as contraindications for
activity, this patient is relatively young, not a falls risk,
receiving treatment causing these iatrogenic changes,
while physiological parameters are within normal
limits. Treatment would be limited in physiological cost
(possibly to bed activities) and the patient would be
monitored closely.
Boissonnault25
APTA 28 University of Pittsburgh Medical Center29
Winningham30
6 Patient is a 54 year old male 2 days post TKA.
Patient has a long history of HBP and CAD.
Patient is comfortable at rest. With usual activity
patient complains of “chest tightness”, on the EKG
the ST segment is depressed by 2 mm. Patient
also appears pale.
Our recommendation is not to treat. The patient
has a history of cardiovascular disease. With activity
he demonstrates signs and symptoms of myocardial
ischemia: pallor, chest tightness, and ST segment
depression. The risk of precipitating a cardiac event
such as life-threatening dysrhythmias or myocardial
infarction with physical activity outweighs the benefits of
mobilization following joint arthroplasty.
American College of Sports Medicine4
7 Patient is a 72 year old female one day post-THA
with a known history of dysrhythmias. While
performing her activity she goes into ventricular
tachycardia (evidenced by EKG telemetry).
Our recommendation is to terminate treatment/
activity and notify medical personnel. Guidelines for
stopping an exercise test which can be translated into
stopping any aerobic activity according to AACVPR and
ACSM include ventricular tachycardia.
American Association of Cardio-vascular and Pulmonary Rehabilitation24
American College of Sports Medicine4
8 Patient is day two post-CABG. Physiological
measurements reveal resting heart rate of 94 bpm,
blood pressure 114/64 mmHg, oxygen saturation
92% (on room air), respiratory rate of 16 bpm.
With usual activity, the patient goes into sinus
tachycardia rate of 110 bpm, blood pressure of
132/70 mm Hg, oxygen saturation 94% (on room
air), respiratory rate of 20 bpm.
Our recommendation is to treat. All physiological
variables changed as expected with the onset of physical
activity. Heart rate increased but by less than 30 bpm
as recommended by AACVPR and ACSM for the
management of patients following CABG surgery.
American Association of Cardio-vascular and Pulmonary Rehabilitation26 American College of Sports Medicine.4
Table 1. Patient Case Scenarios (continued)
AACPT

Summer 2011 ● Volume 2 ● Number 2 JACPT51
immunosuppressed prior to surgery
with depressed low white blood cells,
hemoglobin and platelets counts. Vital
signs were as follows: resting HR of
114, RR of 16, BP of 114/64 and O2
saturation of 92% on room air. Although
our recommendation was to treat
based on existing guidelines and patient
history (relatively young patient, not a
falls risk, receiving treatment causing the
iatrogenic changes) approximately 42%
of respondents chose not to treat this
patient. Additional comments highlight
the concern of the respondents over the
depressed lab values, especially platelets
Clinical Decision Making in the Acute Care Environment: A Survey of Practicing Clinicians
Table 2. Type of Educational Training, Years of Experience and Mean Correct Score of Survey Respondents
Type of Educational Training N Percent Mean Score (s.e.)
Bachelor level trained PT 116 32.6 5.87 (.15)
Master level trained PT 121 34.0 6.26 (.11)
Doctoral or transitional Doctoral trained PT 119 33.4 6.51 (.12)
Years of Experience N Percent Mean Score (s.e.)
1 to 10 years 137 38.5 5.79 (.15)
11-20 years 107 30.0 6.47 (.11)
> 21 years 112 31.5 6.39 (.12)
Table 3. Correct frequency responses per case for 356 respondents
Case # Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8
% Correct 61.8 82.9 89.9 61.2 57.3 94.1 90.2 94.4
Table 4. Mean score by type of education and grouped years of clinical experience
Type of Education Grouped Years of
Experience
Number & (Percent) of
respondents
Mean (s.e.)
