Embed Size (px)
Citation preview
SICOT-J 2018, 4, 10© The Authors, published by EDP Sciences, 2018https://doi.org/10.1051/sicotj/2018002
Available online at:www.sicot-j.org
REVIEW ARTICLE
Current paediatric orthopaedic practice in hereditary multipleosteochondromas of the forearm: a systematic reviewTamer A. EL-Sobky1,*, Shady Samir1, Ahmed Naeem Atiyya2, Shady Mahmoud1, Ahmad S. Aly1,and Ramy Soliman2
1 Division of Paediatric Orthopaedics, Department of Orthopaedic Surgery, Faculty of Medicine, Ain-Shams University,Abbasia, Cairo, Egypt
2 Division of Hand Surgery, Department of Orthopaedic Surgery, Faculty of Medicine, Ain-Shams University, Abbasia,Cairo, Egypt
Received 25 October 2017, Accepted 29 December 20
*Correspon
This is anO
17, Published online 21 March 2018
Abstract -- Introduction: This systematic review aims to answer three research questions concerning themanagement of hereditarymultiple osteochondromas of forearm in children:What is the best available evidencefor the currently employed surgical procedures? What patient characteristics are associated with betterprognosis? What disease characteristics are associated with better prognosis?Methods: We searched the literature using three major databases with no publication date restrictions. Toenhance search sensitivity and maintain precision we used keywords/subject terms correlating with patientpopulation, problem and interventions.We used strict inclusion/exclusion criteria to improve validity evidence.Results: The search process yielded 34 eligible studies with a total of 282 patients (315 forearms). Wecomprehensively analysed study and patient demographics and interventions and outcomes. Eleven studies(32%) had a long-term follow-up and 31 studies (91%)were retrospective. Of the total number of forearms, ulnarlengthening +/� associated procedures was used in 210 forearms (66.7%), isolated osteochondroma excision in65 forearms (20.6%) and isolated distal radius hemiepiphysiodesis in 15 forearms (4.7%) among others.Discussion: Ulnar lengthening can restore radiologic anatomy, improve appearance and to a lesser extentobjective clinical parameters like joint range of motion on the short/intermediate term. Isolatedosteochondroma excision can relief pain and satisfy cosmetic concerns occasionally. There is poor evidenceto suggest that surgery improves quality of life or function. Predictors of surgical success in regard to patient anddisease characteristics remain elusive. Natural history and prospective randomized control studies where thecontrol group receives no treatment should be rethought. They have the potential for bias control andidentification of the ideal surgical candidate. The complex interplay between the confounding variables hasundermined the capability of most studies to provide well-grounded evidence to support and generalize theirconclusions. Valid quality of life scales should supplement objective outcome measures.
Key words: Children, Hereditary multiple exostoses, Multiple cartilaginous exostoses, Diaphyseal aclasis,Benign forearm tumours, Skeletal dysplasia, Ulna lengthening.
Introduction
Hereditary multiple osteochondromas (HMO) areuncommon benign bone tumors. They are usuallydiagnosed in early childhood. HMO are inherited in anautosomal dominant manner. The two genes in whichpathogenic variants are known to cause HMO are EXT1and EXT2 [1,2]. The pathogenesis is linked a criticalreduction in heparan sulfate chain elongation [2]. Con-trastingly, solitary osteochondromas are common benign
ding author: [email protected]
penAccess article distributed under the terms of the CreativeComwhich permits unrestricted use, distribution, and reproduction i
bone tumours. The growth pattern of a solitary osteo-chondromas is comparable to that of HMO. The diagnosisof HMO is based upon a distinct clinical and radiographicappearance. A fundamental clinical feature is multiplefirm swellings erupting from the ends of long bones or fromthe surface of flat bones usually symmetrical [1].Radiologically they present as multiple juxtaphysealcartilage capped bony growths with undisturbed courseof cortex and medullary bone from the normal bone intothe osteochondroma [1,2]. Masada and colleagues [3]classified HMO into three main groups based upon thepathologic anatomy. Patients with HMO can exhibit limb
monsAttribution License (http://creativecommons.org/licenses/by/4.0),n any medium, provided the original work is properly cited.

2 T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10
length discrepancy, angular deformities around the knee,ankle and forearm, short stature, painful joint range ofmotion, joint subluxation and neurovascular compression[1,2]. Up to 70% of patients with HMOmanifest in forearmdeformities [4]. Most forearm and hand deformities areclinically pronounced [4,5]. Unbalanced physeal growthbetween the radius and ulna can result in forearm bowing,relative shortening of radius or ulna, carpal instability,and radial head dislocation with subsequent limitation offorearm rotation [1,4]. Forearm HMO has been managedby one or more of the following procedures: isolatedexcision of osteochondroma [6–12], acute [7,12,13], and/orgradual [6,14–26] ulnar lengthening, combined ulnar andradial lengthening [27], distal radial hemiepiphysiodesis[3,12,28,29], corrective radial osteotomy [7,13,30], crea-tion of one-bone forearm [31–33], radial head relocation[8,10,22], reconstruction of the distal ulnar epiphysis byvascularized proximal fibula epiphysis [34] and Sauve-Kapandji procedure [10]. Nevertheless, the optimalmanagement of HMO of the forearm is greatly disputable.The best evidence for each of the practiced surgicalprocedures, the optimal timing for intervention andpredictors for surgical success are alike unsettled disputes.Some authors cast fresh doubts about the value of surgeryin regard to improving function [7,35]. This topic has notbeen critically appraised before in the literature. Thissystematic review aims to resolve the above-mentioneddisputes. In consequence we formulated the followingresearch questions relating to the management of HMO offorearm in children: 1)What is the best available evidencefor surgical procedures used to manage HMO? 2) Whatpatient characteristics are associated with better progno-sis? 3) What disease characteristics are associated withbetter prognosis?
MethodsSearch approach
This article does not contain any studies with humanparticipants or animals performed by any of the authors.All authors shared in the study selection and dataextraction process relating to the surgical managementof HMO of the forearm in children.We conducted a searchfor English language publications before July 2017employing the following electronic databases: PubMed,Google scholar andEmbase.We checked the reference listsof the captured articles and review articles for additionaleligible publications. We also screened articles that citedthe captured articles. We discarded non-peer reviewedliterature that was not published in scientific journals andsecondary research such as review articles, letter to theeditor and commentaries. We conducted the initial searchon May 2017. We performed an additional search prior tomanuscript submission to make certain the extractedliterature is updated. To expand the recapture of relevantstudies our search strategy comprised both keywords andindexwords in accordancewithMedical SubjectHeadings.
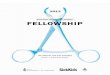
We used Boolean operators properly to optimize searchresults quantitatively and qualitatively. The three mainBoolean operators are AND, OR, and NOT. Booleanoperators are used to narrow, broaden or restrict thesearch results. We aimed at avoiding biased inclusionterms. Hence, the selection of search terminology wassubdivided according to (a) patient population, (b)problem and (c) intervention terms.We retrieved relevantstudies using the following patient population andproblem terms: children, paediatric, hereditary multipleosteochondromas, hereditary multiple exostoses, multiplecartilaginous exostoses, diaphyseal aclasis, forearmtumors, ulnar shortening. Additionally, we used thefollowing intervention terms: osteochondroma excision,radius osteotomy, ulnar lengthening, distraction osteo-genesis. We did not impose limiting terms with regard tostudy design types. The collected studies were excluded asfollows; (a) descriptive studies reporting the clinical and/or radiologic features, (b) studies reporting the naturalhistory, (c) studies reporting on adults, (d) studiesreporting exclusively on solitary osteochondromas, (e)studies reporting solely on pathologies other than HMO,(f) studies with follow-up< one year, (g)HMOmanaged inthe context of malignant transformation and (f) studiesreporting solely on HMO of the hand. We includedprospective and retrospective studies. We also includedcase series and case reports. If studies were heterogenousfor age population and pathologic disorder, only skeletallyimmature patients with HMO were selected. Disputes inregard to study selection were settled with face-to-facemeetings. A schematic representation of the literatureextraction process together with exclusions is provided(Figure 1).
Quality appraisal instruments
The reported items of this review were in concordancewith the Preferred Reporting Items for SystematicReviews and Meta-Analyses statement [36]. We usedthe systematic review critical appraisal worksheet fromthe University of Oxford Centre for Evidence-basedMedicine www.cebm.net/critical-appraisal to checkquality through all phases of this systematic review[37]. We identified factors that may reflect a significantresearch bias before, during and after the conduction ofincluded studies with respect to patient selection,outcome measure assessment, statistics and confoundingvariables. We employed a valid instrument designed toevaluate the methodological quality of non-randomizedsurgical studies, whether comparative or non-compara-tive (MINORS) [38]. We selected MINORS [38] evalua-tion instrument as case series observational studies werethe key of the primary studies. We conducted acomprehensive comparison between the aggregatedtreatment outcomes and tried to identify patient anddisease features linked to better prognosis. To avoid biasin favour of reporting positive findings only we decided tofinalize our systematic review protocol in advance of anydata extraction.

Figure 1. A schematic representation of literature extraction process.
T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10 3
ResultsStudy demographics
The literature extraction process involved 4 phases: (a)identification, (b) screening, (c) eligibility, and (d)inclusion. There were only three prospective case seriesstudies [20,27,39] (OCEBM type II) versus 31 retrospec-tive studies (OCEBM type III). These prospective studieshad small sample sizes [39] or were simply case reports[20,27]. The characteristics of the 34 final studies includedin this systematic review are presented in Table 1. Elevenstudies (32%) had a follow-up> 5 years, five of which wererelatively sizable with study participants ≥ 10. Of the 34included studies, 32 were published in recognized ortho-paedic society journals. The publication years ranged from2016 to 1984. Eight were multicentre studies [8,11,13,15–17,19,23]. According to MINORS the methodologicquality all but three prospective studies scored 5 out of 8.
Patient characteristics
The summed number of patients enrolled in the includedstudies was 304. One study with 22 patients was excludedfrom analysis due to poor demographic reporting but itsimplicationswere discussed [29].Therefore, thefinal number
of patients enrolled was 282 patients with 315 forearms. Themean age of patients for individual studies ranged from (5–13.5) years. One study provided a separate mean age foreach of the three surgical procedures conducted [10] andanother provided a separatemean age for boys and girls [28].Gender distribution was provided for 222 patients (79%) ofthe 282 patients finally enrolled in the review. There were118 (53%) males and 104 (47%) females. Six studies did notprovide the gender distribution [7,10,11,16,28,29]. Onestudy did not provide a mean age or follow-up and provideda range instead [29]. For publications that did not directlyreport the Masada types the information was extrapolatedfrom descriptive clinical picture and/or radiographs.Interestingly, in one study [26] neither Masada types norosteochondroma excisionwere reported.Of the 257 forearmsthat “reported” Masada types, 166 (64.6%) were type I, 25(9.7%) were type IIA, 48 (18.7%) were type IIB and 18 (7%)were type III. Two studies [22,25] referencedMasada but didnot provide details of patients’ radiographic grading.
