Embed Size (px)
Citation preview
Current Therapies for Immune Mediated Hemolytic Anemia in Dogs.
Autoimmune disease treatment in dogs currently relies on the use of broad-spectrum
immunosuppressive drugs, which are associated with unacceptable adverse effects in
some patients. Immune Mediated Hemolytic Anemia (IMHA) requires high doses and
long-term administration of these medications, often resulting in a terrible choice for the
pet owner between the disease, the medications or euthanasia (1) (2). Stem cell
therapy offers an alternative option for these pets.
Overview Immune Mediated Hemolytic Anemia (IMHA) is caused by antibody deployment against
red blood cells. The presence of these autoantibodies initiate destruction of the red
blood cells through one of two ways: complement activation results in hemolysis
(rupture) of the red blood cells within the blood stream, or macrophages in the spleen
and liver gradually destroy the red blood cells (3). Immunosuppressive drugs dampen
the immune response but do not address the underlying cause - the inciting antibody
production. Stem Cell Therapy addresses both the underlying cause of anti-red blood
cell antibody production and protects the antibody tagged red blood cells from
destruction. Stem Cells, unlike conventional therapeutics are alive and dynamically self-
modulate their response to immune disease thereby preventing over-reaction or
overdoses in therapy (4).
To best understand the mode of action of Allogenic Mesenchymal Stem Cell (AMSC)
therapy we need to review a detailed description of the pathogenesis of the immune
dysfunction underlying Immune Mediated Hemolytic Anemia (IMHA) in dogs.
Understanding IMHA Immune reactions against red blood cells happen when antibodies are made against the
proteins on the surface of these cells. These antibodies signal that these “tagged” cells
should be destroyed. This happens either in the bloodstream (intravascular hemolysis)
or within the liver and spleen (extravascular hemolysis). Once red blood cells are
destroyed, the clinical signs are mostly attributable to loss of oxygen to the tissues. The
by-products of red blood cell destruction affect the liver and kidney and the lungs
causing blood clots and multiple organ failure. Death occurs in approximately 25% of
extravascular cases and 75% of intravascular cases.
Steven D. Garner
Chief of Staff
Safari Veterinary Care Centers
2402 Marina Bay Drive
League City, TX 77573
281-332-5612
Why does the Body Produce Antibodies against its own Red Blood Cells?
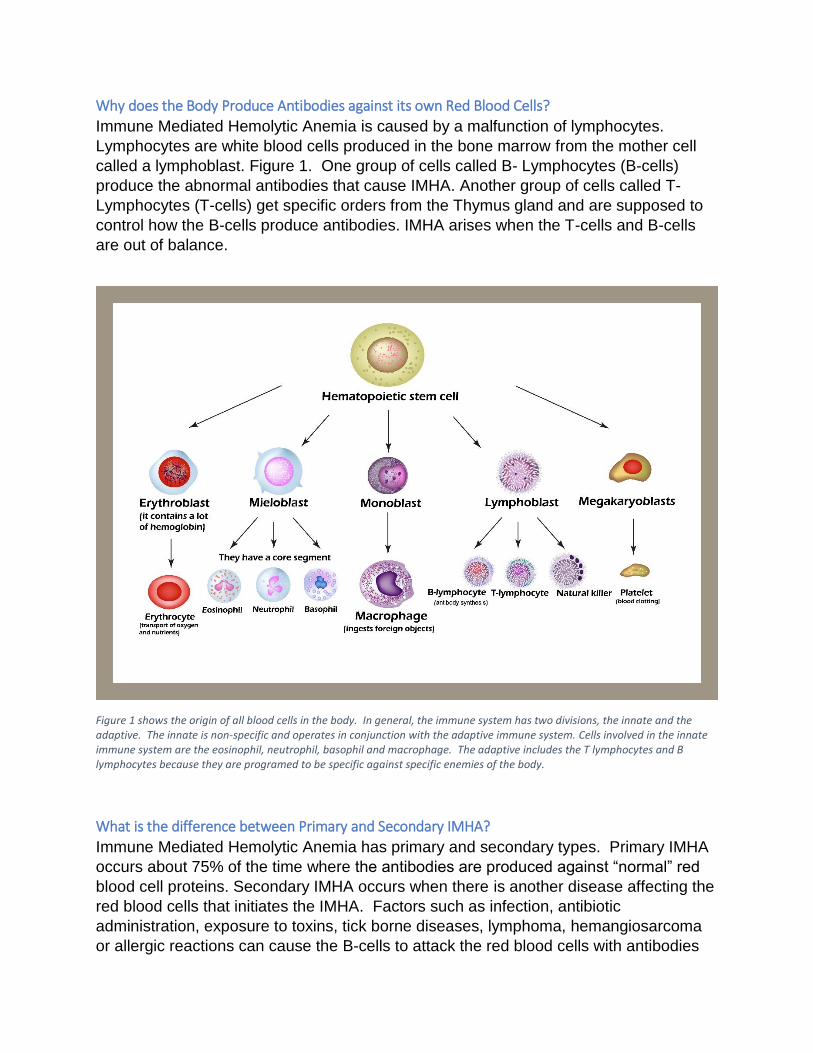
Immune Mediated Hemolytic Anemia is caused by a malfunction of lymphocytes.
