Embed Size (px)
Citation preview

Current Status of Interventional RadiologyResearch: Results of a CIRREF Survey andImplications for Future Research StrategiesJohn H. Rundback, MD, Kenneth Wright, PhD, Gordon McLennan, MD, Elvira Lang, MD, Kevin Sullivan, MD,
Michael Bettmann, MD, Swati Bansal, MA, Wendy Landow, MPH, Nella Bloom, MA, and the Cardiovascularand Interventional Radiology Research and Education Foundation (CIRREF) Research Committee
J Vasc Interv Radiol 2003; 14:1103–1110
Abbreviation: CIRREF � Cardiovascular and Interventional Radiology Research and Education Foundation
MEDICAL research forms the founda-tion for health-care advancement andthe development of nascent therapies.The specialty of vascular and interven-tional radiology has been character-ized by a rich history of new technol-ogy development, validation, andadoption of new procedures into med-ical practice. Despite this, the level ofparticipation of practicing interven-tional radiologists in basic science andclinical research remains poorly de-fined and has lagged behind othersubspecialties as well as diagnostic ra-diology (www.search.nih.gov).
To better determine the demo-graphics of interventional radiology
research practices, a survey was com-missioned by the Cardiovascular andInterventional Radiology Researchand Education Foundation (CIRREF)and distributed to the membership ofthe Society of Interventional Radiol-ogy (neé SCVIR). The objectives of thisproject were to provide insights for thedevelopment of an intellectual foun-dation for the creation of a vascularand interventional radiology researchinfrastructure. Specifically, the surveysought to identify (i) research experi-ence and training, (ii) current researchactivity, (iii) individual and institu-tional research support, (iv) reasonsthat limit interventional radiologists’participation in or development of re-search initiatives, and (v) vascular andinterventional and radiology researchpriorities.
SURVEY INSTRUMENT
The survey was created by the re-search committee cochairs and staffwith input from research committeeand CIRREF leadership and com-prised of four main groups of ques-tions: practice demographics, researchexperience, research support, and re-search priorities. An initial draft ver-sion of the survey was piloted in April2001 to selected Society of Cardiovas-cular and Interventional Radiologycommittee members. This initial ver-sion contained additional questionsabout the survey scope and content,and feedback from these questions
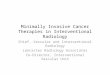
was used to modify the survey vehicleand create a final version. The finalversion (Figure) was distributed bybroadcast fax, surface mail, and e-mailto U.S. members of the Society of Car-diovascular and Interventional Radiol-ogy (now named the Society of Inter-ventional Radiology). With a Dillmanapproach (1), the survey was dissemi-nated three times (fax: May; mail:June; e-mail: July). Data were collectedand collated on an Excel spreadsheet(Microsoft, Redmond, WA) for subse-quent review and analysis. Due to thevariable number of responses to indi-vidual questions, the calculated per-centage of a given response to any par-ticular question was determined bythe response rate to that questionrather than the overall survey re-sponse. When evaluating questionsthat were tabulated by site (rather thanindividual) responses, sites that didnot provide identification and thatcould possibly represent duplicate re-sponse sites were not counted.
SURVEY RESPONSES
The overall response rate was 13%(420 of 3351), with responses receivedfrom 311 different institutions. Seven-ty-nine percent (332 of 420) respondedthat they had completed an interven-tional radiology fellowship. Practicedemographics were academic (34%),private practice (58%), government(3%), managed care (3%), and other
From the Division of Interventional Radiology, Co-lumbia-Presbyterian Medical Center, MHB 4-100,177 Fort Washington Avenue, New York, New York10032 (J.H.R.), Diagnostic Radiology, M. D. Ander-son Cancer Center, Houston, TX (K.C.W.), Depart-ment of Radiology, Indiana University Hospital, In-dianapolis, IN (G.M.), Department of Radiology,Harvard School of Medicine, Beth Israel DeaconessMedical Center, Boston, MA (E.L.), Department ofRadiology, Thomas Jefferson University Hospital,Philadelphia, PA (K.S.), Department of Radiology,Dartmouth Hitchcock Medical Center, Lebanon, NJ(M.B.), Sage Computing, Herndon, VA (S.B.), andSociety of Interventional Radiology/CIRREF, Fair-fax, VA (W.L., N.B.). Received March 3, 2003; revi-sion requested April 7; final revision received andaccepted May 8. Address correspondence to J.H.R;E-mail: [email protected]
G.M. and S.B. have identified a potential conflict ofinterest.