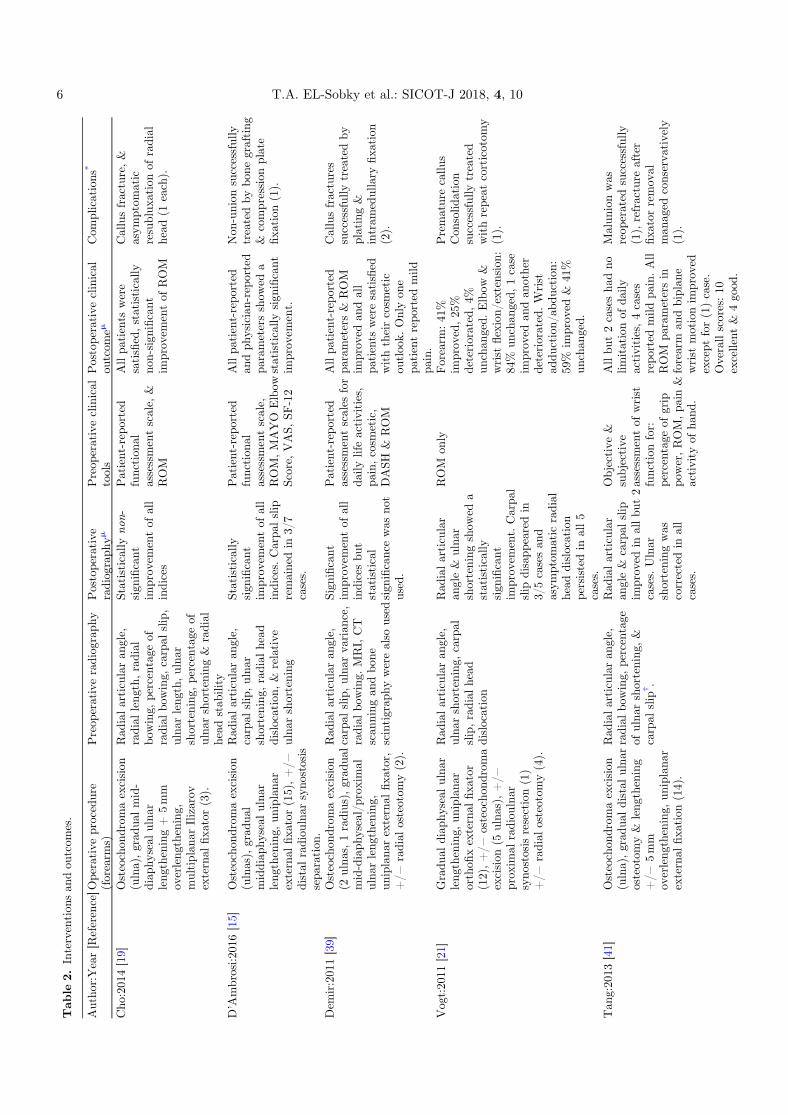
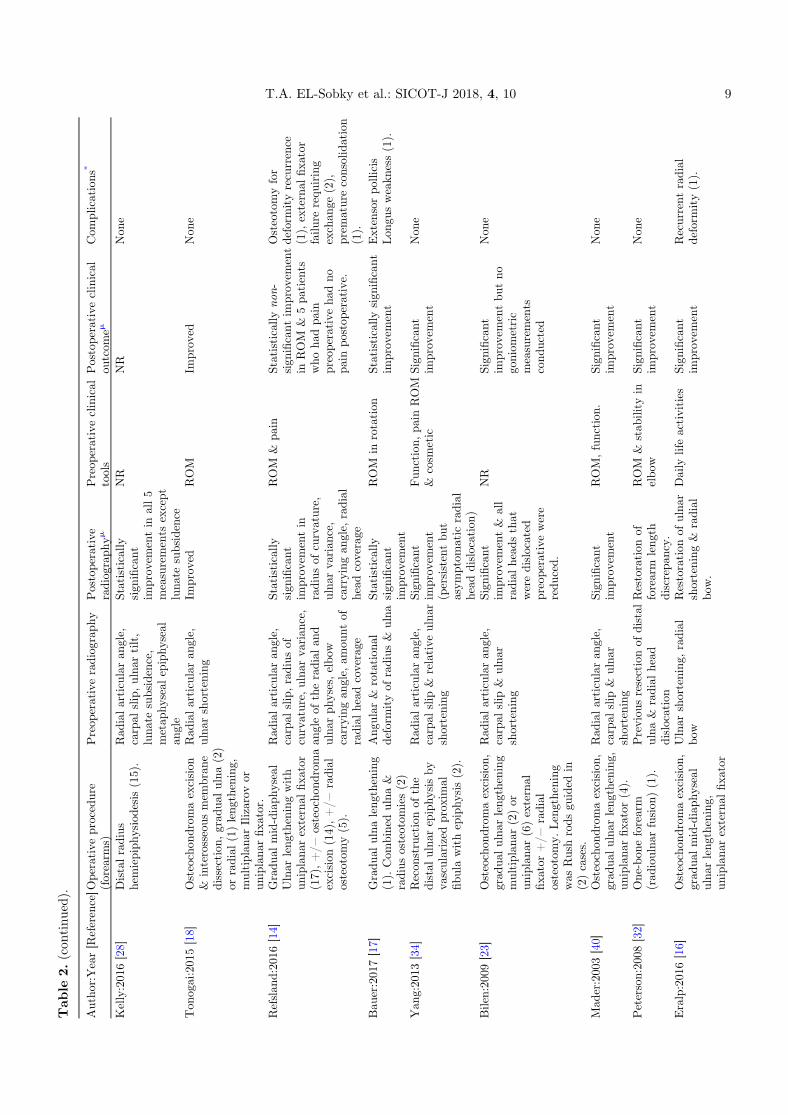
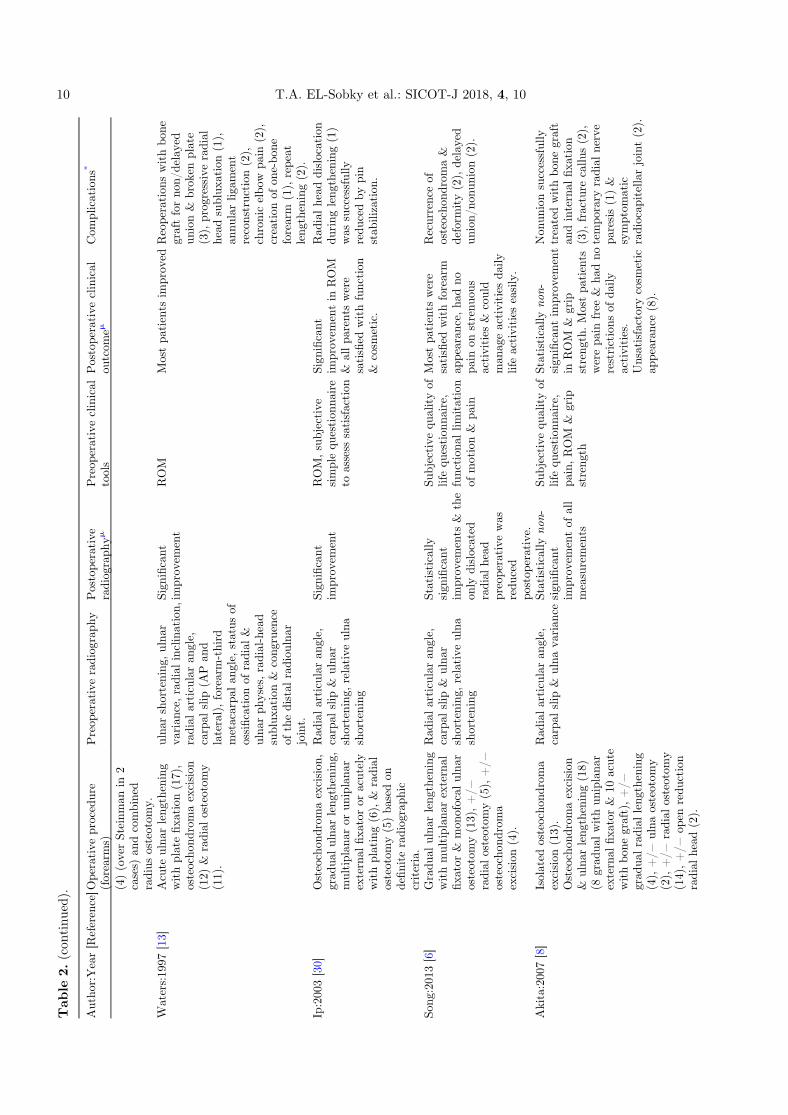
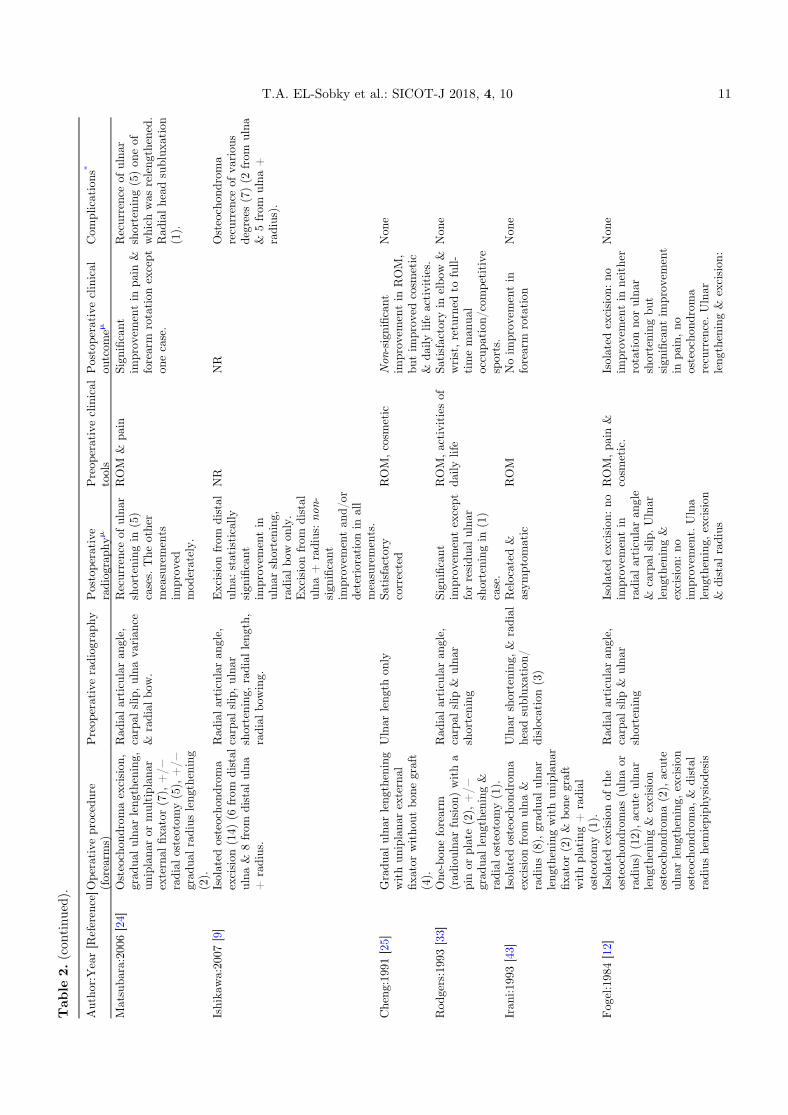
Interventions and outcomes
A detailed reporting of the interventions, outcomes,and complications at final follow-up of the included studiesin this review is presented (Table 2). The indications of

Tab
le1.
