Embed Size (px)
Citation preview
Knee Injuries in the Skeletally
Immature Adolescent Athlete: Current Questions and Challenges
Corey Dean MD Internal Medicine-Pediatrics, CAQ Sports Medicine

Mascots….

Mascots….
Objectives
1. Discuss the most common cause of adolescent knee pain,
ways to treat this without referral and when to allow the
athlete to return to play.
2. Discuss the various apophysitis/tendonitis injuries
associated with the skeletally immature knee.
3. Discuss the anterior cruciate ligament (ACL) epidemic
in young women, treatment controversies, and ways to
prevent them.
4. Discuss the one knee injury you do not want to miss and
why referral early is so crucial.
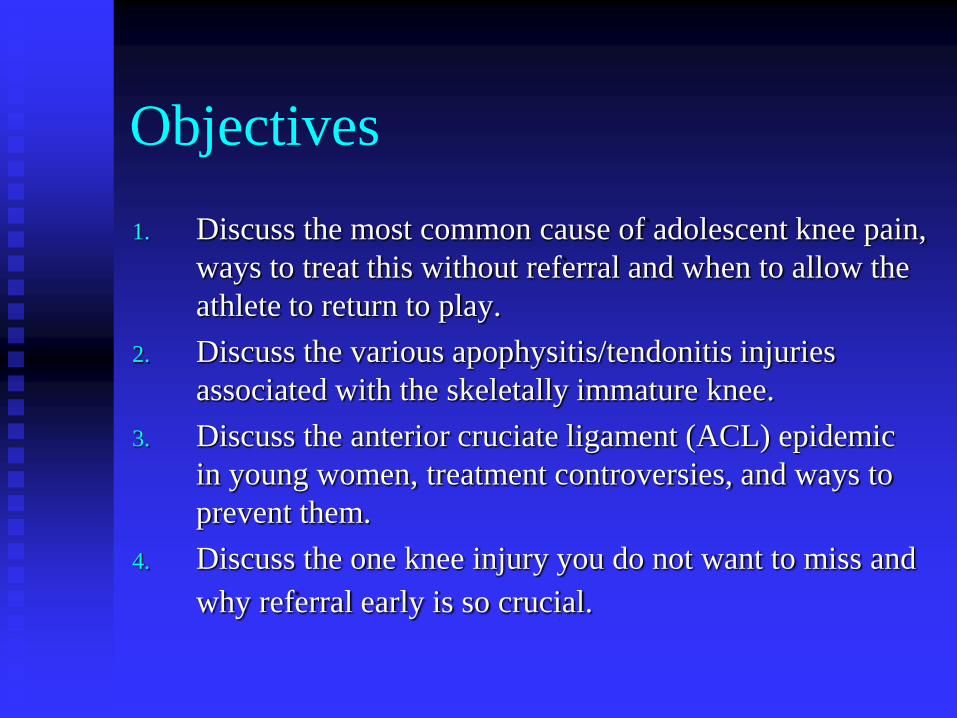
Anatomy of the knee-3
compartments The Knee is broken
down into 3
compartments:
1. Patellofemoral
(including bursa)
2. Ligamentous
3. Meniscal
Case 1
An 17-year-old cross country runner c/o anterior knee pain for 6 weeks.
Provoked by walking up and down stairs and sitting in class.
No history of locking, catching, swelling, or instability.
On physical exam, Mild tenderness over the medial aspect of the patella. Quadriceps tone was poor over vastus medialis. + Patellar inhibition testing (subluxation tenderness).
Patellofemoral knee physical
exam
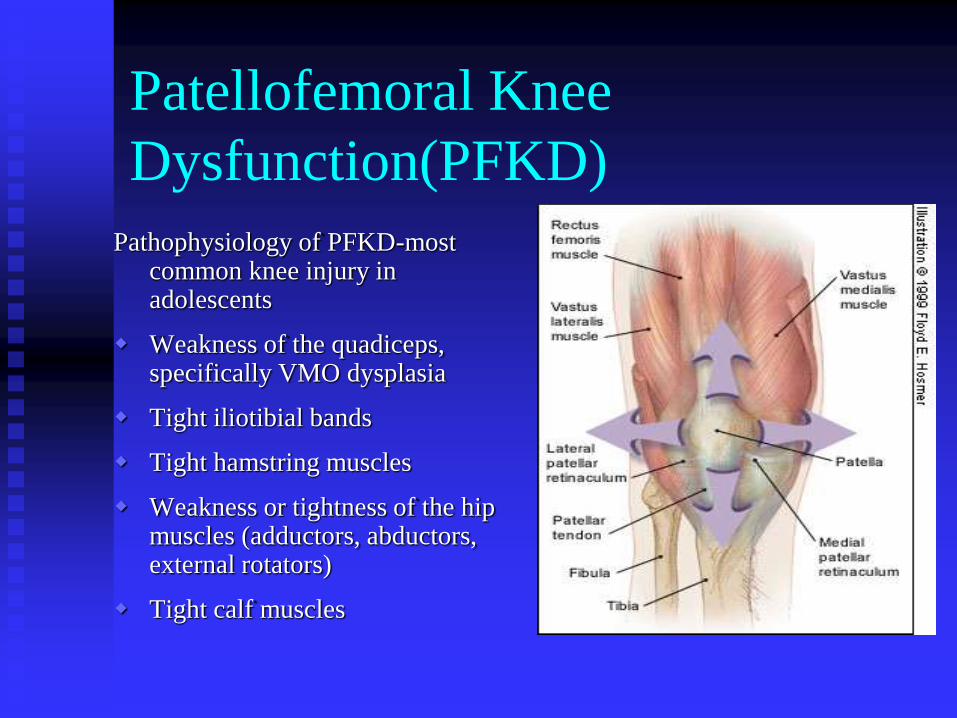
Patellofemoral Knee
Dysfunction(PFKD)
Pathophysiology of PFKD-most common knee injury in adolescents