© SIR, 2003
DOI: 10.1097/01.RVI.0000088283.26875.58
1103

Figure. CIRREF research survey questionnaire.
1104 • Current Status of Interventional Radiology Research September 2003 JVIR

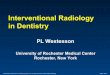
Figure. Continued.
Rundback et al • 1105Volume 14 Number 9

(1%). Just more than two-thirds weresingle specialty.
Research Training and Experience
Forty-three percent of respondents(182 of 420) have had formal trainingin research methodology. This in-cluded specific training or didactics inbiostatistics (30% of overall respon-dents), experimental design (31%),data collection and management(25%), literature synthesis and review(24%), grant writing (19%), and regu-latory issues related to research (15%).
Fifty-eight percent have partici-pated in either basic science (n � 91,22%) or clinical research trials (n �230, 55%), whereas 24% have not (n �
99). Nineteen percent have partici-pated in both clinical and basic scienceinvestigations. Only 3% have per-formed basic science research only.For those with research experience,the mean and median numbers of clin-ical trials participated in were sevenand four, respectively, with 83 (35%)having been involved with one to twotrials, 78 (33%) with three to five trials,and 76 (31%) with more than five tri-als. With regard to basic science re-search, 37 (37% of 102 responses to thisquestion) have been involved with oneto two trials, 35 (35%) with three tofive, and 30 (30%) in more than five,with a median of four basic scienceprojects.
To assess the role of interventional
radiologists as lead investigators,questions were asked regarding ex-perience with protocol authorship,U.S. Food and Drug Administration(FDA)–sponsor investigations andfunding record. Fifty-four percent (n� 225) have authored research proto-cols, with an average of four protocolswritten by these individuals. Sixteenpercent (n � 67) have been FDA–spon-sored investigators by securing inves-tigator device exemption or investiga-tional new drug status for theirresearch.
Funding Record
Thirty-two percent (130 of 413)have applied for extramural funding.
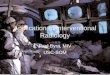
Figure. Continued.
1106 • Current Status of Interventional Radiology Research September 2003 JVIR

Of these, 95% of responders from aca-demic practices have sought extramu-ral funding compared with 43% ofphysicians from private practices.However, the timing of fundingwithin the individuals’ career was notassessed, and it is thus not clearwhether this reflects activity at thecurrent job position or funding se-cured during prior employment (eg,physicians who made the transitionfrom academic to private practices).The source of funding is shown in Ta-ble 1. The greatest amount of researchfunding was from industry, with 76(18%) of responding interventional ra-diologists having sought and 15% hav-ing obtained industry support for re-search (an 86% funding success; 281funded projects). According to the sur-vey results, CIRREF has awardedgrants for 18 projects by 15 interven-tional radiologists (not all CIRREFgrants are accounted for in the surveyresults). Federal research funding hasbeen pursued for 132 projects by 50interventional radiologists (12% of to-tal survey response and 38% of thosewith research grant experience), withsuccessful funding in 47% of projectsand 44% of applicants.
Research Activity
Forty-one percent (172 of 420) re-sponding interventional radiologistsare actively participating in clinical orbasic science research. Overall, an av-erage of 6% of work time was spentperforming or supervising research(mean: 13.5% of academic time; 1.7%of private practice time). Eight percent(32 of 420) reported 20% or more of
their work time to be dedicated to re-search activities. Forty-four percent(141 of 420) are currently involved inthe training of residents or fellows.Of responding institutions, 37% (115programs) and 40% (124 programs)provide residency and fellowshiptraining, respectively. Fellowship pro-grams described an average of 8% ofthe fellow’s time being spent doingresearch; 13 programs (4%) reported atleast 20% of the fellow’s time to bespent on research.
Research Resources and Limitations
Ninety-three responding institu-tions (23%) have a clinical research co-ordinator or other dedicated researchstaff: clinical nurse specialists were themost common research staff em-ployed, reported at 60 institutions,compared with 23 institutions havingnurse practitioners, 22 with physicianassistants, and nine with research fel-lows. Eleven sites reported having adedicated clinical research coordina-tor, although the overlap of the re-sponsibilities served by this positionversus other research staff was notclearly delineated.
Available research facilities in-cluded a research-dedicated angiogra-phy suite at 54 institutions (17%), mag-netic resonance (MR) imaging in 34(11%), computed tomography (CT) in12 (4%), laboratory space in 60 (19%),animal facilities in 86 (28%), and vet-erinary assistance in 65 (21%). An ad-ditional 141 (45%), 185 (59%), and 190(61%) reported research access to aclinical unit angiography laboratory,MR imaging, and CT, respectively.