Stud
ydemog
raph
ics.
Autho
r:Year
[Reference]
Patients
(N)
Forearm
s(N
)Male:Fem
ale
(N)
Mean
age(Y
)Mean
follo
w-up
(Y.M
)
Fam
ilyhistory(N
)Su
rgical
indication
sMasad
asubtyp
e
Cho
:201
4[19]
33
0:3
7.2
2.1
NR
Restrictedrotation
&cosm
etic
IIB
(3)
D’A
mbrosi:2
016[15]
1515
8:7
10.1
6.4
NR
Restrictedrotation
orda
ilyactivities,ulna
rshortening
≥1.5cm
IIA
(6),IIB
(8),III
(1)
Dem
ir:201
1[39]
66
2:4
124.2
NR
Restrictedrotation
,pa
in,neurov
ascularcompression
&cosm
etic
IIA
(3),IIB
(3)
Vog
t:20
11[21]
1212
3:9
9.8
2NR
Ulnar
shortening
≥1cm
,prog
ressivedeform
ity,
function
alim
pairment
I(7),IIA
(1),IIB
(4)
Tan
g:20
13[41]
1414
8:6
9.2
3.6
NR
Restrictedda
ilyactivities,Ulnar
shortening
≥1.5cm
,&
cosm
etic
I(14)
Masad
a:19
89[3]
1113
5:6
10.3
2.6
7Restrictedda
ilyactivities
&ROM
I(9),IIA
(1),IIB
(2),
III(1)
Beutel:2
014[20]
11
1:0
112
Non
ePain&
restricted
ROM
inelbo
wI(1)
Hill:201
1[22]
#4
52:2
8.8
2.2
NR
Wrist,forearm
orelbo
wdeform
itywithulna
ror
radial
shortening
>2cm
,pa
rticularly
youn
gchild
ren,
restricted
daily
activities
NR
Litzelm
ann:20
12[7]
1415
NR*
11.1
9.8
NR
Cosmetic
orfunction
al(painor
limited
mob
ility)
basedup
onsurgeonpreference
I(7),IIA
(1),IIB
(4),
III(3)
Jiya
:199
7[11]
1012
NR
13.3
6.3
NR
Restrictedda
ilyactivities,grip
streng
thI(9),III(3)
Shin:200
6[10]
2222
NR
9.2,
8.8,
11.1
†3.6
NR
Pain,
function
alloss
ofmov
ementof
theforearm
&cosm
esis.
I(11),Ian
d/or
IIB
(11)
Rasoo
l:200
8[31]
22
0:2
51.3
NR
Elbow
pain
&deform
ity
IIA
(1),IIB
(1)
Pritchett:198
6[26]
810
3:5
11.4
3.1
NR
Ulnar
shortening
≥1.5,
carpal
slip
≥50
%,
symptom
atic
radial
head
instab
ility,restricted
daily
activities
&cosm
etic.
NR
Massobrio:201
5[27]
11
0:1
920
NR
Fun
ctiona
lrestrictionof
ROM
inelbo
w&
wrist
I(1)
Kelly:201
6[28]
1315
NR
Boy
s:10
.3&
Girls:11
.55
NR
NR
NR
Ton
ogai:201
5[18]
23
1:1
9.5
3.7
NR
RestrictedROM
I(2),III(1)
Refslan
d:20
16[14]
1717
11:6
74.6
NR
RestrictedROM
I(10),IIB
(7)
Bau
er:201
7[17]
33
NR*
15NR
NR
RestrictedROM
NR
Yan
g:20
13[34]
22
1:1
6.5
Boy
:1&
Girl:8
1Deformed
wrist
I(1),IIB
(1)
Bilen:20
09[23]
78
3:4
103.3
NR
NR
I(5),IIB
(3)
Mad
er:200
3[40]
24
1:1
8.8
2NR
Fun
ctiona
lrestricted
ofROM,ulna
r/radial
shortening
≥2cm
,carpal
slip
≥50
%&
RAA
≥40°
I(4)
Peterson:20
08[32]
11
1:0
9.2
15NR
Elbow
deform
ity&
unstab
le,forearm
leng
thdiscrepa
ncy,
restricted
motion
IIB
(1)
Eralp:201
6[16]
34
NR
105.8
NR
Deformity&
restricted
daily
lifeactivities
I(4)
Waters:19
97[13]
17NR
11:11*
10.7
*3
NR
Progressive
forearm/w
rist
deform
ity,
limited/p
ainful
ROM,radial
head
sublux
ation&
basedon
definite
radiog
raph
iccriteria
I(12),IIA
(4),IIB
(1)
4 T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10

Tab
le1.
(con
tinu
ed).
Autho
r:Year
[Reference]
Patients
(N)
Forearm
s(N
)Male:Fem
ale
(N)
Mean
age(Y
)Mean
follo
w-up
(Y.M
)
Fam
ilyhistory(N
)Su
rgical
indication
sMasad
asubtyp
e
Ip:200
3[30]
66
5:1
7.6
2.5
5Daily
lifeactivities
&cosm
etic
I(6)
Song
:201
3[6]
1013
6:4
9.6
4.8
NR
Fun
ctiona
llim
itationof
motion,
pain
&definite
radiog
raph
iccriteria
I(12),IIB
(1)
Akita:200
7[8]
23<
3117
:6*
1112
.818
Osteochon
drom
aexcision
:pa
infulROM
orcosm
etic.
Lengthening
/osteotomy:
basedon
definite
radiog
raph
iccriteria
I(21),IIA
(2),IIB
(3),
III(5)
Matsuba
ra:200
6[24]
77
3:4
10.8
7.1
NR
Rad
ialhead
dislocation,
daily
lifeactivities,pa
inful
forearm
rotation
,deform
ity&
cosm
etic.
I(6),IIA
(1)
Ishika
wa:20
07[9]
1314
6:7
7.9
4.5
NR
NR
I(14)
Cheng
:199
1[25]
44
2:2
121.5
NR
Ulnar
shortening
≥2cm
,radial
head
instab
ility
&function
allim
itationof
ROM
NR
Rod
gers:199
3[33]
22
2:0
13.5
8.5
1Painful
radial
head
dislocation+/�
severe
elbo
w&
forearm
deform
ity
IIA
(1),IIB
(1)
Iran
i:199
3[43]
1012
4:6
10.8
6.5
NR
Pain&
cosm
etic,prog
ressivedeform
ity(≥
1cm
ulna
rshortening
).I(4),IIA
(4),III(4)
Fog
el:198
4[12]
1721
12:5
94.5
NR
Pain&
cosm
etic,prog
ressiveradiolog
icdeform
ity(≥
1.5cm
ulna
rshortening
,radial
articularan
gle≥
30°&
carpal
slip
≥30°),rotation
restriction&
symptom
atic
radial
head
sublux
ation.
NR
Arm
s:19
97[29]
∞22
NR
NR
Ran
ge7–
77(m
eanNR)
>2
NR
Symptom
atic
osteocho
ndromaprom
inent,pa
inful,
aesthetically
unacceptab
le.
NR
Nnu
mber,NR
notrepo
rted.
*gend
erdistribu
tion
&otherdemog
raph
icswereprov
ided
either
fortheov
eralln
umberof
child
rendiag
nosedwithHMO
andno
tforthoseop
erated,o
rforov
eralln
umberof
differentdiag
nostic
grou
psan
dno
tforHMO,o
rforbo
thskeletally
mature&
immature;
#pa
tientcharacteristics,follo
w-up,
metho
dology
,outcomean
dcomplications
(exceptradial
head
status)wereprov
ided
for10
patients
withva
riou
sdiag
nosticgrou
psan
dthe
details
ofHMO
patients
wereno
tprov
ided
sepa
rately;
†asepa
rate
meanwas
givenforeach
ofhe
3surgical
procedures
cond
ucted;
<4/
23pa
tients
wereskeletally
mature;
∞thestud
ycomprised
acoho
rtof
patients
treatedconserva
tively
andsurgically
37of
which
weresubjectedto
ateleph
onequ
estion
nairebu
tpa
tientdemog
raph
ics,
disease
characteristicsan
dintervention
swereno
tprov
ided
sepa
rately
forop
erated
grou
p.
T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10 5
Tab
le2.
Intervention
san
dou
tcom
es.
Autho
r:Year[R
eference]O
perative
procedure
(forearm
s)Preop
erativeradiog
raph
yPostoperative
radiog
raph
ymPreop
erativeclinical
tools
Postoperative
clinical
outcom
emCom
plications
*
Cho
:201
4[19]
Osteochon
drom
aexcision
(ulna),grad
ualmid-
diap
hyseal
ulna
rleng
thening+
5mm
overleng
thening,
multiplan
arIlizarov
external
fixa
tor(3).
Rad
ialarticularan
gle,
radial
leng
th,radial
bowing,
percentage
ofradial
bowing,
carpal
slip,
ulna
rleng
th,ulna
rshortening
,percentage
ofulna
rshortening
&radial
head
stab
ility
Statistically
non-
sign
ificant
improv
ementof
all
indices
Patient-reported
function
alassessmentscale,
&ROM
Allpa
tients
were
satisfied,statistically
non-sign
ificant
improv
ementof
ROM
Callusfracture,&
asym
ptom
atic
resublux
ationof
radial
head
(1each).
D’A
mbrosi:2
016[15]
Osteochon
drom
aexcision
(ulnas),grad
ual
middiap
hyseal
ulna
rleng
thening,
uniplana
rexternal
fixa
tor(15),+/−
distal
radiou
lnar
syno
stosis
sepa
ration
.
Rad
ialarticularan
gle,
carpal
slip,ulna
rshortening
,radial
head
dislocation,
&relative
ulna
rshortening
Statistically
sign
ificant
improv
ementof
all
indices.
Carpa
lslip
remainedin
3/7
cases.
Patient-reported
function
alassessmentscale,
ROM,MAYO
Elbow
Score,
VAS,
SF-12
Allpa
tient-repo
rted
andph
ysician-repo
rted
parametersshow
eda
statistically
sign
ificant
improv
ement.
Non
-union
successfully
treatedby
bone
grafting
&compression
plate
fixa
tion
(1).
