Embed Size (px)
Citation preview
Cyanotic congenital heart disease
Case Presentation
• Term male infant delivered by spontaneous vaginal delivery and appears cyanotic at birth
• respiratory rate 70 bpm, baby has grunting and nasal flaring with chest retractions
• Heart murmur on exam
• ABG: pH 7.32 PaCO2 45 PaO2 35
Case Presentation
• What is happening?
• Have you seen this problem?
• What is causing her problem?
• What can we do about it?
Cyanosis defined
• Bluish discoloration of skin or mucous membranes
• Presence of 5g/dL of deoxyhemoglobin• Low flow areas with increased oxygen
extraction have more deoxyhemoglobin• High flow areas with less extraction
should not have enough deoxyhemoglobin to appear cyanotic– Under normal circumstances you should not be able to
extract enough O2 to have 5 g/dL deoxyhemoglobin running through the tongue and gums (lips OK when cold)
Cyanosis: Peripheral v. Central
• Peripheral– Response to cool
temperatures– part of normal transition– may last 72hr– May also represent poor
cardiac output• poor perfusion• anemia
• Central– Multiple causes
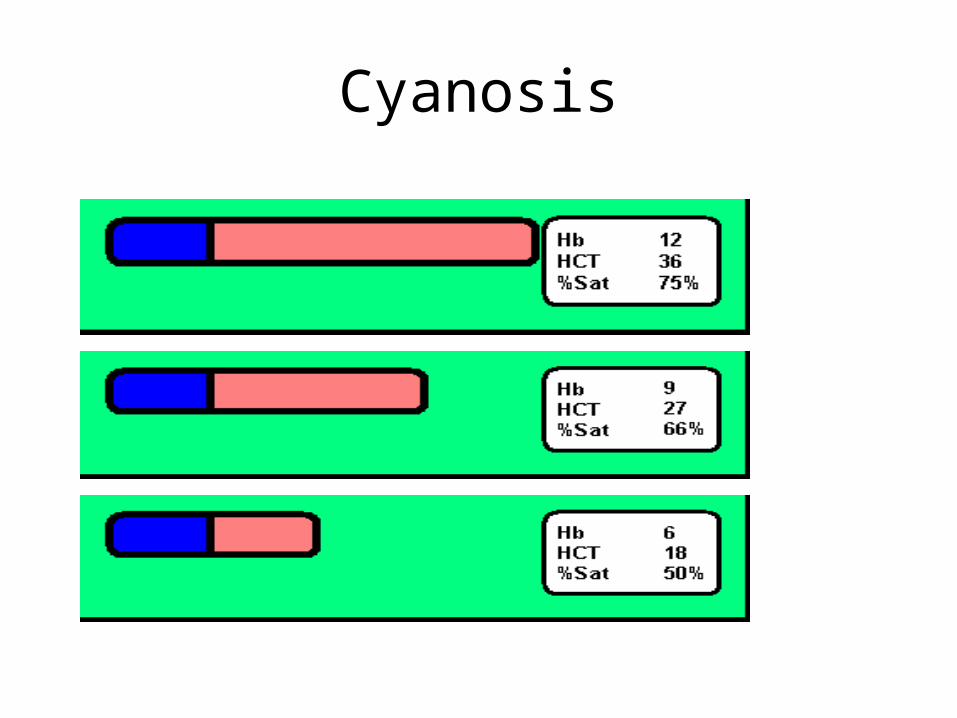
Cyanosis
Cyanosis
0
10
20
30
40
50
60
70
80
90
100
0 20 40 60 80
HCT
% S
atu
rati
on
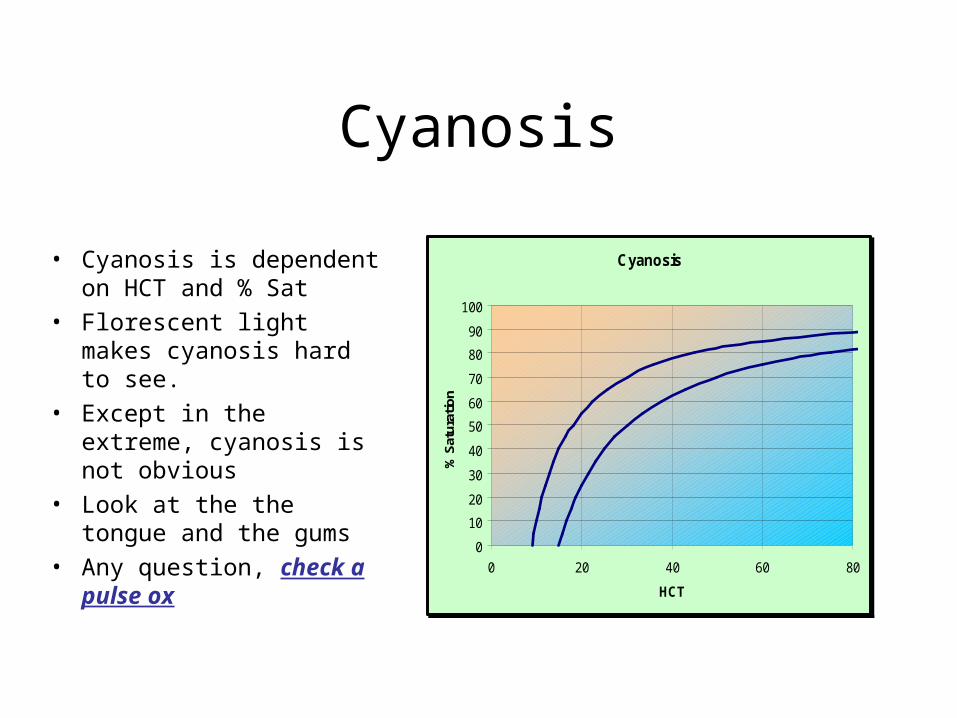
Cyanosis
• Cyanosis is dependent on HCT and % Sat
• Florescent light makes cyanosis hard to see.