When queried as to the major limi-tations to conducting research, the fol-lowing responses were obtained: time(87%), lack of support staff (58%), fa-cilities (25%), interest (28%), and lowpatient volume (15%). With regard tothe perceived institutional climate forconducting research, 45% reportedthat their practice environment was ei-ther highly or somewhat supportive ofresearch activities, whereas 44% re-ported indifference and 10% reportedthe environment to be not supportive.
Respondents were asked whetherthey or their institutions would be in-terested in participating in a clinicalresearch trial if that trial was alreadyprepared and funded. Eighty-threepercent stated that they would partic-ipate in funded clinical trials (95% foracademic practices, 75% for privatepractices).
Research Interests and Priorities
Research priorities were queried byglobal groups representing potentialresearch project areas or procedures,as well as by subcategories withinthese groups. Perceived research pri-orities are shown in Table 2.
Table 1Sources of Vascular Interventional Radiology Research Funding Based onResponses to Question 6 of Survey (Fig)
Source
Number ofIndividuals
Applied
Number ofIndividuals
Funded %
Numberof
ProjectsApplied
for
Numberof
ProjectsFunded %
Industry 76 66 86 328 281 85Radiology 24 14 58 32 20 62CIRREF 26 15 57 31 18 58Private 36 21 58 61 35 57Federal 50 22 44 132 63 47National 26 13 50 41 17 41Other 13 8 61 24 14 58
Table 2Research Priorities (Lowest toHighest)
Topic
Numberof
Responses
TIPS 5Veins 7Biomaterials 7Cardiovascular imaging 19Spine interventions 19Research methods 21Thrombolysis 22Hemodialysis/venous access 27Miscellaneous 30New technologies 34Aneurysm therapies 44Gene therapies 63Uterine fibroid embolization 69Peripheral vascular disease 71Restenosis 98Neurovascular interventions 111Cancer therapies 179
TIPS � transjugular intrahepaticportosystemic shunt.
Rundback et al • 1107Volume 14 Number 9

LESSONS LEARNED: HOW CANWE SECURE THE FUTURE OFINTERVENTIONAL RADIOLOGYRESEARCH?
The history of interventional radiol-ogy is replete with innovation andtechnology that have enhanced thepractice and understanding of medi-cine. The conceptualization, investiga-tion, and development of techniquessuch as peripheral angioplasty (2,3),transjugular intrahepatic portosys-temic shunts (4), uterine fibroid em-bolization (5,6), and regional cancertherapy (7,8), all by interventional ra-diologists, have forever changed andcontinue to challenge the health-carelandscape. Despite these contribu-tions, emerging and confluent trendsin the global medical environmentthreaten to marginalize the future po-tential of interventional radiologists asbrokers of procedural innovation andtranslational research (Table 3). In-creasing interest by other subspecial-ists in areas of research traditionallysubsumed by interventional radiologyis producing strong competition forindustry support and extramural re-search funding (9), and few interven-tional radiologists have the training,time, and resources necessary to effec-tively compete for research dollars. Ofthe $6.8 billion budgeted to the Na-tional Institutes of Health (NIH) in2000, allocations to interventional ra-diology principal investigators ac-counted for small amounts compared
with awards for cardiology, nephrol-ogy, and vascular surgery. Further-more, organized interventional radiol-ogy has failed to inculcate a “cultureof research” (ie, less than one-half ofresponding institutions support re-search). An insufficient number of in-terventional radiologists have trainingin or familiarity with the conduct ofprospective, randomized, controlledtrials, health-care impact assessment,and evidence-based outcome researchnecessary to support and preserve ourtechniques, and even fewer have expe-rience with evolving transformativetechnologies such as genetics, robotics,and nanotechnology. This further re-sults in an insufficient number of ex-perienced mentors able to providegrant support, an important consider-ation in NIH evaluation of a grantsubmission.
