Embed Size (px)
Citation preview

Critical Reviews in Oncology/Hematology 58 (2006) 231–241
Current therapies and advances in the treatment of pancreatic cancer
Andrea Mancuso 1, Fabio Calabro 1, Cora N. Sternberg ∗
Department of Medical Oncology, San Camillo and Forlanini Hospitals, Circonvallazione Gianicolense 87, Rome, Italy
Accepted 17 February 2006
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2312. Resectable disease: adjuvant therapy of pancreas cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2323. Other approaches to adjuvant therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2344. Adjuvant therapy conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2345. Locally advanced disease: chemoradiotherapy, chemotherapy alone or both? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2346. Therapy for locally advanced disease conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2367. Metastatic disease: which standard regimens? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2368. Therapy for metastatic disease conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2379. Metastatic disease: does a salvage regimen exist? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23811
A
hcetrtht©
K
fc
1
0. Salvage therapy for metastatic disease conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2381. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 238
Reviewers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 238References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 238Biographies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 240
bstract
Pancreatic cancer is a common, highly lethal disease with a rising incidence. In the last years continued efforts in pancreatic cancer researchave led to a change in the classic approaches and to the development of new biological agents that appear to show promise. Adjuvanthemotherapy with gemcitabine has recently demonstrated better survival outcomes following surgical resection compared to no treatment,specially in patients with positive margins or lymph nodes. The addition of anti-VEGF agents to adjuvant regimens could improve long-erm outcomes. In locally advanced disease, neoadjuvant regimens have not produced complete remissions, but partial responses have beeneported ranging between 10 and 20%, with conflicting survival results. Combination trials with radiochemotherapy and new drugs appear wellolerated with encouraging preliminary results. In the metastatic setting, novel chemotherapeutic combinations and molecular targeted agentsave shown promise in improving outcomes. To date, second line therapy is increasingly proposed and may even provide survival benefits inhe future. This article summarizes the current standards of therapy for patients with resectable, advanced and metastatic pancreatic cancer.
2006 Elsevier Ireland Ltd. All rights reserved.
eywords: Review; Treatments; New drugs; Pancreatic cancer
∗ Corresponding author. Tel.: +39 06 5870 4262; fax: +39 06 6630771.E-mail addresses: mancuso [email protected] (A. Mancuso),
[email protected] (F. Calabro), [email protected],[email protected] (C.N. Sternberg).1 Tel.: +39 06 5870 4356; fax: +39 06 6630771.
1. Introduction
Pancreatic cancer is the fourth leading cause of cancerdeath in the United States. 32,180 people are expected todevelop pancreatic cancer in 2005, and 31,800 people willdie from the disease [1].
The exact risk factors remain poorly understood; smok-ing is the major known etiologic factor, explaining 20–30%
040-8428/$ – see front matter © 2006 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.critrevonc.2006.02.004
232 A. Mancuso et al. / Critical Reviews in Oncology/Hematology 58 (2006) 231–241
of all cases. Germline mutations, especially mutations in theBRCA2 gene represent another 5–10% of all causes. Pan-creatitis and diabetes increase the risk of pancreatic cancer[2].Globally, long-term survival remains poor with 5-yearsurvival rates of 0.4–4% [3,4]. The only real chance forcure is surgical resection, but unfortunately only 15–20%of patients have resectable disease. The remainder haveeither locally advanced or metastatic disease at presentation.Despite radical surgery, actuarial overall survival rates forpatients with localized diseases without lymph node metas-tases are approximately 20%. Furthermore, in reality less than10% of patients with localized pancreas cancer are able toundergo a truly curative resection [5].
Up to 80% of patients present with locally advanced ormetastatic disease. Their median survivals range from 6 to9 months. For these patients, the mainstay of treatment isa combination of chemotherapy and radiation therapy orchemotherapy alone in unfit patients. This has resulted inmodest improvements in median survival and rare long-termsurvival [6].
Pancreatic cancer is one of the most intrinsically drug-resistant tumors and there is a strong need for active systemictreatments for this cancer. This article will address the useof new standard systemic therapy and combined approachesthat can overcome this drug-refractoriness and actually areproviding hope of improving clinical outcome in this disease.
2c
stfs
Cmhebrec
pf
chemotherapy. Median survival was significantly longer inthe multidisciplinary arm (20 months versus 11 months)[7]. Two subsequent randomized trials failed to confirma similar advantage for the adjuvant chemoradiation arm[8,9].
The GITSG study has been criticized for the smallnumber of patients included and for the high percentageof patients that delayed the beginning of treatment formore than 10 weeks. Moreover, it is impossible to clearlyunderstand whether the survival advantage was due to thechemoradiation, to the maintenance chemotherapy or to bothmodalities.
The ESPAC 1 trial was the first study designed and pow-ered to answer two questions regarding the role of adjuvantchemoradiation and adjuvant chemotherapy in the treatmentof resected pancreatic carcinoma.
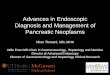
A total of 289 patients who had undergone potentiallycurative resection for pancreatic ductal adenocarcinoma in11 European countries between February 1994 and June2000 were enrolled in this study [10]. Groups of approxi-mately 70 patients were randomized to adjuvant chemother-apy, chemoradiotherapy, chemoradiotherapy and chemother-apy or surgery alone in a 2 × 2 factorial design (Fig. 1).
In 2001, 261 additional patients (ESPAC 1-plus), outsideof the 2 × 2 factorial design, were included as part of a prag-matic approach to randomization for either chemotherapyospdpn
ttaemp
odi
(ot
TR
S No.
G 43N 61E 207
C
. Resectable disease: adjuvant therapy of pancreasancer
Patients with resectable pancreatic cancer comprise amall subgroup (15–20%). Considering that the cure rate forhis patients with surgery alone is low [5] researchers haveocused on adjuvant therapies in an attempt to improve uponurvival.
Until the recent European Study Group for Pancreaticancer (ESPAC) 1 trial, studies of adjuvant therapy haveixed patients with pancreatic and periampullary cancers,
ave been underpowered to detect modest survival differ-nces from postoperative adjuvant treatment or have noteen randomized. Table 1 shows three older generationandomized trials that have evaluated the impact of postop-rative adjuvant therapy in patients with resected pancreaticancer [7–9].
In the Gastrointestinal Tumor Study Group (GITSG), 43atients, were randomized to surgery alone or to surgeryollowed by chemoradiation and subsequent maintenance
able 1esults of randomized trials in adjuvant therapy of pancreas cancer
tudy Year Arms
ITSG [5] 1985 Surgery vs. surgery + chemoXRTorwegian trial [6] 1993 Surgery vs. surgery + CHTORTC overall [7] 1999 Surgery vs. surgery + chemoXRT
HT: chemotherapy; chemoXRT: chemoradiotherapy; OS: overall survival.
r chemoradiotherapy [11]. The chemotherapy regimen con-isted of intravenous bolus 5-fluorouracil (5-FU) 425 mg/m2
lus folinic acid 20 mg/m2 and given on 5 days out of 28ays for six cycles. Median survival was 20.1 months foratients receiving chemotherapy versus 15.5 months for theo chemotherapy group (p = 0.009).
Even after stratification for margin involvement at resec-ion, lymph node involvement, tumor grade and tumor size,he survival benefit was still maintained. On the other hand,djuvant chemoradiotherapy was found to have a detrimentalffect in terms of median survival (15.9 months versus 17.9onths p = 0.05) compared to patients who did not receive
ostoperative chemoradiotherapy.Serious toxic effects (grade 3 or 4) were reported in 27%
f patients but there were only three treatment-associatedeaths, one for each treatment group. Quality of life wasmproved in all groups following surgery.
