Embed Size (px)
Citation preview

CASE & REVIEWS
Cutaneous collagenous vasculopathy with generalizedtelangiectasia in two female patients
Alfonso Perez, Mary E. Wain, MD, MRCP, Alistair Robson, MRCPath, Dip RCPath, Richard W. Groves, FRCP,and Catherine M. Stefanato, MD, FRCPath
London, United Kingdom
From
Fund
Conf
Prese
Repr
of
E-
Publ
0190
ª 20
doi:1
882
Cutaneous collagenous vasculopathy is characterized by generalized cutaneous telangiectasia and uniquemicroscopic and ultrastructural vascular changes, consisting of marked collagen deposition within thevascular walls of the post-capillary venules in the superficial dermis. There are only 4 previous casesdescribed in the medical literature, all in males, mostly middle-aged. We have recently seen two femalepatients with clinical and histopathologic features diagnostic of cutaneous collagenous vasculopathy,indicating that it is not restricted to males. As cutaneous collagenous vasculopathy can be clinicallyindistinguishable from generalized essential telangiectasia, and histopathologic studies are rarely performedfor this condition, it is likely that cutaneous collagenous vasculopathy frequently passes unrecognized, but itmay be more common than previously thought. ( J Am Acad Dermatol 2010;63:882-5.)
CASE REPORTSCase 1
A 51-year-old woman presented with widespreadtelangiectasia. Changes first developed in her lowerlegs shortly after the delivery of her first child, 16years previously. Subsequently, telangiectases ex-tended to her trunk, upper limbs, and neck. Thepatient reported that the changes were more notice-able in the summer and that the skin occasionallyitched. There was no personal or family history of ableeding diathesis and, except for hypothyroidismand psoriasis, she was otherwise well. Review ofsystems was unremarkable with no symptoms sug-gestive of a connective tissue disease. On examina-tion, generalized telangiectasia affecting the trunkand limbs was noted, extending to the neck andretroauricular area, with no nail or mucosal involve-ment (Fig. 1). Darier’s sign was negative. At thisstage, our clinical differential diagnosis includedgeneralized essential telangiectasia and telangiecta-sia macularis eruptiva perstans.
Routine biochemistry, complete blood cell count,and inflammatory markers (C-reactive protein, eryth-rocyte sedimentation rate) were all within normal
St John’s Institute of Dermatology, St Thomas’ Hospital.
ing sources: None.
licts of interest: None.
nted at a regional meeting in the United Kingdom.
int requests: C. M. Stefanato, MD, FRCPath, St John’s Institute
Dermatology, St Thomas’ Hospital, London SE1 7EH, UK.
mail: [email protected].
ished online May 7, 2010.
-9622/$36.00
09 by the American Academy of Dermatology, Inc.
0.1016/j.jaad.2009.06.045
range. An autoimmune screening, including rheuma-toid factor, antinuclear antibodies, double-strandedDNA, extractable nuclear antigen [ENA], and anticen-tromere antibodies, was negative. Creatine kinase andtryptase levels were normal.
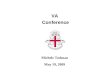
A skin biopsy specimen with control of neighbor-ing unaffected skin taken using lidocaine withoutepinephrine demonstrated telangiectasia of the pap-illary dermal capillaries with thickening of the vesselwalls by hyaline perivascular material. The perivas-cular hyaline material was highlighted by periodicacideSchiff, collagen IV, and laminin stains (Fig 2).Chloracetate esterase stain revealed normal mast cellnumbers. Taken together, these features were diag-nostic of cutaneous collagenous vasculopathy.1
Case 2A 71-year-old woman presented with a 4-year
history of progressive widespread telangiectasia. Theeruption commenced in 2003, 3 to 4 months aftertreatment of a benign pituitary tumor with radiother-apy. Changeswere first noticed on the dorsal surfacesof her feet and thereafter gradually spread to affecther right knee, upper arms, left side of the chest, andright cheek. She was taking no medication at theonset of the rash with the exception of calciumsupplementation for osteoporosis. She was other-wise well and reported no photosensitivity, muscleweakness, or other symptoms, nor was there any pastmedical or family history of a bleeding diathesis.
On examination she had widespread patchy areasof telangiectasia with no atrophy or pigment changeaffecting the feet, right knee, upper arms, and rightcheek. There was no evidence of nail or mucosalinvolvement.