Dem
ir:201
1[39]
Osteochon
drom
aexcision
(2ulna
s,1radius),
grad
ual
mid-diaph
yseal/prox
imal
ulna
rleng
thening,
uniplana
rexternal
fixa
tor,
+/−
radial
osteotom
y(2).
Rad
ialarticularan
gle,
carpal
slip,ulna
rva
rian
ce,
radial
bowing.
MRI,CT
scan
ning
andbo
nescintigrap
hywerealso
used
Sign
ificant
improv
ementof
all
indicesbu
tstatistical
sign
ificancewas
not
used.
Patient-reported
assessmentscales
for
daily
lifeactivities,
pain,cosm
etic,
DASH
&ROM
Allpa
tient-repo
rted
parameters&
ROM
improv
edan
dall
patients
weresatisfied
withtheircosm
etic
outloo
k.Onlyon
epa
tientrepo
rted
mild
pain.
Callusfractures
successfully
treatedby
plating&
intram
edullary
fixa
tion
(2).
Vog
t:20
11[21]
Gradu
aldiap
hyseal
ulna
rleng
thening,
uniplana
rorthofi
xexternal
fixa
tor
(12),+/−
osteocho
ndroma
excision
(5ulna
s),+/−
prox
imal
radiou
lnar
syno
stosis
resection(1)
+/−
radial
osteotom
y(4).
Rad
ialarticularan
gle,
ulna
rshortening
,carpal
slip,radial
head
dislocation
Rad
ialarticular
angle&
ulna
rshortening
show
eda
statistically
sign
ificant
improv
ement.
Carpa
lslip
disapp
earedin
3/5casesan
dasym
ptom
atic
radial
head
dislocation
persistedin
all5
cases.
ROM
only
Forearm
:41
%im
prov
ed,25
%deteriorated,4%
unchan
ged.
Elbow
&wrist
flexion/
extension:
84%
unchan
ged,
1case
improv
edan
dan
other
deteriorated.W
rist
addu
ction/
abdu
ction:
59%
improv
ed&
41%
unchan
ged.
Prematurecallu
sCon
solid
ation
successfully
treated
withrepeat
corticotom
y(1).
Tan
g:20
13[41]
Osteochon
drom
aexcision
(ulna),grad
ualdistal
ulna
rosteotom
y&
leng
thening
+/−
5mm
overleng
thening,
uniplana
rexternal
fixa
tion
(14).
Rad
ialarticularan
gle,
radial
bowing,
percentage
ofulna
rshortening
,&
carpal
slip
† .
Rad
ialarticular
angle&
carpal
slip
improv
edin
allbu
t2
cases.
Ulnar
shortening
was
correctedin
all
cases.
Objective
&subjective
assessmentof
wrist
function
for:
percentage
ofgrip
power,ROM,pa
in&
activity
ofha
nd.
Allbu
t2casesha
dno
limitationof
daily
activities,4cases
repo
rted
mild
pain.All
ROM
parametersin
forearm
andbiplan
ewrist
motionim
prov
edexcept
for(1)case.
Overallscores:10
excellent
&4go
od.
Malun
ionwas
reop
erated
successfully
(1),refracture
after
fixa
torremov
alman
aged
conserva
tively
(1).
6 T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10

Tab
le2.
(con
tinu
ed).
Autho
r:Year[R
eference]O
perative
procedure
(forearm
s)Preop
erativeradiog
raph
yPostoperative
radiog
raph
ymPreop
erativeclinical
tools
Postoperative
clinical
outcom
emCom
plications
*
Masad
a:19
89[3]
Osteochon
drom
aexcision
(12ulna
s&
2radiuses),
grad
ualulna
rleng
thening
withexternal
fixa
tor(3)&
acutewithbo
negraft(10),
radial
osteotom
y(10),
distal
radius
hemiepiph
ysiodesis(2),
open
redu
ctionof
dislocated
radial
head
(2).
Rad
ialarticularan
gle,
carpal
slip,ulna
rshortening
.Relativeradial
shortening
was
measured
fortype
III
Ulnar
leng
thwas
restored
inallbu
ton
eforearm.Rad
ial
articularan
gle&
carpal
slip
improv
edin
allcases.
ROM
Forearm
rotation
improv
eddram
atically
inallcases.
Recurrenceof
ulna
rshortening
(2),prox
imal
radio-ulna
rsyno
stosis,
tran
sientradial
nerve
palsy(1
each).
Beutel:2
014[20]
Gradu
alulna
rleng
thening
withmultiplan
arexternal
fixa
tor(1).
Ulnar
shortening
,ulna
rbo
wing,
posterolateral
radial
head
near
dislocationwereseen.MRI
revealed
entrap
mentof
the
annu
larlig
amentwithin
theradiocap
itellarjoint,
osteocho
ndralim
paction
injuries
ofthean
terior
radial
head
,capitellu
m&
injuries
ofthean
terior
trochlea
andcorono
idprocess.
Ulnar
leng
th&
bow
wererestored
&radial
head
relocated.
MRIwas
notcond
ucted
postop
eratively.
ROM
&pa
inCom
pleterestorationof
elbo
wROM
&resolution
ofpa
in.
Forearm
was
unaffected
preoperatively.
Non
e
Hill:201
1[22]
#Osteochon
drom
aexcision
,grad
ualulna
rleng
thening
(proximal
diap
hyseal),
uniplana
r,multiplan
arIlizarov
orspatial/Ilizarov
hybrid
external
fixa
tor(5),
&op
enredu
ctionof
radial
head
withneck
osteotom
y(1).
Rad
ialarticularan
gle,
ulna
rshortening
,radial
head
dislocation
2dislocated
radial
head
sremainedso,1
dislocated
&1
sublux
edafter
initially
being
locatedan
d1
remainedlocated
before
&after
surgery.
Degreeof
deform
ity
was
recorded
pre&
postop
erativelybu
tNova
lues
orfina
lou
tcom
eswere
prov
ided
NR
Poo
rcallu
sregenerate
successfully
treated.
#
Litzelm
ann:20
12[7]
Inmild
deform
ity:
isolated
osteocho
ndromaexcision
(3radiuses).Isolated
radial
osteotom
ies(2).
Inmod
eratedeform
ity
typically
>11
yold:
corrective
distal
1/3radial
osteotom
ywithacute
ulna
rleng
thening+
bone
grafting
(3).In
severe
deform
ity:
grad
ualulna
rleng
theningov
er
Rad
ialarticularan
gle,
carpal
slip,radial
epiphy
seal
angle,
ulna
rva
rian
ce,radial
bowing&
radial
head
dislocation
assessed
byStoren
line.
Non
-significant
improv
ementof
all
radiolog
icpa
rameter
was
noted.
Twoof
the5dislocated
radial
head
spreoperatively
remainedso
postop
eratively.
ROM,pa
in,Patient-
repo
rted
function
alassessment:
QuickDASH
.
ROM
didno
tshow
statistically
sign
ificant
improv
ement.
One
out
ofthe3pa
tients
with
radial
head
instab
ility
&pa
inpreoperatively
remainedso
postop
erativelyan
drequ
ired
asuccessful
radial
head
resectionat
age17
years.
Revisionsurgeriesat
age17
yfordeform
ity
recurrence
(2)(1
radial
head
resection&
1radial
osteotom
y),
fracture
callu
sat
2yearspo
stop
erative(1).
T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10 7

Tab
le2.
(con
tinu
ed).
Autho
r:Year[R
eference]O
perative
procedure
(forearm
s)Preop
erativeradiog
raph
yPostoperative
radiog
raph
ymPreop
erativeclinical
tools
Postoperative
clinical
outcom
emCom
plications
*
Intram
edullary
pinat
diap
hyso-m
etap
hyseal
junction
,un
iplana
rexternal
fixa
tor(7)(4
with
radial
osteotom
y&
3with
osteocho
ndromaexcision
).
QuickDASH
.Sh
owed
asign
ificant
improv
ement.
Jiya
:199
7[11]
Isolated
osteocho
ndroma
excision
(4),
acuteulna
rleng
theningwithscrew
fixa
tion
,osteocho
ndroma
excision
(8),
+/−
radial
osteotom
y.
Linearax
is,radial
articular
angle,
carpal
slip,ulna
rshortening
Rad
ialarticular
angle,
carpal
slip
improv
edin
most
forearmsor
remained
unchan
ged.
Ulnar
shortening
was
frequent.
NR
(onlychief
complaintswere
recorded)
NR
Recurrenceof
ulna
rshortening
(5),
reop
erationfor
recurrentexostosis(1),
reop
erationfor
fracture/no
n-un
ionof
callu
sto
solid
union
(2).
Shin:200
6[10]
Isolated
osteocho
ndroma
excision
(11)
(6ulna
s&
5radiuses).Osteochon
drom
aexcision
&ulna
rleng
thening(4)(2
grad
ual
withun
iplana
rfixa
tor&
2acute),osteocho
ndroma
excision
withSa
uvé-
Kap
andjiprocedure(7).
Linearax
is,radial
articular
angle,
carpal
slip,ulna
rshortening
Isolated
osteocho
ndroma
excision
&ulna
rleng
thening:
statistically
non-
sign
ificant
improv
ement.
Sauv
é-Kap
andji:
Statistically
sign
ificant
improv
ement
ROM
inforearm
&elbo
wOsteochon
drom
aexcision
&ulna
rleng
thening:
statistically
non-
sign
ificant
improv
ement.
Sauv
é-Kap
andji:Statistically
sign
ificant
improv
ement
36.4
%recurrence
after
simpleosteocho
ndroma
excision
(allrequ
ired
reop
erations).Open
redu
ctionfor
persistently
symptom
atic
radial
head
dislocationafter
ulna
rleng
thening(2).
Reoperation
sfor
recurrent
osteocho
ndromaafter
Sauv
é-Kap
andji(2).
Rasoo
l:200
8[31]
One-bon
eforearm
(rad
ioulna
rfusion
)(2).
Rad
ialarticularan
gle,
carpal
slip
&ulna
rshortening
Residua
lulna
rshortening
inon
eforearm
ROM,grip
streng
thBothpa
tients
sign
ificantly
improv
edin
elbo
w,forearm
rotation
&grip
streng
th
Non
e
Pritchett:198
6[26]
Gradu
almid-diaph
yseal
ulna
rleng
thening,
uniplana
rexternal
fixa
tor
(6).Acute
ulna
rleng
thening(4)includ
ing
(2withiliac
crestgraft
andplatefixa
tion
&2ov
erRushrods).+/−
radial
osteotom
y(5).
Rad
ialarticularan
gle,
carpal
slip,relative
ulna
rshortening
,
Ofthe6sublux
ed/
dislocated
radial
head
spreoperative,5
becamestab
lepo
stop
erative.
ROM
ROM
improv
edin
most
forearms
Recurrenceof
ulna
rshortening
(6),
especially
child
ren&
youn
gad
olescents,
asym
ptom
atic
ulna
rno
n-un
ion&
deep
infection(1
each).
