Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry 1991;54:877-881
Cutaneous thermal thresholds in patients withpainful burning feet
Shelagh J M Smith, Z Ali, Clare J Fowler
AbstractSmall nerve fibre sensory function wasassessed by psychophysical estimates ofcutaneous thermal thresholds in 30patients who presented with the symp-toms of painful burning feet. Thresholdswere abnormal in 12 and normal in 18patients although symptoms in the twogroups were very similar. Varioushypotheses for the mechanism of pain insmall fibre neuropathy have beenproposed previously and these are dis-cussed, but the cause of symptoms inpatients with normal thresholds, is un-known. The possibility exists that thesepatients have a neuropathic disorderwhich affects only those unmyelinatedfibres involved with pain.
Data from human microneurographyexperiments have shown that the sensation ofcooling is conveyed in small myelinated fibres8and that of warming in unmyelinated fibres.39The conduction velocity of each of the ther-mal sensations generated when using theapparatus employed here was estimated inearlier reaction time experiments'0 as being0 5-0-2 m/s for warming and 2-1-0-8 m/s forcooling: velocities consistent with conductionin unmyelinated and small myelinated fibresrespectively.We have looked for evidence of small fibre
dysfunction using psychophysical estimationof cutaneous thermal thresholds in a group ofpatients presenting with pain and burning intheir feet.
Department ofClinicalNeurophysiology, TheNational Hospital forNervous Diseases,London, UKS J M SmithZ AliC J FowlerCorrespondence to:Dr Fowler, Department ofClinical Neurophysiology,Middlesex Hospital, LondonWIN 8AA, UK.Received 12 September 1990and in final revised form15 March 1991.Accepted 26 March 1991
The symptoms and signs of a peripheralneuropathy depend on whether theneuropathic process produces "positive" or"negative" features.' Negative manifestationsresult in loss of light touch, vibration and jointposition sense if predominantly large fibres areaffected. If small fibre loss predominates, painand temperature sensation are defective, andthe patient may present with painless plantarulceration. Neuropathic damage which causessmall myelinated and unmyelinated fibres(those fibres which convey nociception andthermal sensations) to become generators ofpositive phenomena, may present with pain ina glove and stocking distribution or just painand burning in the feet.
In patients complaining of painful feet, adiagnosis of small fibre neuropathy should beconsidered. Appropriate investigation of thisdisorder has presented a considerable problemin the past. Nerve conduction studies withsurface electrodes measure conduction in thefastest conducting, large diameter myelinatedfibres and are therefore of little value in detect-ing small fibre neuropathy. Near nerve needleelectrode recordings of compound nerveaction potentials, with averaging over a 1000times, yields waveforms in which late, slowlyconducted potentials can be resolved,2 but donot show activity of unmyelinated fibres. Ofthe few methods available which can assessunmyelinated fibre function, microneurogra-phy3 and morphometry4 are well established,but both are invasive and unsuitable to applyroutinely. However, psychophysical estimatesof cutaneous thermal thresholds are simple,non-invasive tests, acknowledged to be ofvalue in the assessment of small fibre sensoryfunction."
Patients and methodsPatientsThirty patients (six male, 24 female, age range21-81 years) with painful, burning feet astheir predominant symptom, were investi-gated. They had all been referred byneurologists from the National Hospital forNeurology and Neurosurgery, suspected onclinical grounds of suffering from small fibreneuropathy, other possible causes such asorthopaedic disorders and inflammatory fasci-itis having been excluded as far as possible onclinical grounds. A clinical history wasobtained by one of the investigators (SJMS orCJF), corroborated when necessary from thecase notes made by the referring clinician.Group differences in symptoms and signs
were compared using the chi-squared test.
Nerve conduction studiesAll patients underwent standard nerve con-duction studies using surface recording andstimulating electrodes." 12 Sensory actionpotentials of the median, ulnar, and suralnerves were measured and motor conductionvelocity in the ulnar and lateral popliteal orposterior tibial nerves. Measurements weremade at room temperature without heatingthe limb.