Weakness of the quadiceps, specifically VMO dysplasia
Tight iliotibial bands
Tight hamstring muscles
Weakness or tightness of the hip muscles (adductors, abductors, external rotators)
Tight calf muscles
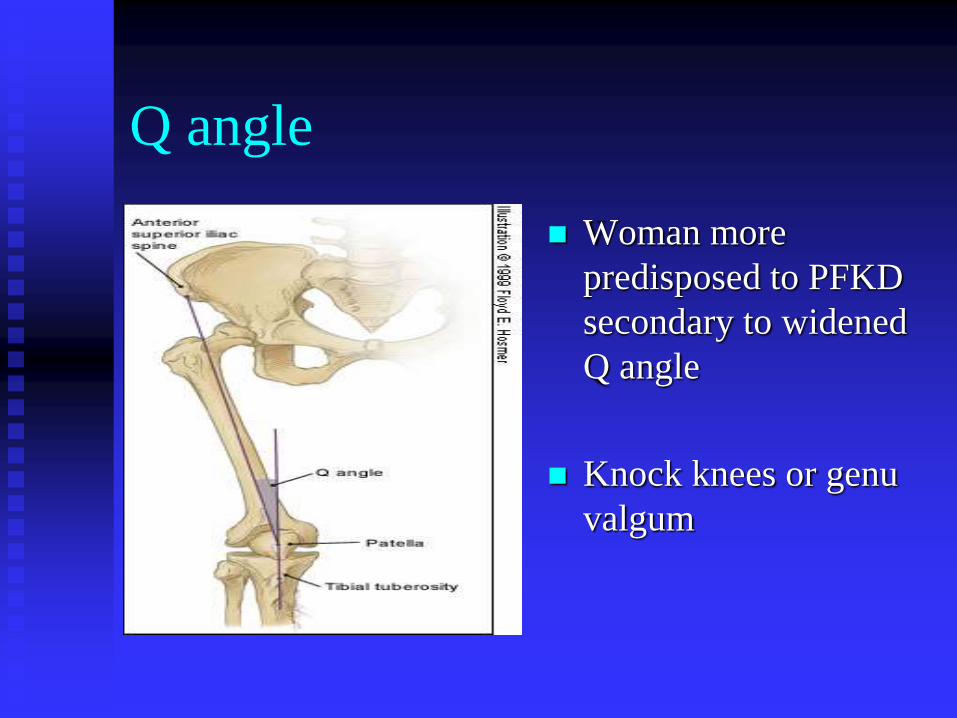
Q angle
Woman more
predisposed to PFKD
secondary to widened
Q angle
Knock knees or genu
valgum
PFKD
Diagnostic Testing:
1. No testing is needed-
clinical diagnosis
2. X-rays-usually
normal. Rare cases of
severe PFKD leading
to arthritic changes.
PFKD-Treatment
- Running was reduced (preferably on grass or on a treadmill).
- Keep the athlete in the game-Swimming as cross training.
- Ice massage was recommended three to four times daily over patellofemoral complex.
- Open and closed-chain exercises with an emphasis on the vastus medialis obliques strengthening.
- A lower-extremity flexibility program was also started, focusing on the hamstrings/quadriceps.
- Use of NSAIDs as needed.
PFKD-Return to play
-90/90 rule (90% range of
motion and 90% strength in
comparison to the unaffected
side)
-10% rule - Graded progression
in return to athletic competition
in using “pain as your guide” to
increase mileage of running (by
10% per week). If pain recurs,
then plateau running.
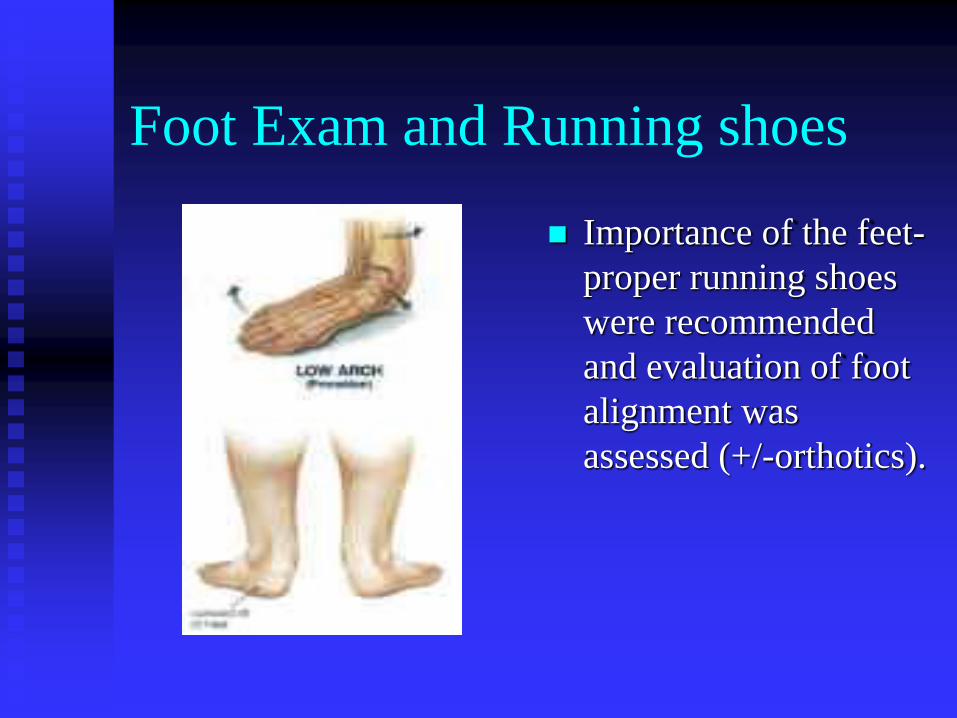
Foot Exam and Running shoes
Importance of the feet-
proper running shoes
were recommended
and evaluation of foot
alignment was
assessed (+/-orthotics).