Massobrio:201
5[27]
Simultaneou
sgrad
ual
prox
imal
ulna
anddistal
radius
leng
theningwith
uniplana
rexternal
fixa
tor
(2).
Rad
ialarticularan
gle,
carpal
slip,ulna
rshortening
,relative
ulna
rshortening
&radial
leng
th
Sign
ificant
improv
ementin
all
measurements
Fun
ction,
ROM
&cosm
etic
Sign
ificant
improv
ementin
ROM
&function
Non
e
8 T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10
Tab
le2.
(con
tinu
ed).
Autho
r:Year[R
eference]O
perative
procedure
(forearm
s)Preop
erativeradiog
raph
yPostoperative
radiog
raph
ymPreop
erativeclinical
tools
Postoperative
clinical
outcom
emCom
plications
*
Kelly:201
6[28]
Distalradius
hemiepiph
ysiodesis(15).
Rad
ialarticularan
gle,
carpal
slip,ulna
rtilt,
luna
tesubsidence,
metap
hyseal
epiphy
seal
angle
Statistically
sign
ificant
improv
ementin
all5
measurements
except
luna
tesubsidence
NR
NR
Non
e
Ton
ogai:201
5[18]
Osteochon
drom
aexcision
&interosseous
mem
bran
edissection
,grad
ualulna
(2)
orradial
(1)leng
thening,
multiplan
arIlizarov
orun
iplana
rfixa
tor.
Rad
ialarticularan
gle,
ulna
rshortening
Improv
edROM
Improv
edNon
e
Refslan
d:20
16[14]
Gradu
almid-diaph
yseal
Ulnar
leng
theningwith
uniplana
rexternal
fixa
tor
(17),+/−
osteocho
ndroma
excision
(14),+/−
radial
osteotom
y(5).
Rad
ialarticularan
gle,
carpal
slip,radius
ofcurvature,
ulna
rva
rian
ce,
angleof
theradial
and
ulna
rph
yses,elbo
wcarrying
angle,
amou
ntof
radial
head
coverage
Statistically
sign
ificant
improv
ementin
radius
ofcurvature,
ulna
rva
rian
ce,
carrying
angle,
radial
head
coverage
ROM
&pa
inStatistically
non-
sign
ificant
improv
ement
inROM
&5pa
tients
who
hadpa
inpreoperative
hadno
pain
postop
erative.
Osteotomyfor
deform
ityrecurrence
(1),external
fixa
tor
failu
rerequ
iring
exchan
ge(2),
prem
atureconsolidation
(1).
Bau
er:201
7[17]
Gradu
alulna
leng
thening
(1).Com
binedulna
&radius
osteotom
ies(2)
Ang
ular
&rotation
aldeform
ityof
radius
&ulna
Statistically
sign
ificant
improv
ement
ROM
inrotation
Statistically
sign
ificant
improv
ement
Extensorpo
llicis
Lon
gusweakn
ess(1).
Yan
g:20
13[34]
Recon
structionof
the
distal
ulna
repiphy
sisby
vascularized
prox
imal
fibu
lawithepiphy
sis(2).
Rad
ialarticularan
gle,
carpal
slip
&relative
ulna
rshortening
Sign
ificant
improv
ement
(persistentbu
tasym
ptom
atic
radial
head
dislocation)
Fun
ction,
pain
ROM
&cosm
etic
Sign
ificant
improv
ement
Non
e
Bilen:20
09[23]
Osteochon
drom
aexcision
,grad
ualulna
rleng
thening
multiplan
ar(2)or
uniplana
r(6)external
fixa
tor+/−
radial
osteotom
y.Lengthening
was
Rushrods
guided
in(2)cases.
Rad
ialarticularan
gle,
carpal
slip
&ulna
rshortening
Sign
ificant
improv
ement&
all
radial
head
sthat
weredislocated
preoperative
were
redu
ced.
NR
Sign
ificant
improv
ementbu
tno
goniom
etric
measurements
cond
ucted
Non
e
Mad
er:200
3[40]
Osteochon
drom
aexcision
,grad
ualulna
rleng
thening,
uniplana
rfixa
tor(4).
Rad
ialarticularan
gle,
carpal
slip
&ulna
rshortening
Sign
ificant
improv
ement
ROM,function
.Sign
ificant
improv
ement
Non
e
Peterson:20
08[32]
One-bon
eforearm
(rad
ioulna
rfusion
)(1).
Previou
sresectionof
distal
ulna
&radial
head
dislocation
Restoration
offorearm
leng
thdiscrepa
ncy.
ROM
&stab
ility
inelbo
wSign
ificant
improv
ement
Non
e
Eralp:201
6[16]
Osteochon
drom
aexcision
,grad
ualmid-diaph
yseal
ulna
rleng
thening,
uniplana
rexternal
fixa
tor
Ulnar
shortening
,radial
bow
Restoration
ofulna
rshortening
&radial
bow.
Daily
lifeactivities
Sign
ificant
improv
ement
Recurrent
radial
deform
ity(1).
T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10 9
Tab
le2.
(con
tinu
ed).
Autho
r:Year[R
eference]O
perative
procedure
(forearm
s)Preop
erativeradiog
raph
yPostoperative
radiog
raph
ymPreop
erativeclinical
tools
Postoperative
clinical
outcom
emCom
plications
*
(4)(overSteinm
anin
2cases)
andcombined
radius
osteotom
y.W
aters:19
97[13]
Acute
ulna
rleng
thening
withplatefixa
tion
(17),
osteocho
ndromaexcision
(12)
&radial
osteotom
y(11).
ulna
rshortening
,ulna
rva
rian
ce,radial
inclination,
radial
articularan
gle,
carpal
slip
(AP
and
lateral),forearm-third
metacarpa
lan
gle,
status
ofossification
ofradial
&ulna
rph
yses,radial-head
sublux
ation&
cong
ruence
ofthedistal
radiou
lnar
joint.
Sign
ificant
improv
ement
ROM
Mostpa
tients
improv
edReoperation
swithbo
negraftforno
n/delayed
union&
brok
enplate
(3),prog
ressiveradial
head
sublux
ation(1),
annu
larlig
ament
reconstruction
(2),
chronicelbo
wpa
in(2),
creation
ofon
e-bo
neforearm
(1),repeat
leng
thening(2).
Ip:200
3[30]
Osteochon
drom
aexcision
,grad
ualulna
rleng
thening,
multiplan
aror
uniplana
rexternal
fixa
toror
acutely
withplating(6),
&radial
osteotom
y(5)ba
sedon
definite
radiog
raph
iccriteria.
Rad
ialarticularan
gle,
carpal
slip
&ulna
rshortening
,relative
ulna
shortening
Sign
ificant
improv
ement
ROM,subjective
simplequ
estion
naire
toassess
satisfaction
Sign
ificant
improv
ementin
ROM
&allpa
rentswere
satisfied
withfunction
&cosm
etic.
Rad
ialhead
dislocation
during
leng
thening(1)
was
successfully
redu
cedby
pin
stab
ilization
.
Song
:201
3[6]
Gradu
alulna
rleng
thening
withmultiplan
arexternal
fixa
tor&
mon
ofocal
ulna
rosteotom
y(13),+/−
radial
osteotom
y(5),
+/−
osteocho
ndroma
excision
(4).
Rad
ialarticularan
gle,
carpal
slip
&ulna
rshortening
,relative
ulna
shortening
Statistically
sign
ificant
improv
ements
&the
only
dislocated
radial
head
preoperative
was
redu
ced
postop
erative.
Subjective
qualityof
lifequ
estion
naire,
function
allim
itation
ofmotion&
pain
Mostpa
tients
were
satisfied
withforearm
appearan
ce,ha
dno
pain
onstrenu
ous
activities
&could
man
ageactivities
daily
lifeactivities
easily.
Recurrenceof
osteocho
ndroma&
deform
ity(2),delayed
union/
nonu
nion
(2).
Akita:200
7[8]
Isolated
osteocho
ndroma
excision
(13).
Osteochon
drom
aexcision
&ulna
rleng
thening(18)
(8grad
ualwithun
iplana
rexternal
fixa
tor&
10acute
withbo
negraft),+/−
grad
ualradial
leng
thening
(4),+/−
ulna
osteotom
y(2),+/−
radial
osteotom
y(14),+/−
open
redu
ction
radial
head
(2).
Rad
ialarticularan
gle,
carpal
slip
&ulna
varian
ceStatistically
non-
sign
ificant
improv
ementof
all
measurements
Subjective
qualityof
lifequ
estion
naire,
pain,ROM
&grip
streng
th
Statistically
non-
sign
ificant
improv
ement
inROM
&grip
streng
th.Mostpa
tients
werepa
infree
&ha
dno
restrictions
ofda
ilyactivities.
Unsatisfactorycosm
etic
appearan
ce(8).
Non
unionsuccessfully
treatedwithbo
negraft
andinternal
fixa
tion
(3),fracture
callu
s(2),
tempo
rary
radial
nerve
paresis(1)&
symptom
atic
radiocap
itellarjoint(2).
10 T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10
Tab
le2.
(con
tinu
ed).
Autho
r:Year[R
eference]O
perative
procedure
(forearm
s)Preop
erativeradiog
raph
yPostoperative
radiog
raph
ymPreop
erativeclinical
tools
Postoperative
clinical
outcom
emCom
plications
*
Matsuba
ra:200
6[24]
Osteochon
drom
aexcision
,grad
ualulna
rleng
thening,
uniplana
ror
multiplan
arexternal
fixa
tor(7),+/−
radial
osteotom
y(5),
+/−
grad
ualradius
leng
thening
(2).
Rad
ialarticularan
gle,
carpal
slip,ulna
varian
ce&
radial
bow.
Recurrenceof
ulna
rshortening
in(5)
cases.
The
other
measurements
improv
edmod
erately.
ROM
&pa
inSign
ificant
improv
ementin
pain
&forearm
rotation
except
onecase.
Recurrenceof
ulna
rshortening
(5)on
eof
which
was
releng
thened.
Rad
ialhead
sublux
ation
(1).
Ishika
wa:20
07[9]
Isolated
osteocho
ndroma
excision
(14)
(6from
distal
ulna
&8from
distal
ulna
+radius.
Rad
ialarticularan
gle,
carpal
slip,ulna
rshortening
,radial
leng
th,
radial
bowing.
Excisionfrom
distal
ulna
:statistically
sign
ificant
improv
ementin
ulna
rshortening
,radial
bow
only.
Excisionfrom
distal
ulna
+radius:no
n-sign
ificant
improv
ementan
d/or
deteriorationin
all
measurements.
NR
NR
Osteochon
drom
arecurrence
ofva
riou
sdegrees(7)(2
from
ulna
&5from
ulna
+radius).
Cheng
:199
1[25]
Gradu
alulna
rleng
thening
withun
iplana
rexternal
fixa
torwitho
utbo
negraft
(4).
Ulnar
leng
thon
lySa
tisfactory
corrected
ROM,cosm
etic
Non
-significant
improv
ementin
ROM,
butim
prov
edcosm
etic
&da
ilylifeactivities.
