Embed Size (px)
Citation preview

Born : Jakarta, September 1955 Education 1. GP : FKUI, 1980 2. Radiologist : FKUI, 1987 3. Radiation Oncologist : FKUI / Muenster
(Germany) 1990 4. PhD : FKUI, 1998 (EBV LMP1 and
Proliferation in NPC)
Current Positions : Chairperson of Indonesian National Cancer Control Committee (KPKN)
President of Indonesian Radiation Oncology Society (PORI) President of Federation of Asian Organizations of Radiation Oncology (FARO)
Past President of South East Asia Radiation Oncology Group (SEAROG)
CURRICULUM VITAE Soehartati Gondhowiardjo, MD. PhD

Implementation of New Technologies in LMIC: 3D HDR Brachytherapy
Soehartati Gondhowiardjo
ICARO2, Vienna, June 20th-23rd , 2017

Introduction
• In 2011 Potter et al. reported the clinical outcome of the patients treated after the introduction of IGBT (2001–2008) vs historical controls , showed :
• Significant improvement in local control at 3 years; 95–100% in stage IB/IIB, and 85–90% in stage IIB–IV
• relative reduction of pelvic recurrence of 65–70% compared to their conventional results.
• Overall survival rates at 3 years were 74–79% for stage IB/IIB, and 45% for stage IIIB, significantly increased compared to their historical series, and rates of severe morbidity were reduced
• Other institutions which have published their first results also showed promising outcomes
Potter et al. , Radiotherapy and Oncol.,2011

Conventional BT vs IGBT
Rijkmans et al., Gynecologic Oncol., 2014

•
Kim, Hayeon et al. Cost-effectiveness analysis of 3D image-guided brachytherapy compared with 2D brachytherapy in the treatment of locally advanced cervical cancer Brachytherapy 2015, 14 (1):, 29 - 36


Sensitivity Analysis....
Note: The x-axis represents the difference in costs between 3D and 2D treatments. The y- axis is the difference in survival between 3D and 2D treatments. The ‘‘X’’ on the graph represents the baseline values. Area above the line slope represents that 3D image-guided brachytherapy is a favored strategy. (using a $50,000 per QALY gained threshold ) Kim, Hayeon et al. Cost-effectiveness analysis of 3D image-guided brachytherapy compared with 2D brachytherapy in the treatment of locally advanced cervical cancer. Brachytherapy 2015, 14 (1):, 29 - 36

IAEA/RCA RAS/6/062 “Supporting 3D IGBT Services”
(2012-2015)
Courtessy of Prof Shingo Kato, PLCC for IAEA RCA RAS 6/062
・ 4 RTCs were held from 2012 to 2015, NTC in each country
・ 121 RO and MP were trained at RTCs.
・ Training materials were available at the IAEA website.
・ Guideline Transition from 2DBrachytherapy to 3D High Dose Rate Brachytherapy” was published.
・ Number of hospitals which implement 3D IGBT have increased in RCA MS (11% in 2012, 19% in 2015) .

Objective To Improve regional and national capacities for brachytherapy services by implementing 3D-IGBT by 2020. To strengthen the ability of RCA Member States to use the modern technology and evidence-based guidelines.
9
Participating countries
AUL, BAN, CHA, IND, INS, JPN, KOR, MAL, MON, MYN, PAK, PHI, SIN, THA, VIE (15 countries)
1. Ros & MPs in RCA MSs are trained in the knowledge and techniques 2. Treatment guidelines for 3D IGBT are developed among RCA MSs.
Expected outcomes

National Training Courses
National Training Courses
National Training Courses
4 RTCs (mumbai, chiang mai, saitama, singapore) NTCs in each country
Training of ROs and MPs Regional Training Courses
Activities

11
Transition from 2-D Brachytherapy to 3-D High Dose
Rate Brachytherapy
INTERNATINAL ATOMIC ENERGY IAEA DRAFT 2013-06-25
Guidelines IAEA TECDOC “Transition from 2-D brachytherapy to 3-D high dose rate brachytherapy” was published.
Utilization of guideline
Utilization of Guideline
Utilization of guideline
http://www-pub.iaea.org/MTCD/Publications/PDF/Pub1681web-80878722.pdf
Activities