DPT or tDPT 1-10 years 76 (21.34) 6.27 (.12)
11-20 years 18 (5.05) 6.50 (.25)
> 21 years 25 (7.02) 6.76 (.21)
MSPT 1-10 years 54 (15.16) 6.24 (.14)
11-20 51 (14.33) 6.37 (.14)
>21 years 16 (4.49) 6.18 (.26)
BSPT 1-10 years 7 (1.96) 4.85 (.40)
11-20 years 38 (10.67) 6.55 (.17)
>21 years 71 (19.94) 6.22 (.12)
Table 5. Summary Table: Two –Way ANOVA: Effect of Educational Training and Grouped Years of Clinical
Experience on Score
Sum of Squares df Mean
Square
F Sig.
Educational Training 12.384 2 6.192 5.465 .005
Years of Practice 16.633 2 8.317 7.341 .001
Education Training *
Years Practice
13.395 4 3.474 3.066 .017
Error 393.133 347 1.133
Total 14625.00 356

Summer 2011 ● Volume 2 ● Number 2JACPT 52
in light of any proposed activities other
than low-level bed exercises. The
clinicians’ decision not to treat may
be based on limited exposure to this
particular patient population, which led
them to use lab value guidelines as an
absolute contraindication to treatment
without consideration of other factors.
Clinicians who frequently treat persons
with cancer may be more likely to
stretch the reference value boundaries
when weighing the benefits of mobilizing
the patient versus the deleterious
effects of continued bedrest.
Limitations
Generalizing the findings must be done
with caution for a number of reasons.
Although correct responses to the
clinical case scenarios were based on
current literature and confirmed among
all three authors, the survey itself was
constructed by only one author and
was not peer reviewed prior to its
administration. In addition, the cases
themselves were hypothetical in nature
and provided only a snapshot of the
information available to a clinician,
which may have contributed to the
respondent’s difficulty in choosing the
correct management decision.
The response rate was low (17.8%),
which may have resulted in response
bias. Individuals who found the
survey questions too challenging may
have elected not to complete the
survey, resulting in a respondent
pool more equipped to accurately
choose the correct management
decision. Additionally, the survey was
purposefully distributed to section
members, who would be familiar with
management of clients with medical
conditions one might encounter in the
acute care environment. Therefore
the respondents may be a select
group of individuals who have made a
commitment through their association
and section membership to continued
competency. Hence the findings cannot
be generalized to therapists who may
not be APTA or section members.
The demographic portion of the survey
did not address the respondent’s
current or past practice setting and
years of clinical experience in those
settings. This information coupled
with type of educational training and
total years of clinical experience would
have added another dimension to the
analysis offering further insight into
therapists’ decision-making process.
CONCLUSIONS
Overall more than 80% of the survey’s
participants answered five out of eight
cases correctly, suggesting that clinicians
who are members of the acute care and
cardiovascular and pulmonary sections
are utilizing current evidence to support
their clinical decision-making process.
Incorrect responses in two cases may
be related to the therapists’ current or
prior clinical experiences and subsequent
comfort level in treating a particular
patient population. Respondents with
less clinical experience may have been
less confident in their decision making
process, with the result that lab values
falling outside the normal range were
used as an absolute contraindication
for treatment without consideration of
other factors.
Incorrect responses in one case appear
to be related to lack of knowledge
regarding patient management following
LovenoxTM administration or the
result of institutionally-driven practice
guidelines. This highlights the need for
physical therapists to stay up to date
regarding patient medical management
and stresses the importance of educating
other health care professionals on our
role as exercise and activity specialists
in this environment. As exercise
specialists, we should act as the catalyst
for change for institutional practices
based on weak or nonexistent evidence
by bringing evidence-based practice to
the forefront of the clinical decision-
making paradigm.
Overall, physical therapists who have
more years of clinical experience and
who continued their professional
education were more likely to choose
the correct management decision
in these particular scenarios. This
emphasizes the importance of clinical
experience coupled with knowledge
in the clinical decision making process.
These individuals were more likely
to use guidelines judiciously, while
integrating other patient related factors
into their clinical decision making
process
REFERENCES
American Physical Therapy 1.