Non
e
Rod
gers:199
3[33]
One-bon
eforearm
(rad
ioulna
rfusion
)witha
pinor
plate(2),+/−
grad
ualleng
thening&
radial
osteotom
y(1).
Rad
ialarticularan
gle,
carpal
slip
&ulna
rshortening
Sign
ificant
improv
ementexcept
forresidu
alulna
rshortening
in(1)
case.
ROM,activities
ofda
ilylife
Satisfactory
inelbo
w&
wrist,returned
tofull-
timeman
ual
occupa
tion
/com
petitive
sports.
Non
e
Iran
i:199
3[43]
Isolated
osteocho
ndroma
excision
from
ulna
&radius
(8),
grad
ualulna
rleng
theningwithun
iplana
rfixa
tor(2)&
bone
graft
withplating+
radial
osteotom
y(1).
Ulnar
shortening
,&
radial
head
sublux
ation/
dislocation(3)
Relocated
&asym
ptom
atic
ROM
Noim
prov
ementin
forearm
rotation
Non
e
Fog
el:198
4[12]
Isolated
excision
ofthe
osteocho
ndromas
(ulnaor
radius)(12),acuteulna
rleng
thening&
excision
osteocho
ndroma(2),acute
ulna
rleng
thening,
excision
osteocho
ndroma,
&distal
radius
hemiepiph
ysiodesis
Rad
ialarticularan
gle,
carpal
slip
&ulna
rshortening
Isolated
excision
:no
improv
ementin
radial
articularan
gle
&carpal
slip.Ulnar
leng
thening&
excision
:no
improv
ement.
Ulna
leng
thening,
excision
&distal
radius
ROM,pa
in&
cosm
etic.
Isolated
excision
:no
improv
ementin
neither
rotation
norulna
rshortening
but
sign
ificant
improv
ement
inpa
in,no
osteocho
ndroma
recurrence.Ulnar
leng
thening&
excision
:
Non
e
T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10 11

Tab
le2.
(con
tinu
ed).
Autho
r:Year[R
eference]O
perative
procedure
(forearm
s)Preop
erativeradiog
raph
yPostoperative
radiog
raph
ymPreop
erativeclinical
tools
Postoperative
clinical
outcom
emCom
plications
*
(7).Fixations
werewith
plate/rush
rod,
+/−
bone
graft.
hemiepiph
ysiodesis:
sign
ificant
improv
ement.
noim
prov
ement.
Ulna
leng
thening,
excision
,&
distal
radius
hemiepiph
ysiodesis:
sign
ificant
improv
ement.
Arm
s:19
97[29]
∞Osteochon
drom
aexcision
s(36),radial-headexcision
s(6),distal
radius
hemiepiph
ysiodesis(5),
distal
radial
osteotom
ies
(2),an
dulna
rleng
thenings
withexternal
fixa
tors
(4).
Com
binedprocedures
performed
onasing
lepa
tientin
(11)
occasion
s.
Rad
ialarticularan
gle,
carpal
slip,relative
ulna
rshortening
,an
dforearm-
thirdmetacarpa
lan
gle.
Majorityof
patients
demon
strated
radiog
raph
icab
norm
alities
Telepho
nepa
tient-
repo
rted
question
naireof
qualityof
life
Majorityof
patients
werein
full-timejobs
withminim
alim
pact
onactivities
ofda
ilylife.
NR
Nnu
mber,NR
notrepo
rted,ROM
rang
eof
motionin
forearm
&elbo
w,+/−
wrist,VASvisual
analog
scale,
SF-12aqu
alityof
lifescalethat
measuresph
ysical
andmental
compo
nents,DASH
disabilitiesof
thearm,sho
ulderan
dha
ndscore.
mclinicorad
iologicresultsat
fina
lfollow-up;
*on
lysign
ificant
complications
weremention
ed;
†carpal
slip
couldno
tbe
measuredin
5casesbecausetheluna
tewas
poorly
ossified;
#meanag
ean
dfollo
w-up,
metho
dology
,outcomean
dcomplications
(exceptradial
head
status)wereprov
ided
for10
patients
withva
riou
sdiag
nosticgrou
psan
dthedetails
ofHMO
patients
wereno
tprov
ided
sepa
rately;
∞thestud
ycomprised
acoho
rtof
patients
treatedconserva
tively
andsurgically
37of
which
weresubjectedto
ateleph
onequ
estion
nairebu
tpa
tientdemog
raph
ics,
disease
characteristicsan
dintervention
swereno
tprov
ided
sepa
rately
forop
erated
grou
p.
12 T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10

T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10 13
surgical intervention expressed variability among studies.Restriction of daily activities and/or range of motion inforearm/elbow were the most common indications ofintervention. Most studies tended to favour objectivephysician-reported clinicoradiologic data as an outcomemeasure. Contrastingly, the majority of subjectivepatient-reported rating scales/questionnaires were non-validated and statistical significance was inadequatelyimplemented. One study [7] restricted the implementationof the patient-reported rating scale on the sub-category ofpatients subjected to gradual ulnar lengthening by anexternal fixator. This is seen as an effort to reduce theimpact of confounding variables. All studies employedplain radiography as a principal diagnostic tool. Twostudies [20,39] employed MRI as an adjuvant imagingmodality one of which [39] used CT scan and bonescintigraphy in addition. One study [27] employedultrasound to monitor callus progression. The vastmajority of studies assessed the radiographic outcome inaccordance with proposed measurements by Fogel andcolleagues which are a widely reported [12]. Five studies[6,9–11,41] used another referenced radiographic measure-ment by Burgess and Cates [42]. Among the variousradiographic measurements, radial articular angle, carpalslip, ulnar shortening, and radial head stability were themost commonly shared by included studies. Contrasting-ly, radial length was the least used measurement. Ulnarlengthening +/� an associated on demand procedure wasconducted on 210 forearms (66.7%) of the summednumber of forearms. Associated procedures included acombination of one or more of the following: angularcorrection, osteochondroma excision, corrective radialosteotomy distal radial hemiepiphysiodesis and openreduction of radial head. Of the 210 forearms (66.7%)subjected to ulnar lengthening, 145 forearms (69%) wereperformed gradually and 65 forearms (31%) were per-formed acutely mostly with bone grafting [3,7,8,10–13,26,30]. Of these later studies two used acute ulnarlengthening exclusively [12,13]. All “gradual” ulna length-enings were performed by a uniplanar fixator except in 17forearms (11.7%) a multiplanar fixator was used [6,19,20]and five studies with 22 forearms (15.2%) used bothuniplanar and multiplanar [18,22–24,30]. All ulnarlengthening osteotomies/cortectomies were performed ata mid or proximal diaphyseal level. One study employed asimultaneous radial and ulnar lengthening in one forearm[27] and three others (seven forearms) conducted isolatedradial lengthening as part of a series including ulnarlengthenings [8,18,24]. The vast majority of radialosteotomies were performed in association with ulnarlengthening procedures. Isolated corrective radial osteot-omies were done in two forearms (0.5%) only [7].
Isolated excision of osteochondroma or at least withoutbone lengtheningwas conducted on 65 forearms (20.6%) ofthe summed number of forearms [7–12]. Temporaryhemiepiphysiodesis of distal radial physis was performedon 29 forearms (9.2%) [3,12,28,29] one of which [28] 15forearms (4.8%) was exclusively devoted to hemiepiphy-siodesis. Sauvé-Kapandji procedure +/� osteochondroma
excision was performed on seven forearms (2.2%) [10].Creation one-bone forearm through radioulnar fusion waspracticed on five forearms (1.6%) [31–33] and reconstruc-tion of the distal ulnar epiphysis by vascularized proximalfibula including epiphysis was practiced on two forearms(0.5%) [34]. An open reduction of radial head +/� neckosteotomy was successfully performed on four forearms(1.3%) [3,10] and unsuccessfully on three forearms (1%)[8,22]. Resection of distal or proximal radioulnar synosto-sis was practiced on demand in two studies [15,21]. Radialhead excision was not practiced in pediatric patients atleast as a primary procedure. Proximal radio-ulnar fusionwas practiced on one forearm to manage symptomaticradial head subluxation [12]. The comparative prevalenceof the main interventions and techniques used in thisreview is demonstrated (Figures 2A, B, C). The overallcomplication rate was tolerable and showed no specificpredilection for any of the main interventions employed inthis review.