Psychophysical estimation of thermal thresholdsCutaneous thermal thresholds were estimatedusing a computer controlled warm and coldstimulus generator."' Stimuli were deliveredfrom a thermode made of a Peltier junctionmodule, sandwiched between a thin copperplate and air-cooling fins, with a thermo-cou-ple embedded in the copper plate to monitorthe temperature at the skin-thermode junc-
877
on Novem
ber 30, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.10.877 on 1 October 1991. D
ownloaded from

Smith, Ali, Fowler
tion. The test consisted of a warning tonefollowed by a dynamic thermal ramp stimulusof predetermined intensity and the subjectasked to respond "yes" or "no" as to whetherthe stimulus was felt. Stimuli were of progres-sively diminishing amplitude and randomlyinterspersed among real stimuli were "catch"trials, when no temperature change followedthe warning tone; these allow the reliability ofthe subject to be assessed. Threshold wascalculated by the microcomputer using analgorithm similar to that devised by Dyck'4 inwhich the mean was taken of all values bet-ween the last three turns, or in this instance"no s". On average eight test levels areneeded to define threshold using this method.
Threshold for cooling was tested first as allsubjects found the cooling stimulus less subtlethan the warming one. The test protocol forwarming was identical except that the polarityof the current through the thermode wasreversed.The thermode was attached to the non-
keratinised skin on the instep of the foot. Bothsensory modalities were tested on one foot andif those results were abnormal the other foot
was also tested to confirm the deficit was gen-uine. As with all psychophysical tasks thesubject's full cooperation was critical andefforts were made to ensure an abnormal resultwas due to impaired sensation rather than aninability to perform the test adequately.
Control data were collected earlier from 1 16subjects, 60 men and 56 women, age range 18-73. These were mainly healthy volunteersrecruited from hospital personnel, althoughhealthy subjects over 65 years old were soughtoutside the hospital. The effect of age onthresholds was examined using least squaresregression methods and examination of theresiduals showed that the simple linear regres-sion formula provided the best fit to the data.'3Ninety five per cent confidence limits based ontwo standard deviations were calculated foreach thermal modality, and in men andwomen separately. Results from the patientswere superimposed on graphs of the controldata.
Nerve biopsyFour patients had sural nervelocal anaesthetic.
biopsy under
Male61 Threshold for warming (foot)
:1___
0
0
Female1 hreshold for warming (foot)
Threhold1- _I.___ _
3-0 0
0 0
0 002 0~~B0 00
00
1 0 0:0000 0 c .0
0~~ ~ ~ ~ ~~~
oo 0 x0 % c 0"0%__ __E_I.I- - - - -
Threshold for cooling (foot) Threshold for cooling (foot)
0~~~~~
11-0~~~~~~~~~~~~
EHJR
0§ __ _ __ _
o. i o~~ ciod' ~ n 0 _ _EP_ _-19-3---20 40 60 80
Age (years)
60
Age (years)
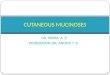
Figure Thresholds for warming (a) and cooling (c) in males and warming (b) and cooling (d) infemales, measured on the sole of the foot. Thegraphs show thresholds for control subjects (open symbols) andpatients (solid circles) . The line indicates upper limit of normal thresholdfor age(mean +2SD)."
*00
0
'n
0
a'0m
tA:)
80
878
20 40
on Novem
ber 30, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.10.877 on 1 October 1991. D
ownloaded from

Cutaneous thermal thresholds in patients with painful burningfeet
Table 1 Clinical findings
Normal TT Abnormal TTn= 18 n= 12
M:F 2:16 4:8Mean age (range) 54 4 (21-72) 55-6 (28-81) NS*
SymptomsPain alone 6 (33%) 3 (25%) NSBurning alone 8 (44%) 3 (25%) NSPain and burning 3(22%) 7 (58%) p < 0-02Reliefby cooling 2 (11%) 3 (25%) NSRelief by movement 8 (44%) 3 (25%) NSMean duration (range) 5-7 (9m-20y) 3 7 (2w-20y) NS*
SignsReduced pinprick 2 (11%) 7 (58%) p < 0 01
TT-Thermal Threshold.*-Mann Whitney U test other chi-squared test.