Lymphocytes are white blood cells produced in the bone marrow from the mother cell
called a lymphoblast. Figure 1. One group of cells called B- Lymphocytes (B-cells)
produce the abnormal antibodies that cause IMHA. Another group of cells called T-
Lymphocytes (T-cells) get specific orders from the Thymus gland and are supposed to
control how the B-cells produce antibodies. IMHA arises when the T-cells and B-cells
are out of balance.
Figure 1 shows the origin of all blood cells in the body. In general, the immune system has two divisions, the innate and the adaptive. The innate is non-specific and operates in conjunction with the adaptive immune system. Cells involved in the innate immune system are the eosinophil, neutrophil, basophil and macrophage. The adaptive includes the T lymphocytes and B lymphocytes because they are programed to be specific against specific enemies of the body.
What is the difference between Primary and Secondary IMHA?
Immune Mediated Hemolytic Anemia has primary and secondary types. Primary IMHA
occurs about 75% of the time where the antibodies are produced against “normal” red
blood cell proteins. Secondary IMHA occurs when there is another disease affecting the
red blood cells that initiates the IMHA. Factors such as infection, antibiotic
administration, exposure to toxins, tick borne diseases, lymphoma, hemangiosarcoma
or allergic reactions can cause the B-cells to attack the red blood cells with antibodies

resulting in secondary IMHA. Secondary IMHA is usually a temporary disease that
resolves when the offending substance or infection is removed, stopped, or treated.
Primary IMHA occurs when normal red blood cell proteins are attacked abnormally.
Primary IMHA has two forms – Intravascular and Extravascular. Intravascular IMHA
has a much higher mortality rate (75%) and occurs when the antibodies activate
Complement. Extravascular IMHA occurs when nibbles are bitten off the surface of the
red blood cells by macrophages as they pass through the spleen and liver. This slower
process is still very serious but has only a 25% mortality rate.
The Importance of Complement
Complement is the name for a group of molecules present in the blood plasma that
enhances (complements) the immune system. These molecules when combined cause
intravascular hemolysis in IMHA. Complement activation is shown in Figure 2.
Figure 2. Complement activation starts when antibodies are attached to Red Blood Cells, ultimately creating the Membrane Attack Complex (knife) shown above. Once formed this knife cuts through the surface of the red blood cells see Figure 3.
Figure3. “Mr. Red Cell being attacked by activation of the complement cascade causing intravascular hemolysis in IMHA.
Figure 4. Depicts the stem cell as a superhero which produces Factor H that acts like Kevlar to protect the cell membrane from the Membrane Attack complex (knife).
NORMAL RBC➔ ANTIGEN COATED ➔ANTIBODY COATED ➔ COMPLEMENT ATTACK
Mr. Red Cell
STEM CELL ➔FACTOR H (KEVLAR) ➔PREVENTS COMPLEMENT ATTACK
Mr. Stem Cell
Factor H Protects Cells from Complement Attack
Factor H regulates complement. Factor H provides control by binding to the surfaces of
cells to protect cell surfaces from the cutting and puncturing of the knife-like
complement molecule. Like the Kevlar worn by law enforcement officials protects them
from knives and bullets, Factor H protects the cells from complement attack. Factor H is
produced by stem cells.
Stem Cells Produce Factor H
We have known for some time that Mesenchymal stem cells (MSCs) possess potent
immunosuppressive properties (5). But only recently did we understand that MSCs
produce Factor H (6). Mesenchymal stem cell therapy has been shown to stop the
damage from many auto-immune diseases and the mechanism for this effect has been
shown to be due to the production of Factor H by the mesenchymal stem cells and
subsequent protection against complement damage (7). MSCs production of Factor H
is constitutive (8). This means that Factor H is produced in relatively constant amounts
regardless of the environment or stimulation. This is an important justification for the use
of allogenic mesenchymal stem cells for the treatment of IMHA.
What is meant by Immune Tolerance? The purpose of the immune system is to remove foreign invaders. To do this it has to
recognize who is supposed to be in the body and who is alien and a potential threat to
the body. Red blood cells that are being attacked by antibodies in IMHA have been
mistakenly determined to be foreign. How did this happen and how can this problem be
fixed?
There are natural balances in the controls of the immune system that we are just
coming to understand. These balances involve the production of different types of T-
Lymphocytes (T-cells) depending on the need for immunity vs. the need to tolerate the
presence of a seemingly abnormal protein or substance. For example, our intestine
houses many species of bacteria that are arguably foreign to our bodies, yet our
immune system tolerates their presence. Mammals who maintain placental pregnancy
within their bodies must tolerate the foreign tissue of the developing fetus with different
DNA than the mother and not attack it as foreign. The surface of the skin and opening of
the mucous membranes harbor “normal” bacterial and fungal flora that must be
tolerated by the immune system. On the other hand, cells that are infected or damaged
or that have turned cancerous should be attacked and removed from the body by the
same immune system. It is this balance that is defective with IMHA.
Recent experiments involving the thymus gland have uncovered previously unknown
elements of the T-cell populations that help control these systems. The thymus is a
small gland in the chest between the left and right lungs at the level of the trachea that
has been found to be essential in the control of the immune system. T-cells are named
after the thymus because they are processed within this small organ. Mutant mice
which do not have a thymus gland spontaneously develop fatal, widespread, early-onset
autoimmunity (9). Removal of the thymus gland in three-day old mice led to the rapid
development of autoimmunity that was corrected by the infusion of T-cells from adult
mice. This research advanced our understanding of the creation and management of
the T-cell lineage and how it controls the immune system. Certain T-cell types regulate
or keep in check the aberrant or overactive activity of other T-cells. When the immune
system functions normally, the immune system produces a population of T-cells that are
regulatory called regulatory T cells or Tregs that are specialized for immune
suppression (10). In addition, it is becoming apparent that every immune reaction not
only creates specific B-Cells and T-Cells but also Tregs and the balance between the
populations of cells is critical for the proper control of the immune response. IMHA is an
example of an excessive attack on self-antigens as a result of improper immune
tolerance resulting from dysregulation or deficiency of the Tregs (1) (10).