Missing data
The included studies had missing data related to thefollowing items: gender distribution (five studies)[10,11,16,28,29], number of forearms (one study) [29]and Masada subtype (seven studies) [12,17,22,25,26,28,29]. The overall skeletal burden of HMO wasreported in only four studies [11,16,33,43] and detailedin one [27]. Hand dominance was reported in only fourstudies [19,31,33,39] and 11 studies used pain as anoutcomemeasure. Previous surgeries were reported in fourstudies [13,16,27,32] and age of initial presentation in four[20,27,32,33]. Results of histopathologic examination werereported in six studies [16,20,24,27,34,41] and familyhistory in six [3,8,20,30,33,34]. No study reported genetictesting and physiotherapy protocols were either poorly ornot reported at all except for one study [22]. One study didnot report the follow-up period as it was primarilydesigned to assess the utility of a computer simulationmodel [17]. One study reported patient ethnicity [28]. Thestudy that practiced reconstruction of the distal ulnarepiphysis by vascularized proximal fibula did not reportdonor site morbidity [34]. One study reported conclusionsthat were discordant with the results [11]. The authorsunderscored the importance of ulnar lengthening inpreventing progressive deformity and minimising func-tional disability despite reporting frequent deformityrecurrence rates [11]. Grippingly, the authors employedneither objective nor subjective clinical outcomemeasures[11]. Generally speaking, we suggest that some of themissing data may have a potential impact on the validityof results and conclusions. For example failure to reportthe overall skeletal burden of HMO in terms of number andlocation and pain can influence the subjective patient-reported quality of life assessment [44–47]. Pain that wasgrossly underreported by the primary studies of thisreview has been found to be a major drive for surgery andnegatively influenced by surgery [47]. The incidence of apositive family history in patients with HMO has been

(A) (B) (C)
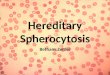
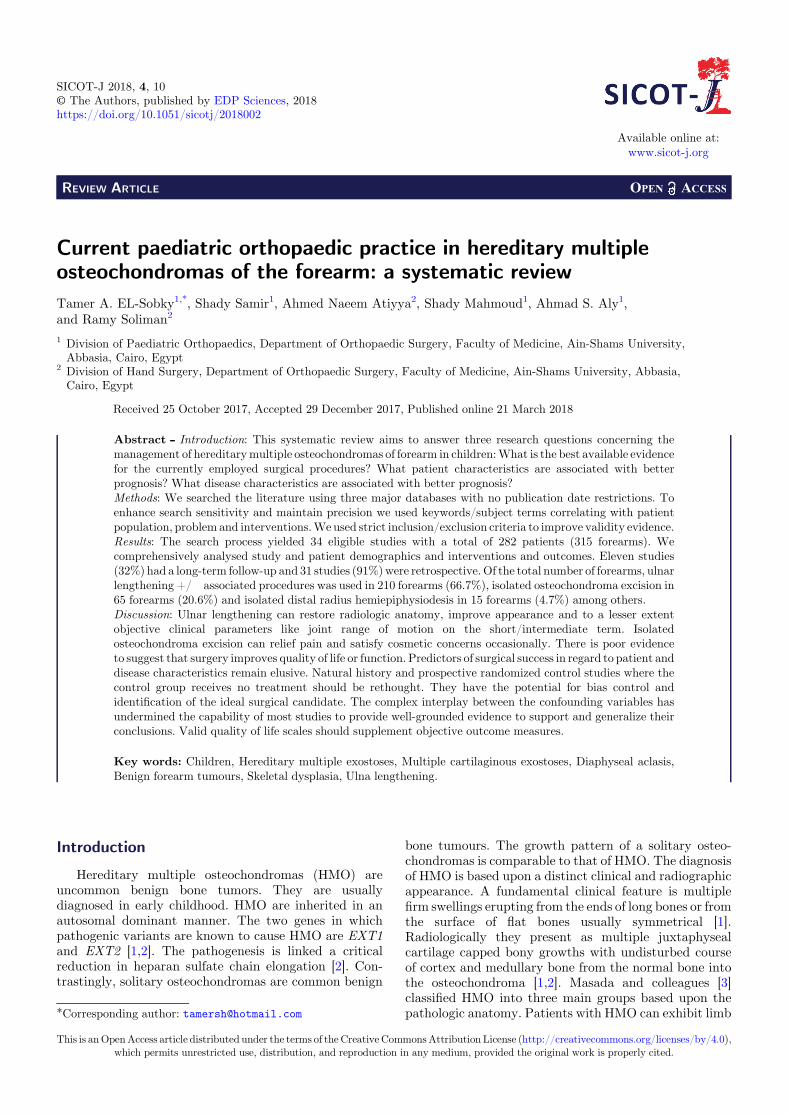
Figure 2. Comparative prevalence of the main interventions and techniques used in this review as percentages of forearms; (A) themain intervention groups used. Associated procedures include; osteochondroma excision, corrective radial osteotomy, distal radialhemiepiphysiodesis and open reduction of radial head. “Others” refers to isolated procedures as one-bone forearm, reconstruction of thedistal ulnar epiphysis by vascularized proximal fibula epiphysis, radial osteotomy and lengthening; (B) gradual versus acute ulnarlengthening; (C) fixator choice of included studies.
14 T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10
estimated to range from 62–96% [1]. Genotype-phenotypecorrelation studies demonstrated that certain types ofgene mutations and the overall skeletal burden of HMOare associated with a worse clinical presentation particu-larly with respect to deformity and function [1,2,44,45,48–50]. This may actually have a predetermined impact ontreatment outcomes.
DiscussionSummary of evidence
This systematic review included many chief surgicalinterventions each of which was multifaceted. For clarityand consensus, we will discuss each chief interventionseparately. We believe that this practical approach willassist in answering our first research question. The mostprevalent combination of surgical procedures encounteredin this review was ulnar lengthening, +/� an associatedprocedure. Generally speaking, this surgical technique wasadequately described and fairly constant across studieswith a tolerable complication rate on the short-term.Nevertheless, there is poor evidence to demonstrate thatthe seemingly satisfactory results of many short-termstudies are maintained on the intermediate-term [10] andmore precisely on the long-term [7,8]. These long-termrelatively sizable well-designed studies have questionedthe value of surgical intervention even in association withdeformity and radiographic abnormalities [7,8]. Thesestudies correlated the clinicoradiologic outcomes withpatients’ self- reported functional outcome measures inchildren operated for HMO of forearm and argued for thechoice of conservative treatment [7,8]. They foundinsufficient functional gains to justify surgery. In otherwords, preoperatively patients reported minimal func-
tional impairment despite major clinical and radiologicabnormalities [7,8]. The only exception was symptomaticradial head dislocation. This discrepancy between thefunctional capacity and amount of forearm deformity wascorroborated by three relatively sizable studies [22,24,29].These findings have been confirmed by a natural history ina large cohort of untreated adult subjects with HMO [35].
Generally speaking, most studies tended to focus on theradiographic outcome measures at the expense of objectiveclinical parameters. Likewise, the objective physician-reported clinical outcome measures were implemented atthe expense of the subjective patient-reported measureswhich were mostly non-validated and lacked in depth.Notwithstanding, these studies reported recognized cosmet-ic satisfaction of patients. Interestingly, in some studiespatients were selected for surgery exclusively based uponradiographic criteria while clinical (objective or subjective)outcome measures were neither reported before nor aftersurgery [9,11,22,28]. It is noteworthy that complicationssuch as recurrence of osteochondromas, and/or forearmdeformityneed longerdurations to resurface especially in theskeletally immature population [9,24]. This undoubtedlyoveremphasizes the significance of conducting long-termfollow-up studies and greatly undermines the quality ofevidence extracted from such short-term studies. Addition-ally, this critically calls attention to thevalueof thevalidatedsubjective patient-reported overall quality of life scales.Using these scales has shown that HMO patients had lowerscores compared to the general population [46,48]. Weunderstand that a comprehensive assessment of patients’outcomes entails both subjective patient-reported andobjective physician-reported instruments. In the light ofsuch observations, it is important to rethink the cost/benefitprofile of surgical intervention in paediatric HMO. In thatregard, retrospective natural history studies may refine the

T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10 15
wide and crude indications of surgery currently used inchildren withHMO.Two natural history studies are praisedfor aiming to identify radiographic predictors of radial headdislocation [4,51]. Likewise, well-designed randomizedcontrol studies where one group receives a definite surgicaltreatment and the other receives no treatment should berethought. To satisfy the ethical demands of such studies,strict inclusion/exclusion criteria will have to be imple-mented before enrolment and randomization. Besides,adequate patient orientation in regard to risks and benefitsof each treatment group and nature of the study will have toprecede enrolment and randomization. Such study designscan generally yield valid results and generalizable conclu-sions. Nevertheless, we acknowledge the logistic andpractical difficulties associated with such study designs.We believe that insufficient consensus about the indicationsof surgery and outcome scores in paediatric HMO is a majorlimitation of this systematic review. These discordantindications of surgery have also been noticed withinindividual study participants, further complicating evidenceextraction. Likewise, the heterogeneity of the surgicalprocedures used, diversity in patient characteristics andrelatively small study populations complicates evidenceextraction. These above-mentioned features are inherent toretrospective studies that constituted the majority ofincluded studies. Nonetheless, certain studies were remark-able for their methodologic quality. They implementedstudy designs that allow for control of selection andperformance bias [6,8,10]. They neatly and separatelyreported the results of HMO patients in accordance witheach distinct surgical procedure implemented. Additionally,some used assessor blinding methods and standardisedsurgeon related factors [6,8,10]. Isolated excision of osteo-chondroma can relief pain, satisfy cosmetic concerns andoccasionally improve range of motion. Nevertheless, there isinsufficient evidence for its use to initiate spontaneousdeformity correction or improve overall limb function. Inthis review the cases of radial hemiepiphysiodesis, one-boneforearm, vascularized fibular graft, isolated radial osteoto-mies or lengthenings practiced as “stand alone” procedureswere insufficiently prevalent to allow for meaningfulconclusions. These procedures may be better suited tospecificpatientprofiles andbasedupon surgeon’s preference.
Limitations and strengths
We acknowledge limitations of this review. Themajority of the included studies were of low methodologicquality. Studies with low methodologic quality mayimpact negatively on outcome validity and conclusions.Narrative/traditional reviews are usually biased andsubjective in contrast to systematic reviews which areoften unbiased and objective [52]. The reliability andaccuracy of systematic review recommendations shouldnot be determined by methodologic quality of the primarystudies included, but rather by the degree of methodologi-cal integrity implemented by researchers [52]. In thissystematic review we formulated focused research ques-tions that require specific answers. Additionally, we
implemented a comprehensive review methodology thatallowed for a reasonable control of bias. Therefore, weestimate that our comprehensive systematic reviewstrategy can counterbalance the shortcomings of includingstudies with low methodologic quality. Of the 18 studiesexcluded on basis of language 11were provisionally eligiblefor inclusion in this review. These 11 studies comprised 54forearms. It is noteworthy that in three of these 11 studiesthe size of study population could not be accounted for dueto missing or deficient abstracts. In general, the excludedstudies were comparable to the included studies in terms ofmethodology and individual sample size. Hence, theselanguage exclusions seem inconsequential.
Conclusions
Ulnar lengthening +/� associated procedures canrestore radiologic anatomy, improve appearance and to alesser extent objective clinical parameters on the short/intermediate term. There is Poor evidence to demonstratethatthesegainsaremaintainedonthe long-term.The impactof surgery on quality of life and function has not beenadequately investigated. Considerable evidence suggeststhat surgery minimally impacts preoperative function.Predictors of surgical success in regard to patient anddiseasecharacteristics remain elusive. The complex interplaybetween the arrays of confoundingvariables hasunderminedthe capability of most studies to provide well-groundedevidence to support and generalize their conclusions.
Recommendations
–
Comprehensive reporting of all actually and potentiallyrelevant patient and disease characteristics that providescope for determination of predictors of surgical successis prompted.–
Multicenter studies that allow for greater patientpopulations are encouraged because of disease rarity.–
Well-designed ethically tolerable prospective random-ized “control” trials in carefully selected patient popula-tion groups should be considered.–
Validated quality of life assessment scales should beincorporated into patients’ outcome measures.Conflict of interest
The authors Tamer A. EL-Sobky, Shady Samir,Ahmed Naeem Atiyya, Shady Mahmoud, Ahmad S. Alyand Ramy Soliman declare that they have no conflict ofinterest in connection with this article.
References
1. Guo XL, Deng Y, Liu HG (2014) Clinical characteristics ofhereditary multiple exostoses: a retrospective study ofmainland chinese cases in recent 23 years. J Huazhong UnivSci Technolog Med Sci 34, 42–50.
16 T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10
2. Jones KB (2011) Glycobiology and the growth plate:current concepts in multiple hereditary exostoses. J PediatrOrthop 31, 577–586.
3. Masada K, Tsuyuguchi Y, Kawai H, Kawabata H, NoguchiK, Ono K (1989) Operations for forearm deformity causedby multiple osteochondromas. J Bone Joint Surg Br 71, 24–29.
4. Gottschalk HP, Kanauchi Y, Bednar MS, Light TR (2012)Effect of osteochondroma location on forearm deformity inpatients with multiple hereditary osteochondromatosis. JHand Surg Am 37, 2286–2293.
5. Woodside JC, Ganey T, Gaston RG (2015) Multipleosteochondroma of the hand: initial and long-term follow-up study. Hand. New York, NY, 10, 616–620.