In a 1998 commentary in Radiology(10), Dr. Krishna Kandarpa wrote “Wecan seldom control the motives andbehavior of competitors, nor shouldwe waste our time doing so. We can,however, take steps to ensure our ownsecure future.” Furthermore, interven-tional radiology researchers must de-velop initiatives independent of thosesupported by industry, who in the fu-ture may no longer see interventionalradiologists as the primary purveyorsof new technology, and increasinglyuse principal investigators from otherdisciplines to oversee clinical trials. Infact, since Dr. Kandarpa’s cogent com-mentary, organized radiology and in-terventional radiology have takensteps to enhance the research activitiesof its members. The CIRREF “IA 2000”campaign successfully secured $5 mil-lion for investigator-initiated inter-ventional radiology research grants.CIRREF has to date sponsored morethan a dozen pilot research grants, theuterine fibroids outcome registry andfibroid quality of life instrument, theRAND fibroid research agenda pro-gram, a skin-entry dose study for in-terventional radiologists, and severalresearch-focused symposia. Through a$23-million grant from the NationalCancer Institute, the American Collegeof Radiology Imaging Network (11,12)has funded interventional radiologist–initiated projects on hepatic chemoem-bolization and radiofrequency abla-tion, with several additional projectsin the pipeline. These are great firststeps. However, the plethora of neces-
sary scientific investigations remainsunfulfilled by these limited resources,and competition by providers, institu-tions, and alternative technologiesthreaten to dilute patient enrollmentin these trials. Furthermore, investiga-tors participating in pilot research of-ten do not publish their results, a nec-essary precursor to obtaining largerfunding. Of the more than 25 individ-uals awarded CIRREF pilot grants, forexample, only 10 have resulted in sci-entific publications (mostly within theinterventional radiology literature)and only a few have gone on to pro-cure federal grant support for addi-tional research.
How then can the results of thissurvey be used to expand vascular in-terventional radiology research in thisnew millennium? In fact, the resultspublished herein help to identifystrengths and weaknesses in the inter-ventional radiology community thataffect global strategies for research de-velopment. The data base created fromthe survey represents a unique colla-tion of members’ current research ex-pertise and interests, providing apowerful resource for infrastructuredevelopment. Specifically, the datacaptured—institutional procedure vol-ume, level of investigator training inresearch methodology, experience inbasic and clinical trials, extramuralfunding record, and resources—pro-vide the backbone for the identi-fication of sites, investigators, andmentors suitable for participation inmulticenter clinical trials. In addition,this information can be used to facili-tate the creation of expert teams(“think tanks”) capable of identifyingresearch priorities within project areasand for developing specific protocolsto address this research agenda.Teams can be created that consist ofexperience mentors, active sites, andgrant writers and reviewers to en-hance the likelihood of successful ex-tramural funding. Finally, site and in-vestigator data can be freely suppliedto industry representatives to assist inthe selection of interventional radiol-ogy investigators for relevant clinicaltrials.
The results of this survey representa snapshot of the current researchclimate, and when compared with thepractice distribution of all Society ofInterventional Radiology members,there is a threefold response bias
Table 3Factors Affecting the Future of VIRResearch
ExternalInterest by other subspecialists in
traditional areas of VIR researchIncreased competition for extramural
research fundingLack of interventional radiologists on
NIH study sectionsInternal
Lack of formal research trainingLimited departmental financial
resources for VIR researchTime constraintsGroup structureInadequate support staffPoor facilities and administration
VIR � vascular interventionalradiology.
1108 • Current Status of Interventional Radiology Research September 2003 JVIR

from academic groups comparedwith private practices. Although in-ternal Society of Interventional Radiol-ogy socioeconomic data have shown ademographic of 13% of interventionalradiologists in academic groups and79% in private groups, the survey re-sponders were academic in 34% andprivate practice affiliated in 58%. Inaddition, the limited response likelyrepresents a bias toward interven-tional radiologists interested in re-search. These biases are reflected inthe unexpectedly high grant successrates seen in Table 1, particularly forfederal funding, in which successfulNIH support occurs in approximately15%–20% of applications and isstrongly affected by the prior grantexperience of the applicant.
Despite its deficiencies, this surveysuggests that several organizationalstrategies may be valuable in nurtur-ing interventional radiology research.Less than half of the respondentsclaimed to have formal training in re-search methodology, suggesting thatthe development of a research educa-tion curriculum as part of interven-tional radiology training may increaseinvestigator development. Depart-mental and vascular interventional ra-diology financial and time limitationscontinue to represent a major con-straint for research activities. The So-ciety of Interventional Radiology andAmerican College of Radiology needto continue to pursue initiatives to en-hance support and time for researchamong interventional radiology fac-ulty. Most interventional radiologistsalso lack the necessary fundamentalsupport, ie, grant writers, biostatisti-cians, and research personnel, to allowsuccessful participation in research ac-tivities. Despite this, most interven-tionalists would willingly participatein clinical trials that were already de-veloped and funded. It is incumbenton the Society of Interventional Radi-ology and the CIRREF to actively de-velop centralized programs for pre-submission grant review assistance aswell as the independent internal de-velopment of strategically importantprotocols that can then be distributedto interested investigators. This latterprogram is currently being developedas part of the recently created CIRREFstrategic initiative and can providecritical infrastructure for the future
creation of multicenter trials within in-terventional radiology.