It’s important to specify the suboptimal 5-FU scheduleto be preferred in continuous infusion) and the old regimenf radiotherapy delivered in this trial (taken from the GITSGrial designed in the early 1970s) with the use of a split-course
of patients Median OS 5-Year OS
11 months vs. 20 months (p = 0.035) N/A11 months vs. 23 months (p = 0.02) 8% vs. 4%19 months vs. 24.5 months (p = NS) 22% vs. 28%

A. Mancuso et al. / Critical Reviews in Oncology/Hematology 58 (2006) 231–241 233
Fig. 1. ESPAC 1: two-by-two randomization procedure. Courtesy: Neoptolemos JP, N Engl J Med 2004;351(7):726.
technique, known to prolong the overall treatment time andreduce the rate of local control [12].
Perhaps due to the multiple concerns related to thistrial, there has not been universal abandonment of adju-vant chemoradiotherapy even if a recent meta-analysis on 30high quality adjuvant trials, including ESPAC 1-plus patients,underlines its marginal role at least after radical surgery [13].The meta-analysis performed by Stocken identified a 25%significant reduction (p = 0.001) in the risk of death withchemotherapy with median survival estimated at 19.0 monthsversus 13.5 months. The 2- and 5-year survival rates wereestimated at 38 and 19%, respectively with chemotherapyand 28 and 12% without. Chemoradiation did not reduce therisk of death with median survivals estimated at 15.8 monthswith chemoradiotherapy and 15.2 without. Subgroup analy-ses revealed that chemoradiation could have a role in patientswith positive resection margins, being more effective thanchemotherapy (decreasing of 28% the risk of death p = 0.04).
The Radiation Therapy Oncology Group (R9704) mul-ticenter randomized trial is evaluating whether gemcitabinechemotherapy administered before and following radiationwith concurrent 5-FU is superior to 5-FU given in continu-ous infusion before and after radiation therapy for patientswith completely resected tumors. This trial should help todefine the role of 5-FU chemoradiotherapy in the adjuvantsetting. Preliminary analyses are pending and awaited for2
lac[d
in the observational arm received no specific postoperativetreatment, but were followed similarly to the gemcitabinegroup. Three hundred and sixty-eight patients, with well-balanced characteristics, were included in this study.
A difference in median disease free survival (DFS)was observed for the adjuvant group (14.2 months versus7.5 months, p < 0.05). Subgroup analysis demonstrated thatincreased DFS was maintained in patients with (n = 62) orwithout (n = 294) microscopic resection margin involvementand in those with (n = 256) or without (n = 100) positivelymph nodes. Grade 3/4 toxicities were minimal with leu-copenia in less 10% of cases and thrombocytopenia in about3% of patients. Final results are expected in 2006.
Many other adjuvant trials are currently, under develop-ment. In Europe, results of ESPAC-3 including more than300 patients are awaited in 2006 [16]. This study was origi-nally designed to compare surgery alone versus surgery fol-lowed by adjuvant therapy with either gemcitabine or 5-FU,after the updated results from ESPAC-1, closed the surgery-alone arm leaving the randomization to either gemcitabine(1000 mg/m2 day 1–8–15 q 21 × 6 cycles) or 5-FU + folinicacid (Mayo Clinic regimen for six cycles). Radiation therapyis not included as a component of this trial.
EORTC trial 40013 plans to randomize 538 patients (269per treatment arm) with R0 resected pancreatic carcinoma toreceive either two courses of Gemcitabine followed by radi-ao
cvAc
006 [14].To support the role of adjuvant chemotherapy alone, a
arge randomized study to evaluate the efficacy and toxicity ofdjuvant gemcitabine in patients with resected pancreas can-er was presented at the 41th annual ASCO meeting in 200515]. Gemcitabine was administered at a dosage of 1 g/m2
ays 1, 8 and 15 every 4 weeks for 6 months. Patients (n = 177)
tion therapy concurrently with Gemcitabine or four cyclesf Gemcitabine alone [17].
Ongoing American Intergroup trials will evaluate the effi-acy and safety of incorporating novel agents targeting theascular endothelial growth factor (VEGF; bevacizumab,vastin®) or the epidermal growth factor receptor (EGFR;etuximab, Erbitux®) as well as the safety of switching to an

234 A. Mancuso et al. / Critical Reviews in Oncology/Hematology 58 (2006) 231–241
oral prodrug of 5-FU, capecitabine (Xeloda®), during con-comitant radiation therapy in the adjuvant setting.
Concomitant immunohistochemistry analyses on tissuecores will define molecular prognostic factors in orderto select patients that might benefit most from adjuvanttherapy.
3. Other approaches to adjuvant therapy
Other approaches to adjuvant therapy include moreaggressive regimens of chemoimmunotherapy administeredconcurrently with radiation therapy or studies of intra-arterialadministration of cytostatics.
Picozzi and colleagues reported results of a phase II trialin 43 patients with high-risk resected pancreatic adenocarci-noma (84% positive nodes, 19% margin positive) [18]. Pan-creaticoduodenectomy was combined with adjuvant therapywith 5-FU, cisplatin, interferon alpha and radiation therapy.Their results, after a median follow-up of 32 months, the 2-year survival rate was 64% and the 5-year survival rate was55%. The overall recurrence rate was 12%, 80% of whichoccurred within 2 years after surgery. Despite a hospitaliza-tion rate of 42%, there were no deaths from therapy.
This regimen is currently under evaluation in two multi-irGv
tracaTaats5
drie
vival difference between the two arms. This study is ongoing;some 50 patients have been recruited in 2 years, although onlyfew patients have received all of the planned treatment.
In conclusion, regional adjuvant therapy shows somepromise, but results of randomized trials must be awaitedto better define its actual role.
4. Adjuvant therapy conclusions
Postoperative adjuvant therapy appears to improve sur-vival in patients with complete resection of pancreatic ade-nocarcinoma. Chemoradiation may have a role in patientswith positive margins. The roles of chemotherapy, radiation,and newer targeted therapies against growth factor receptors,or the VEGF receptor need to be clarified by ongoing ran-domized trials.
5. Locally advanced disease: chemoradiotherapy,chemotherapy alone or both?
Locally advanced disease refers to extension of the tumorto adjacent organs such that complete surgical excision withnegative pathologic margins is impossible. Local extensionila
aatoifa[a
5yi
trw
TR
S
GGE
H py (400s
nstitutional trials (a phase II and a phase III study) conductedespectively by the American College of Surgeons Oncologyroup (ACOSOG) and by the Department of Surgery, Uni-ersity of Heidelberg, Germany.
In an attempt to maximize the dose of the chemotherapeu-ic agents and to reduce systemic effects at the same time,esearchers have focused their efforts on adjuvant regionaldministration of chemotherapy. Hans Beger and colleaguesarried out several studies of regional adjuvant chemother-py with 5-FU, mitoxantrone, folinic acid and cisplatin [19].wenty patients (18 with pancreatic ductal adenocarcinoma,nd 2 with cystadenoma) underwent this regimen via celiacxis infusion. Median survival was 21 months as comparedo 9.3 months in historical controls. In the last update of thistudy, the median survival in 24 patients was 23 months with4% 4-year survival.