What is the role of stem cells in the immune system
Mesenchymal stem cells exert powerful control over the creation and modulation of
Tregs through the release of powerful chemicals called cytokines. Mesenchymal stem
cells release the cytokine Transforming Growth Factor Beta (TGF-β) which induces the
development of Tregs (4) (9) (8) (11). This is an important justification for the use of
allogenic mesenchymal stem cells for the treatment of IMHA.
To understand the implications of treatment choices made for the benefit of pets with
IMHA it is best to understand how the immune system works normally when fighting
disease and how it is deranged in the case of IMHA.
How does the body differentiate between self and foreign material?
Lymphocytes are on constant surveillance – their job is to detect and remove invaders
and abnormal cells. All lymphocytes are formed in the bone marrow, but, where they
mature determines their function. B-cells mature in the bone marrow. T-cells mature in
the thymus. The thymus is like “Boot Camp” for T-cells. The T-cells have to memorize a
list of all the proteins in the body. This list is called the Major Histocompatibility Complex
I (MCH I). If the T-cell finds a cell with something not on the list, such as an infected cell
or a cancer cell, it knows to attack it. The thymus tests each T-cell to make sure they
have memorized the list and that they will not attack normal tissues. T-cells that pass
the MHC I test are labeled with a protein called CD8+. Some T-cells have a second list,
the Major Histocompatibility Complex II (MCH II). This list has additional information
about cells that process antigens. These T-cells are labeled CD4+ and they receive
their orders from Antigen Processing Cells (APCs) in the lymph nodes. Their job is to
tell the T-cells what to attack. Any T-cell that does not pass “Boot Camp” is killed. T-
cells that pass “Boot Camp” are termed naïve T-cells or TH0 cells. Only about 2%
survive “Boot Camp”.
What tells the T-cells to attack?
These CD4+ T-Cells cells (TH0 cells) that passed “Boot Camp” are ready for battle but
do not know who the enemy is or how to fight them. The process of activation of a TH0-
cell is a two-stage process. Stage one occurs when the TH0 cells are shown who their
enemy is by an Antigen Presenting Cell (APC). This is like being shown a photo of the
enemy. Once the enemy is known the TH0 cells are then fully activated in the second
stage of the activation process. This stage results in determining the type of “soldier”
that the Boot Camp graduate will become. This second stage activation and
programming determines the branch of the armed forces, the type of soldier and the
method for killing the enemy that will be employed once he is activated.
The military analogy is that the soldier receives an enemy photo from an APC then his
“orders” that directs his future in military service. “Orders” come in the form of cytokines.
These cytokines affect the cell’s DNA and make actual transformations in the cell type.
The cell will then take on a different role and will in turn secrete different cytokines that
will allow him to perform his mission against the enemy in the photo. This mission
usually involves recruiting and directing B-Cells to produce antibodies against the
enemy. The new T-Cell will also have the ability to direct other parts of the innate
immune system through the use of newly formed cytokines that have been unlocked in
his DNA.
What stops the T-cell attack once the job is done?
Different soldier types are required because the body must defend different fronts (the
gut, the skin, mucous membranes, respiratory tract etc.) from different invaders: viruses,
fungi, worms, bacteria and cancer. In addition, once the war is over, there must be
peacekeepers (Tregs) who stop the battle and prepare the body for repair and
regeneration. For example, TH1 lymphocytes respond to interleukin 12. In response to
these chemical orders they secrete interferon and interleukin 2 which allows them to
control the less trained cells of the immune system. TH1 cells act on macrophages,
cytotoxic T cells and IgG antibody producing cells. When Tregs malfunction, we get
autoimmune disease. TH1 malfunction is the cause of Type 4 hypersensitivity, flea
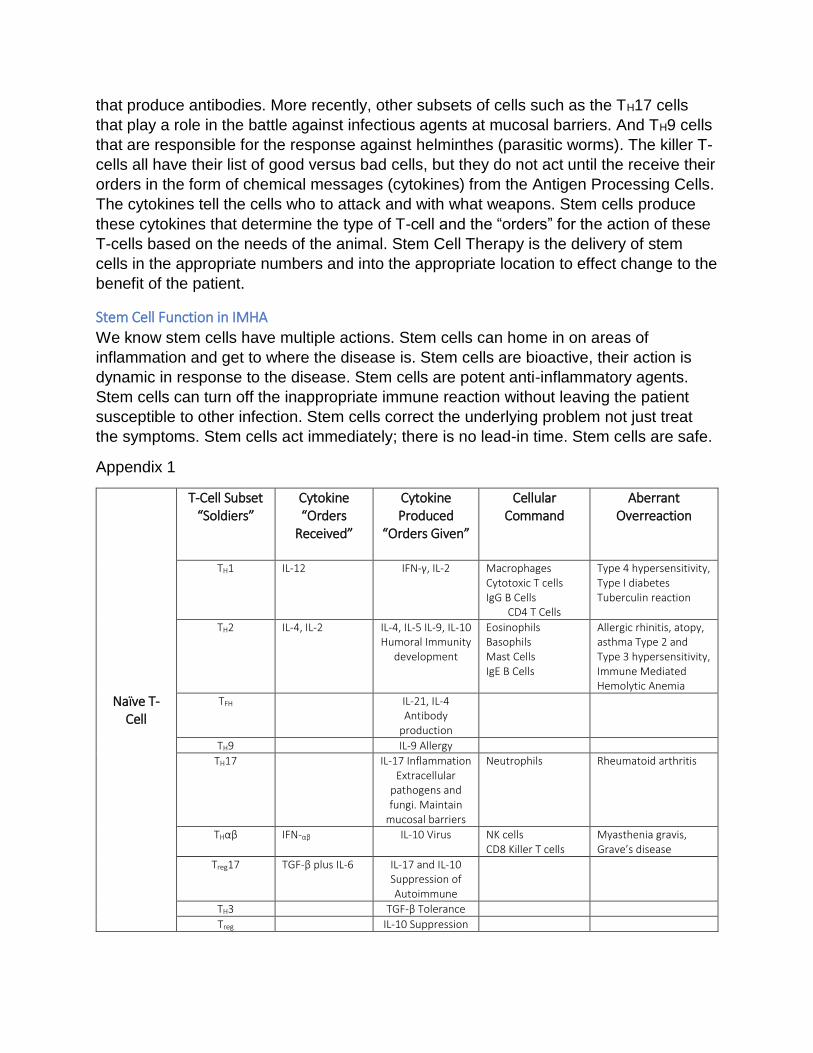