ResultsWarming and cooling thresholds were withinthe normal range in 18 patients, age range 21-72 years, mean age 54 1. One or both thresholdswere abnormal in 12 patients, age range 28-81years, mean age 55-6. Six of the 12 patients hadabnormal thresholds for both warming andcooling; four had only abnormal warmingthresholds and two, only an abnormal coolingthreshold (figure).The mean duration of symptoms in patients
with abnormal thresholds (mean 3-7 years,range 2 weeks-20 years, SD 5 3) was less thanthat in patients with normal thresholds (mean5 6 years, range 9 months-20 years, SD 5 6)although this difference was not statisticallysignificant.
Six patients with normal thresholds andthree patients with abnormal thresholds com-plained of painful feet as their only symptom(table 1). The nature of the pain varied; somepatients described a sharp shooting pain,whereas others complained of a dull continuousache or throbbing pressure felt in the feet andlower part of the legs. In some cases, the painhad an unpleasant dysaesthetic quality, andwas likened to a sensation of insects crawlingbeneath the skin of the feet or pins being stuckinto the legs. Most patients found that the painwas worse at night. Two patients with normalthresholds and three patients with abnormalthresholds could obtain some relief from theirpain either by hanging their legs out of bed,walking around, or applying pressure to thesoles of their feet.There was no obvious difference between the
two groups for quality or severity of pain.Eight patients with normal thresholds and
three with abnormal thresholds described a
Table 2 Nerve conduction studies
Group Mean (range) SD p
Sural Normal TT 18 9 (6-60) 14 3SAP p < 0 01amplitude (uV) Abnormal TT 9 6 (0-20) 5-9
Median Normal TT 20-2 (10-34) 8-03SAP NSamplitude (uV) Abnormal TT 15-0 (5-21) 5 9
Upper Normal TT 60 (49-71) 7 34limb MCV NS(m/s) Abnormal TT 61 (50-73) 7-72
Lower Normal TT 48 (40-64) 5-74limb MCV NS(m/s) Abnormal TT 50(40-65) 9-88
burning sensation in their feet as their onlysymptom. Five patients (three with abnormaland two with normal thresholds) found relieffrom the burning feeling by cooling their feet orlegs in a bucket ofcold water. One patient (withnormal thresholds) found the burning sensa-tions to be worse in cold weather.There was a significant difference (p < 0-02,
chi-squared test) in the number of patientsfrom each group who complained of bothburning and pain in their feet; seven patientswith abnormal thresholds, but only threepatients with normal thresholds described bothsymptoms. Patients with abnormal thresholdswere also more likely to have abnormalities onclinical examination with a reduction in pin-prick sensation in the lower limbs in sevencompared with only two of patients with nor-mal thresholds. This difference was significant(p < 0-01, chi-squared test).Nerve conduction tests were abnormal in
only one case; this patient also had abnormalthresholds for warming and cooling. Sensoryaction potentials (sural 4 uv, median 5 uv) andthe compound muscle action potential from theextensor digitorum brevis (2 8 mV) were oflowamplitude; motor conduction velocity in theulnar and lateral popliteal nerves was normal.None of the remaining patients had abnor-
mal sensory action potentials or motor conduc-tion velocities, although the mean amplitude ofthe sural sensory action potential was smaller(see table 2) in the group with abnormalthresholds (p < 0-01, Mann-Whitney U test).Four patients in the group with abnormal
thresholds had sural nerve biopsies with mor-phometry, confirming a predominantly smallfibre neuropathy.A possible aetiological factor was identified in
eight of the 12 patients with abnormal thermalthresholds (table 3). Two gave a history ofalcohol abuse; three patients were known orfound to be diabetic (one insulin dependent andtwo maturity onset). In one case, the suralnerve biopsy showed evidence of vasculitis(case 7); this patient's symptoms appeared afew days after he had been given Cotrimoxazolefor sinusitis. He complained ofvery severe painand burning and had abnormal nerve conduc-tion studies in addition to abnormal thresholds.In one further patient, (case 10) polycythaemiawas thought to be responsible for theneuropathy and in the remaining case, thediagnosis was a drug related (perhexilene)neuropathy (case 1 1).Of the 18 patients with normal thresholds,
none was found to be diabetic or to have anyother history relevant for a small fibreneuropathy. Three patients had long standingintermittent low back pain, two had a history ofischaemic heart disease, one was found to havean iron deficiency anaemia and one was achronic epileptic on long term anticonvulsantmedication (phenytoin).