On the basis of these results, the ESPAC-2 study wasesigned. This is a phase III multicenter prospective trialandomizing patients into two groups; surgery alone versusntra-arterial chemotherapy and radiotherapy. The plannednrolment is 220 patients in an attempt to reach a 2-year sur-
able 2esults of randomized trials in locally advanced pancreatic cancer
tudy Year Arms
ITSG trial [16] 1981 HDRT vs. SDRT vs. HDRT + 5-FUITSG trial II [17] 1988 ChemoXRT vs. CHTORTC trial [18] 1985 ChemoXRT vs. CHT
DRT: high dose radiotherapy (6000 cGy); SDRT: standard dose radiotheraurvival.
ncludes organs, such as the liver or duodenum, regionalymph nodes, or, most commonly, vascular structures suchs the superior mesenteric artery or the celiac trunk.
In the USA, radiation therapy and concomitant chemother-py is the mainstay of therapy for patients with locallydvanced disease. This treatment has been defined by olderrials, the GITSG trials and by the Eastern Cooperative Oncol-gy Group (ECOG) trial. These trials have yielded conflict-ng results, but a substantial benefit in overall survival inavor of chemoradiation (9.7 months) over chemotherapylone (7.4 months) has been consistently accepted (Table 2)20–22]. In these studies, continuous infusion 5-FU was useds the standard therapy to induce radiosensitization.
It is likely that oral fluoropyrimidines as an alternative to-FU may have the same effectiveness but their use cannotet be recommended in clinical practice, as phase III non-nferiority studies are still lacking [23,24].
Since publication of the GITSG and ECOG studies,here have not been other phase III studies evaluating theole of chemotherapy versus chemoradiation for patientsith locally advanced pancreatic cancer. The potential ben-
No. of patients Median OS
227 9.3 months vs. 5.3 months vs. 9.7 months (p < 0.05)43 9.7 months vs. 7.4 months (p < 0.02)50 9.0 months vs. 9.0 months
0 cGy); CHT: chemotherapy; ChemoXRT: chemoradiotherapy; OS: overall

A. Mancuso et al. / Critical Reviews in Oncology/Hematology 58 (2006) 231–241 235
efits of chemoradiation with 5-FU include local control,improved resectability (ranging between 3 and 20%), palli-ation of symptoms, and the possibility of long-term survivalin approximately 10% of patients [25].
To increase local control and resectability newerapproaches to chemoradiation for locally advanced diseasehave focused on gemcitabine and on new biologic chemora-diotherapy techniques.
Studies of hyperfractionated radiotherapy with protracted5-FU infusion have shown good local control with an accept-able toxicity profile. Data from phase III trials on overallsurvival are awaited in the near future [26].
Gemcitabine, a deoxycytidine nucleoside analogue incor-porated into DNA, is a very potent radiosensitizer and rep-resents a promising alternative to fluoropyrimidine-basedradiosensitizing regimens. The mechanism of gemcitabineradiosensitization is not completely understood, but it isthought to involve the inhibition of ribonucleotide reductase,which in turn causes cell cycle redistribution into S phaseand lowers the threshold for radiation-induced apoptosis. Ini-tial reports of gemcitabine as a radiosensitizer in pancreaticcancer appeared to reveal a significant amount of toxicityat relatively low dose levels, however, more recently com-binations of full dose weekly gemcitabine with radiotherapyappear both feasible and promising [27,28].
McGinn and colleagues from the University of Michiganhcuocd(GfwOentr
lastiea(stm2
c
formal radiotherapy is both feasible and can improve boththe response and resecability rate [30].
Pre-clinical data indicate that inhibition of the EGFRwith erlotinib (Tarceva®) or cetuximab (Erbitux®) poten-tiates the effect of gemcitabine and radiation in pancreaticcancer cell lines. A recent phase I trial and an ongoing phaseII randomized study have established the feasibility of thesecombinations. The MTD of erlotinib was 100 mg daily incombination with gemcitabine 40 mg/m2 given twice weeklyand standard RT (50.4 Gy) [31]. The PARC study is evaluat-ing the combination of cetuximab, gemcitabine and intensitymodulated radiation therapy (IMRT). The study random-izes between two different methods of cetuximab treatmentschedules (concomitant versus concomitant and sequentialcetuximab treatment). An interim analysis showed that theschedules are feasibile and have a good toxicity profile. Nodata regarding activity or patient outcome is available [32].At this time, however, any approach with gemcitabine andradiotherapy remains investigational pending the results ofongoing trials.
Other investigators have sought to develop diverseradiosensitization schedules for pancreatic cancer such as thecombination of capecitabine and bevacizumab [33]. At the41th ASCO meeting in 2005, Crane and colleagues presenteda feasibility study with this combination in 41 patients, show-ing that the addition of bevacizumab did not significantlyiwth
cTtianesroapI
riw
reaEcpr
ave reported a phase II study of concurrent full-dose gem-itabine and radiation therapy in patients with resectable ornresectable locally advanced pancreatic cancer [28]. Forty-ne patients with unresectable locally advanced pancreaticancer received concurrent gemcitabine (1000 mg/m2 onays 1, 8, and 15) and a 3-week course of radiation therapy36 Gy) using three-dimensional treatment planning [28].rade 3 gastrointestinal toxicity was noted in five patients,
atigue in 2, and unexplained death in 1. Objective responsesere seen in two patients, with one complete response.f the 12 patients deemed resectable prior to treatment,
ight were able to undergo an R0 resection (pathologicallyegative margins of resection) and two patients initiallyhought to be unresectable were able to have completeesections.
A similar experience has been conducted by Ioka and col-eagues [29]. Twelve patients were treated with gemcitabinet a dose of 1000 mg/m2 weekly for 3 weeks during RT. Thetarting RT dose was 30 Gy in 2.0 Gy fractions and escala-ion was achieved by increasing the duration in five fractionncrements, keeping the fraction size at 2.0 Gy. No patientxperienced DLT with grade 3 neutropenia in 17% of casesnd grade 2 thrombocytopenia in six patients. Six patients50%) had evidence of a local anticancer effect. Five of theseix patients (41.5%) had a complete or partial response toherapy. The median survival for the entire group was 16.5
onths. The 1- and 2-year survival rates were 58.3 and5.0%.
The results of these studies and other similar studies indi-ate that the combination of full dose gemcitabine, and con-
ncrease acute toxicity. A 22% confirmed partial responseas observed with a resecability rate of 7%. Considering
hese preliminary results, a multiinstitutional phase II studiesave been planned (RTOG PA 0411 and ACOSOG Z5041).
Another interesting approach is a chemobiologic approachombining 5-FU and TNFerade as a radiation sensitizer [34].NFerade is a replication-deficient adenovector containing
he human TNF-� gene regulated by a chemoradiation-nducible promoter, Egr-1. In a phase II trial, TNFerade wasdministered to 50 patients via an image-guided percuta-eous transabdominal approach or via an ultrasound-guidedndoscopic approach in combination with continuous infu-ion 5-FU (200 mg/m2/day × 5 days/week) and 50.4 Gy ofadiotherapy. A surprising high locoregional control rate wasbtained with median survival that had not yet been reachedt a minimum follow-up of 16 months. The dose of 4 × 1011
article units TNFerade has been proposed for a larger phaseII study.
Others agents with radiation sensitizing properties includeubitecan, cetuximab, and other growth-factor and cell-signalnhibitors. These agents are currently under investigationith results expected in 2006.Due to the conflicting results obtained in three historical
andomized trials, it is still not clear whether radiation is anssential element in the treatment of patients with locallydvanced pancreatic cancer. The current Intergroup study4201, a phase III trial comparing gemcitabine alone to gem-itabine and radiation therapy for locally advanced diseaseatients, is therefore a critical study as it will define the cur-ent role of radiation therapy for this group of patients [35].