allergy in dogs and Type I diabetes. Appendix 1 shows the names of many different cell
types or soldiers, their chemical signals and the diseases that result when they
malfunction.
How do Treg Lymphocytes Control Immune Reactions?
Our newest understanding is that upon the issuance of “orders” to attack a certain
enemy, countervailing orders are also issued simultaneously to create Treg cells
directed to protect the same enemy. In addition, these Treg cells have certain
advantages over the regular army version of the T-cells. Treg cells could be considered
Seal Team 6 type cells as they are faster, multiply quicker, have a higher affinity for the
target and can outmaneuver the typical T-cell (10). They can even kill the T-cells or B-
cells if necessary. They are there to regulate the war to prevent the soldiers from going
too far in their mission. They are an essential component of the balance of the immune
system and when the immune system goes awry, they bring it back into order.
Tregs function to suppress the immune responses to beneficial microbes in the gut and
act to protect the developing fetus from harm. Tregs also have been found to protect
cancer cells from being destroyed and excessive Treg activity is being actively
researched as a method for cancer therapy.
The Role of Drug Therapy in IMHA Most of the medications used against IMHA are considered anti-metabolites. That is,
they inhibit metabolism as their mode of action. They turn off DNA synthesis, or
synthesis of one of the essential elements of DNA function or inhibit the communication
between the outer parts of the cell and the DNA. These medications do this to all cells
of the body equally without regard for the knock-on effects to other tissues they might
cause (liver damage, blood clot formation loss of immune function etc.).
Lets consider the common therapies for IMHA and IMTP, their mode of action, side
effects and the results of their use.
1. Glucocorticoids Glucocorticoids (prednisolone, prednisone, methylprednisolone and dexamethasone) bind receptors in
all cells of the body that turn off parts of the DNA (12). This results in reduced release of the chemicals
that cause cell death, reduced release of inflammatory chemicals, reduction in the the number of
receptors for antibodies which blocks cell destruction (13). The part of the DNA that processes foreign
antigens is blocked resulting in reduced immune function (14).
The side effects of glucocorticoids are well documented; steroid resistance occurs in up to 30% of
patients (15). We also see thrombosis (blood clots) (16), Gastrointestinal ulceration, liver disease, and
reduced resistance to disease. Signs of Cushing’s disease are seen with prolonged use of glucocorticoids.
The efficacy of glucocorticoids is not well documented. “To the best of our knowledge, glucocorticoids
have never been subjected to rigorous evaluation by randomized double-blinded, placebo-controlled
trials for treating canine immune-mediated disease (2)”. Glucocorticoid therapy itself carries
considerable morbidity, and treatment failure (2). Nevertheless, withholding glucocorticoids to compare
the effect of another immunosuppressive drug against placebo is cited as unethical (17). 6-month
survival from IMHA is reported to be 72% when used with azathioprine (18) (3).
2.Azathioprine Azathioprine is a T-cell inhibitor. It has an 11-day lead time which may be too long for severe or acute
cases. The side effects include bone marrow suppression (19), acute pancreatitis, hepatopathy and
gastrointestinal distress (20). There are no prospective controlled studies. A few large retrospective
studies lend limited support to its use (21) (2).
3. Cyclophosphamide (Cytoxan) Cyclophosphamide kills T-lymphocytes and regulatory T-cells. It is commonly used for cancer
chemotherapy. Side-effects include hemorrhagic cystitis and bone marrow suppression (2). Efficacy
studies show increased morbidity (makes conditions worse) Does not justify its use as an
immunosuppressive agent (2).
4. Cyclosporin (Atopica) Cyclosporin blocks T cell DNA transcription. It also blocks Interleukin 2 formation. The side-effects of
cyclosporine are gastrointestinal upsets and anorexia. Cyclosporin has good studies showing that it is
effective for atopy (22) and anal furunculosis (23). Prospective controlled studies for other conditions
are lacking (2).