• Except in the extreme, cyanosis is not obvious
• Look at the the tongue and the gums
• Any question, check a pulse ox
Terms• Oxygen tension (PO2)
– Partial pressure of oxygen in the blood (mm Hg)– Measured on an ABG machine– Oxygen dissolved in plasma
• 0.003 ml O2/mm Hg/dl plasma
• Oxygen saturation (SO2)– Amount of oxygen actually combined with hemoglobin as a percent of total
oxygen that could be bound to hemoglobin– Measured by saturation monitor (pulse-oximeter)– ~1.34ml O2/g Hb
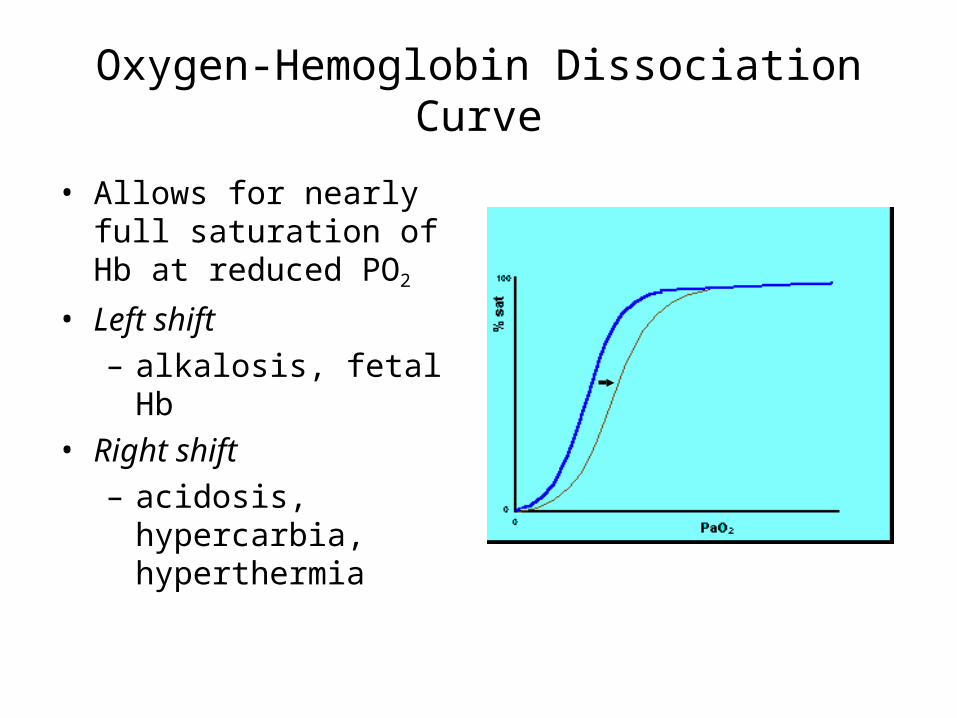
Oxygen-Hemoglobin Dissociation Curve
• Allows for nearly full saturation of Hb at reduced PO2
• Left shift– alkalosis, fetal Hb
• Right shift– acidosis, hypercarbia,
hyperthermia
Differential Diagnosis of cyanosis