Orthotics

Case 2
14 year old basketball player has
c/o anterior knee pain for 3
months. He has grown 4 inches
in the past 5 months. No
locking or giving way.
-Provoked by jumping, kneeling
and palliated by rest.
-On examination, tenderness
localized to the tibial tubercle.
All other tests are normal.
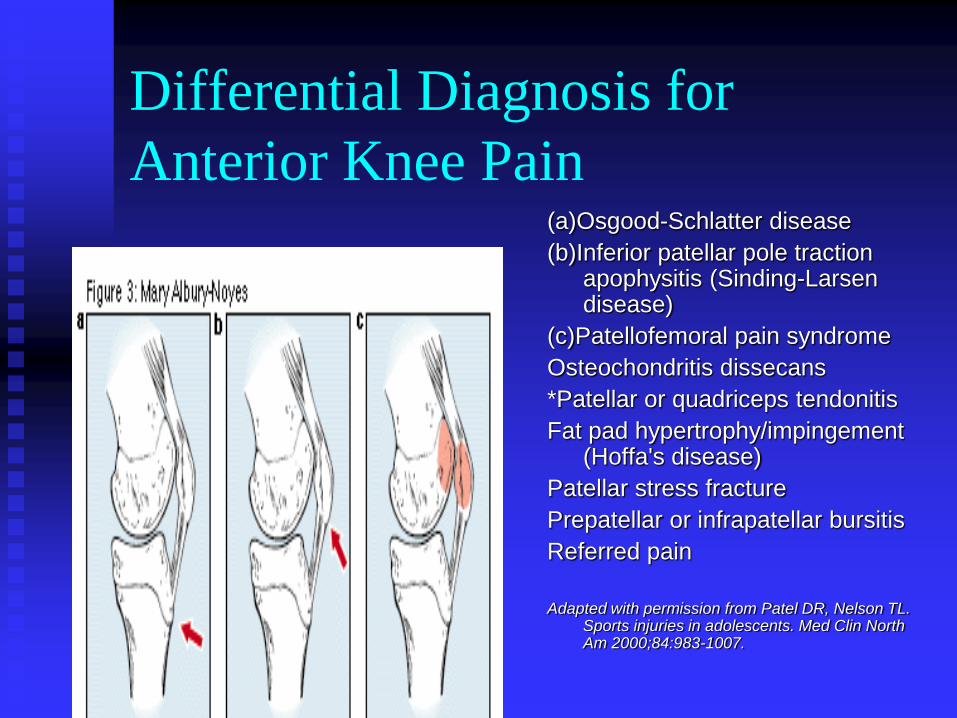
Differential Diagnosis for
Anterior Knee Pain (a)Osgood-Schlatter disease
(b)Inferior patellar pole traction apophysitis (Sinding-Larsen disease)
(c)Patellofemoral pain syndrome
Osteochondritis dissecans
*Patellar or quadriceps tendonitis
Fat pad hypertrophy/impingement (Hoffa's disease)
Patellar stress fracture
Prepatellar or infrapatellar bursitis
Referred pain
Adapted with permission from Patel DR, Nelson TL.
Sports injuries in adolescents. Med Clin North Am 2000;84:983-1007.
Epidemiology of Apophysitis
Knee Injuries in Adolescents Osgood Schlatter
disease(OSD)
-Prevalence athletic
adolescents 21% vs. 4.5%
of age matched non-
athletes
-Age of onset:
Girls 8-13 Boys 10-15
-Boys > Girls, equalizing
-Bilateral in 20%
Sinding-Larsen-Johansson disease(SLD)
-Prevalence athletic adolescents unkown, but 10-20% coexist with OSD
-Age of onset-similar to OSD
-Boys > Girls
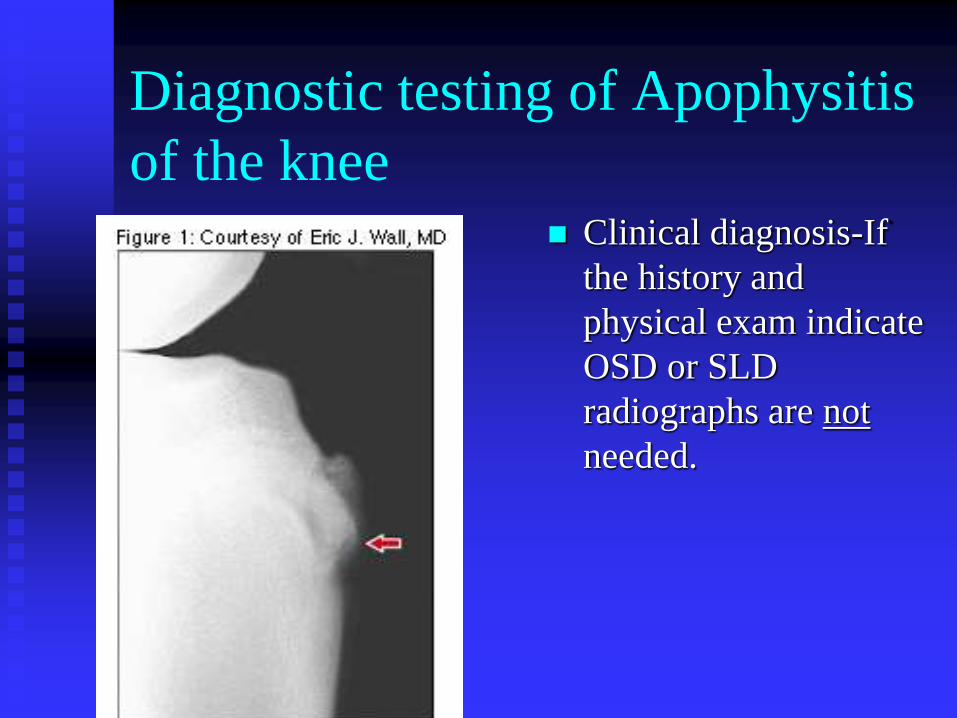
Diagnostic testing of Apophysitis
of the knee Clinical diagnosis-If
the history and
physical exam indicate
OSD or SLD
radiographs are not
needed.