5. Human Intravenous immunoglobulin Human Intravenous immunoglobulin competitively inhibits the binding of canine immunoglobulin G to
macrophages (24). It works from day 1 but only lasts 3 weeks (25).The side effects include increased
blood clotting and it increases inflammation in healthy dogs (26). Although IVIG has been used for
various conditions in dogs, efficacy data are limited to case reports and two small controlled studies.
6. Vincristine Vincristine increases platelet numbers. The main side-effect is myelosuppression in higher doses, and it
has been shown to cause abnormal platelet function in vitro (27).
7. Leflunomide Leflunomide is only available in some countries. It inhibits T and B cell proliferation. It has profound anti-
inflammatory effects. It may induce regulatory T cells (2). Leflunomide is used when pets are refractory
to glucocorticoids or the side-effects are intolerable (28). Controlled studies in the dog are confided to
renal transplantation.
8. Mycophenolate mofetil Mycophenolate mofetil blocks purine biosynthesis which blocks T cell and B cell proliferation. It may kill
activated T- cells (29). It has low toxicity and side-effects are limited to gastrointestinal effects. Is being
used for refractory myasthenia gravis, IMHA and pemphigus vulgaris (2).
9. Clodronate (LC) Clodronate is used for management of hypercalcemia from vitamin D intoxication in dogs. It kills
macrophages and dendritic cells that eat antibody tagged red blood cells. This drug is well-tolerated and
has few side effects. Controlled trials of LC are in progress at Colorado State University (CSU) for
management of IMHA in dogs (30).
10. Plasmapheresis Plasmapheresis is the partial removal of autoantibodies, immune complexes and complement
components from the blood. It can increase the chances of blood clots in the lungs. Most commonly
used for IMHA as a rescue therapy. Has some utility in this regard in dogs. Plasmapheresis has been
studied in Immune Mediated Thrombocytopenia Patients and no patients showed a response (31). As
such it is no longer recommended in humans for chronic IMHA or IMTP.
11. Splenectomy Splenectomy is the removal of the spleen as the organ most responsible for the destruction of antibody
coated red blood cells. Surgery is usually done when medical therapy has failed. Complications include
bleeding, infection, thrombosis, prolonged hospitalization, readmission to the hospital and therapeutic
failure. Results are extremely variable (32). No prospective studies available.
12. Allogenic Mesenchymal Stem Cell Therapy Allogenic mesenchymal stem cell therapy is the intravenous use of adipose derived stem cells from the
same species. In intravascular IMHA where red blood cells are destroyed by complement activation (3)
Stem cells block Complement attacks by secreting Factor H (27)(28)(29) (30). Regulatory T-cells increase
red cell tolerance (2). Lack of red cell tolerance causes IMHA. Stem Cells create Regulatory T-cells by
production of TGF-β (31). Stem Cells down regulate the production of antibodies by B-cells and down
regulate macrophage consumption of red blood cells. The stem cells’ response is modulated by the
relative need and will not affect the rest of the immune system’s ability to fight disease. Allogenic Stem
Cells are not allergenic or recognized by the immune system. They have been shown safe when given
intravenously in numerous human Phase I and Phase II Clinical Trials (33), (34), (4).
Randomized clinical trials for IMHA therapy in dogs with Stem Cells are lacking. It should be noted that
neither are there randomized controlled trials for the use of Parachutes to prevent death from
gravitational challenges. Gordon C S Smith’s article explores the need for common sense and
observation as an alternative to this method of determination of effectiveness of a therapeutic protocol.
Such is the case with stem cell therapy (35). More general research has shown that stem cells possess
anti-inflammatory and immunomodulatory properties; primarily by modulating the type and function of
T-Lymphocytes (36), (37), (38), (39), (40), (41), (42), (43), (44) (45). Unlike pharmaceutical treatments
that deliver a single agent at a specific dose, MSCs are site regulated and secrete bioactive factors and
signals at variable concentrations in response to local microenvironmental cues (4).
How do Drugs act on the Immune System to treat IMHA? The drugs listed above all interfere with DNA in some way. The reason these
medications work for IMHA is that IMHA is caused by lymphocytes and lymphocytes are
among the most rapidly dividing cells of the body. Lymphocytes use their DNA more
and are therefore, more affected by substances that damage DNA than other cells.
Tregs divide faster, have a higher metabolic rate and are more affected than other
lymphocytes by these medications (10). These medications do nothing to cure the
disease, or to stop the creation of the offending antibodies. The medications only act to
stop the manufacture of the antibodies after they have been created. In some cases,
the side-effects of the drugs are more damaging than the disease.
The Case for Stem Cells in the Treatment of IMHA Unlike these anti-metabolites, Mesenchymal Stem Cells are site regulated. Stem cells
secrete bioactive factors and signals at variable concentrations in response to local
micro-environmental cues and actually offer a cure for IMHA (4). This is another
important justification for the use of allogenic stem cells for the management of IMHA.
The importance of Regulatory T Cells in Preventing Disease
There is a large body of research demonstrating the importance of TH1 and TH2 subsets
of T-cells in preventing disease. TH1 cells produce Interferon (IFN)-γ which stimulates
cell mediated immunity against tumor cells or intracellular bacterial or viral infected
cells. In contrast TH2 cells produce many cytokines including interleukin (IL)-4, IL-5, IL-9
and IL-13 which activate B-cells allowing them to transform into the plasma cell clones
that produce antibodies. More recently, other subsets of cells such as the TH17 cells
that play a role in the battle against infectious agents at mucosal barriers. And TH9 cells
that are responsible for the response against helminthes (parasitic worms). The killer T-
cells all have their list of good versus bad cells, but they do not act until the receive their
orders in the form of chemical messages (cytokines) from the Antigen Processing Cells.