236 A. Mancuso et al. / Critical Reviews in Oncology/Hematology 58 (2006) 231–241
The ECOG 1200 study, a randomized phase II trial, willcompare two selected chemoradiation regimens in patientswith surgically unresectable disease.
The Groupe Cooperateur Multidisciplinaire en Oncologie(GERCOR group) has performed a retrospective analysis on181 patients with pancreatic unresectable disease enrolled inprospective phases II and III GERCOR studies. Patients weredivided into two groups: in the first group subjects underwentchemotherapy with new drugs for 3 months and than receivedchemoradiotherapy (group A); in the second group patientsreceived only chemotherapy (group B) [36]. The two groupswere well balanced in terms of prognostic and biologicalcharacteristics. After 3 months of induction chemotherapy,30% of patients had disease progression and were not consid-ered eligible for chemoradiotherapy. Among the remainingpatients, 56% received chemoradiotherapy, and the remain-ing 44% continued with chemotherapy alone. The medianprogression free survival (PFS) was 10.8 months in group Aand 7.4 months in group B (p = 0.005); the median overallsurvival (OS) was 15.0 months in group A and 11.7 monthsin group B (p = 0.0009). Although hampered by the retro-spective nature of this study, there is a suggestion that, aftercontrol of disease by induction chemotherapy, chemoradio-therapy can improve survival in locally advanced pancreaticcancer as compared to chemotherapy alone.
The addition of new active agents such as bevacizumab,op2c
6
ctsa
tbhglr
7
tlc
B
the major symptoms of pancreatic cancer (weight loss andtumor-associated pain) as well as achieving a modest survivalbenefit when compared to bolus 5-FU [42].
Recent clinical trials with single-agent gemcitabine havefocused on the optimal administration of gemcitabine con-sidering that it is a prodrug and that the activating enzyme,deoxycytidine kinase, appears to be saturable. The abil-ity of deoxycytidine kinase to activate gemcitabine maybe overwhelmed by the standard dosing administration of1000 mg/m2 over 30 min and advantages in dose intensityand efficacy could be reached with longer infusion sched-ules.
In a phase II randomized trial, two different infusionschedules of gemcitabine were compared (the standard 30-min infusion or the fixed dose rate (FDR) infusion of10 mg/m2/min) in patients with pancreatic adenocarcinoma[43]. Ninety-two patients, 91% of whom had metastatic dis-ease, were enrolled into this study. Time to treatment failurewas comparable in both treatment groups, but median sur-vival for all patients was 5.0 months in the standard arm and8.0 months in the FDR arm (p = 0.013).
FDR gemcitabine has been evaluated in a phase II study incombination with cisplatin. The combination is well toleratedand appears to be an acceptable, albeit not clearly superior,alternative to other gemcitabine/platinum regimens for thetreatment of metastatic pancreatic cancer [44].
abc
p1mtwEhbobUtgi
iiaocd
eln
xaliplatin and irinotecan to an induction regimen may alsorovide better disease control (response rates ranging from7 to 38%) and perhaps also an increase in the efficacy ofhemoradiotherapy [37–39].
. Therapy for locally advanced disease conclusions
Until the results of Intergroup study E4201 are available,omparing gemcitabine alone to gemcitabine and radiationherapy, chemoradiotherapy with 5-FU must still be con-idered as the standard treatment in patients with locallydvanced disease.
Chemotherapy alone should be considered a suboptimalreatment that should be reserved for unfit patients. Dou-let chemotherapy regimens or drug triplets have not yieldedigher overall survival results in comparison to single agentemcitabine. The combined approach of chemotherapy fol-owed by chemoradiotherapy is of considerable interest, butemains investigational.
. Metastatic disease: which standard regimens?
Pancreatic cancer has traditionally been considered resis-ant to chemotherapy. Before 1996, 5-FU was the best firstine option as it had been shown superior to best supportiveare in palliative therapy trials [40,41].
An important breakthrough was the first demonstration byurris and colleagues that gemcitabine was able to improve
FDR gemcitabine is now being evaluated in phase III trialsgainst standard single-agent gemcitabine and gemcitabine-ased combinations in patients with advanced pancreaticancer.
It should be emphasized, that the 1-year survival rate ofatients treated with gemcitabine alone is not higher than8%, indicating that single agent gemcitabine is not an opti-al regimen. Several phase III randomized clinical trials have
ried to improve upon these results by combining gemcitabineith other agents (5-FU, Irinotecan, Rubitecan, Pemetrexed,xatecan and platinum salts). All of these studies, however,ave failed to demonstrate an increase in survival for the com-ination regimens over gemcitabine alone with the exceptionf the combination of gemcitabine/capecitabine publishedy Cunningham (Royal Marsden Hospital, Medicine, Sutton,nited Kingdom) (Table 3) [45,56]. Yet, additional phase III
rials are ongoing employing different 5-FU dosing strate-ies to determine whether survival could be meaningfullyncreased over single-agent gemcitabine.
The combination of oxaliplatin and gemcitabine hadnitially shown very interesting results, but ultimately nomprovement in survival [51]. The results have been encour-ging enough to warrant further investigation combiningxaliplatin with fixed-dose rate infusion gemcitabine andomparing it with standard gemcitabine alone or in a fixed-ose rate infusion (ECOG Study 6201).
Other interesting combinations explore the role of doc-taxel in combination with gemcitabine or cisplatin as firstine therapy [57]. Although encouraging, the results doot clearly exceed the ones observed in trials of gemc-

A. Mancuso et al. / Critical Reviews in Oncology/Hematology 58 (2006) 231–241 237
Table 3Results of phase III combination trials in metastatic pancreatic cancer
Author or study group Regimens No. of patients Median OS (months) p sign.
Berlin, E2297, 2002 [45] Gemcitabine vs. gemcitabine + 5-FU 162, 160 5.4, 6.7 p = 0.09Colucci, 2002 [46] Gemcitabine, gemcitabine + cisplatin 54, 53 5, 6 p = 0.43Rocha Lima, 2004 [47] Gemcitabine vs. gemcitabine + irinotecan 169, 173 6.6, 6.3 p = 0.789Richards, 2004 [48] Gemcitabine vs. gemcitabine + pemetrexed 282, 283 6.3, 6.2 NSCheverton, 2004 [49] Gemcitabine vs. exatecan 170, 169 6.5, 5.0 NSO’Reilly, 2004 [50] Gemcitabine vs. gemcitabine + exatecan 174, 175 6.2, 6.7 NSLouvet, 2005 [51] Gemcitabine vs. gemcitabine + oxaliplatin 156, 157 7.1, 9.0 p = 0.13Reni, 2005 [52] Gemcitabine vs. PEFG 46, 51 1 year OS: 38.5%; 21.3 p = 0.011Riess, 2005 [53] Gemcitabine vs. GFF 236, 230 6.2, 5.85 p = 0.68Stathopoulos, 2005 [54] Gemcitabine vs. gemcitabine + irinotecan 50, 42 1 year OS: 19.6% vs. 24%. NSHerrmann, 2005 [55] Gemcitabine vs. gemcitabine + capecitabine 159, 160 7.3, 8.4 p = 0.314Cunningham, 2005 [56] Gemcitabine vs. gemcitabine + capecitabine 266, 267 6.0, 7.4 p = 0.026
PEFG: cisplatin, epirubicin, 5-fluorouracil, gemcitabine; OS: overall survival. GFF: gemcitabine, 5-fluorouracil, folinic acid.
itabine alone (1-year overall survival ranging between 16and 30%).