DiscussionPsychophysical estimates ofthermal thresholdsin this group of 30 patients with painful,burning sensations in their feet demonstratedabnormalities compatible with a small fibreneuropathy in only 40%.
879
on Novem
ber 30, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.10.877 on 1 October 1991. D
ownloaded from

Smith, Ali, Fowler
Table 3 Details ofpatients with abnormal thresholds
Patient Age Symptoms Duration Relevant history Biopsy NCS
1 28 Burning 6 mths Diabetes - Normal2 78 Burning 2 yrs - - Normal3 46 Pain 5-6 yrs Diabetes - Normal4 55 Pain 3-4 yrs Alcohol abuse + + - Normal5 59 Pain 20 yrs Alcohol abuse + + - Normal6 36 Pain + burning 4 yrs - - Normal7 39 Pain + burning 2 wks Vasculitis SFN Abnormal8 45 Pain + burning 2 yrs - - Normal9 63 Pain + burning 2 yrs Diabetes SFN Normal10 66 Pain + burning 2 yrs Polycythemia SFN Normal11 73 Pain + burning 1 yr Drug related SFN Normal12 81 Pain + burning 18 mths - - Normal
NCS-nerve conduction studies.SFN-small fibre neuropathy.
Of the 12 patients with abnormal thermalthresholds, four had nerve biopsy which confir-med damage to a significant proportion of smallfibres; in all four patients a possible aetiologicalfactor was present, that is, diabetes, vasculitis,neuropathy related to polycythaemia and drugrelated neuropathy. Of the eight patients withabnormal thresholds who did not have abiopsy, a possible relevant history was found infour (diabetes or alcohol excess) and a combin-ation of this and the abnormal thresholds wasconsidered sufficient by the referring clinicianto make a diagnosis of small fibre neuropathy.In the four remaining patients, no definitediagnosis was reached. None of the patientswith normal thresholds had medical historiessuggesting a cause ofsmall fibre neuropathy andnone had sural nerve biopsies.The mean amplitude of the sural sensory
action potential was smaller in the 12 patientswith abnormal thermal thresholds, although inonly one patient was the amplitude below thelower limit of normal for our laboratory. Thissuggests additional large fibre involvement insome patients.Although there was no clear difference in the
nature of the symptoms between the twogroups, patients with both pain and burning intheir feet or those who had reduced sensation ofpinprick on the feet, were more likely to haveabnormal thermal thresholds.