1. Not enough oxygen in2. Oxygen “mal-absorption”3. Too much oxygen out
Not enough oxygen in
• Apnea– neurologic and drugs
• Diffusion barrier– RDS, aspiration, pneumonia
• Obstruction– pneumothorax, head position
Oxygen “mal-absorption”
• Shunting lesions– cardiac– non-cardiac (like PPHN)
• Hematologic– methemoglobinemia– carboxyhemoglobinemia
Too much oxygen out
• High oxygen consumption
– sepsis
– low flow, high extraction• acrocyanosis• hyperviscosity/polycythemia• extravasated (e.g. bruising)
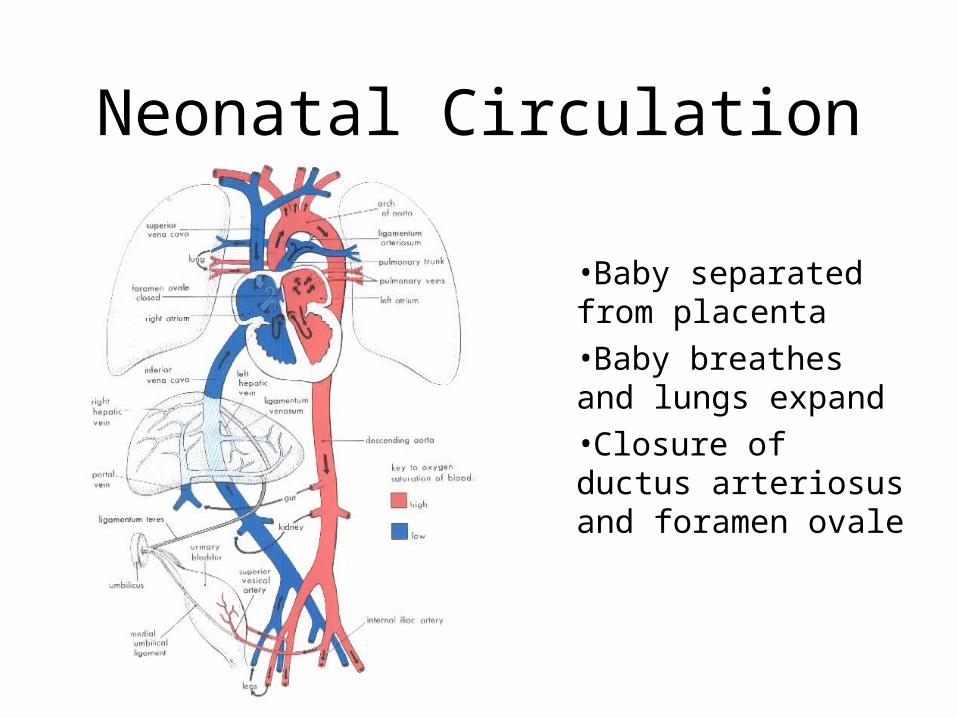
Neonatal Circulation
•Baby separated from placenta•Baby breathes and lungs expand•Closure of ductus arteriosus and foramen ovale
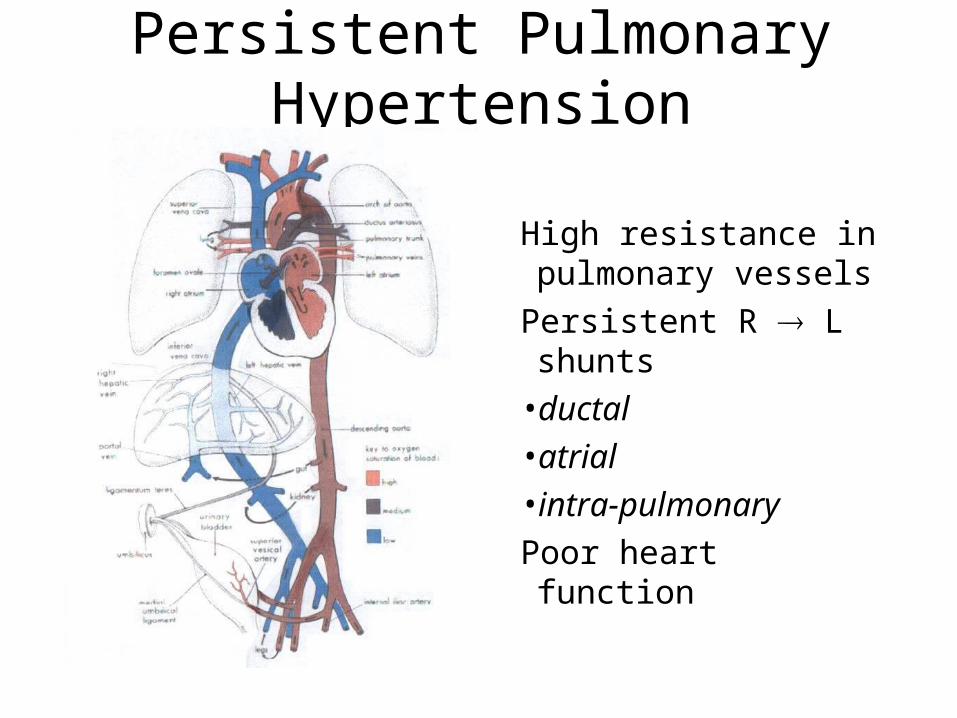
Persistent Pulmonary Hypertension