Despite the bias toward academicpractitioners, it is encouraging to notethat a large number (43%) of respond-ing physicians reported formal train-ing in at least one area of research,with approximately one-third havingeducation in biostatistics and studydesign, one-fourth having been edu-cated in data analysis, and one-fifthexposed to grant writing courses. Nev-ertheless, research education and in-vestigator development should remainorganizational priorities to ensure aviable future pool of experienced sci-entists. Creative use of the time avail-able during residency and interven-tional radiology fellowship could bethe foundation for training radiolo-gists to be clinician scientists. Currenttraining options include The HolmanPathway (http://www.theabr.org/1_Ex41_Holman.html), which includesup to 24 months of research time dur-ing radiology residency, a dedicatedinterventional radiology pathway thatincludes 6 months of research anddedicated clinical training to becomean effective interventional radiologist,and incorporating as much as 12months of research into the 48 monthsof radiology residency training. Thelast option requires the most commit-ment on the part of residency pro-grams but offers the option to tailorthe research experience to each resi-dent. One of the most important obsta-cles to any of these programs is thetraditional role of the radiology resi-dent in residency programs. Most ra-diology residencies focus the schedul-ing of radiology resident rotationsbased on clinical service needs of thepractice that supervises the residents.This has resulted in a culture of hos-tility toward research time and insuf-ficient guidance and planning of “re-search electives.” If radiology is tobecome a center of academic researchactivity, then the approach to researchtime must change. This will requireexcellent mentors and a large amountof planning of research electives. Infact, research time in residency shouldnot be elective. It should be time that isassigned for specific activities that theradiology faculty has planned for theresidents, and time doing researchshould be critiqued with as muchvigor as their ability to read chest x-rays or an MR imaging of the shoul-
der. If radiologists plan to incorporateresearch into their residencies and arewilling to support their residents’ re-search activities, it is possible that wecould build a cadre of individuals whohave enough preliminary data by thethird year of their residency to applyfor funding for research fellowshipsfrom societies like the Radiological So-ciety of North America and the Amer-ican Heart Association. If we are ableto successfully secure these fellow-ships for our research-oriented resi-dents, we will ensure them 2-year fel-lowships with good salaries and willsupply them with dedicated time andsupport during their fellowship togenerate enough preliminary data fortheir first mentored training award(K-08 or K-23) or R-21 grant from theNIH as first- or second-year faculty intheir first job. This is the pipeline forproductive research that already existsin surgery and internal medicineprograms.
Future organizational efforts mustmaintain the objective of creating pro-grams and clinical research networksaccessible to and serving the majorityof practicing interventional radiolo-gists. As market forces continue todynamically change the structure andfocus of interventional radiology prac-tices and as individuals change jobs,periodic updates of data obtained bythis survey will be necessary. Thus,repeated polling of members will becritical to ensure longitudinal accuracyand completeness and to enable max-imal representation of all interven-tional radiology practices and researchinterests. Only in this way can partic-ipation in future research trials be dis-seminated to a maximal number ofsites and types of practices, reducingsite selection bias and expanding theopportunity for new investigators inall clinical environments to become ac-tive in the research process. Smallerpractices with significant proceduralvolumes can then have equal access toclinical trials.