6. Song SH, Lee H, Youssef H, Oh SM, Park JH, Song HR(2013) Modified Ilizarov technique for the treatment offorearm deformities in multiple cartilaginous exostoses:case series and literature review. J Hand Surg Eur 38,288–296.
7. Litzelmann E, Mazda K, Jehanno P, Brasher C, PennecotGF, Ilharreborde B (2012) Forearm deformities in heredi-tary multiple exostosis: clinical and functional results atmaturity. J Pediatr Orthop 32, 835–841.
8. Akita S, Murase T, Yonenobu K, Shimada K, Masada K,Yoshikawa H (2007) Long-term results of surgery forforearm deformities in patients with multiple cartilaginousexostoses. J Bone Joint Surg Am 89, 1993–1999.
9. Ishikawa J, Kato H, Fujioka F, Iwasaki N, Suenaga N,Minami A (2007) Tumor location affects the results ofsimple excision for multiple osteochondromas in theforearm. J Bone Joint Surg Am 89, 1238–1247.
10. Shin EK, Jones NF, Lawrence JF (2006) Treatment ofmultiple hereditary osteochondromas of the forearm inchildren: a study of surgical procedures. J Bone Joint SurgBr 88, 255–260.
11. Jiya TU, Pruijs JE, van der Eijken JW (1997) Surgicaltreatment of wrist deformity in hereditary multipleexostosis. Acta Orthop Belg 63, 256–261.
12. Fogel GRT, McElfresh EC, Peterson HA, Wicklund PT(1984) Management of deformities of the forearm inmultiple hereditary osteochondromas. J Bone Joint SurgAm 66A, 670–680.
13. Waters PM, Van Heest AE, Emans J (1997) Acute forearmlengthenings. J Pediatr Orthop 17, 444–449.
14. Refsland S, Kozin SH, ZlotolowDA (2016)Ulnar distractionosteogenesis in the treatment of forearm deformities inchildren with multiple hereditary exostoses. J Hand SurgAm 41, 888–895.
15. D’Ambrosi R, Barbato A, Caldarini C, Biancardi E,Facchini RM (2016). Gradual ulnar lengthening in childrenwith multiple exostoses and radial head dislocation: resultsat skeletal maturity. J Child Orthop 10, 127–133.
16. Eralp L, Bilen FE, Rozbruch SR, Kocaoglu M, HammoudaAI (2016) External fixation reconstruction of the residualproblems of benign bone tumours. Strategies Trauma LimbReconstr 11, 37–49.
17. Bauer AS, Storelli DA, Sibbel SE, McCarroll HR, LattanzaLL (2017) Preoperative computer simulation and patient-specific guides are safe and effective to correct forearmdeformity in children. J Pediatr Orthop 37, 504–510.
18. Tonogai I, Takahashi M, Tsutsui T, Goto T, Hamada D,Suzue N, Matsuura T, Yasui N, Sairyo K (2015) Forearmlengthening by distraction osteogenesis: a report on 5 limbsin 3 cases. J Med Invest 62, 219–222.
19. Cho YJ, Jung ST (2014) Gradual lengthening of the ulna inpatients with multiple hereditary exostoses with a dis-located radial head. Yonsei Med J 55, 178–184.
20. Beutel BG, Klifto CS, Chu A (2014) Timing of forearmdeformity correction in a child with multiple hereditaryexostosis. Am J Orthop (Belle Mead NJ) 43, 422–425.
21. Vogt B, Tretow HL, Daniilidis K, Wacker S, Buller TC,Henrichs MP, Roedl RW, Schiedel F (2011) Reconstructionof forearm deformity by distraction osteogenesis in childrenwith relative shortening of the ulna due to multiplecartilaginous exostosis. J Pediatr Orthop 31, 393–401.
22. Hill RA, Ibrahim T, Mann HA, Siapkara A (2011) Forearmlengthening by distraction osteogenesis in children: a reportof 22 cases. J Bone Joint Surg Br 93, 1550–1555.
23. Bilen FE, Eralp L, Balci HI, Kocaoglu M, Ozger H (2009)Correction of forearm deformities in children with multipleosteochondroma, by corrective radial osteotomy and ulnarlengthening by distraction osteogenesis. Acta Orthop Belg75, 743–747.
24. Matsubara H, Tsuchiya H, Sakurakichi K, Yamashiro T,Watanabe K, Tomita K (2006) Correction and lengtheningfor deformities of the forearm in multiple cartilaginousexostoses. J Orthop Sci 11, 459–466.
25. Cheng JC (1991) Distraction lengthening of the forearm. JHand Surg Br 16, 441–445.
26. Pritchett JW (1986) Lengthening the ulna in patients withhereditarymultiple exostoses. J Bone Joint Surg Br 68, 561–565.
27. Massobrio M, Antonietti G, Pellicano G, Necci F (2015)Single forearm radius and ulna asymmetric lengthening inmultiple cartilaginous exostoses: a case report and a long-term follow-up. J Pediatr Orthop B 24, 561–566.
28. Kelly JP, James MA (2016) Radiographic outcomes ofhemiepiphyseal stapling for distal radius deformity dueto multiple hereditary exostoses. J Pediatr Orthop 36,42–47.
29. Arms DM, Strecker WB, Manske PR, Schoenecker PL(1997) Management of forearm deformity in multiplehereditary osteochondromatosis. J Pediatr Orthop 17,450–454.
30. Ip D, Li YH, Chow W, Leong JC (2003) Reconstruction offorearm deformities in multiple cartilaginous exostoses. JPediatr Orthop B 12, 17–21.
31. Rasool MN (2008) Radioulnar fusion for forearm defects inchildren � a salvage procedure. SA Orthop J 7 (1), 60–67.
32. Peterson HA (2008) The ulnius: a one-bone forearm inchildren. J Pediatr Orthop B 17, 95–101.
33. Rodgers WB, Hall JE (1993) One-bone forearm as a salvageprocedure for recalcitrant forearm deformity in hereditarymultiple exostoses. J Pediatr Orthop 13, 587–591.
34. Yang YF, Zhang GM, Huo ZQ, Xu ZH, Xu DC (2013)Reconstruction of the distal ulnar epiphysis with vascular-ized proximal fibula including epiphysis in children afterosteochondroma resection: report of two cases. PlastReconstr Surg 132, 784e–789e.
35. NoonanKJ, LevendaA, Snead J, Feinberg JR,MihA (2002)Evaluation of the forearm in untreated adult subjects withmultiple hereditary osteochondromatosis. J Bone Joint SurgAm 84A, 397–403.
36. Moher D, Liberati A, Tetzlaff J. Altman DG, PRISMAGroup (2004) (2009) Preferred reporting items for system-atic reviews and meta-analyses: the PRISMA statement.BMJ 21(339), b2535.
37. Centre for evidence-based medicine. [Internet]. [cited on2017 Aug 21]. Available from www.cebm.net/critical-appraisal
38. Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y,Chipponi J (2003) Methodological index for non-random-ized studies (MINORS): development and validation of anew instrument. ANZ J Surg 73, 712–716.

T.A. EL-Sobky et al.: SICOT-J 2018, 4, 10 17
39. Demir B, Gursu S, Ozturk K, Yildirim T, Konya MN, Er T(2011) Single-stage treatment of complete dislocation ofradial head and forearm deformity using distractionosteogenesis in paediatric patients having multiple cartilag-inous exostosis. Arch Orthop Trauma Surg 131, 1195–1201.
40. Mader K, Gausepohl T, Pennig D (2003) Shortening anddeformity of radius and ulna in children: correction of axisand length by callus distraction. J Pediatr Orthop B 12,183–191.
41. Tang ZW, Cao YL, Liu T, Chen T, Zhang XS (2013)Management of forearm deformities with ulnar shorteningmore than 15mm caused by hereditary multiple osteochon-dromas. Eur J Orthop Surg Traumatol 23, 611–618.
42. Burgess RC, Cates H (1993) Deformities of the forearm inpatients who have multiple cartilaginous exostosis. J BoneJoint Surg Am 75, 13–18.
43. Irani RN, Petrucelli RC (1993) Ulnar lengthening fornegative ulnar variance in hereditary multiple osteochon-dromas. J Pediatr Orthop B 1, 143–147.
44. BeltramiG, Ristori G, Scoccianti G, Tamburini A, CapannaR (2016) Hereditary multiple exostoses: a review of clinicalappearance and metabolic pattern. Clin Cases Miner BoneMetab 13, 110–118.
45. Clement ND, Porter DE (2014) Hereditary multipleexostoses: anatomical distribution and burden of exostosesis dependent upon genotype and gender. Scott Med J 59,35–44.
46. Chhina H, Davis JC, Alvarez CM (2012). Health-relatedquality of life in people with hereditary multiple exostoses. JPediatr Orthop 32, 210–214.
47. Darilek S, Wicklund C, Novy D, Scott A, Gambello M,Johnston D, Hecht J (2005) Hereditary multiple exostosisand pain. J Pediatr Orthop 25, 369–376.
48. Pacifici M (2017) Hereditary multiple exostoses: newinsights into pathogenesis, clinical complications, andpotential treatments. Curr Osteoporos Rep 15, 142–152.
49. Pedrini E, Jennes I, Tremosini M, Milanesi A, Mordenti M,Parra A, Sgariglia F, Zuntini M, Campanacci L, Fabbri N,Pignotti E, Wuyts W, Sangiorgi L (2011) Genotype-phenotype correlation study in 529 patients with multiplehereditary exostoses: identification of “protective” and “risk”factors. J Bone Joint Surg Am 93, 2294–2302.
50. Pei Y, Wang Y, Huang W, Hu B, Huang D, Zhou Y, Su P(2010) Novel mutations of EXT1 and EXT2 genes amongfamilies and sporadic cases with multiple exostoses. GenetTest Mol Biomarkers 14, 865–872.
51. Jo AR, Jung ST, Kim MS, Oh CS, Min BJ (2017) Anevaluation of forearm deformities in hereditary multipleexostoses: factors associated with radial head dislocationand comprehensive classification. J Hand Surg Am 42,292.e1–292.e8.
52. SambunjakD, FranićM(2012) Steps in the undertaking of asystematic review in orthopaedic surgery. Int Orthop 36,477–484.
Cite this article as: EL-Sobky TA, Samir S, Atiyya AN, Mahmoud S, Aly AS, Soliman R (2018) Current paediatric orthopaedicpractice in hereditary multiple osteochondromas of the forearm: a systematic review. SICOT-J, 4, 10.













![Effectiveness of Physiotherapy in the Improvement of the ... · physiotherapy, orthopaedic, rheumatology, paediatric or geriatric [11]. Restore the functionality after a hemarthrosis,](https://img.pdfslide.us/doc/110x75/5ff55fc1f1c5aa0545238982/effectiveness-of-physiotherapy-in-the-improvement-of-the-physiotherapy-orthopaedic.jpg)