Association. Guide to Physical
Therapist Practice: Second Edition.
Alexandria, Va: American Physical
Therapy Association; 2003.
O'Sullivan S. Clinical decision 2.
making. In: O'Sullivan S, Schmitz T,
eds. Physical Rehabilitation. 7th ed.
Phila: F.A. Davis; 2007:3-25.
McGinnis PQ, Hack LM, Nixon-3.
Cave K, Michlovitz SL. Factors
that influence the clinical decision
making of physical therapists in
choosing a balance assessment
approach. Phys Ther. 2009;89:233-
247.
American College of Sports 4.
Medicine. ACSM's Guidelines for
Exercise Testing and Prescription.
8th ed. Philadelphia: Lippincott
Williams & Wilkins; 2010.
Hillegass E, Sadowsky HS. 5. Essentials
of Cardiopulmonary Physical Therapy.
2nd ed. Philadelphia: Saunders;
2001.
American Physical Therapy 6.
Cardiovascular and Pulmonary
Sect ion. American Physical
Therapy Cardiovascular and
Pulmonary Section Membership
and Leadership. Available at:
www.apta.org/AM/Template.
cfm?Section=Chapters&template=/
aptaapps/componentsonline/
componentsonline.cfm&processF
orm=1&componentType=Section
s&specChoice=L&convertList2For
m=yes. Accessed June 10, 2010.
American Physical Therapy 7.
Acute Care Section. American
Physical Therapy Acute Care
S e c t i o n M em b e r s h i p a nd
Leadership. Available at: www.
a p t a . o r g / A M / T e m p l a t e .
cfm?Section=Chapters&template=/
aptaapps/componentsonline/
componentsonline.cfm&processF
orm=1&componentType=Sections
&specChoice=I&convertList2Form
=yes. Accessed June 10, 2010.
Clinical Decision Making in the Acute Care Environment: A Survey of Practicing Clinicians
Academy of Acute Care PhysicalTherapy

Summer 2011 ● Volume 2 ● Number 2 JACPT53
Clinical Decision Making in the Acute Care Environment: A Survey of Practicing Clinicians
Table 6. Incorrect Response Comments by Case
Case 1 Case 2 Case 3
“THA with diagnosed DVT currently treated with Lovenox TM”
Wait 24 hours (n=16)yyWait 3 days (n=1)yyWait 12 hours if cleared yyby MD (n=1)Check PT/PTT or INR yyfirst (n=12)Clear with MD (n=7)yyNeed new order if it is yya new DVT (n=1)Do not treat b/c it is a yyproximal DVT (n=1)
“S/P one day AMI w/ r a d i a t i n g CP”
Treat while monitoring vitals yy&/or EKG (n=5)Check with MD (n=2)yyCheck with RN (n=2)yyModi fy intervent ion as yyindicated by S & S (n=1)1 mm only relative risk; do yybedside activities & monitorIf stable angina do deep yybreathing & relaxationSit EOB, watch ST segment & yysymptoms; education (n=1)Check troponin levels (n=1)yyStop treatment if symptoms yyworse or in CO (n=1)
“S/P Q wave MIDyspnea at rest, JVD, crackles”
Breathing activities to yyimprove O2 sat (n=3)I f g o o d h i s t o r i a n , yybasic ther. ex with VS monitoring (n=1)EOB activities; yy O2 prn & monitor VS (n=1)Dangle feetyy chair i f tolerated (n=1)Treat within parameters yyand modify to tolerance (n=1)Gentle ROM, no amb, no yyexercise (n=1)How long post MI?; ther yyex (n=1)Low level activity if cardiac yymarkers falling (n=1)Pending cardiology consult yy(n=1)
Case 4 Case 5 Case 6
“DM s/p amputation;Low Glucose & confused