APPENDIX: CIRREFRESEARCH COMMITTEEMEMBERS
John H. Rundback, MD, Cochair,Columbia Presbyterian Medical Cen-ter Milstein Pavilion, Vascular and In-terventional Radiology, New York,NY
Rundback et al • 1109Volume 14 Number 9

Kenneth C. Wright, PhD, Cochair,Diagnostic Radiology, M.D. AndersonCancer Center, Houston, TX
Kamran Ahrar, MD, Department ofRadiology, M.D. Anderson CancerCenter, Houston, TX
Curtis W. Bakal, MD, MPH, Ex-officio, Department of Radiology, St.Luke’s–Roosevelt Hospital Center,New York, NY
Michael A. Bettmann, MD, Dart-mouth Hitchcock Medical Center, Leb-anon, NH
John F. Cardella, MD, SUNY Syra-cuse Health Science Center, Syracuse,NY
Joseph Bonn, MD, CIRREF ViceChair, Department of Radiology,Thomas Jefferson University MedicalCenter, Philadelphia, PA
Patricia E. Cole, PhD, MD, Novar-tis Corporation, East Hanover, NJ
Paul M. Consigny, PhD, GuidantVascular Intervention, Santa Clara,CA
William C. Culp, MD, Vascularand Interventional Radiology, Univer-sity of Arkansas for Medical Sciences,Little Rock, AR
James R. Duncan, MD, PhD,Mallinckrodt Institute of Radiology,St. Louis, MO
Robert Donald G. Ferguson, MD,Department of Radiology, ForsythMedical Center, Winston-Salem, NC
Jeff H. Geschwind, MD, Depart-ment of Radiology, Johns HopkinsMedical Institute, Baltimore, MD
Antoinette S. Gomes, MD, Depart-ment of Radiological Sciences, UCLAMedical Center, Los Angeles, CA
Richard J. Gray, MD, Departmentof Radiology, Washington HospitalCenter, Washington, DC
Matthew S. Johnson, MD, Depart-ment of Radiology, Indiana UniversityHospital, Indianapolis, IN
Krishna Kandarpa, MD, PhD,CIRREF Past Chair, Division of Radi-ology, University of MassachusettsMemorial Medical Center/UniversityCampus, North Worcester, MA
Elvira V. Lang, MD, HarvardSchool of Medicine, Beth Israel Dea-coness Medical Center, Boston, MA
Matthew A. Mauro, MD, CIRREFChair, Department of Radiology, Uni-versity of North Carolina Hospitals,Chapel Hill, NC
Gordon McLennan, MD, Depart-ment of Radiology, Indiana UniversityHospital, Indianapolis, IN
Franklin J. Miller, Jr., MD, Depart-ment of Radiology, UCSD MedicalCenter, San Diego, CA
Sanjay Misra, MD, Mayo Clinicand Foundation, Rochester, MN
Kevin L. Sullivan, MD, Depart-ment of Radiology (CVIR), ThomasJefferson University Hospital, Phila-delphia, PA
Karim Valji, MD, Ex-officio, De-partment of Radiology, UCSD MedicalCenter, San Diego, CA
References1. Dillman DA. Mail and telephone sur-
veys: the total design method. NewYork: Wiley-Interscience, 1978.
2. Dotter CT, Judkins MP. Transluminaltreatment of arterio-sclerotic obstruc-tion: description of a new technic and a
preliminary report of its application.Circulation 1964; 30:654–670.
3. Seldinger SI. Catheter replacement ofthe needle in percutaneous arteriogra-phy. Acta Radiol 1953; 39:368–376.
4. Rosch J, Hanafee W, Snow H, BarenfusM, Gray R. Transjugular intrahepaticportacaval shunt. An experimentalwork. Am J Surg 1971; 121:588–592.
5. Ravina JH, Herbreteau D, Ciraru-Vign-eron N, Bouret JM, Houdart E, AymardA, et al. Arterial embolisation to treatuterine myomata. Lancet 1995; 346:671–672.
6. Goodwin SC, Vedantham S, McLucasB, Forno AE, Perrella R. Preliminaryexperience with uterine artery emboli-zation for uterine fibroids. J Vasc IntervRadiol 1997; 8:517–526.
7. Wallace S, Charnsangavej C, CarrascoCH, Bechtel W. Infusion-emboliza-tion. Cancer 1984; 54(suppl 11):2751–2765.
8. McGahan JP, Browning PD, Brock JM,Tesluk H. Hepatic ablation using ra-diofrequency electrocautery. Invest Ra-diol 1990; 25:267–270.
9. Vogelzang RL. Future directions invascular and interventional radiologyresearch. Radiology 1998; 209:17–18.
10. Kandarpa K. Future directions invascular and interventional radiologyresearch: a commentary. Radiology1998; 209:19–21.
11. Hillman BJ. The American College ofRadiology Imaging Network (ACRIN):research educational opportunities foracademic radiology. Acad Radiol 2002;9:561–562.
12. Hillman BJ. Opportunities for re-search with the American College ofRadiology Imaging Network (ACRIN)image database. Acad Radiol 2002;9:996–997.
1110 • Current Status of Interventional Radiology Research September 2003 JVIR