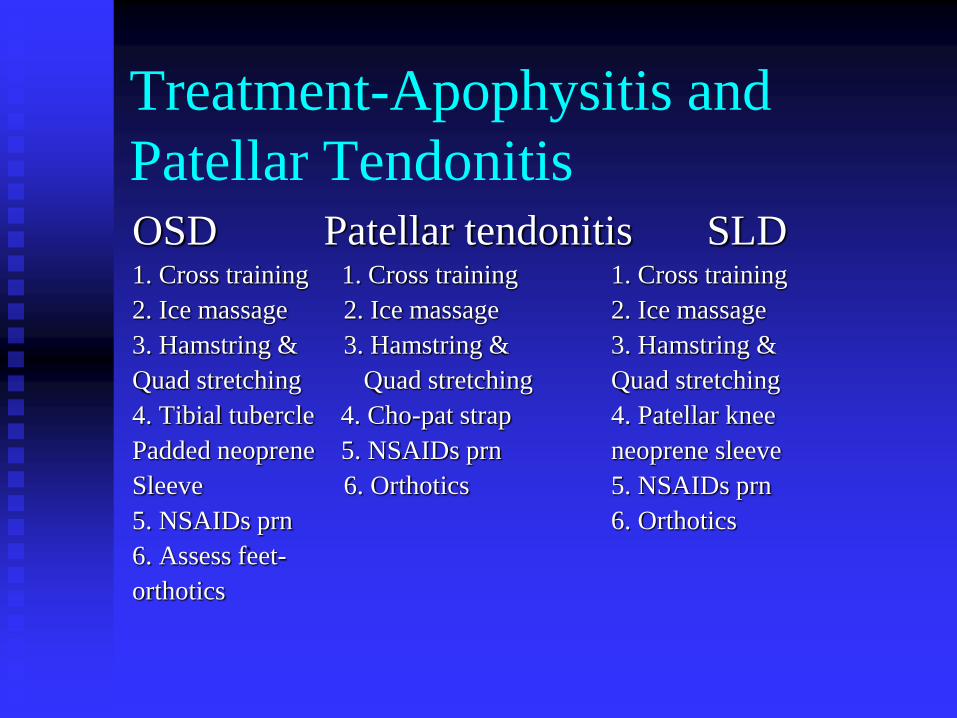
Treatment-Apophysitis and
Patellar Tendonitis OSD Patellar tendonitis SLD
1. Cross training 1. Cross training 1. Cross training
2. Ice massage 2. Ice massage 2. Ice massage
3. Hamstring & 3. Hamstring & 3. Hamstring &
Quad stretching Quad stretching Quad stretching
4. Tibial tubercle 4. Cho-pat strap 4. Patellar knee
Padded neoprene 5. NSAIDs prn neoprene sleeve
Sleeve 6. Orthotics 5. NSAIDs prn
5. NSAIDs prn 6. Orthotics
6. Assess feet-
orthotics

Cho-pat strap
Complications of Apophysitis
Painful kneeling-60% of all OSD patients
have chronic pain on hitting tibial tuberosity
Painless “bump” over tibial tuberosity-most,
benign
Painful ossicle @ distal or proximal patellar
tendon insertion or avulsion of tibial
tubercle - surgical removal (rare)
Case 3 14 year old female basketball
player c/o knee pain after sudden fall to floor. No contact or trauma occurs to the knee. She heard a “pop.” She is still growing and is currently going through “puberty” w/o menses yet. Her knee is acutely swollen.
On examination:
Inspection: + effusion
Special tests: + Anterior drawer and + Lachmans. Remainder of testing difficult due to swelling.
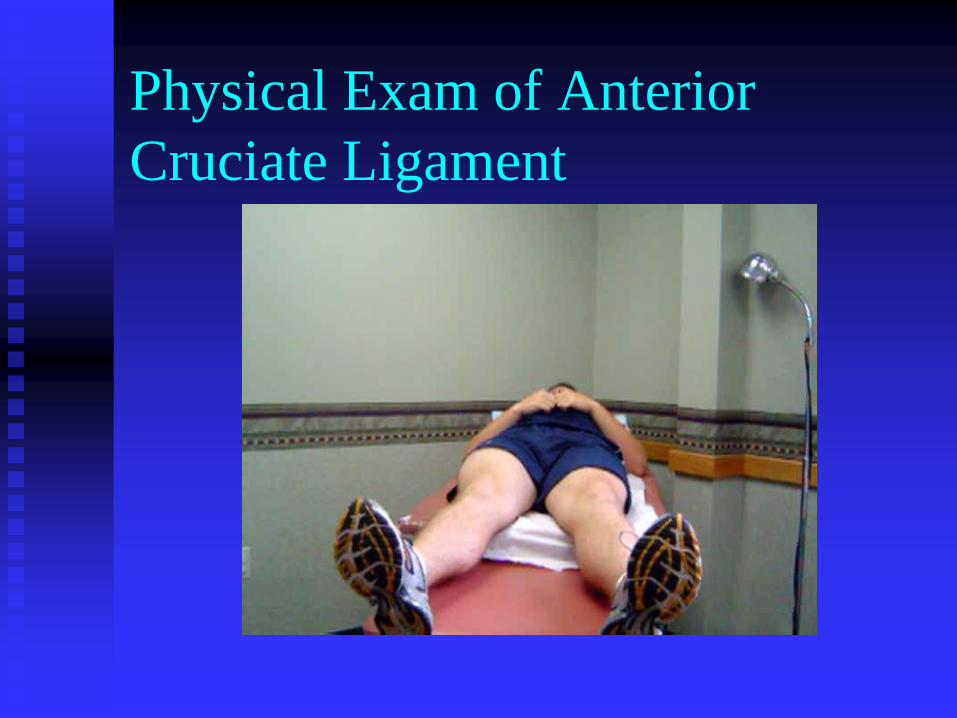
Physical Exam of Anterior
Cruciate Ligament
Epidemiology of ACL injuries-
epidemic in woman athletes
80,000 – 250,000 ACL injuries per year in
young athlete (15-25 years of age)
More common in woman than in men
Non-contact mechanism much more
common in woman and in jumping and
quick starting and stopping sports
(basketball, soccer, etc.)