Surveys on 3D IGBT among RCA MSs
1st survey: 2012 and to assess current status on resources and capabilities of 3D IGBT and 2nd survey : 2015 to assess the progress
Activities
13
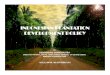
Dissemination of 3D IGBT to RCA Countries
Country
AUL
CHA
JPN
MAL
MON
PHL
SIN
THA
INS
All
No. of hospitals implementing 3D IGBT 2012
20/23
10/300
22/135
0/7
0/1
2/25
3/3
5/26
0/27
62/520 (12%)
2015
21/23
20/300
39/135
5/8
0/1
3/32
3/3
11/29
5/29
103/531 (19%)
Survey Data
INS 0/27 5/29
All 62/547(11%) 108/560 (19%)

Difficulties in introducing 3D IGBT in the hospital
Difficulty in accessing MRI/CT at BT, in use CT/MRI for planning
Manpower shortage
Heavy workload
Shortage of equipment; CT/MRI, 3D TPS, MRI applicator
Poor cost/remuneration
Small number of patient (MAL) ???
Limited time for 3D planning
Survey Data

Current Radiotherapy Condition in FARO member countries
World Population : 7 B people Asia Population : 4.478.315.164 FARO Population : 3.762.526.250 ASIA 60 % of World Population FARO 84% OF ASIA Population FARO 53 % of World Population