The cytokines tell the cells who to attack and with what weapons. Stem cells produce
these cytokines that determine the type of T-cell and the “orders” for the action of these
T-cells based on the needs of the animal. Stem Cell Therapy is the delivery of stem
cells in the appropriate numbers and into the appropriate location to effect change to the
benefit of the patient.
Stem Cell Function in IMHA
We know stem cells have multiple actions. Stem cells can home in on areas of
inflammation and get to where the disease is. Stem cells are bioactive, their action is
dynamic in response to the disease. Stem cells are potent anti-inflammatory agents.
Stem cells can turn off the inappropriate immune reaction without leaving the patient
susceptible to other infection. Stem cells correct the underlying problem not just treat
the symptoms. Stem cells act immediately; there is no lead-in time. Stem cells are safe.
Appendix 1
Naïve T- Cell
T-Cell Subset “Soldiers”
Cytokine “Orders
Received”
Cytokine Produced
“Orders Given”
Cellular Command
Aberrant Overreaction
TH1 IL-12 IFN-γ, IL-2 Macrophages Cytotoxic T cells IgG B Cells
CD4 T Cells
Type 4 hypersensitivity, Type I diabetes Tuberculin reaction
TH2 IL-4, IL-2 IL-4, IL-5 IL-9, IL-10 Humoral Immunity
development
Eosinophils Basophils Mast Cells IgE B Cells
Allergic rhinitis, atopy, asthma Type 2 and Type 3 hypersensitivity, Immune Mediated Hemolytic Anemia
TFH IL-21, IL-4 Antibody
production
TH9 IL-9 Allergy
TH17 IL-17 Inflammation Extracellular
pathogens and fungi. Maintain
mucosal barriers
Neutrophils Rheumatoid arthritis
THαβ IFN-αβ IL-10 Virus NK cells CD8 Killer T cells
Myasthenia gravis, Grave’s disease
Treg17 TGF-β plus IL-6 IL-17 and IL-10 Suppression of Autoimmune
TH3 TGF-β Tolerance
Treg IL-10 Suppression
References 1. Novel immunotherapies for immune-mediated haemolytic anaemia in dogs and people. James W
Swann, Oliver A Garden. London : Elsevier, October 15, 2016, The Veterinary Journal, Vol. 207, pp. 13-
19.
2. Immunomodulatory drugs and their application to the management of canine immune-mediated
disease. N. T. Whitley, M.J. Day. s.l. : British Small Animal Veterinary Association, 2011, Journal of Small
Animal Practice, Vol. 52, pp. 70-85.
3. Idiopathic Immune-Mediated Hemolytic Anemia: Treatment Outcome and Prognostic Factors in 149
Dogs. C.J. Piek, G. Junius, A. Dekker, E. Schrauwen, R.J. Slappendel, and E. Teske. Utrecht, The
Netherlands : s.n., 2008, J Vet Intern Med, Vol. 22, pp. 366-373.
4. Mesenchymal stem cells: environmentally responsive therapeutics for regenerative medicine.
Matthew B Murphy, Kathryn Moncivais and Arnold I Caplan. Austin : s.n., July 8, 2013, Experimental &
Molecular Medicine, Vol. 45, p. 54.
5. Immunoregulation by Mesenchymal Stem Cells:Biological Aspects and Clinical Applications. Marta E.
Castro-Manrreza, Juan J.Montesinos. [ed.] Marco Antonio Velasco-Vel´azquez. s.l. : Hindawi Publishing
Corporation, 2015, Journal of Immunology Research, p. 20.
6. Mesenchymal Stem Cells Inhibit Complement Activation by Secreting Factor H. Zhidan Tu, Qing
Li,Hong Bu,Feng Lin. 11, s.l. : © Mary Ann Liebert, Inc., 2010, STEM CELLS AND DEVELOPMENT, Vol. 19.
DOI: 10.1089/scd.2009.0418.
7. Mesenchymal Stem Cells Control Complement C5 Activation by Factor H in Lupus Nephritis. Haijun Ma,
Chang Liu,Bingyu Shi,Zhuoya Zhang,Ruihai Feng,Minghao Guo,Liwei Lu,Songtao Shi,Xiang Gao,Wanjun
Chen,Lingyun Sun. 32, s.l. : Elsevier, 2018, EBioMedicine, pp. 21–30.
8. Mesenchymal stromal cells and the innate immune response. Katarina Le Blanc, Lindsay C. Davies.
s.l. : Elsevier, 2015, Immunology Letters, pp. 140-146.
9. Regulatory T Cells: Differentiation and Function. Rudensky, George Plitas and Alexander Y. s.l. :
American Association for Cancer Research, 2016, Cancer Immunology Research.
10. Regulatory T Cells and Immune Tolerance. Shimon Sakaguchi, Tomoyuki Yamaguchi, Takashi
Nomura, and Masahiro Ono. Kyoto : Elseiver, 2008, Cell, Vol. 133, pp. 775-787.