Fig 1. Generalized telangiectasia affecting trunk and limbs in case 1.
J AM ACAD DERMATOL
VOLUME 63, NUMBER 5
Perez et al 883
Routine investigations, autoimmune screen, crea-tine kinase, and lactate dehydrogenase were allwithin the normal range. Skin biopsy showed telan-giectatic vessels in the papillary dermis with perivas-cular hyalinization, which was highlighted with PASand collagen IV stains. A diagnosis of cutaneous
collagenous vasculopathy was made in view of thecharacteristic histologic findings.
DISCUSSIONCutaneous collagenous vasculopathy was first
described by Salama and Rosenthal1 in 2000. Since
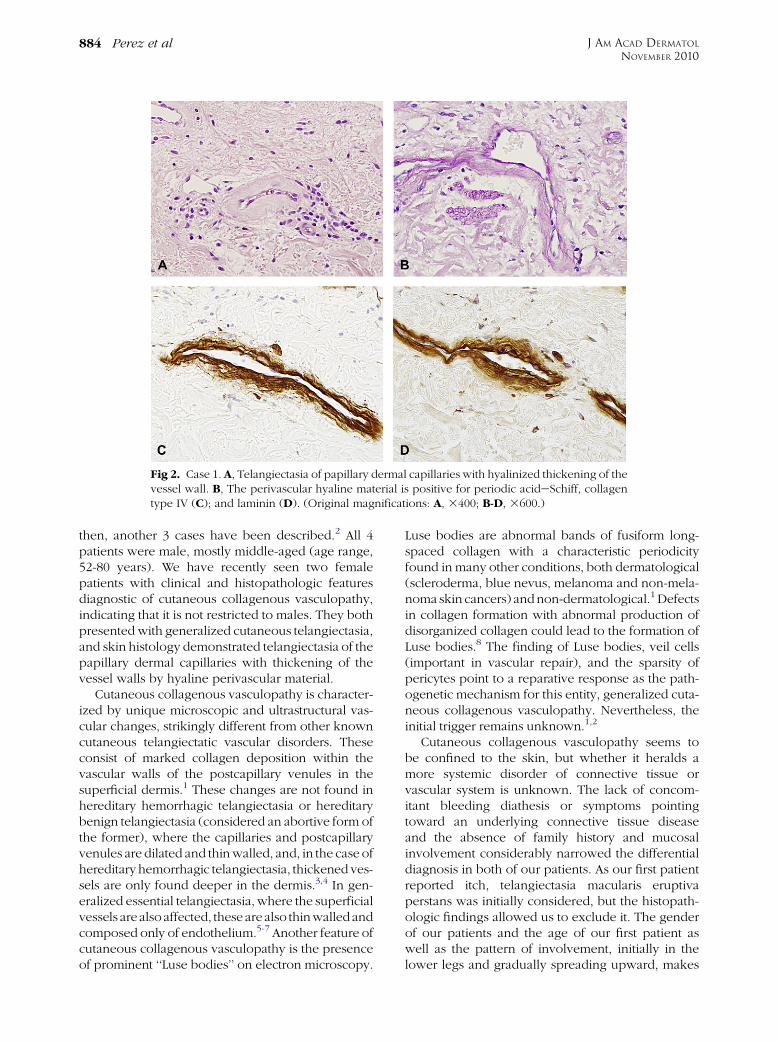
Fig 2. Case 1. A, Telangiectasia of papillary dermal capillaries with hyalinized thickening of thevessel wall. B, The perivascular hyaline material is positive for periodic acideSchiff, collagentype IV (C); and laminin (D). (Original magnifications: A, 3400; B-D, 3600.)
J AM ACAD DERMATOL
NOVEMBER 2010
884 Perez et al
then, another 3 cases have been described.2 All 4patients were male, mostly middle-aged (age range,52-80 years). We have recently seen two femalepatients with clinical and histopathologic featuresdiagnostic of cutaneous collagenous vasculopathy,indicating that it is not restricted to males. They bothpresented with generalized cutaneous telangiectasia,and skin histology demonstrated telangiectasia of thepapillary dermal capillaries with thickening of thevessel walls by hyaline perivascular material.