Japan P:126 M M : 841
Ratio: 1:0.15
South Korea P: 50 M M : 1.36
Ratio: 1:0.3
China P:1386 M M : 2140
Ratio: 1:0.65
Indonesia P: 261 M
M : 80 Ratio: 1:3.26
Philippines P:103 M M : 36
Ratio: 1:0.15 Srilanka P: 20 M M : 14
Ratio: 1:1.43
India P:1338 M M : 589
Ratio: 1:2.27
Bangladesh P:164 M M : 25
Ratio: 1:6.56
Malaysia P: 31 M M : 47
Ratio: 1:0.15
Thailand P:68 M M : 76
Ratio: 1:0.39
Singapore P: 6 M M : 20
Ratio: 1:0.3
Pakistan P: 200 M
M : 29 Ratio: 1: 6.89
Radiotherapy In OUR REGION No Negara Population
in Million Total
Machines Ratio TT : Pop 2017
/ equipment
1 Japan 126 841 1 : 0.15 6.67
2 South Korea 50 136 1 : 0.3 3.33
3 Singapore 6 20 1 : 0.3 3.33
4 Thailand 68 76 1 : 0.39 2.56
5 China 1.386 2140 1 : 0.65 1.53
6 Malaysia 31 47 1 : 0.66 1.51
7 Srilanka 20 14 1 : 1.43 0.699
8 Philippines 103 36 1 : 2.26 0.44
9 India 1.342 589 1 : 2.27 0.44
10 Indonesia 263 80 1 : 3.26 0.30
11 Bangladesh 164 25 1 : 6.56 0.15
12 Pakistan 196 29 1 : 6.89 0.14
The diversities in FARO Countries : a huge gap!
How about Brachytherapy ??
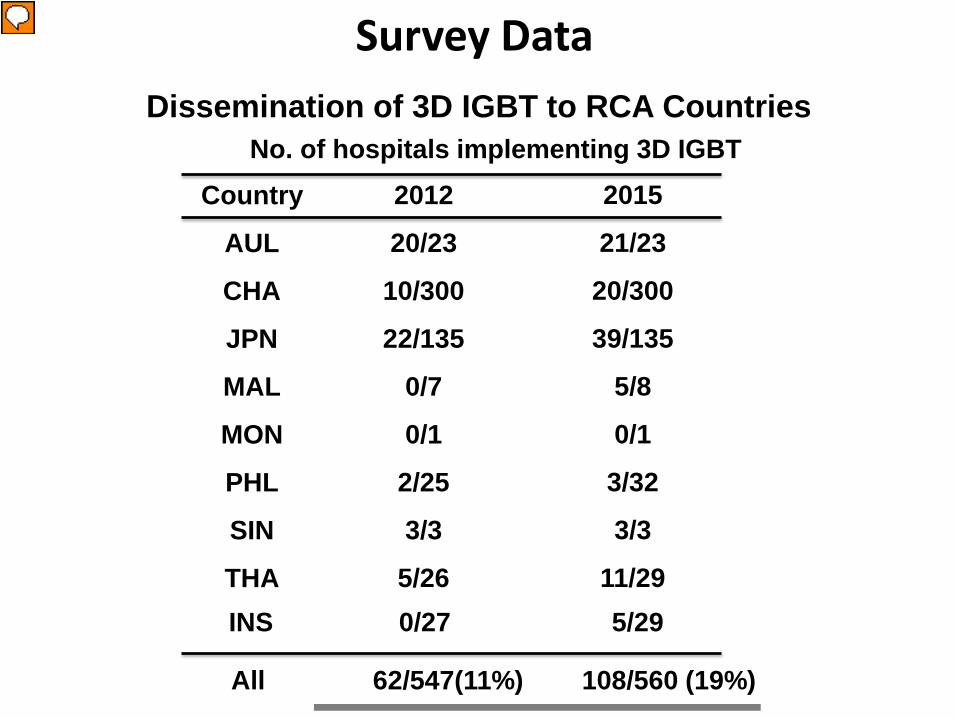
FARO Survey (2017): Availability of 3D Brachytherapy
0
200
400
600
800
1000
1200
1400
1600
1800
Japa
n
Kore
a
Sing
apor
e
Chin
a
Thai
land
Mal
aysia
Phill
ipin
es
Indo
nesia
Indi
a
Paki
stan
Sri L
anka
Bang
lade
sh
1 2 3 4 5 6 7 8 9 10 11 12
Availability of RT Centers, Brachytherapy service, and
Brachytherapy 3D in FARO member countries
Total RT centres RT Centers with BT 3D Brachytherapy
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Proportion of centers with EBRT only, 2D and 3D Brachytherapy
EBRT Only 2D BT 3D BT
21 % in average
(Except India and Malaysia)
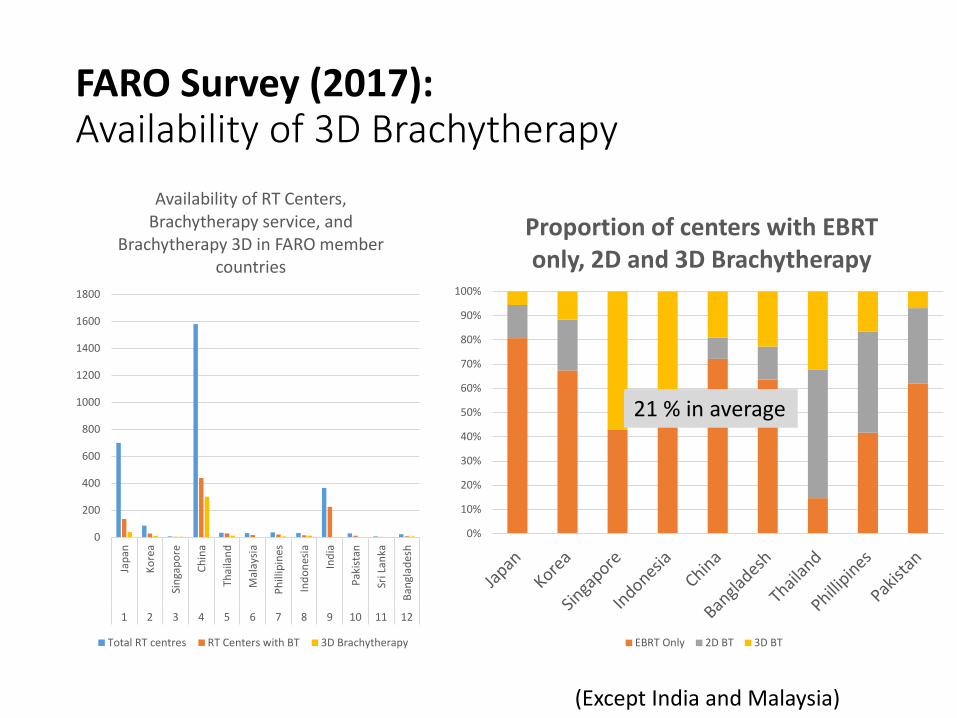
FARO Survey (2017): Imaging modality for 3D Brachytherapy
CT Scan is the most commonly used imaging
FARO Survey (2017): Most common diagnosis for BT: Cervical Cancer