Why is an ACL tear an epidemic
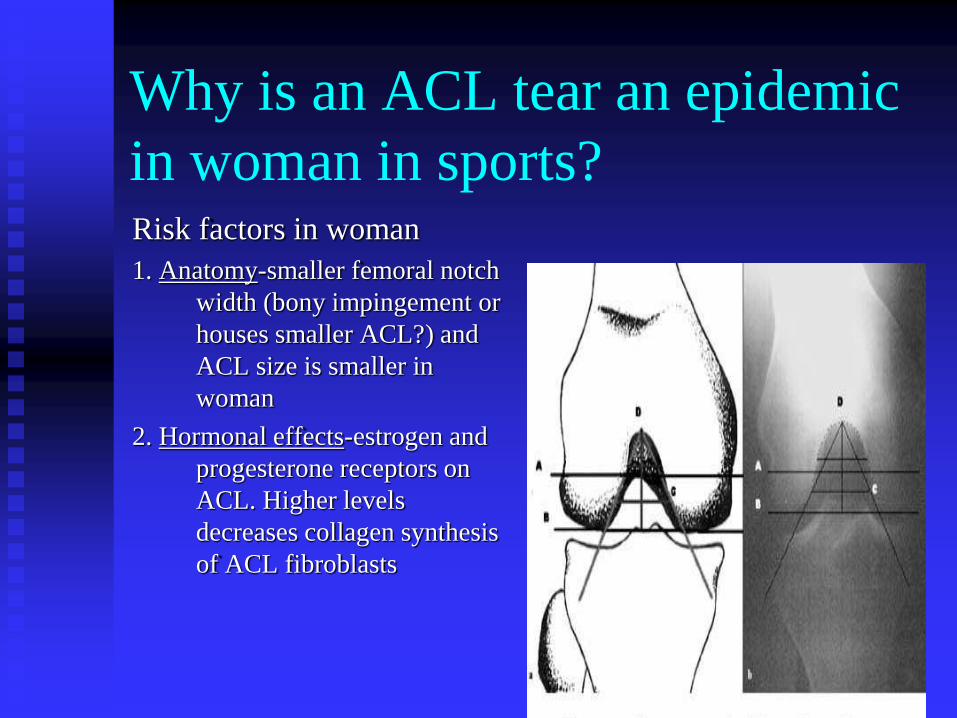
in woman in sports? Risk factors in woman
1. Anatomy-smaller femoral notch
width (bony impingement or
houses smaller ACL?) and
ACL size is smaller in
woman
2. Hormonal effects-estrogen and
progesterone receptors on
ACL. Higher levels
decreases collagen synthesis
of ACL fibroblasts
Why is an ACL tear an epidemic
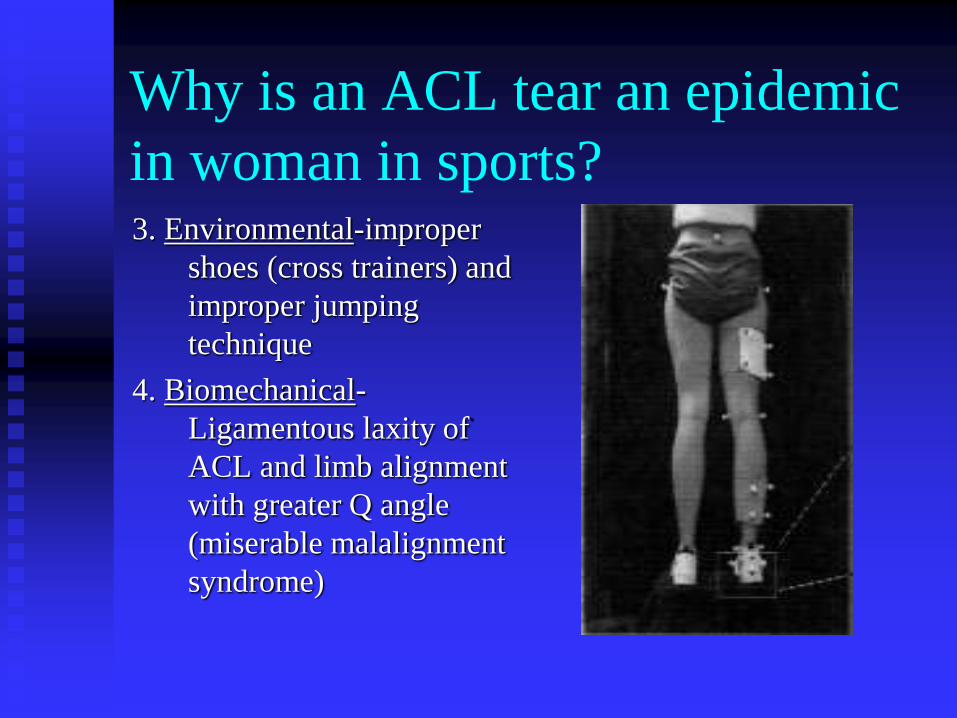
in woman in sports? 3. Environmental-improper
shoes (cross trainers) and
improper jumping
technique
4. Biomechanical-
Ligamentous laxity of
ACL and limb alignment
with greater Q angle
(miserable malalignment
syndrome)
Physes of immature knee
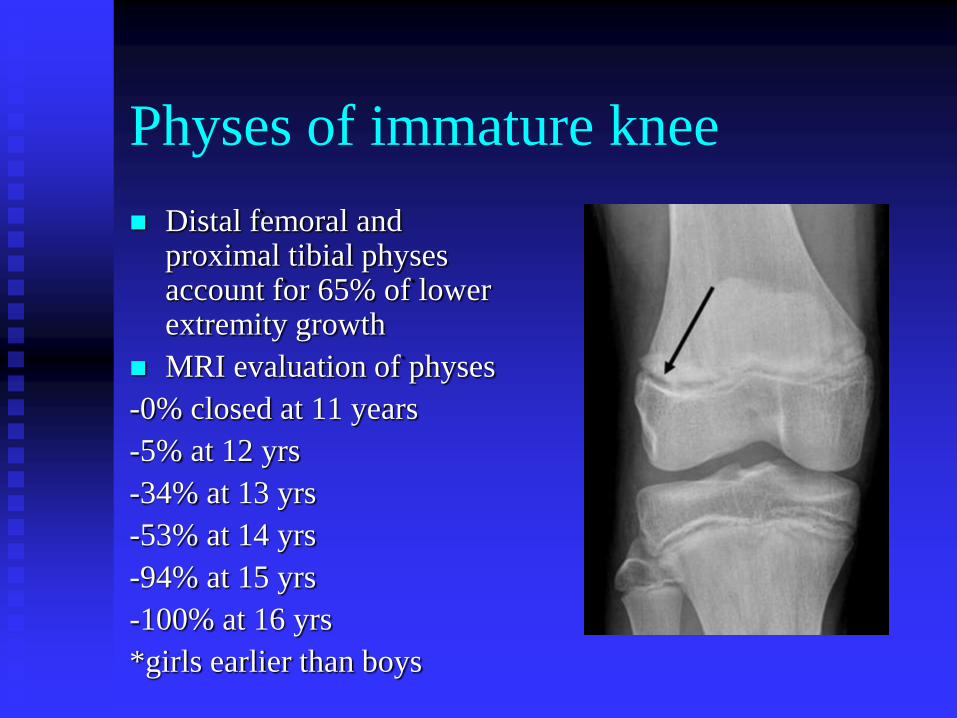
Distal femoral and proximal tibial physes account for 65% of lower extremity growth
MRI evaluation of physes
-0% closed at 11 years
-5% at 12 yrs
-34% at 13 yrs
-53% at 14 yrs
-94% at 15 yrs
-100% at 16 yrs
*girls earlier than boys
Evaluation of skeletal maturity
An accurate assessment of skeletal maturity aids in
discussing risks and benefits of operative and non-
operative treatment options.
-Tanner staging
-Radiographs of the hand and knee
-Timing of adolescent growth spurt
-Onset of menses
-Comparison of parental height
Treatment
Midsubstance Tears
-Non-operative treatment-traditionally accepted as standard
1. Activity modification: no cutting or stop/start activities
2. Physical therapy
3. Bracing
4. Monitor until skeletal maturity-once reaches skeletal maturity, then operative ACL reconstruction
Return to play-to brace or not to
brace……
Derotational braces by most authorities in
Sports Medicine are thought as simply
“psychological aids to recovery.”
-Problems: Difficult to properly fit
No Evidence based studies to
support