In the last few years, a number of biologic agents havebeen developed to exploit specific molecular targets in thetumor cell or in the tumor microenvironment. Incorporat-ing these targeted therapies into standard treatment regimenshas yielded clinical benefits in many malignancies, includingbreast, lung, and colorectal cancers.
Some of these agents in combination with chemothera-peutic agents have been evaluated in pancreatic cancer.
After the failure of matrix metalloproteinases (proteinsthat regulate tumor invasion, metastasis, and angiogenesis)and farnesyl transferase inhibitors (proteins that prevent K-ras activation and K-ras-mediated cellular proliferation) toimprove clinical outcomes in phase III clinical trials, the inter-est in targeted therapies in pancreatic cancer has focused uponsmall molecule tyrosine kinase inhibitors [58,59].
Many features of the pancreatic malignant phenotype,such as increased proliferation, angiogenesis, and evasionof apoptosis, are associated with the signaling networks thatinvolve the epidermal growth factor receptor (EGFR). TheEGFR is detectable by immunohistochemistry in approxi-mately 90% of cases [60]. In malignant cells, members ofthe EGFR family possess an increased intrinsic tyrosine-kinase activity and inhibition of autophosphorylation andsubsequent signaling events with small molecules tyro-sac
mcwpsdaiat
Despite an increase in grades 1 and 2 rash, diarrhea andhematological toxicity in the erlotinib group, the rates ofgrades 3 and 4 toxicity were comparable in both arms. Anal-yses for EGFR expression in 170 biopsy or surgical samplesis ongoing. If the results of this combination are confirmed inother ongoing studies, this association could become a realfirst line option for these patients.
Other studies of the combination of gefitinib and gemc-itabine at fixed dose rate infusion are ongoing [62].
Two other biologic agents, specifically cetuximab(Erbitux, EGFR targeting monoclonal antibody) and beva-cizumab (Avastin, anti-VEGF monoclonal antibody) havebeen under investigation.
The Southwest Oncology Group (SWOG), on the basisof a phase II trial showing a 1-year survival rate of 32%with the combination of cetuximab and gemcitabine, has ini-tiated a phase III trial (S0205) comparing the combination ofcetuximab and gemcitabine versus single-agent gemcitabinein advanced pancreatic cancer. The results of this study shouldbecome available in 2006 [63].
Likewise, bevacizumab, approved by the FDA in 2004for the treatment of advanced colorectal cancer, has shownpromise in a phase II trial in metastatic pancreatic cancer, witha median survival of 8.8 months and 1-year survival of 29%[64]. A large phase III study (CALGB 80303) comparinggemcitabine alone versus gemcitabine and bevacizumab isa
8
csarps(t
ine kinase inhibitors (i.e. erlotinib, gefitinib) has beenn important strategy for research in metastatic pancreaticancer.
Moore and colleagues have presented at the 2005 ASCOeeting results of a phase III trial of the National Can-
er Institute of Canada Clinical Trials Group [61]. Patientsere randomized to receive Erlotinib (Tarceva, OSI-774)lus gemcitabine versus gemcitabine alone. Five hundred andixty-nine patients were enrolled in this study. A significantifference in OS (p = 0.025) was seen in the erlotinib arm withhazard ratio of 0.81 (95% CI: 0.67–0.97). The correspond-
ng 1-year survival rates were 24% versus 17%. PFS waslso significantly improved in the gemcitabine plus erlotinibreatment group with a hazard ratio of 0.76, p = 0.003.
ccruing patients to confirm these results.
. Therapy for metastatic disease conclusions
Significant advances in understanding the biology of pan-reatic cancer have been made and evidence of increasedurvival has been observed with the combination of erlotinibnd gemcitabine. Single agent gemcitabine, however, stillemains the treatment of choice in patients with metastaticancreatic cancer. In fact, two recent meta-analysis havehown only marginally significant (p = 0.05) improvement3–4%) in 1-year survival for gemcitabine-based combina-ions over gemcitabine alone. This small advantage is not

238 A. Mancuso et al. / Critical Reviews in Oncology/Hematology 58 (2006) 231–241
enough to justify broad-based change in recommendations,without further evidence from confirmatory phase III trials[65,66]. The gemcitabine FDR infusion will be studied moreextensively as are new biologic agents.
9. Metastatic disease: does a salvage regimen exist?
There is no established second-line treatment for patientswith advanced pancreatic cancer after gemcitabine failure.Single-agent second-line therapy for metastatic pancreaticcancer following gemcitabine has been associated with amedian survival of less than 5 months [67].
In view of the urgent need for second line therapy, andsince preclinical and phase I/II clinical data have suggesteda potentially synergistic activity of Oxaliplatin and 5-FU,a phase III randomized trial was designed by Oettle andcolleagues to compare this combination versus best sup-portive care (BSC) [68]. Following confirmed failure withfirst line gemcitabine, patients were randomized between acombination of oxaliplatin, 5-FU and folinic acid or BSC.After 46 out of 165 planned patients were enrolled, theBSC arm was closed because BSC alone was no longeraccepted by the participating centers. Median survival ofsecond line therapy was 21 weeks compared to 10 weeksfor the BSC group (p = 0.0077); likewise overall survivalwfjf
iw[ismsvd[
1c
sjp
1
h
carcinoma. Ongoing phase III trials will provide evidenceas to whether or not an increase in survival can really beobtained. The next few years should be characterized by newrational treatment strategies based on an increased under-standing of multiple and specific biologic pathways. Thisknowledge, coupled with our experience with chemotherapyin pancreatic cancer, will hopefully lead to improved resultsand a better understanding of the treatment and the drivingmechanisms responsible for pancreatic cancer.
Reviewers
Prof. Alberto F. Sobrero, Medical Oncology, Ospedale S.Martino, Largo Benzi 10, IT-16132 Genova, Italy.
References
[1] ACS. Cancer facts and figures 2005. American Cancer Society; 2005.[2] Lowenfels AB, Maisonneuve P. Risk factors for pancreatic cancer. J
Cell Biochem 2005:22.[3] Bramhall SR, Allum WH, Jones AG, Allwood A, Cummins C, Neop-
tolemos JP. Treatment and survival in 13,560 patients with pancreaticcancer, and incidence of the disease, in the West Midlands: an epi-demiological study. Br J Surg 1995;82(1):111–5.
[4] Sener S, Fremgen A, Menck H, Winchester D. Pancreatic cancer: areport of treatment and survival trends for 100,313 patients diagnosed
[
[
[
[
[
as 40 weeks for the investigational arm and 34.4 weeksor the BSC group (p = 0.0312). In conclusion, this studyustifies the use of salvage chemotherapy after gemcitabineailures.
Other studies have confirmed the feasibility and activ-ty (phase II non-randomized trials) of salvage treatmentsith median survivals ranging between 4.8 and 6.7 months
69–70]. Flavopiridol is a potent cyclin dependent kinasenhibitor potentiating docetaxel-induced apoptosis. It hashown promising activity as second line therapy, but resultsust be confirmed in further trials [71]. However, a phase III
tudy comparing Rubitecan, a new topoisomerase I inhibitor,ersus “best choice” in 409 pretreated patients appeared toiscourage salvage treatment with topoisomerase I inhibitors72].