FARO Survey (2017): Challenges in implementing Brachytherapy 3D
• Lack of government investment • Difficulty in accessing CT/MRI at BT • Longer time to perform IGBT compared to 2D (2D: 5 pts,
3D: 2-3 pts) • Lack of man power and training • Higher workload for dosimetry/physics staff and physicians • Additional cost for CT Scan for 3D brachytherapy (per
session) • Additional cost of an MRI prior to doing a 3D brachytherapy • In some countries, health insurance doesn’t cover the
additional cost for 3D brachytherapy.
Survey Implementing 3D BT in Indonesia
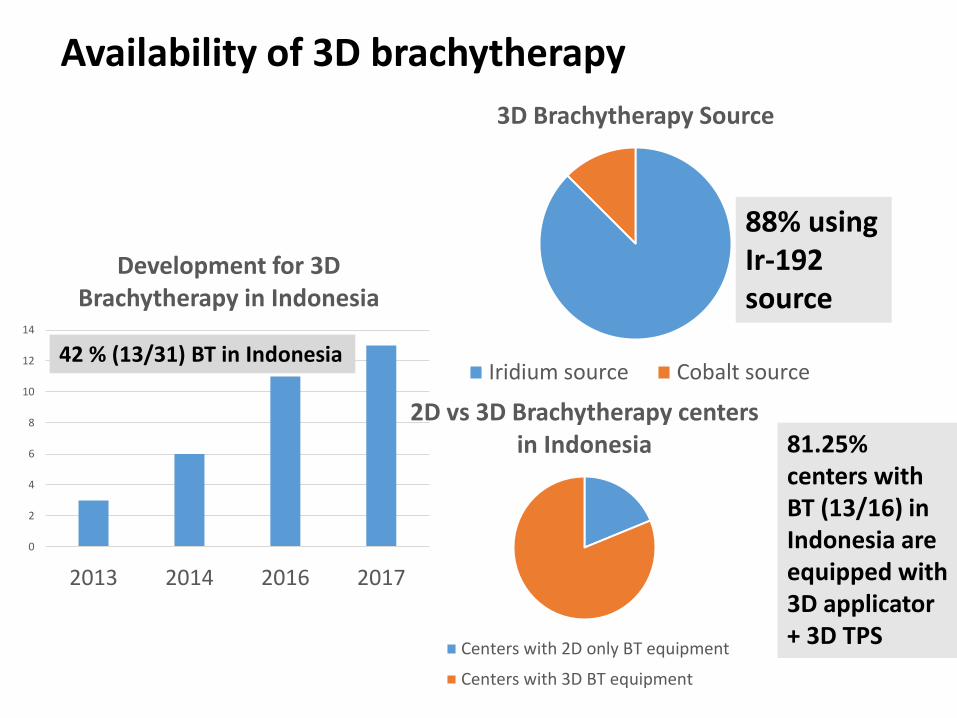
Availability of 3D brachytherapy
88% using Ir-192 source
81.25% centers with BT (13/16) in Indonesia are equipped with 3D applicator + 3D TPS
0
2
4
6
8
10
12
14
2013 2014 2016 2017
Development for 3D Brachytherapy in Indonesia
3D Brachytherapy Source
Iridium source Cobalt source
2D vs 3D Brachytherapy centers in Indonesia
Centers with 2D only BT equipment
Centers with 3D BT equipment
42 % (13/31) BT in Indonesia

• 11 centers with 3D BT equipment available
Despite the availability of 3D applicator and 3D TPS, more than 64% of those centers are still performing 2D technique
0% 20% 40% 60% 80% 100% 120%
Dharmais Cancer Center
Saiful Anwar Hospital
Kariadi Hospital Semarang
Margono Soekarjo Hospital
Sardjito Hospital
Murni Teguh Hospital
Dr Cipto Mangunkusumo Hospital
Univ Hasanuddin Makasar Hospital
Santosa Bandung Hospital
Soetomo Hospital
MRCCC Hospital
% of 3D Pts % of 2D Pts
11
10
9
8
7
6
5
4
3
2
1
0
1
2
3
4
5
6
Access toCT/MR
Time consumingReimbursement Lack of trainedman power
Limitedapplicator
Challenges in performing 3D techniques