11. Immunobiology of mesenchymal stem cells. S Ma, N Xie, W Li, B Yuan, Y Shi*, and Y Wang. s.l. :
Macmillan Publishers Limited, 2014, Cell Death and Differentiation, Vol. 21, pp. 216-225.
12. Glucocorticoids in T cell development. ASHWELL, J. D., LU, F. W. & VACCHIO, M. S. 2000, Annual
Review of Immunology, Vol. 18, pp. 309-345.
13. Rapid glucocorticoid effects on immune cells. BUTTGEREIT, F. & SCHEFFOLD, A. 2002.
14. DAY, M. J. & MACKIN, A. J. (2008). Immune-mediated haematological disease. In Clinical
Immunology of the Dog and Cat. 2nd. Edn. London, UK : Manson Publishing, 2008. pp. 94-121.
15. The effects of cytokines on suppression of lymphocyte proliferation by dexamethasone. CREED, T. J.,
LEE, R. W., NEWCOMB, P. V., DI MAMBRO, A. J., RAJU, M. & DAYAN, C. M. 2009, Journal of
Immunology, Vol. 183, pp. 164-171.
16. Biochemical basis for the hypercoagulable state seen in Cushing syndrome. CHASTAIN, C. B. &
PANCIERA, D. 2002, Small Animal Clinical Endocrinology, Vol. 12, p. 11.
17. Comparison of platelet count recovery with the use of vincristine and prednisolone or prednisone
alone for treatment for severe immune-mediated thrombocytopenia in dogs. ROZANSKI, E. A., CALLAN,
M. B., HUGHES, D., SANDERS, N. & GIGER, U. 2002, Journal of the American Veterinary Medical
Association, Vol. 220, pp. 477-481.
18. Evaluation of prognostic factors, survival rates, and treatment for immune-mediated haemolytic
anaemia in dogs:. WEINKLE, T. K., CENTER, S. A., RANDOLPH, J. F., WARNER, K. L., BARR, S. C. & ERB,
H.N. 2005, Journal of the American Veterinary Medical Association, Vol. 226, pp. 1869-1880.
19. Azathioprine-induced bone marrow toxicity in four dogs. RINKARDT, N. E. & KRUTH, S. A. 1996,
Canadian Veterinary Journal, pp. 612-613.
20. Thiopurine methyltransferase activity in red blood cells of dogs. KIDD, L. B., SALAVAGGIONE, O. E.,
SZUMLANSKI, C. L., MILLER, J. L., WEINSHILBOUM, R. M. & TREPANIER, L. 2004, Journal of Veterinary
Internal Medicine, Vol. 18, pp. 214-218.
21. Immune-mediated haemolytic anaemia – a retrospective study – focus on treatment and mortality.
ALLYN, M. E. & TROY, G. C. 2007, Journal of Veterinary Internal Medicine, Vol. 11, p. 131.
22. A systematic review and meta-analysis of the efficacy and safety of cyclosporin for the treatment of
atopic dermatitis in dogs. STEFFAN, J., FAVROT, C. & MUELLER, R. 2006, Veterinary Dermatology, Vol.
17, pp. 3-16.
23. Randomized controlled trial of cyclosporine for treatment of perianal fistulas in dogs. MATHEWS, K.
A. & SUKHIANI, H. R. 1997, Journal of the American, Vol. 211, pp. 1249-1253.
24. Effects of human intravenous immunoglobulin on canine monocytes and lymphocytes. REAGAN, W.
J., SCOTT-MONCRIEFF, C., CHRISTIAN, J., SNYDER, P., KELLY, K. & GLICKMAN, L. 1998, American Journal
of Veterinary Research, Vol. 59, pp. 1568-1574.
25. Therapeutic options for immune-mediated thrombocytopenia. Reid K. Nakamura, DVM, DACVECC
and Emily Tompkins, DVM and Domenico Bianco, DVM, PhD, DACVIM. 2012, Journal of Veterinary
Emergency and Critical Care, Vol. 22, pp. 59-72.
26. Prothrombotic and inflammatory effects of intravenous administration of human immunoglobulin G
in dogs. TSUCHIYA, R., AKUTSU, Y., IKEGAMI, A., SCOTT, M. A., NEO, S., ISHIKAWA, T., HISASUE, M. &
Yamada, T. 2009, Journal of Veterinary Internal Medicine, Vol. 23, pp. 1164-1169.
27. Vincristine impairs platelet aggregation in dogs with lymphoma. GRAU-BASSAS, E. R., KOCIBA, G. J.
& COUTO, G. C. Journal of Veterinary Internal Medicine, Vol. 14, pp. 81-85.
28. Treatment of Evans’ syndrome with human intravenous immunoglobulin and leflunomide in a
diabetic dog. BIANCO, D. & HARDY, R. M. 2009, Journal of the American Animal Hospital Association,
Vol. 45, pp. 147-150.
29. Mycophenolate mofetil impairs the maturation and function of murine dendritic cells. MEHLING, A.,
GRABBE, S., VOSKORT, M., SCHWARZ, T., LUGER, T. A. & BEISSERT, S. 2000, Journal of Immunology,
Vol. 165, pp. 2374-2381.
30. Innovative therapies for immune-mediated hemolysis in dogs. LUNN, K. F. Montreal, Canada. : s.n.,
2009. Proceedings of the American College of Veterinary Internal Medicine forum. Vols. June 3-6, pp.
549-551.