High resistance in pulmonary vessels
Persistent R L shunts
•ductal•atrial• intra-pulmonary
Poor heart function
The Five Ts of Cyanotic Congenital Heart Disease
• Transposition of the great arteries• Tetralogy of Fallot • Truncus arteriosus• Total Anomalous Pulmonary
Venous Return• Tricuspid Atresia
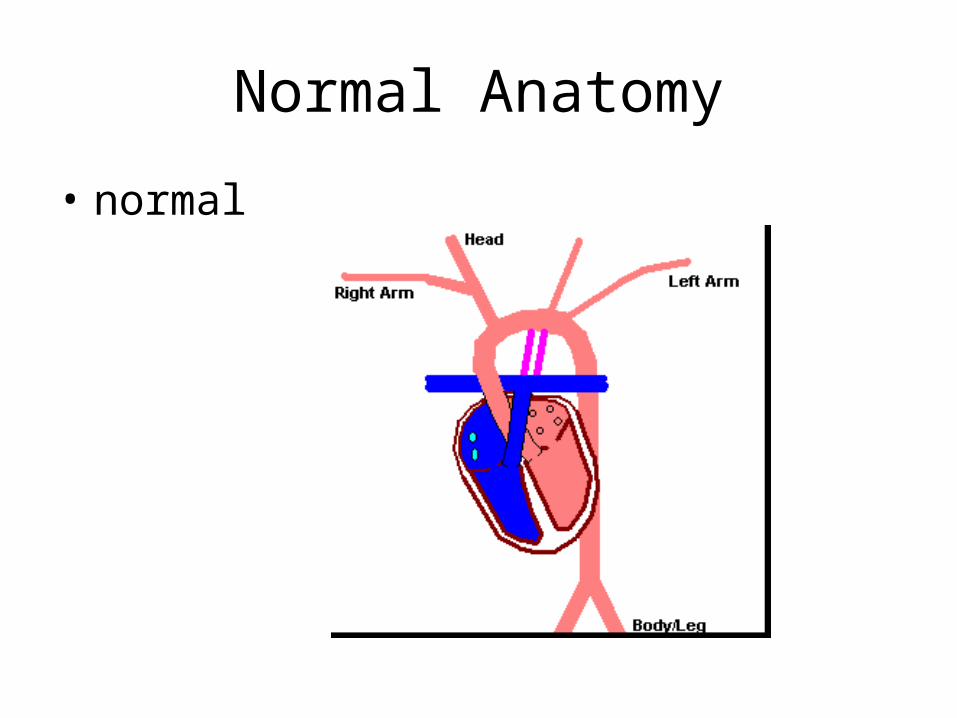
Normal Anatomy
• normal
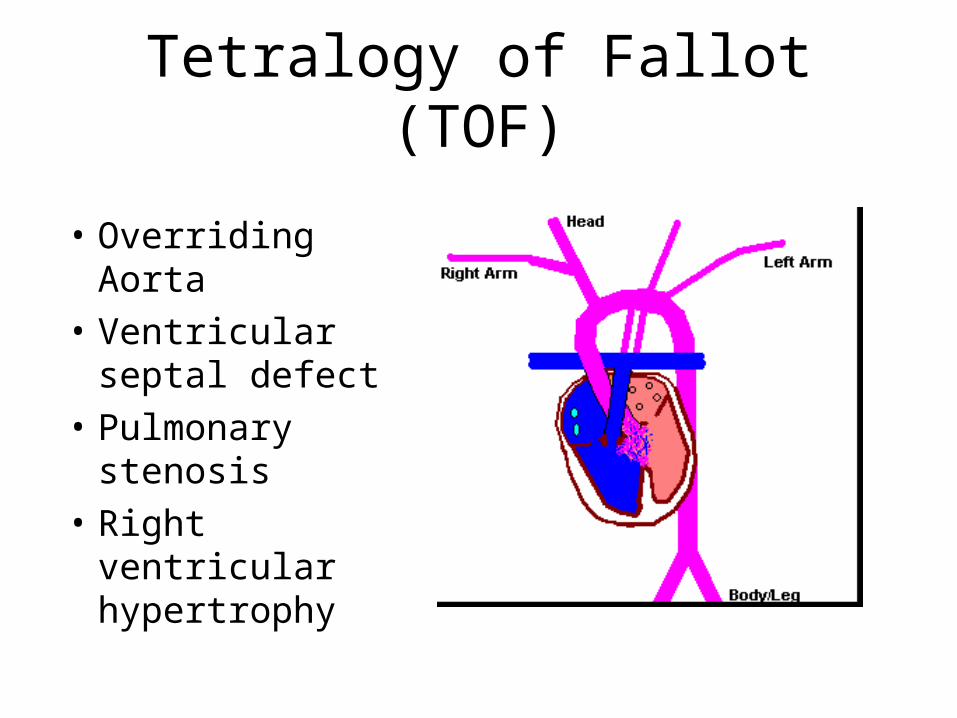
Tetralogy of Fallot (TOF)
• Overriding Aorta
• Ventricular septal defect
• Pulmonary stenosis
• Right ventricular hypertrophy
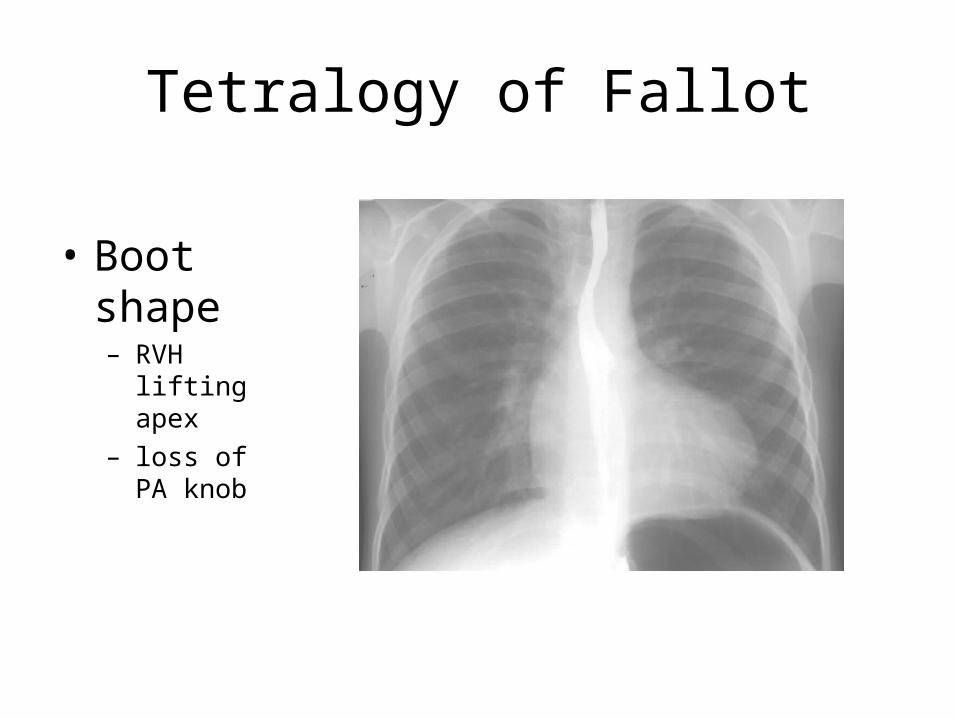
Tetralogy of Fallot
• Boot shape– RVH lifting
apex– loss of PA
knob
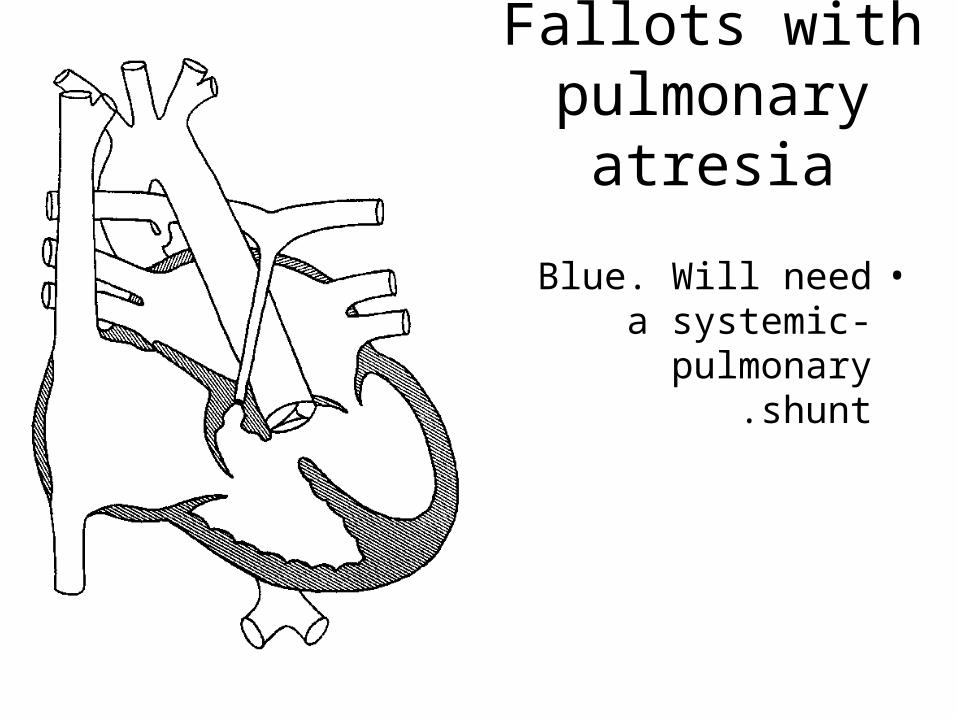
Fallots with pulmonary
atresia
•Blue. Will need a systemic- pulmonary
shunt.