0. Salvage therapy for metastatic diseaseonclusions
In good performance status patients, an oxaliplatin-basedalvage regimen after failure of first line gemcitabine appearsustified. This decision must obviously be shared with theatient, evaluating benefits and toxicity.
1. Conclusions
New biologic drug based combinations appear to offerope for the future for patients with advanced pancreatic
from 1985–1995, using the National Cancer database. J Am CollSurg 1999;189:1–7.
[5] Smeenk HG, Tran TC, Erdmann J, van Eijck CH, Jeekel J. Sur-vival after surgical management of pancreatic adenocarcinoma: doescurative and radical surgery truly exist? Langenbecks Arch Surg2005;390(2):94–103.
[6] Lockhart AC, Rothenberg ML, Berlin JD. Treatment for pancre-atic cancer: current therapy and continued progress. Gastroenterology2005;128(6):1642–54.
[7] Kalser MH, Ellenberg SS. Pancreatic cancer Adjuvant combinedradiation and chemotherapy following curative resection. Arch Surg1985;120:899–903.
[8] Bakkevold KE, Arnesjo B, Dahl O, Kambestad B. Adjuvant combi-nation chemotherapy (AMF) following radical resection of carcinomaof the pancreas and papilla of Vater—results of a controlled, prospec-tive, randomised multicentre study. Eur J Cancer 1993;29A:698–703.
[9] Klinkenbijl JH, Jeekel J, Sahmoud T, et al. Adjuvant radiotherapyand 5-fluorouracil after curative resection of cancer of the pancreasand periampullary region: phase III trial of the EORTC gastrointesti-nal tract cancer cooperative group. Ann Surg 1999;230:776–84.
10] Neoptolemos JP, Stocken DD, Friess H, et al. A randomized trial ofchemoradiotherapy and chemotherapy after resection of pancreaticcancer. N Engl J Med 2004;351(7):726.
11] Neoptolemos JP, Dunn JA, Stocken DD, et al. Adjuvant chemora-diotherapy and chemotherapy in resectable pancreatic cancer: a ran-domised controlled trial. Lancet 2001;358(9293):1576–85.
12] Morris SL, Beasley M, Leslie M, et al. Chemotherapy for pancreaticcancer. N Engl J Med 2004;350(26):2713–5.
13] Stocken DD, Buchler MW, Dervenis C, Bassi C, Jeekel H, Klinken-bijl JHG. Meta-analysis of randomised adjuvant therapy trials forpancreatic cancer. Br J Cancer 2005;91:1372–81.
14] Regine WF. Radiation therapy oncology group: phase iii randomizedstudy of adjuvant fluorouracil-based chemoradiotherapy precededand followed by fluorouracil versus gemcitabine in patients withresected adenocarcinoma of the pancreas, RTOG-9704, Clinical trialsummary from the National Cancer Institute’s PDQ® database.

A. Mancuso et al. / Critical Reviews in Oncology/Hematology 58 (2006) 231–241 239
[15] Neuhaus P, Oettle H, Post S, et al. A randomised, prospective, mul-ticenter, phase III trial of adjuvant chemotherapy with gemcitabinevs. observation in patients with resected pancreatic cancer. Proc AmSoc Clin Oncol 2005 [Abstract LBA4013].
[16] ESPAC-3(v2), Phase III adjuvant trial in pancreatic cancer comparing5FU and D-L-folinic acid vs. gemcitabine, clinical trial summaryfrom the National Cancer Institute’s PDQ® database.
[17] EORTC-40013: phase II/III randomized study of gemcitabine fol-lowed by chemoradiotherapy with gemcitabine versus gemcitabinealone after prior curative resection in patients with pancreatic headadenocarcinoma, Clinical trial summary from the National CancerInstitute’s PDQ® database.
[18] Picozzi VJ, Traverso LW. The Virginia Mason approach to localizedpancreatic cancer. Surg Oncol Clin N Am 2004.
[19] Beger H, Gansauge F, Buchler MW, Link KH. Intraarterial adjuvantchemotherapy after pancreaticoduodenectomy for pancreatic cancer:significant reduction in occurrence of liver metastasis. World J Surg1999;23:946–9.
[20] Moertel CG, Frytak S, Hahn RG, et al. Therapy of locally unre-sectable pancreatic carcinoma: a randomized comparison of highdose (6000 rads) radiation alone, moderate dose radiation (4000rads + 5-fluorouracil), and high dose radiation + 5-fluorouracil: TheGastrointestinal Tumor Study Group. Cancer 1981;48:1705–10.
[21] Anonymous. Treatment of locally unresectable carcinoma of the pan-creas: comparison of combined-modality therapy (chemotherapy plusradiotherapy) to chemotherapy alone, Gastrointestinal Tumor StudyGroup. J Natl Cancer Inst 1988;80:751–5.
[22] Klaassen DJ, MacIntyre JM, Catton GE, Engstrom PF, MoertelCG. Treatment of locally unresectable cancer of the stomach andpancreas: a randomized comparison of 5-fluorouracil alone with radi-ation plus concurrent and maintenance 5-fluorouracil—an Eastern
[
[
[
[
[
[
[
[
[
[32] Krempien R, Muenter MW, Huber PE, et al. Randomized phaseII – study evaluating EGFR targeting therapy with cetuximab incombination with radiotherapy and chemotherapy for patients withlocally advanced pancreatic cancer – PARC: study protocol. BMCCancer 2005;11:5–131 [ISRCTN56652283].
[33] Crane CH, Ellis LM, Abbruzzese JM, et al. Phase I trial of beva-cizumab (BV) with concurrent radiotherapy (RT) and capecitabine(CAP) in locally advanced pancreatic adenocarcinoma (PA). ProcAm Soc Clin Oncol 2005:4033 [Abstract].
[34] Senzer N, Hanna N, Chung T, et al. Updated response and survivaldata for TNFerade combined with chemoradiation in the treatmentof locally advanced pancreatic cancer (LAPC). Proc Am Soc ClinOncol 2005:4097 [Abstract].
[35] E4201: a randomized phase III study of gemcitabine in combina-tion with radiation therapy versus gemcitabine alone in patientswith localized, unresectable, pancreatic cancer, clinical trial sum-mary from the National Cancer Institute’s PDQ® database.
[36] Huguet F, Andre T, Hammel P, et al. Chemoradiotherapy (CRT) afterchemotherapy (CT) improves survival for locally-advanced (LA)pancreatic cancer patients: retrospective analysis of 181 patientsenrolled in prospective phases II and III GERCOR studies. ProcAm Soc Clin Oncol 2005:4095 [Abstract].
[37] Louvet C, Labianca R, Hammel P, et al. Gemcitabine in com-bination with oxaliplatin compared with gemcitabine alone inlocally advanced or metastatic pancreatic cancer: results of a GER-COR and GISCAD phase III trial. J Clin Oncol 2005;23:3509–16.
[38] Reni M, Cordio S, Milandri C, et al. Gemcitabine versus cisplatin,epirubicin, fluorouracil, and gemcitabine in advanced pancreatic can-cer: a randomised controlled multicentre phase III trial. Lancet Oncol2005;6(6):369–76.
[
[
[
[
[
[
[
[
[
Cooperative Oncology Group study. J Clin Oncol 1985;3:373–8.23] Sudo K, Yamaguchi T, Ito H, et al. Phase I study of S-1 and concur-
rent radiotherapy in patients with unresectable locally advanced pan-creatic carcinoma. Proc Am Soc Clin Oncol 2005:4187 [Abstract].