Treatment
Problem: Adolescent population by nature is
active and commonly suffers other injuries due to
an unstable knee
-Multiple studies have shown increased rates of
meniscal tears, chondral injuries, and early
degenerative arthritis *Graf et al, Arthroscopy, 1992 and Pressman et al, J Ped Ortho, 1997.
Treatment
-Alternative treatment: Transphyseal, soft tissue
allograft (patellar tendon) reconstruction.
Concern: Growth abnormalities
One study of 16 pts Tanner stage 3 or 4 showed all
athletes returned to competitive athletics w/o
growth abnormalities *Shelbourne et al, AJSM, 2004.

ACL injury prevention programs
Prevention Programs: combine proper jumping, landing and cutting techniques for athletes while providing strength training, flexibility, plyometrics and sports specific exercises.
-Baystate, Massachusetts-Jump Program
-University of Michigan-Leap program
-California Prevention Injury and Enhance Performance Program (PEP)-17 minutes
www.aclprevention.org
Case 4
JL is a 15 yo boy w/ acute onset of R knee pain and swelling x 1 day
-Tackled in football, knee “twisted” and he heard a “pop”
-Denies knee “giving out under him”
-On exam had effusion and right thigh atrophy over VMO. Tenderness over medial femoral condyle. Decreased ROM as could flex only 45 degrees. Remainder of exam (including ligament testing) was normal.
-PMH- Knee injury 1 year ago.
Osteochondritis Dissecans of the
Knee(OCD)-Epidemiology Most common in 13-21 yr olds in sports
Most common site is medial femoral condyle
Likely secondary to avascular necrosis of subchondral bone from multifactorial causes (trauma, repetitive impact to tibial spine, abnormal ossification of epiphyseal cartilage)
Clinical Findings of OCD
Physical exam often inconclusive.