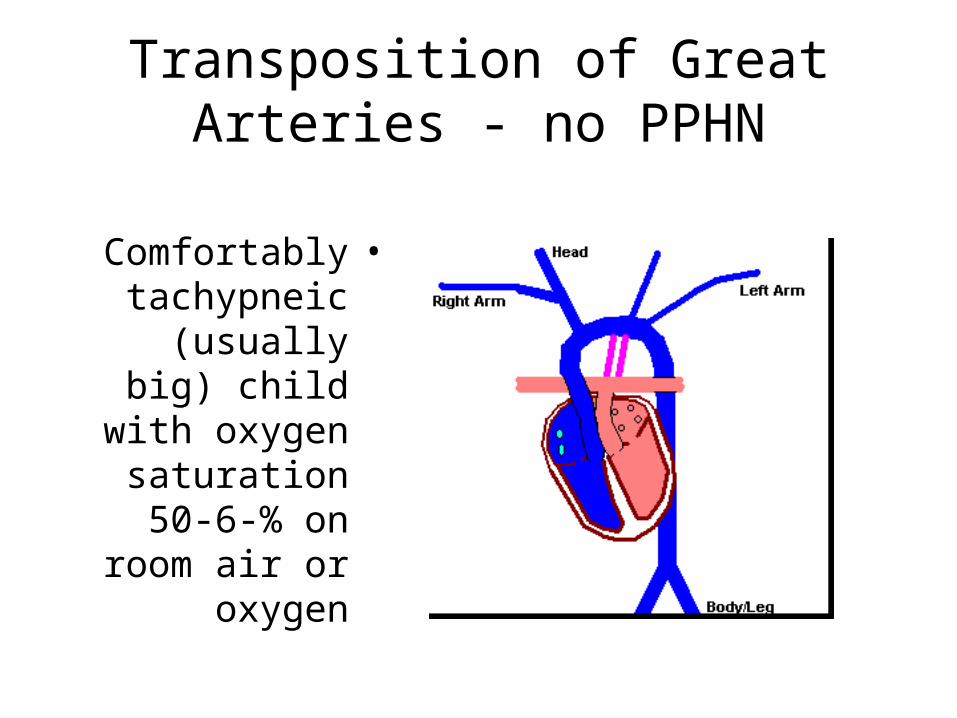
Transposition of Great Arteries - no PPHN
•Comfortably tachypneic
(usually big) child with
oxygen saturation 50-6-
% on room air or oxygen
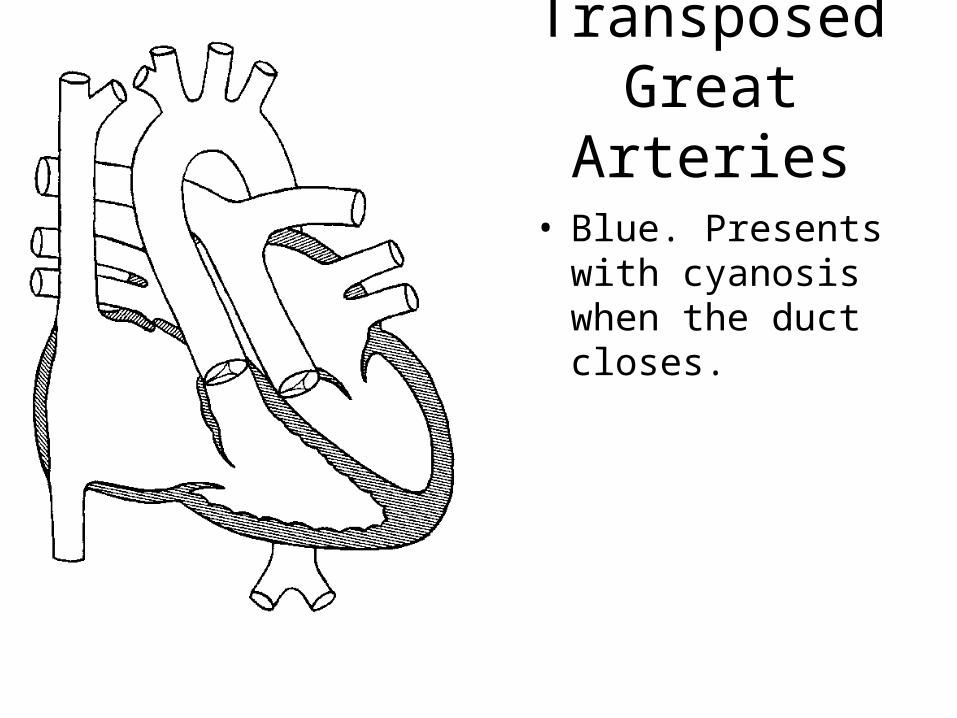
Transposed Great Arteries
• Blue. Presents with cyanosis when the duct closes.