Low leve l beds ide yyactivity closely monitor VS (n=24)Treat later that day yywhen glucose (n=5)P r o v i d e p r o t e i n , yycarbohydrates and modify and monitor (n=3)Give snack or ask RN yyto give him snack and recheck BS (n=6)Modify treatment as yyneed (n=2)Discuss why he is yyself injecting with RN (overmedicate?) (n=1)Check w/ RN to r/o yyAfib then start (n=1)OOByy chair (n=1)Gen t l e A / P ROM yy(n=1)Recheck BS & treat yybased on results (n=1)Norms @ our hospital yy70-110 so treat with monitoring (n=1)
“ B o n e M a r r o w T r a n s p l a n t with abnormal lab values”
Platelets too low (n=8)yyHgb too low (n=8)yyTalk to RN; if this is baseline yydo AROM/ADL as tolerated (n=3)Just take the history (n=1)yyCheck chart for last 3 days yybefore proceeding (n=1)Are WBC going up or down? yyHgb may be most compelling reason to not Rx (n=1)WBC, platelets, Hct too yylowMostly due to HR. Look at yyMD parameters for lab values (n=1)Hgb too low and HR too yyhigh (n=1)A b n o r m a l l a b v a l u e ; yyencourage ambulation if gait steady (n=1)Not clear presentation; is she yyimmunosuppressed but has not been transplanted?Depends on stand for Bone yyMarrow Transplant Unit. Needs special precautions b/c of WBC (n=1)Check with MD (n=1)yy
“S/P THA; h/o HBP & CAD; chest tightness and EKG changes”
Awa i t MD eva l and yycon t i nue i f f u r t he r intervention not indicated (n=1)Modi fy treatment as yyneeded (n=1)Hold mobility, check VS, yyconsult RN; ther ex/ROM (n=1)Back off activity & monitor. yyWhat is Hct? (n=1)Check with RN. Monitor yyactivity (n=1)Adjust POC according to yysymptoms (n=1)Check lab values (n=1)yyTher ex in sitting, find limits yyof activity w/ constant monitoring (n=1)
Case 7 Case 8
“One day post THA; h/o dysrhythmias w/ ventricular tachycardia (by telemetry)”
Monitor VS and adjust accordingly (n=5)yyDepends on symptoms, length of vtach, how extensive yyh/o dysrhythmias (n=1)If it was brief period and asymptomatic, would continue yyand monitor; if it persists, would stop (n=2)Give patient a rest period and resume if she regains yyNSR (n=1)Ask RN if normal vs. acute EKG change (n=3)yyCheck with RN & observe before deciding what to do yy(n=1)
“2 day post CABG; sinus tach 110; BP 132/70; O2 sat 94%”
Would return later to yyprovide short treatment of AROM & monitor VS (n=1)

Summer 2011 ● Volume 2 ● Number 2JACPT 54
Portney L, Watkins M, eds.8.
Foundations of Clinical Research:
Applications to Practice. 3rd ed.
Saddle River, NJ: Pearson Education
Inc; 2009.
Lewis-Beck MS, Bryman A, Liao TF.9.
The Sage Encyclopedia of Social Science
Research Methods. Vol 1. Thousand
Oaks, Ca: Sage Publications; 2004.
Patton MQ, ed.10. Qua l i ta t i ve
Evaluation and Research Methods.
3rd ed. Newbury Park, CA: Sage
Publications, Inc.; 2001.
Rassafiani M. Is length of experience 11.
an appropriate criterion to identify
level of expertise? Scand J Occup
Ther. 2009;16:247-256.
Jensen G, Shepard K, Gwyer JH, L. 12.
Attribute dimensions that distinguish
master and novice physical therapy
clinicians in orthopedics settings.
Phys Ther. 1992;10:711-722.
Jensen GS, K., Hack L. The novice 13.
versus the experienced clinician:
Insights into the work of the physical
therapist. Phys Ther. 1990;70:314-
323.
Embry D, Guthrie M, White O, 14.
Dietz J. Clinical decision making
by experience and inexperienced
pediatric physical therpists for
children with diplegic cerebral palsy.