It is unlikely that the thermal thresholdtesting system employed in this study wasinsufficiently sensitive to detect abnormalitiesof sensation. The control ranges for thresholdson the soles ofthe feet using this device showeda positive correlation with age,"3 which is apowerful indicator of biological sensitivity.Also in another study 11 patients who had haddiabetes for more than 20 years but werewithout symptoms ofneuropathy, were subjec-ted to a battery of sensory tests and nerveconduction studies, and an impairment of per-ception of warming using the techniqueemployed here, was the commonest abnor-mality. 5 Perception ofwarming requires a highdegree of spatial summation 6 and since theproportion of unmyelinated fibres which con-vey this modality is low, any peripheral nervepathology which damages the population ofunmyelinated afferents will be manifest bycausing an abnormally high threshold for war-ming. Thus in 60% of this group of patientswith symptoms of pain and burning in the feet,a test which is sensitive and appropriate forunmyelinated afferent dysfunction, wasnormal.It can, however, be argued that an abnormality
might have been demonstrated had estimates ofthermal pain been made (although not tech-nically feasible using the apparatus employedhere) since it is now recognised that painfulsyndromes exist in which heat and coldhyperalgesia can be demonstrated in theabsence of warm or cold sensory deficits. 17
In a review of aspects of pain in peripheralneuropathy, Thomas made the point that spon-taneous pain is not a feature of neuropathieswhich cause a selective loss of large myelinatedfibres but is a prominent symptom ofneuropathies that have been shown to result inrelatively selective small fibre loss.' Themechanism for pain in the presence of smallfibre neuropathy has been considered in severalreviews"'2' and the hypothesis that pain is apositive manifestation of nerve fibre diseaseaffecting the nociceptive afferents seems emi-nently plausible. The precise patho-physiological basis of symptoms, however, isfar from being understood.
In a study which examined nerve fibre path-ology in teased sural nerve biopsy specimensfrom a group of patients with peripheralneuropathy, some of whom had moderate tosevere neuropathic pain, an association bet-ween painfulness and the occurrence of acutebreakdown of myelinated fibres was shown.The authors explain that since it was notpossible to distinguish between myelin rem-nants from large and small myelinated fibresthey were not able to provide direct evidencethat painfulness was correlated with degenera-tion of a particular nerve fibre group.22 Othershave argued that there is evidence from mor-phological studies that the presence of dysesth-etic pain correlates with sprouting of-unmyelinated fibres.20 It has been suggestedthat in a distal axonopathy, axonal sprouts maybecome generators of spontaneous activitybehaving in the same way as proximal fibrestumps in neuromas.2" Alternatively, paincould be arising from ephaptic transmission ofeither ascending or descending impulses cross-ing into pain fibres.'9Evidence is accumulating from micro-
neurography studies that in some instances,positive neurogenic symptoms may be due toabnormal afferent fibre activity.'2'24 As yet,however, no microneurography recordingshave been made showing spontaneous activityin C-fibres in patients with painful neuropathy.Tenable hypotheses exist as to the cause of
painful burning feet in patients with peripheralneuropathy. The almost indistinguishablesymptoms in the group of patients with normal
880
on Novem
ber 30, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.10.877 on 1 October 1991. D
ownloaded from

Cutaneous thermal thresholds in patients with painful burningfeet
thermal thresholds are more difficult to explain.It seems probable that alterations in the centralnervous system could produce peripheral sen-sations of pain and this may be the mechanismunderlying the syndrome of "painful legs andmoving toes" described by Spillane et al5Schott reported five such cases who developedpainful legs and moving toes following traumato the feet and proposed that the trauma mayhave set up a spreading irritative central disor-der possibly in the lower spinal cord.26 Ekbom'ssyndrome is another disorder in which there isa combination of pain in the legs relieved bymovement.27 Although some cases areassociated with a neuropathy,2" this is not aprerequisite and two cases of restless legs havebeen described in association with arborisingtelangectasia.29A yet further possibility exists which is that