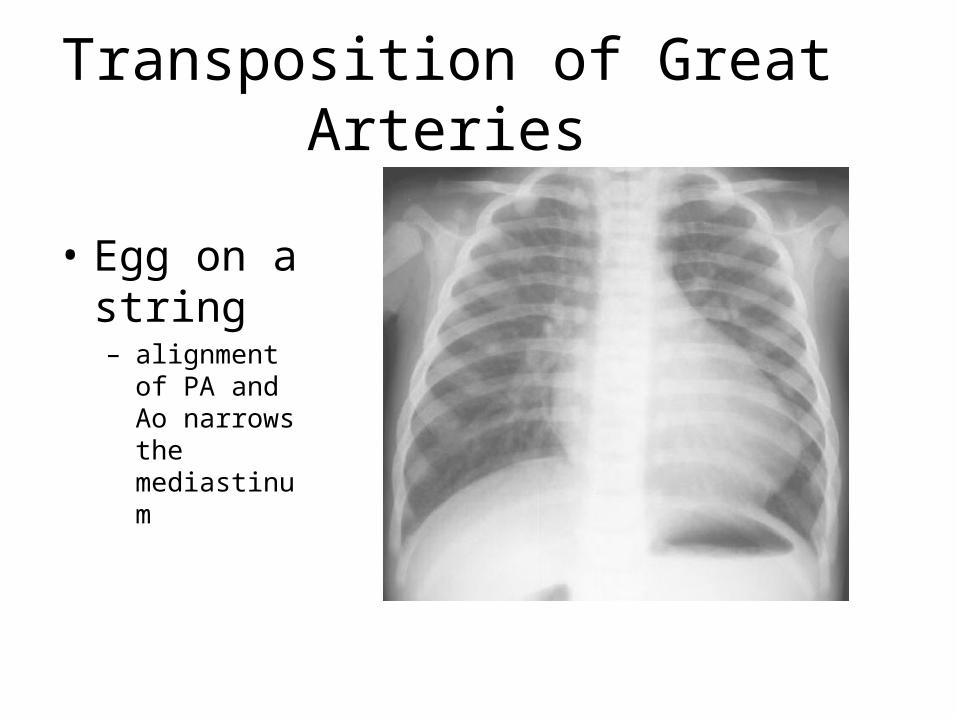
Transposition of Great Arteries
• Egg on a string– alignment of
PA and Ao narrows the mediastinum
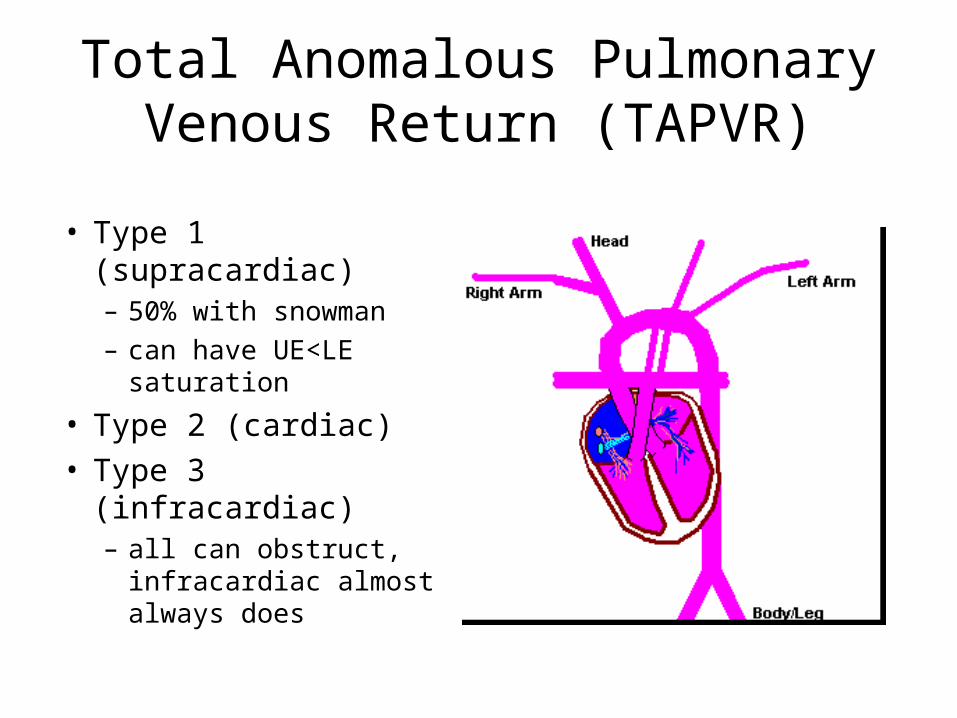
Total Anomalous Pulmonary Venous Return (TAPVR)
• Type 1 (supracardiac)– 50% with snowman– can have UE<LE
saturation
• Type 2 (cardiac)• Type 3 (infracardiac)
– all can obstruct, infracardiac almost always does
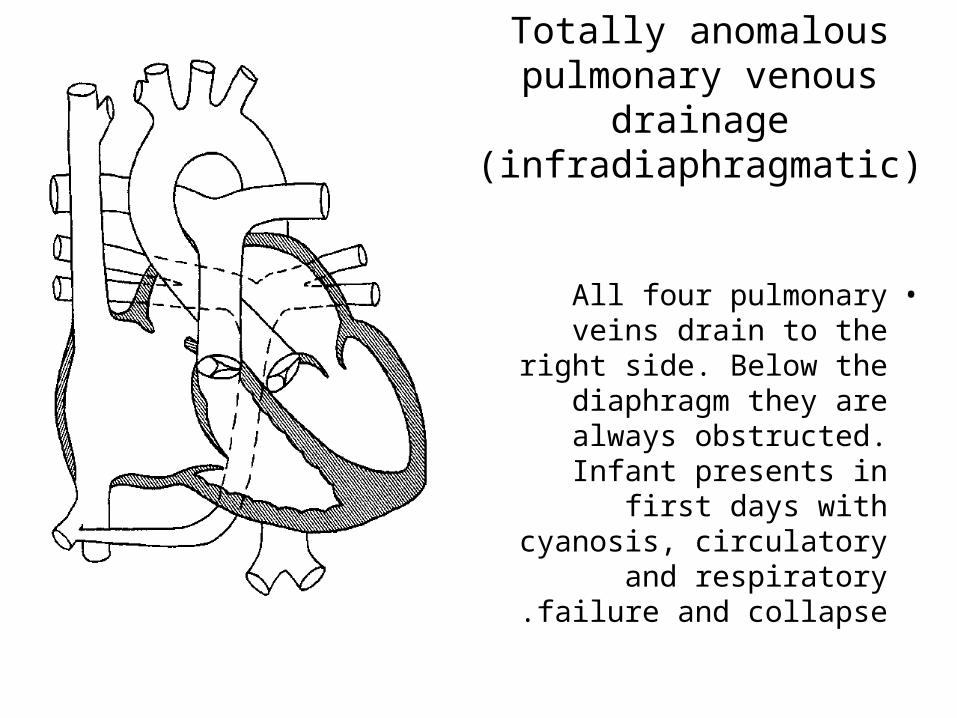
Totally anomalous pulmonary venous drainage
(infradiaphragmatic)
•All four pulmonary veins drain to the right side. Below the diaphragm