Cutaneous collagenous vasculopathy is character-ized by unique microscopic and ultrastructural vas-cular changes, strikingly different from other knowncutaneous telangiectatic vascular disorders. Theseconsist of marked collagen deposition within thevascular walls of the postcapillary venules in thesuperficial dermis.1 These changes are not found inhereditary hemorrhagic telangiectasia or hereditarybenign telangiectasia (considered an abortive form ofthe former), where the capillaries and postcapillaryvenules are dilated and thin walled, and, in the case ofhereditary hemorrhagic telangiectasia, thickened ves-sels are only found deeper in the dermis.3,4 In gen-eralized essential telangiectasia, where the superficialvessels are alsoaffected, these are also thinwalledandcomposed only of endothelium.5-7 Another feature ofcutaneous collagenous vasculopathy is the presenceof prominent ‘‘Luse bodies’’ on electron microscopy.
Luse bodies are abnormal bands of fusiform long-spaced collagen with a characteristic periodicityfound in many other conditions, both dermatological(scleroderma, blue nevus, melanoma and non-mela-noma skin cancers) andnon-dermatological.1 Defectsin collagen formation with abnormal production ofdisorganized collagen could lead to the formation ofLuse bodies.8 The finding of Luse bodies, veil cells(important in vascular repair), and the sparsity ofpericytes point to a reparative response as the path-ogenetic mechanism for this entity, generalized cuta-neous collagenous vasculopathy. Nevertheless, theinitial trigger remains unknown.1,2
Cutaneous collagenous vasculopathy seems tobe confined to the skin, but whether it heralds amore systemic disorder of connective tissue orvascular system is unknown. The lack of concom-itant bleeding diathesis or symptoms pointingtoward an underlying connective tissue diseaseand the absence of family history and mucosalinvolvement considerably narrowed the differentialdiagnosis in both of our patients. As our first patientreported itch, telangiectasia macularis eruptivaperstans was initially considered, but the histopath-ologic findings allowed us to exclude it. The genderof our patients and the age of our first patient aswell as the pattern of involvement, initially in thelower legs and gradually spreading upward, makes

J AM ACAD DERMATOL
VOLUME 63, NUMBER 5
Perez et al 885
generalized essential telangiectasia the main clinicaldifferential diagnosis for our patients’ presentation.
We have described two additional cases of cuta-neous collagenous vasculopathy, this time both infemales. As this entity is clinically indistinguishablefrom generalized essential telangiectasia and physi-cians often fail to perform a biopsy, we suspect thatcutaneous collagenous vasculopathy frequentlypasses unrecognized. The unique microscopic andultrastructural abnormalities that are found in thepostcapillary venules of the superficial dermis arenevertheless diagnostic and highlight the importanceof clinicopathologic correlation for the accuratediagnosis of this condition.
REFERENCES
1. Salama S, Rosenthal D. Cutaneous collagenous vasculopathy
with generalized telangiectasia: an immunohistochemical and
structural study. J Cutan Pathol 2000;27:40-8.
2. Davis TL, Mandal RV, Bevona C, Tsai KY, Moschella SL,
Staszewski R, et al. Cutaneous collagenous vasculopathy: a
report of three cases. J Cutan Pathol 2008;35:967-70.
3. Braverman IM, Keh A, Jacobson BS. Ultrastructural and
three-dimensional organization of telangiectases of heredi-
tary haemorrhagic telangiectasia. J Invest Dermatol 1990;95:
422.
4. Zahorcsek ZS, Schneider I. Hereditary benign telangiectasia.
Dermatology 1994;189:286-8.
5. Requena L, Sangueza OP. Cutaneous vascular anomalies: Part 1:
Hamartomas, malformation and dilatation of pre-existing ves-
sels. J Am Acad Dermatol 1997;37:523.
6. McGrae JD Jr, Winkelmann RK. Generalized essential telangiec-
tasia. JAMA 1963;185:909.
7. Sanchez JL, Ackerman AB. Vascular proliferations of
skin and subcutaneous fat. In: Fitzpatrick TB, Eisen AZ,
Wolff K, Freedberg IM, Austen KF, editors. Dermatology in
general medicine. 4th ed. New York: McGraw-Hill; 1993. p.
1209.
8. Ghadially FN. Extracellular matrix (extracellular components).
Ultrastructural pathology of the cell and matrix. 4th ed. London:
Butterworths-Heineman; 1997. p. 1307.