24] Vervenne WL, Bruno MJ, Gouma DJ, Phoa SS, Richel DJ, vanTien-hoven G. Short intensive chemoradiation, 50 Gy/4 weeks withtegafur/uracil, leucovorin and celecoxib for non-metastatic locallyadvanced pancreatic cancer. Proc Am Soc Clin Oncol 2005:4191.Abstract.
25] Kamthan AG, Morris JC, Dalton J, et al. Combined modality ther-apy for stage II and stage III pancreatic carcinoma. J Clin Oncol1997;15:2920–7.
26] Ikeda M, Ueno H, Okusaka T, et al. Phase II study of hyperfraction-ated radiotherapy with protracted 5-fluorouracil infusion in patientswith locally advanced pancreatic cancer. Proc Am Soc Clin Oncol2005:4111 [Abstract].
27] Blackstock AW, Bernard SA, Richards F, et al. Phase I trial oftwice-weekly gemcitabine and concurrent radiation in patients withadvanced pancreatic cancer. J Clin Oncol 1999;17:2208–12.
28] McGinn CJ, Talamonti MS, Small W, et al. A phase II trial of full-dose gemcitabine with concurrent radiation therapy in patients withresectable or unresectable non-metastatic pancreatic cancer. In: Pro-gram and abstracts of the 2004 Gastrointestinal Cancers Symposium.2004 [Abstract 96].
29] Ioka T, Tanaka S, Nakaizumi A, Nishiyama K. A phase I trial ofchemoradiation therapy with concurrent full dose gemcitabine forunresectable locally advanced pancreatic adenocarcinoma. Proc AmSoc Clin Oncol 2005:4209 [Abstract].
30] Allen AM, Zalupski MM, Robertson JM, et al. Adjuvant therapy inpancreatic cancer: phase I trial of radiation dose escalation withconcurrent full-dose gemcitabine. Int J Radiat Oncol Biol Phys2004;59(5):1461–7.
31] Kortmansky JS, O’Reilly EM, Minsky BD, et al. A phase I trialof erlotinib, gemcitabine and radiation for patients with locally-advanced, unresectable pancreatic cancer. Proc Am Soc Clin Oncol2005:4107 [Abstract].
39] Yip D, Goldstein D. Adding irinotecan to first-line gemcitabineimproves tumour response in advanced pancreatic cancer. CancerTreat Rev 2005:6.
40] Mallinson CN, Rake MO, Cocking JB, et al. Chemotherapy inpancreatic cancer: results of a controlled, prospective, randomised,multicentre trial. Br Med J 1980;281:1589–91.
41] Palmer KR, Kerr M, Knowles G, Cull A, Carter DC, Leonard RC.Chemotherapy prolongs survival in inoperable pancreatic carcinoma.Br J Surg 1994;81:882–5.
42] Burris HA, Moore MJ, Andersen J, et al. Improvements in survivaland clinical benefit with gemcitabine as first-line therapy for patientswith advanced pancreas cancer: a randomized trial. J Clin Oncol1997;15:2403–13.
43] Tempero M, Plunkett W, Ruiz Van Haperen V, et al. Random-ized phase II comparison of dose-intense gemcitabine: thirty-minuteinfusion and fixed dose rate infusion in patients with pancreatic ade-nocarcinoma. J Clin Oncol 2003;21:3402–8.
44] Ko AH, Dito E, Schillinger B, Venook AP, Bergsland EK, Tem-pero MA. Phase II study of fixed dose rate gemcitabine with cis-platin for metastatic adenocarcinoma of the pancreas. J Clin Oncol2006;24(3):379–85.
45] Berlin JD, Catalano P, Thomas JP, Kugler JW, Haller DG, Benson IIIAB. Phase III study of gemcitabine in combination with fluorouracilversus gemcitabine alone in patients with advanced pancreatic car-cinoma: Eastern Cooperative Oncology Group Trial E2297. J ClinOncol 2002;20(15):3270–5.
46] Colucci G, Giuliani F, Gebbia V, et al. Gemcitabine alone or withcisplatin for the treatment of patients with locally advanced and/ormetastatic pancreatic carcinoma: a prospective, randomized phaseIII study of the Gruppo Oncologia dell’Italia Meridionale. Cancer2002;94(4):902–10.
47] Rocha Lima CM, Green MR, Rotche R, et al. Irinotecan plus gemc-itabine results in no survival advantage compared with gemcitabinemonotherapy in patients with locally advanced or metastatic pan-creatic cancer despite increased tumor response rate. J Clin Oncol2004;22(18):3776–83.

240 A. Mancuso et al. / Critical Reviews in Oncology/Hematology 58 (2006) 231–241
[48] Richards DA, Kindler HL, Oettle H, et al. A randomized phaseIII study comparing gemcitabine + pemetrexed versus gemcitabine inpatients with locally advanced and metastatic pancreas cancer. ProcAm Soc Clin Oncol 2004;22:4007 [Abstract].
[49] Cheverton P, Friess H, Andras C, et al. Phase III results of exate-can (DX-8951f) versus gemcitabine (Gem) in chemotherapy-naıvepatients with advanced pancreatic cancer (APC). Proc Am Soc ClinOncol 2004;22:4005 [Abstract].
[50] O’Reilly EM, Abou-Alfa GK, Letourneau R, et al. A randomizedphase III trial of DX-8951f (exatecan mesylate; DX) and gemcitabine(GEM) vs. gemcitabine alone in advanced pancreatic cancer (APC).Proc Am Soc Clin Oncol 2004;22:4006 [Abstract].
[51] Louvet C, Labianca R, Hammel P, et al. Gemcitabine in combina-tion with oxaliplatin compared with gemcitabine alone in locallyadvanced or metastatic pancreatic cancer: results of a GERCORand GISCAD phase III trial. J Clin Oncol 2005;23(15):3509–16.
[52] Reni M, Cordio S, Milandri C, et al. Gemcitabine versus cisplatin,epirubicin, fluorouracil, and gemcitabine in advanced pancreatic can-cer: a randomised controlled multicentre phase III trial. Lancet Oncol2005;6(6):369–76.
[53] Riess H, Helm A, Niedergethmann M, et al. A randomised, prospec-tive, multicenter, phase III trial of gemcitabine, 5-fluorouracil (5-FU),folinic acid vs. gemcitabine alone in patients with advanced pancre-atic cancer. Proc Am Soc Clin Oncol 2005:4009 [Abstract LBA].
[54] Stathopoulos G, Aravantinos G, Syrigos K, et al. A randomizedphase III study of Irinotecan/gemcitabine combination versus gemc-itabine in patients with advanced/metastatic pancreatic cancer. ProcAm Soc Clin Oncol 2005:4106 [Abstract].
[55] Herrmann R, Bodoky G, Ruhstaller T, et al. Gemcitabine (G) pluscapecitabine (C) versus G alone in locally advanced or metastatic
[
[
[
[
[
[
[
[
[64] Kindler HL, Friberg G, Singh DA, et al. Phase II trial of bevacizumabplus gemcitabine in patients with advanced pancreatic. J Clin Oncol2005;23(31):8033–40.
[65] Liang H. Comparing gemcitabine-based combination chemotherapywith gemcitabine alone in inoperable pancreatic cancer: a meta-analysis. Proc Am Soc Clin Oncol 2005:4110 [Abstract].
[66] Banu E, Oudard S, Banu A, et al. Cumulative meta-analysis of ran-domized trials comparing gemcitabine-based chemotherapy versusgemcitabine alone in patients with advanced or metastatic pancre-atic cancer. Proc Am Soc Clin Oncol 2005:4101 [Abstract].