31. Plasma exchanges as treatment of severe acute immune thrombocytopenic purpura. Masseau A,
Guitton C, Bretonniere C, et al. 2005, Rev Med Interne, Vol. 26(10), pp. 824-826.
32. Splenectomy as adjunctive therapy for innune-mediated thrombocytopenia and hemolytic anemia in
the Dog. Feldman BF, Handagama P, Lubberink AA. 1985, J. Am. Vet. Med. Assoc., Vol. 187, pp. 617-
619.
33. Key aspects of the mesenchymal stem cells (MSCs) in tissue engineering for in vitro skeletal muscle
regeneration. Chaudhuri B, Pramanik K. 2012, Biotechnol Mol Biol Rev, Vol. 7, pp. 5-15.
34. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for
Cellular Therapy position. Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini F,Krause D et
al. 2006, Cytotherapy, Vol. 8, pp. 315-317.
35. Parachute use to prevent death and major trauma related to gravitational challenge: systematic
review of randomised controlled trials. Gordon C S Smith, Jill P Pell. 2003.
36. Human mesenchymal stem cells modulate allogeneic immune cell responses. Aggarwal S, Pittenger
MF. 2005, Transplantation, Vol. 105, pp. 1815–1822.
37. Anti-inflammatory effects of mesenchymal stem cells: novel concept for future therapies. Iyer S,
Rojas M. 2008, Expert Opin Biol Ther, Vol. 8, pp. 569-582.
38. Uccelli A, Moretta L, Pistoia V. Uccelli A, Moretta L, Pistoia V. 2008, Nat Rev Immunol, Vol. 8, pp.
726–736.
39. Stem cells and cell therapies in lung biology and lung diseases. Weiss DJ, Bertoncello I, Borok Z, Kim
C, Panoskaltsis-Mortari A,Reynolds S et al. 2011, Proc Am Thorac Soc, Vol. 8, pp. 223–272.
40. MSCs inhibit monocyte-derived DC maturation and function by selectively interfering with the
generation of immature DCs: central role of MSC-derived prostaglandin E2. Spaggiari GM, Abdelrazik H,
Becchetti F, Moretta L. 2009, Blood, Vol. 113, pp. 6576–6583.
41. Human leukocyte antigen-G5 secretion by human mesenchymal stem cells is required to suppress T
lymphocyte and natural killer function and to induce CD4þCD25highFOXP3þ regulatory T cells. Selmani Z,
Naji A, Zidi I, Favier B, Gaiffe E, Obert L et al. 2008, Stem Cells, Vol. 26, pp. 212–222.
42. Mesenchymal stem cell-mediated immunosuppression occurs via concerted action of chemokines and
nitric oxide. Ren G, Zhang L, Zhao X, Xu G, Zhang Y, Roberts AI et al. 2008, Cell Stem Cell, Vol. 2, pp.
141-150.
43. Immunomodulatory properties of mesenchymal stem cells and their therapeutic applications. Yi T,
Song SU. 2012, Arch Pharm Res, Vol. 35, pp. 213–221.
44. The chemokine system in diverse forms of macrophage activation and polarization. Mantovani A,
Sica A, Sozzani S, Allavena P, Vecchi A, Locati M. 2004, Trends Immunol, Vol. 25, pp. 677–686.
45. Mesenchymal stem cells as therapeutics. Parekkadan B, Milwid JM. 2010, Annual Review Biomed
Eng, Vol. 70, pp. 325–330.
46. Intravenous human immunoglobulin for the treatment of immune mediated haemolytic anaemia in
13 dogs. KELLERMAN, D. L. & BRUYETTE, D. S. 1997, Journal of Veterinary Internal Medicine, Vol. 11, pp.
327-332.
47. Mesenchymal Stem Cells Inhibit Complement Activation by secreting Factor H. Zhidan Tu, Z, Qing Li
,Feng Lin. [ed.] Inc. © Mary Ann Liebert. 2010, Stem Cells and Development, Vol. 19 Number 11.
48. The Complement Inhibitor Factor H Generates an Anti-Inflammatory and Tolerogenic State in
Monocyte-Derived Dendritic Cells. Rut Olivar, Ana Luque, Sonia Ca rdenas-Brito, Mar Naranjo-Go mez,
Anna M. Blom,Francesc E. Borra`s, Santiago Rodriguez de Cordoba, Peter F. Zipfel, and Josep M. Aran.
2016, The Journal of Immunology, Vol. 196, pp. 4274-4290.
49. Mesenchymal stromal cells and the innate immune response. Katarina Le Blanc, Lindsay C. Davies.
2015, Immunology Letters, Vol. 168, pp. 140-146.
50. Mesenchymal Stem Cells Control Complement C5 Activation by Factor H In Lupus Nephritis. Haijun
Ma, Chang Liu, Bingyu Shi, Zhuoya Zhang, Ruihai Feng, Minghao Guo, Liwei Lu, Songtao Shi, Xang Gao,
Wanjun Chen, Lingyun Sun. s.l. : Elsiever, 2018, EBioMedicine, Vol. 32, pp. 21-30.
51. Conversion of Peripheral CD4+CD25- Naive T Cells to CD4+CD25+ Regulatory T cells by TGF-B
Induction of Transcription Factor Foxp3. WanJun Chen, Wenwen Jin, Neil Hardegen, Ke-jian Lei, Li Li,
Nancy Marinos, George McGrady, and Sharon M. Wahl. 2003, The Journal of Experimental Medicine,
Vol. 198 Number 12, pp. 1875–1886.