pain is arising from the nerve endings in nervetrunks-the nervi nervorum. Such a mechan-ism would be consistent with normal peri-pheral nerve function and therefore the findingsof normal thermal thresholds. Other expectedclinical features of such a disorder were notseen; there was no noticeable tenderness of thenerve bundles and symptoms were not exacer-bated by movement or any other procedure thatmight have stretched the nerves.Ochoa recently described a new syndrome,
the "Painful ABC syndrome" (Angry Backfir-ing C nociceptor syndrome).0 This has beenproposed as a specific disorder of the conduc-tance channels of the receptor membrane of Cnociceptors. These receptors, usually respon-sive to both heat and painful mechanicalstimuli, become disordered in such a way thatthey operate in a state near to threshold due to"up-regulated thermal activation" and anyincremental change resulting from mechanicalstimulation is sufficientto bringfiring frequencyto a level for conscious sensation. This has beencalled "cross modality threshold modulation"and the phenomenon of pain, induced either byincreasing temperature or light mechanicalstimulation, has been referred to as "polymodalhyperalgesia". The patients described as hav-ing this new syndrome presented with localisedburning pain, hyperalgesia on thermal ormechanical stimuli, and gave histories illustrat-ing the phenomena of cross modality thresholdmodulation. A notable finding was relief ofsymptoms by cooling the affected part.Although five patients in our series gave ahistory of relief from pain by placing their feetin cold water, only one had erythema and skinwarming accompanying the pain. This excep-tion (case 7) was shown on biopsy to have avasculitic, small fibre neuropathy and in retro-spect, probably had the "Painful ABC syn-drome". We were unaware ofthe significance ofthe observation of the effect of cooling onsymptoms at the time of the study, but thesepatients were all so troubled by their symptomsand eager to report any further self-observationthat might have provided a clue as to the causeof their affliction, that it is unlikely we missedother cases of this syndrome. While carryingout the temperature threshold testing, a strik-ing observation was the normal appearance ofthe patients' painful feet.There remains the real possibility that the
patients with pain and normal thermal thre-
sholds have a neuropathic disorder whichaffects only those unmyelinated fibres involvedwith pain.'7 In summary, the essential findingfrom this study is that a high proportion ofpatients with painful burning feet have normalthermal thresholds and possible patho-physiological mechanisms for their symptomsremain obscure.
The nerve biopsy were carried out by Dr Jean Jacobs. We wishto thank Dr R G Willison and Dr Jose Ochoa for helpfuldiscussion and invaluable advice. We also thank the physiciansat The National Hospital, Queen Square for permission to studytheir patients. ZA was supported by a grant given by InperialChemical Industries.
1 Ochoa J. Mechanisms of symptoms in neuropathy. In:Ellingson RJ, Murray NMF, Halliday AM, eds. TheLondon Symposium. EEG 1987;39:121-7.
2 Buchthal F, Rosenfalck A, Behse F. Sensory potentials innormal and diseased nerves. In: Dyck PJ, Thomas PK,Lambert EH, Bunge R, eds. Peripheral neuropathy.Philadelphia: Saunders, 1984:981-1015.
3 Hallin RG, Torebjork HE, Wiesenfeld Z. Nociceptors andwarm receptors innervated by C fibres in human skin.J Neurol Neurosurg Psychiatry 1982;45:313-19.
4 Ochoa J. Recognition of unmyelinated fiber disease: mor-phologic criteria. Muscle Nerve 1978;1:375-87.
5 Heimans JJ, Bertelsmann FW, Van Rooy JCGM. Large andsmall nerve fibre function in painful diabetic neuropathy.JNeurol Sci 1986;74:1-9.
6 Jamal GA, Hansen S, Weir AI, Ballantyne JP. The neuro-physiological investigation of small fiber neuropathies.Muscle Nerve 1987;10:537-45.
7 Report and Recommendations of the San Antonio Con-ference on Diabetic Neuropathy. Diabetes Care 1988;11:592-7.
8 Jarvilehto T, Hamalaien H. Touch and thermal sensations:Psychophysical observations and unit activity in humanskin nerves. In: Kenshalo DR, ed. Sensoryfuhctions of theskin ofhumans. New York: Plenum Press, 1980:279-95.