[67] Stehlin JS, Giovanella BC, Natelson EA, et al. A study of 9-nitrocamptothecin (RFS-2000) in patients with advanced pancreaticcancer. Int J Oncol 1999;14:821–31.
[68] Oettle H, Pelzer U, Stieler J, et al. Oxaliplatin/folinic acid/5-fluorouracil [24 h] (OFF) plus best supportive careversus best sup-portive care alone (BSC) in second-line therapy ofgemcitabine-refractory advanced pancreatic cancer (CONKO 003). Proc Am SocClin Oncol 2005:4031 [Abstract].
[69] Reni M, Bonetto E, Pasetto L, et al. Raltitrexed-eloxatin (TOMOX) salvage chemotherapy (CHT) in gemcitabine (GEM) resistantmetastatic pancreatic cancer (PC): a phase II trial. Proc Am Soc ClinOncol 2005:4115 [Abstract.
[70] Blaszkowsky LS, Kulke KH, Ryan DP, et al. A phase II studyof erlotinib in combination with capecitabine in previously treatedpatients with metastatic pancreatic cancer. Proc Am Soc Clin Oncol2005:4099 [Abstract].
[71] Rathkopf D, Fornier M, Shah MA, et al. A Phase I clinical andpharmacokinetic study of weekly docetaxel followed by flavopiridol:promising activity in metastatic pancreatic cancer. Proc Am Soc ClinOncol 2005:4096 [Abstract].
[72] Jacobs AD, Burris HA, Rivkin S, Ritch PS, Eisenberg PD, Mettinger
B
tastaMC23fii2Iragti(th
pancreatic cancer. A randomized phase III study of the Swiss Groupfor Clinical Cancer Research (SAKK) and the Central EuropeanCooperative Oncology Group (CECOG). Proc Am Soc Clin Oncol2005:4010 [Abstract LBA].
56] Cunningham D, Chau I, Stocken D, et al. Phase III randomised com-parison of gemcitabine (GEM) versus gemcitabine plus capecitabine(GEM-CAP) in patients with advanced pancreatic cancer. EJC2005;3(2):3 [Abstract].
57] Lutz MP, Cutsem EV, Wagener T, et al. Docetaxel plus gemcitabineor docetaxel plus cisplatin in advanced pancreatic carcinoma: ran-domized phase II study 40984 of the European Organisation forResearch and Treatment of Cancer Gastrointestinal Group. J ClinOncol 2005;23(36):9250–6.
58] Moore MJ, Hamm J, Dancey J, et al. Comparison of gemcitabine ver-sus the matrix metalloproteinase inhibitor BAY 12–9566 in patientswith advanced or metastatic adenocarcinoma of the pancreas: a phaseIII trial of the National Cancer Institute of Canada Clinical TrialsGroup. J Clin Oncol 2003;21(17):3296–302.
59] Van Cutsem E, van de Velde H, Karasek P, et al. Phase III trial ofgemcitabine plus tipifarnib compared with gemcitabine plus placeboin advanced pancreatic cancer. J Clin Oncol 2004;22(8):1430–8.
60] Mendelsohn J. The epidermal growth factor receptor as a target forcancer therapy. Endocrinol Relat Cancer 2001;8:3–9.
61] Moore MJ, Goldstein D, Hamm J, et al. Erlotinib plus gemcitabinecompared to gemcitabine alone in patients with advanced pancreaticcancer, a phase III trial of the National Cancer Institute of CanadaClinical Trials roup [NCIC-CTG]. Proc Am Soc Clin Oncol 2005:1[Abstract].
62] Carneiro B, Brand R, Fine E, et al. Phase I trial of fixed dose rateinfusion (FDRI) gemcitabine (GEM) with gefitinib in patients withadvanced pancreatic carcinoma. Proc Am Soc Clin Oncol 2005:4118[Abstract].
63] Xiong HQ, Rosenberg A, LoBuglio A, et al. Cetuximab, a mon-oclonal antibody targeting the epidermal growth factor receptor, incombination with gemcitabine for advanced pancreatic cancer: a mul-ticenter phase II trial. J Clin Oncol 2004;22(13):2610–6.
KL. A randomized phase III study of rubitecan (ORA) vs. best choice(BC) in 409 patients with refractory pancreatic cancer report froma North-American Multi-Center Study. Proc Am Soc Clin Oncol2004;22:4013.
iographies
Andrea Mancuso received his M.D. with honors fromhe University “La Sapienza”, Italy, in 1998. He received
fellowship in medical oncology from the same univer-ity (Oncology Certification with honors, November 1998o November 2003). His principal experience/service is asttending medical observer of the Thoracic Head and Neckedical Oncology Department of MD Anderson Cancerenter, Houston, TX, USA (November 2002 to February003). He was a grant winner as young oncologist (under5 years old) to have published during 2004 a paper asrst name in a high impact factor international oncolog-
cal journal, “Fondazione Federico Calabresi” (December004). He has been an investigator in more than 20 phase/II/II research protocols, author of 15 publications in peer-eviewed journals (original articles), and has authored 40bstracts presented during national and international con-resses. He has actively participated in Italian and Interna-ional Congresses for oral reports and/or moderations. Hes a member of the Italian North West Oncology GroupGONO) since 2001. He is a member of the Italian Associa-ion of Medical Oncology (AIOM) since 2002. Since 2003,e has been a junior member of the European Society of

A. Mancuso et al. / Critical Reviews in Oncology/Hematology 58 (2006) 231–241 241
Medical Oncology (ESMO), and a member of the Ameri-can Society of Clinical Oncology (ASCO, Associate).
Fabio Calabro obtained his M.D. in 1991 from Univer-sity of Rome “La Sapienza” (Summa Cum Laude). In 1996,he became Certified Specialist in Medical Oncology fromUniversity of Rome. He completed his Postdoctoral Train-ing from University of Rome from 1992 to 1996. He heldmany Positions and Academic Appointments in many insti-tutes of repute. He also coordinated many selected Protocolsfrom 1992 to 2004. He is associated with Italian Associationof Medical Oncology and Italian Association for Researchof Cancer (AIRC).
Cora N. Sternberg is the Chairman of the Department ofMedical Oncology at the San Camillo and Forlanini Hos-pitals in Rome, Italy, a Clinical Professor of Oncology atLa Sapienza University of Rome and is an Adjunct Clin-ical Professor in the Department of Medicine, Tufts Uni-versity School of Medicine in Boston, Massachusetts. She
is a Board Member of the EORTC, scientific chairman forGU Cancer at the ECCO 13 meeting, program chairmanfor the ASCO 2006 prostate cancer meeting, ESMO 2006GU chairman, and a faculty member of the ESU. She isthe Solid Tumor Editor of Critical Reviews in Hematologyand Oncology, an Associate Editor of the British Journal ofUrology International and is on the editorial board of inter-national journals including the Journal of Clinical Oncology,Annals of Oncology, Oncology and others. She is coor-dinating several international cooperative group trials. Dr.Sternberg is an internationally respected researcher and haspresented at >295 international cancer symposia, includingthe ASCO plenary session, AUA plenary session, ASCOeducational symposium, ECCO, ESMO and EAU meetings.Her major interests are clinical and translational research,molecular mechanisms of risk and progression of tumors,and developmental therapeutics in solid tumors. Dr. Stern-berg is also a strong advocate of patients’ rights and ofeducation.