they are always obstructed. Infant
presents in first days with cyanosis, circulatory and
respiratory failure and collapse.
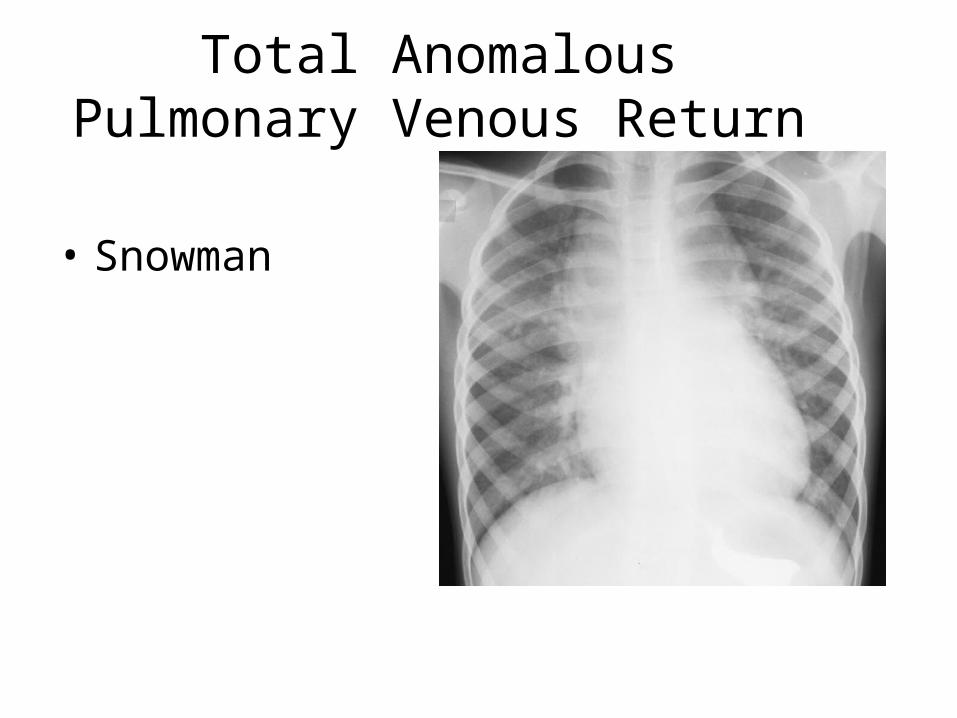
Total Anomalous Pulmonary Venous Return
• Snowman
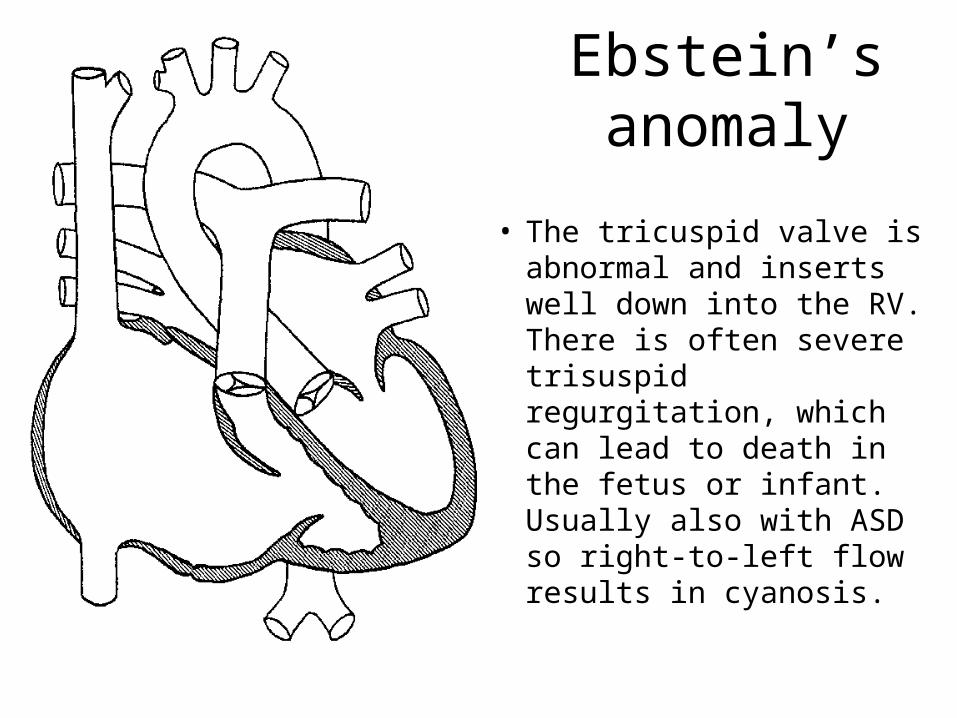
Ebstein’s anomaly
• The tricuspid valve is abnormal and inserts well down into the RV. There is often severe trisuspid regurgitation, which can lead to death in the fetus or infant. Usually also with ASD so right-to-left flow results in cyanosis.