Difficulties in introducing 3D IGBT in the hospital
Survey Data (Summary)
Items IAEA RCA RAS6/062
FARO Survey 2017
IROS Survey 2017
INVESTMENT Shortage of 3D BT Equipment (CT/MR applicator, TPS, CT/MR)
✔ ✔ ✔
Difficulties in accessing CT/MR at BT ✔ ✔ ✔
HUMAN RESOURCE
Lack of man power ✔
✔
✔
Higher workload ✔ ✔ ✔
TIME Longer time to perform IGBT ✔ ✔ ✔
Higher workload for dosimetry ✔ ✔ ✔
COST Additional cost of an MRI prior to doing a 3D brachytherapy
✔ ✔ ✔
In some countries, health insurance doesn’t cover additional cost for 3D BT
✔ ✔ ✔
No OF PTS Small number of patients ✔
High demand BOT
Training program Increase the number of HR
Improve the system CT dedicated for BT Increase the number of HR
Convinced the government to improve the tariff include the CT Cost sharing from the patients
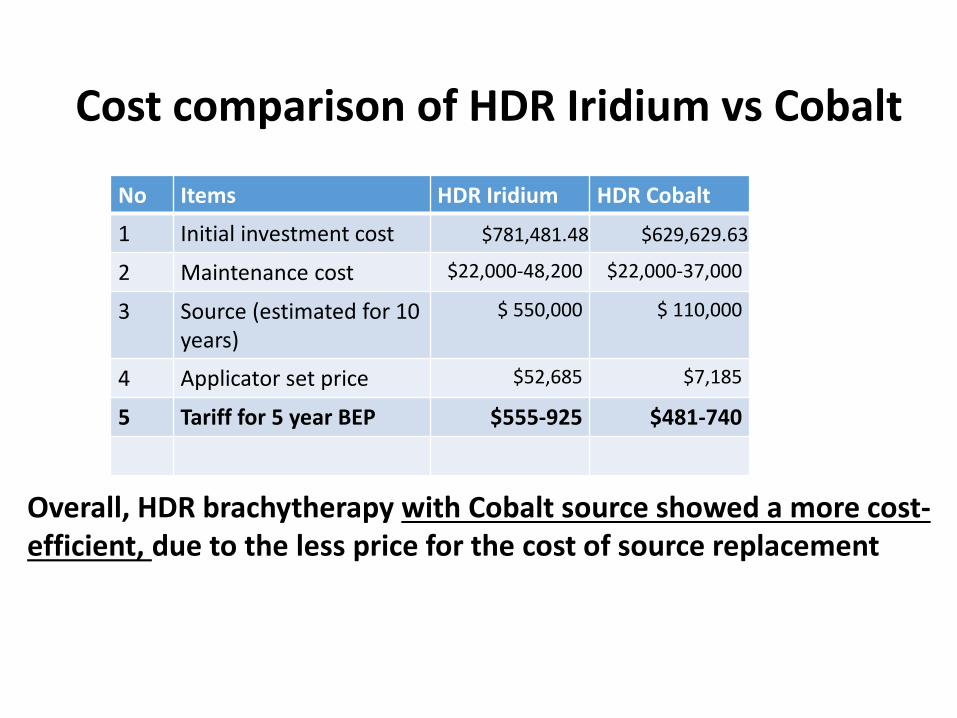
Cost comparison of HDR Iridium vs Cobalt
No Items HDR Iridium HDR Cobalt
1 Initial investment cost $781,481.48 $629,629.63
2 Maintenance cost $22,000-48,200 $22,000-37,000
3 Source (estimated for 10 years)
$ 550,000 $ 110,000
4 Applicator set price $52,685 $7,185
5 Tariff for 5 year BEP $555-925 $481-740
Overall, HDR brachytherapy with Cobalt source showed a more cost-efficient, due to the less price for the cost of source replacement

Cost comparison of 2D vs 3D HDR Brachytherapy
No Items Iridium Cobalt
1 Initial investment cost $781,481.48 $629,629.63
2 Maintenance cost $22,000-48,200 $22,000-37,000
3 Source (estimated for 10 years)
$ 550,000 $ 110,000
4 Applicator set price $52,685 $7,185
5 Tariff for 5 year BEP
2D $555 $481
3D $925 $740
! Not included the additional cost for CT scan with/without MR imaging prior to BT 3D procedure !
Cost difference 3D- 2D = ~ 260-370 USD
3D HDR brachytherapy is more costly, but cost effectiveness could be better depends on clinical outcome and utility (use our own QALY gained threshold )