Phys Ther. 1996;76:20-33.
Jensen G, Gwyer JH, L., Shepard K.15.
Expertise in Physical Therapy Practice.
2nd ed. St. Louis: Saunders; 2007.
Spake E.16. Clinical reasoning and decision
making of experienced clinicians and
entry-level physical therapist students.
[PhD]. Kansas: University of Kansas;
2003.
Wainwright SF, Shepard KH, L., 17.
Stephens J. Novice and experienced
physical therapist clinicians: A
comparison of how reflection
is used to inform the clinical
decision-making process. Phys Ther.
2010;90:75-88.
Aissaoui N, Martins E, Mouly S, 18.
Weber S, Meune C. A meta-analysis
of bedrest versus early ambulation
in the management of pulmonary
embolism, deep vein thrombosis, or
both. Int J Cardiol. 2009;137:37-41.
Aldrich D, Hunt D. When can 19.
the patient with deep venous
thrombosis begin to ambulate? Phys
Ther. 2004;84:268-273.
Anderson CM, Overend TJ, Godwin 20.
J, Sealy C, Sunderji A. Ambulation
after deep vein thrombosis: A
systematic review. Physiother Can.
2009;61:133-140.
Junger M, Diehm C, Storiko H, et al. 21.
Mobilization versus immobilization
in the treatment of acute proximal
deep venous thrombosis: A
prospective, randomized, open,
multicentre trial. Curr Med Res Opin.
2006;22(3):593-602.
U.S. Department of Health and 22.
Human Services. Drugs at FDA:
Lovenox. Available at: www.
accessdata.fda.gov/drugsatfda_
docs/label/2009/020164s085lbl.pdf.
Accessed November 5, 2010.
Frydman AM, Bara L, Le Roux Y, 23.
Woler M, Chauliac F, Samama MM.
The antithrombotic activity and
pharmocokinetics of enoxaprarin,
a low molecular weight heparin, in
humans give single subcutaneous
doses of 20 to 80 mg. J Clin
Pharmacol. 1988;28:609-618.
Singal RJ, Kenny GP, Wasserman 24.
DH, Castaneda-Sceppa C, White
RD. Physical activity/exercise and
type 2 diabetes: A consensus
statement from the American
Diabetes Association. DiabetesCare.
2006;29(6):1433-1438.
National Institute of Diabetes 25.
and Digest i ve and Kidney
Diseases. Hypoglycemia. Available
at: diabetes.niddk.nih.gov/dm/
pubs/hypoglycemia/. Accessed
November 7, 2010.
Amer i c an A s soc i a t i on o f 26.
Cardiovascular and Pulmonary
Rehabilitation. Guidelines for
Cardiac Rehabilitation and Secondary
Prevention Programs. 4th ed.
Champaign, IL: Human Kinetics;
2004.
Boissonnault WG.27. Primary Care for
the Physical Therapist: Examination
and Triage. 2nd ed. St. Louis:
Saunders; 2011.
Butman SM, Ewy GA, Standen 28.
JR, Kern Kb, Hahn E. Bedside
cardiovascular examination in
patients with severe chronic heart
Clinical Decision Making in the Acute Care Environment: A Survey of Practicing Clinicians
failure: Importance of rest or
inducible jugular venous distention.
J Am Coll Cardiol. 1993;22:968-974.
F r o w n f e l t e r D , D e a n E .29.
Cardiovascular and Pulmonary Physical
Therapy: Evidence and Practice. 4th
ed. St. Louis: Mosby; 2006.
Laboratory values interpretation
resource. Available at: www.
acutept.org/displaycommon.
cfm?an=1&subarticlenbr=27#lab_
values. Accessed November 7,
2010.
University of Pittsburgh Medical 31.
Center. Stem cell transplant
rehab: what to expect. Available
at: www.upmc.com/healthatoz/
patienteducation/documents/
stemcell.pdf. Accessed November
7, 2010.
30. Academy of Acute Care Physical
Therapy
Academy of Acute CarePhysical Therapy