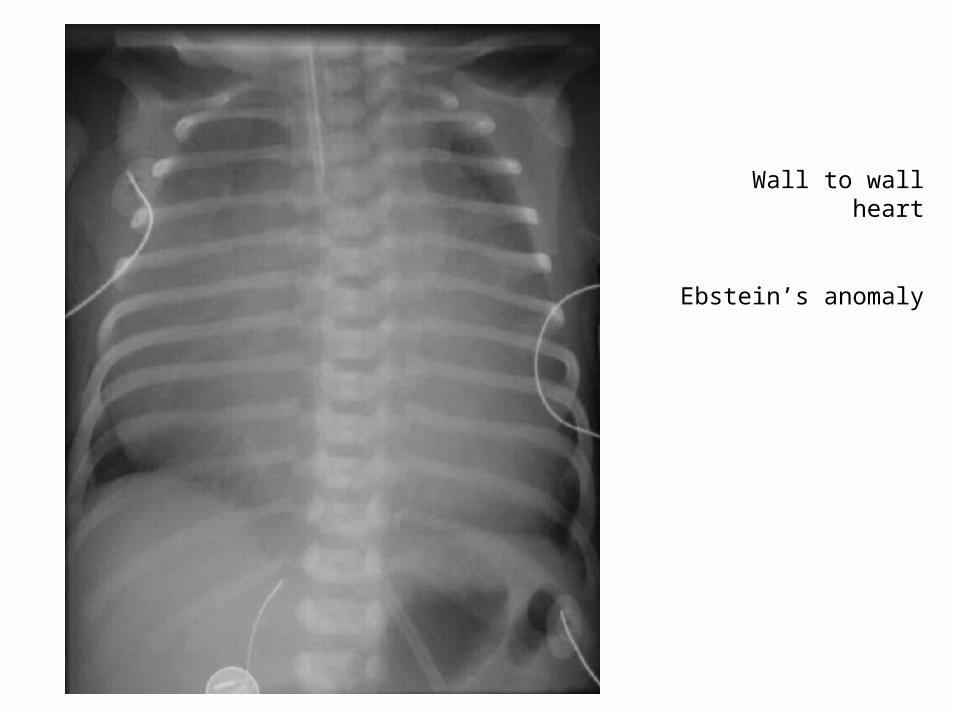
Wall to wall heart
Ebstein’s anomaly
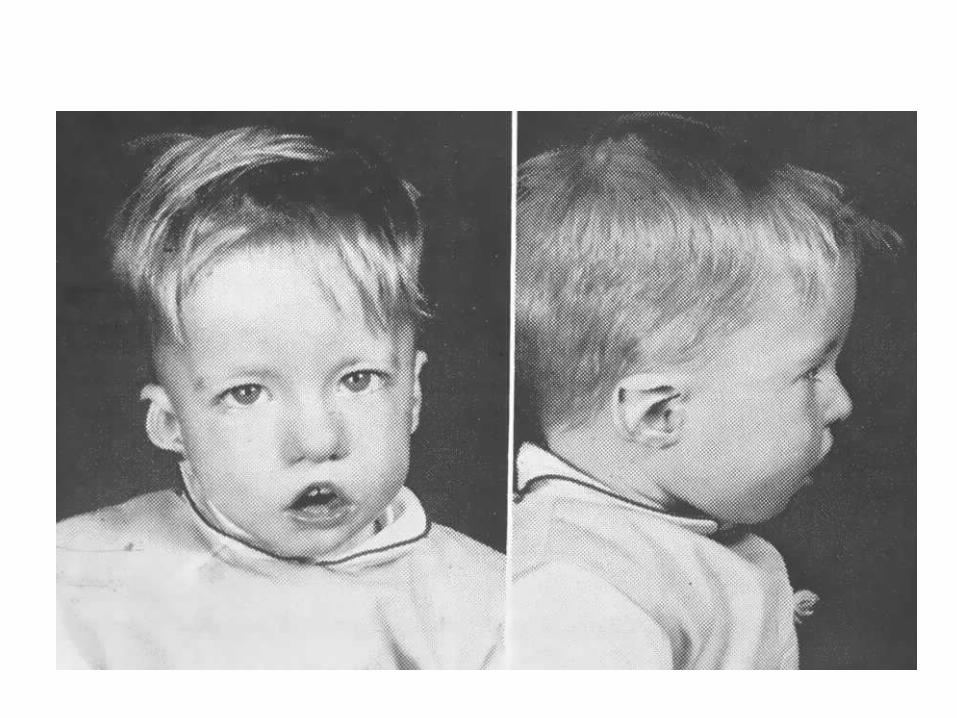
DiGeorge syndrome
• Thymic aplasia (T-cell, immune problems)• Hypocalcaemia (hypothyroid gland
aplasia, seizures)• Dysmorphism (unusual facial appearance)• Outflow tract abnormalities in the heart
Tricuspid Atresia
• DiGeorge syndrome with low calcium seen in 1/3 of the cases