Special Acknowledgement for Data Contribution • All FARO council members • Prof Shingo Kato, PLCC for IAEA RCA RAS 6/062 • Members of the Indonesian Radiation Oncology
Society (IROS)
Year 0Investment
Ye
28,660,000,000.00 34,563
28,660,000,000.00 34,563
3,117 20,815
23,932
9,573
14,359Rp
14,359 (20,204
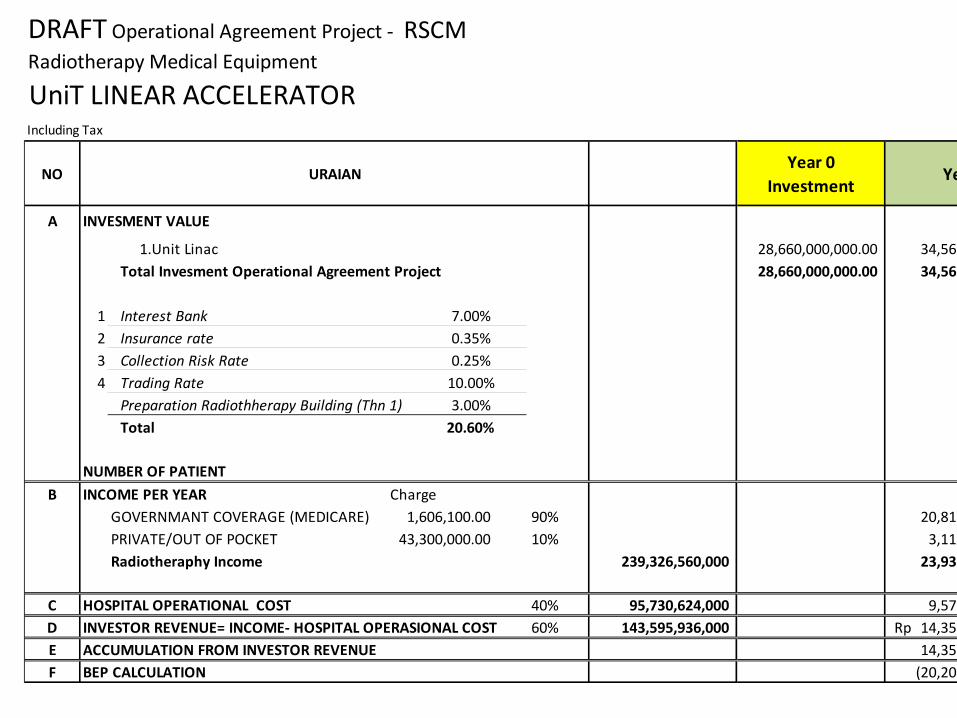
DRAFT Operational Agreement Project - RSCMRadiotherapy Medical Equipment
UniT LINEAR ACCELERATORIncluding Tax
INVESMENT VALUE
1.Unit LinacTotal Invesment Operational Agreement Project
1 Interest Bank2 Insurance rate3 Collection Risk Rate4 Trading Rate
Preparation Radiothherapy Building (Thn 1)Total
NUMBER OF PATIENTINCOME PER YEAR Charge
GOVERNMANT COVERAGE (MEDICARE) 90%PRIVATE/OUT OF POCKET 10%Radiotheraphy Income 239,326,560,000
HOSPITAL OPERATIONAL COST 40% 95,730,624,000 INVESTOR REVENUE= INCOME- HOSPITAL OPERASIONAL COST 60% 143,595,936,000 ACCUMULATION FROM INVESTOR REVENUEBEP CALCULATION
NO URAIAN
A
7.00%0.35%0.25%
10.00%3.00%
20.60%
B
43,300,000.00 1,606,100.00
C
D
E F

12,500,000,000
Tahun 0Investasi
12,500,000,000
DRAFT BISNIS PLAN Radiotherapy Medical EquipmentUniT Brakiterapi(Dalam RUPIAH) - EXCL PPN
NILAI INVESTASI1 Unit Brachytherapy
Total Investasi (24,6%)
JUMLAH TINDAKAN PER TAHUNPENDAPATAN PER TAHUN Tarif
Tarif rawat jalan 20%
Tarif rawat inap 80%
Ringan 60%Sedang 40%
Pendapatan Radioterapi 38,923,591,680.00
OPERASIONAL RS (40%)
ALOKASI INVESTASI (60%) 23,354,155,008.00
NILAI AKUMULASI ALOKASI INVESTASI
D
E
C
B
NO URAIAN
A
PERHITUNGAN BEP
F
1,144,400.00
4,090,100.00 8,056,000.00

2nd FARO MEETING: BENGALURU, INDia 9-10 November 2017
On ICC website: http://www.indiancancercongress2017.com/#registration
3rd FARO Meeting, BALI 2018
THANK YOU!
Website: www.faroac.org Facebook: www.facebook.com/faro.organization/
Contact Detail FARO Secretariat Office: Address c/o Radiation Oncology, Graduate School of Medicine, Gunma University Show Machi 3-339-22. Maebashi-Shi, Gunma-Ken, 371-8511 Japan Tel +81-027-220-8380 E-mail [email protected]
For FARO Database: project.computesta.com/faro-db/web