9 Konietzny F, Hensel H. The dynamic response of warmunits in human skin nerves. Pflugers Arch 1977;370:111-4.
10 Fowler CJ, Sitzoglou K, Ali Z, Halonen P. The conductionvelocitiesofperipheral nerve fibres conveying sensations ofwarming and cooling. J Neurol Neurosurg Psychiatry1988;51:1 164-70.
11 Gilliatt RW, Sears TA. Sensory nerve action potentials inpatients with peripheral nerve lesions. J Neurol NeurosurgPsychiatry 1958;21:109-18.
12 Kimura J. In: Kimura J, ed. Electrodiagnosis in diseases ofnerve and muscle. Philadelphia: Davis, 1983.
13 Fowler CJ, Carroll MB, Burns D, Howe N, Robinson K. Aportable system for measuring cutaneous thresholds forwarming and cooling. J Neurol Neurosurg Psychiatry1987;50:121 1-15.
14 Dyck PJ, Zimmerman IR, O'Brien PD, Ness A, Caskey PE,Karnes J, Bushek W. Introduction of automated systemsto evaluate touch-pressure, vibration, and thermal cutan-eous sensation in man. Ann Neurol 1978;4:502-10.
15 Le Quesne PM, Fowler CJ, Parkhouse N. Peripheralneuropathy profile in various groups ofdiabetics. JNeurolNeurosurg Psychiatry 1990;53, 7:558-63.
16 Kenshalo DR, Decker T, Hamilton A. Spatial summation onthe forehead, forearm, and back produced by radiant andconducted heat. J Comp Physiol Psychol 1967;3:510-15.
17 Cline MA, Ochoa J, Torebjork HE. Chronic hyperalgesiaand skin warming caused by sensitized C nociceptors.Brain 1989;112:621-47.
18 Thomas PK. The anatomical substratum of pain. Can JNeurol Sci 1974;1:92-7.
19 Thomas PK. Pain in peripheral neuropathy: clinical andmorphological aspects. In: Culp WJ, Ochoa J, eds.Abnormal nerves and muscles as impulse generators. NewYork: Oxford University Press, 1982:553-67.
20 Asbury AK, Fields HL. Pain due to peripheral nervedamage: an hypothesis. Neurology 1984;34:1587-90.
21 Ochoa J. Pain in local nerve lesions. In: Culp WJ, Ochoa J,eds. Abnormal nerves and muscles as impulse generators.New York: Oxford University Press, 1982:568-87.
22 Dyck PJ, Lambert EH, O'Brien PC. Pain in peripheralneuropathy related to rate and kind of fiber degeneration.Neurology 1976;26:466-71.
23 Wall PD, Gutnick M. Properties of afferent nerve impulsesoriginating from a neuroma. Nature 1974;248:740-3.
24 Nordin M, Nystrom B, Wallin U, Hagbarth KE. Ectopicsensory discharges and paraesthesiae in patients withdisorders of peripheral nerves, dorsal roots and dorsalcolumnns. Pain 1984;20:231-45.
25 Spillane JD, Nathan PW, Kelly RE, Marsden CD. Painfullegs and moving toes. Brain 1971;94:541-56.
26 Schott GD. "Painful legs and moving toes": the role oftrauma. J Neurol Neurosurg Psychiatry 1981;44:344-6.
27 Ekbom KA. Restless legs syndrome. Neurology 1960;10:868-73.
28 Read DJ, Feest TG, Nassim MA. Clonazepam: effectivetreatment for restless legs syndrome in uraemia. BMJ1981;283:885-6.
29 Metcalfe RA, Macdermott N, Chalmers RJG. Restless redlegs: an association of the restless legs syndrome witharborising telangiectasia of the lower limbs. J NeurolNeurosurg Psychiatry 1986;49:820-23.
30 Ochoa J. The newly recognized painful ABC syndrome:Thermographic aspects. Thermology 1986;2:65-107.
881
on Novem
ber 30, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.10.877 on 1 October 1991. D
ownloaded from