Most consistent finding is thigh atrophy secondary
to lack of use and de-conditioning.
With floating bodies, can develop locking,
catching, pain and effusion
Meniscal tests are frequently positive due to the
asymmetry of the joint and the compensation by
the athlete for the pain.
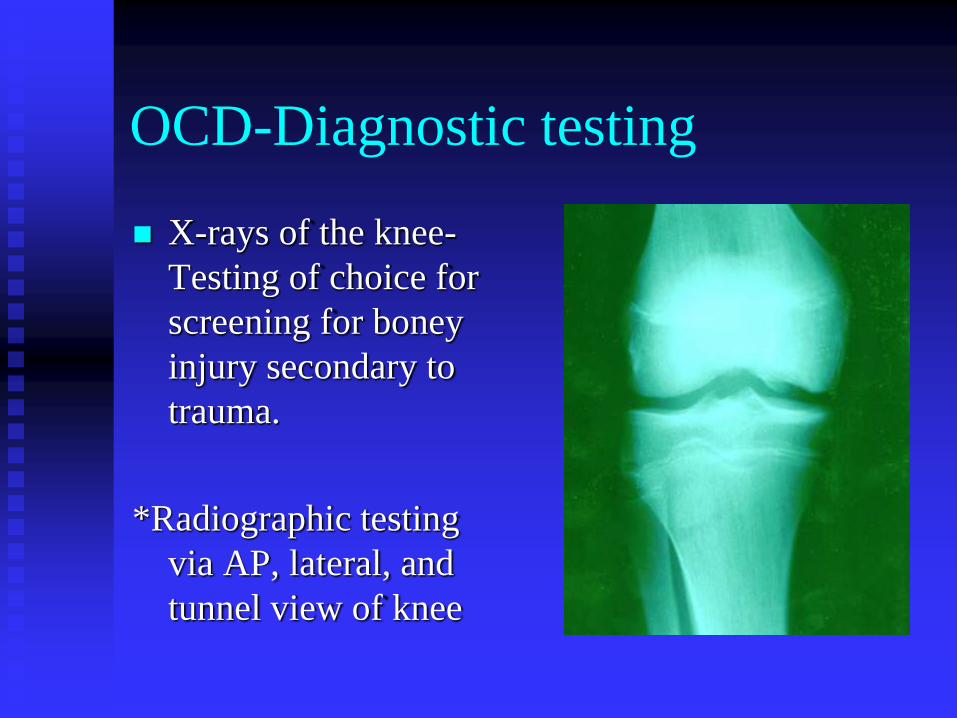
OCD-Diagnostic testing
X-rays of the knee-
Testing of choice for
screening for boney
injury secondary to
trauma.
*Radiographic testing
via AP, lateral, and
tunnel view of knee
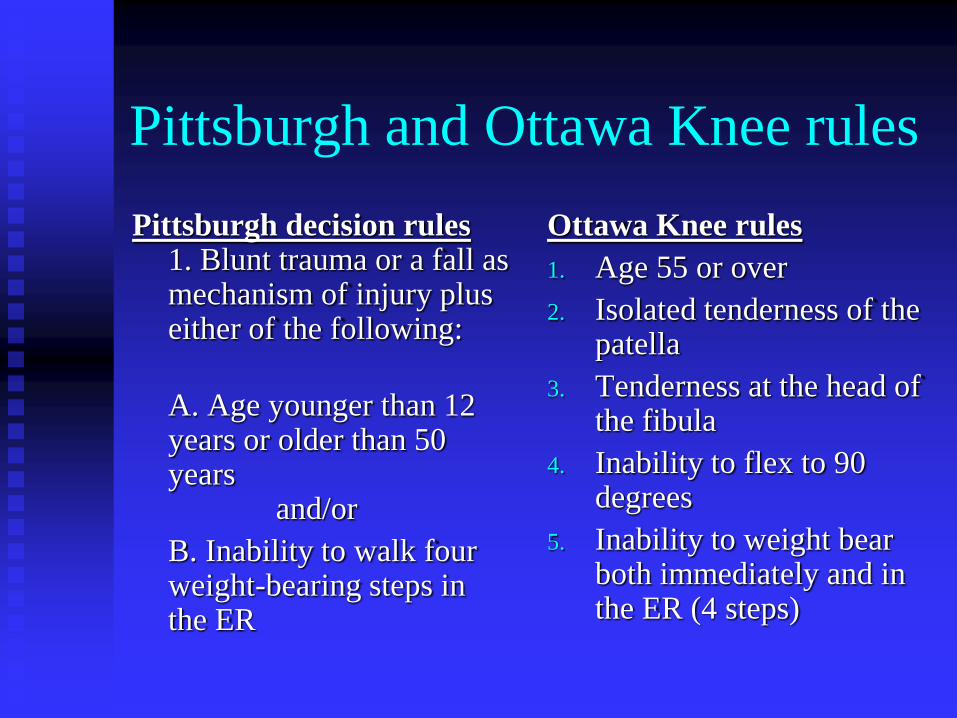
Pittsburgh and Ottawa Knee rules
Pittsburgh decision rules 1. Blunt trauma or a fall as mechanism of injury plus either of the following:
A. Age younger than 12 years or older than 50 years and/or
B. Inability to walk four weight-bearing steps in the ER
Ottawa Knee rules
1. Age 55 or over
2. Isolated tenderness of the patella
3. Tenderness at the head of the fibula
4. Inability to flex to 90 degrees
5. Inability to weight bear both immediately and in the ER (4 steps)
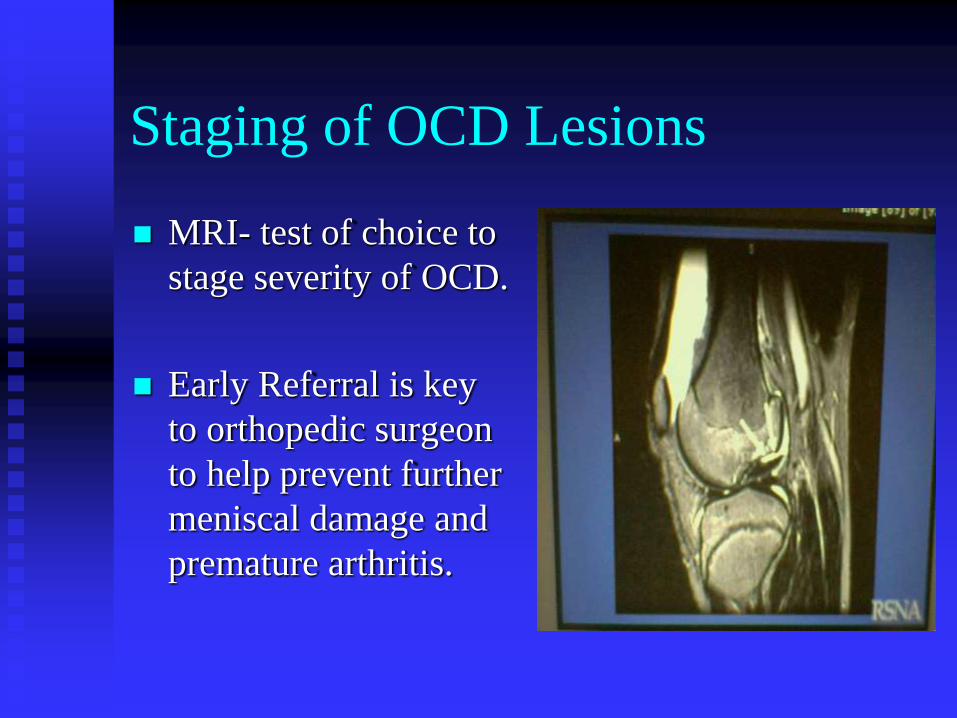
Staging of OCD Lesions
MRI- test of choice to
stage severity of OCD.
Early Referral is key
to orthopedic surgeon
to help prevent further
meniscal damage and
premature arthritis.
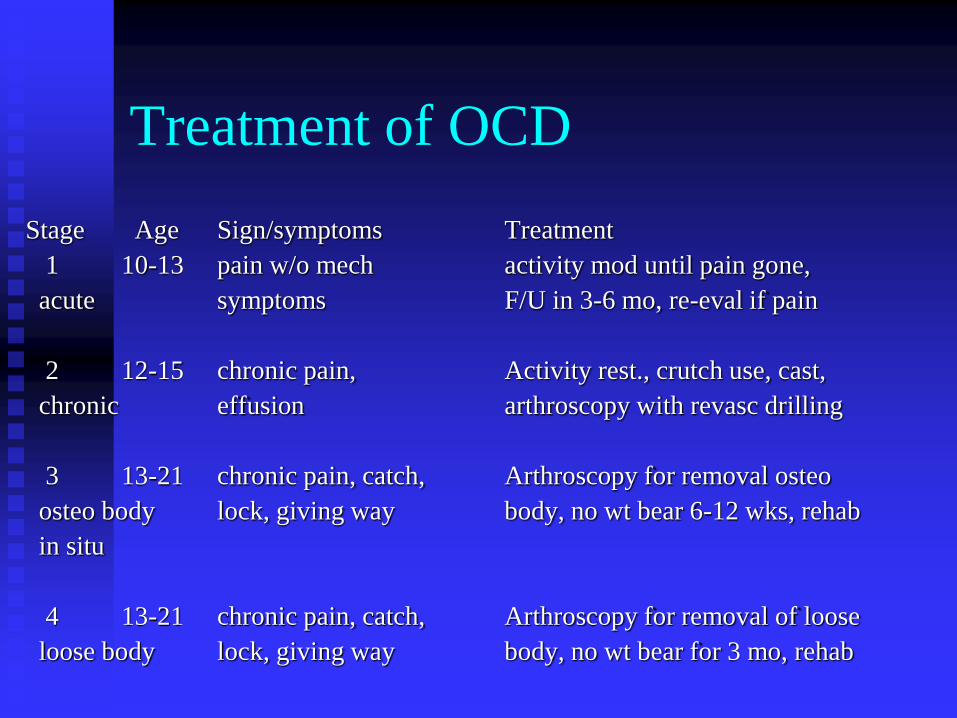
Treatment of OCD
Stage Age Sign/symptoms Treatment
1 10-13 pain w/o mech activity mod until pain gone,
acute symptoms F/U in 3-6 mo, re-eval if pain
2 12-15 chronic pain, Activity rest., crutch use, cast,
chronic effusion arthroscopy with revasc drilling
3 13-21 chronic pain, catch, Arthroscopy for removal osteo
osteo body lock, giving way body, no wt bear 6-12 wks, rehab
in situ
4 13-21 chronic pain, catch, Arthroscopy for removal of loose
loose body lock, giving way body, no wt bear for 3 mo, rehab
Take Home Points
1. PFKD-most common knee injury in adolescents.
2. If the history and physical exam indicate OSD, SLD, or Patellar tendonitis radiographs are not needed.
3. An accurate assessment of skeletal maturity aids in discussing risks and benefits of operative and non-operative treatment options in ACL injuries.
4. ACL Prevention Programs combine proper jumping, landing and cutting techniques for athletes while providing strength training, flexibility, plyometrics and sports specific exercises.
5. Utilize the Pittsburgh or Ottawa knee rules to determine when to obtain radiographs of knee injuries.