Embed Size (px)
Citation preview

Neurosurg Focus / Volume 36 / January 2014
Neurosurg Focus 36 (1):E7, 2014
1
©AANS, 2014
Central retinal artery occlusion (CRAO) is an oph-thalmological emergency that can result in com-plete blindness in the affected eye if untreated.3,5,6,
17,29,38,41,42,45 It is a result of sudden cessation of circulation to the inner retinal layer, which is considered to be a part of the CNS. This condition was first described in 1859 by Albrecht von Graefe, a famous German ophthalmolo-gist known for his contributions in glaucoma and cataract treatment.44 Since then, there has been an abundant accu-mulation of literature regarding the disease.
Although the pathophysiological features of CRAO are well described in the literature, the natural history of this disease is poorly understood. Prolonged retinal ische-mia is usually irreversible, suggesting a grim prognosis if the occlusion is not corrected in a timely manner.38 In a matter of hours cellular hypoxia will ensue, with subse-quent necrosis if circulation is not restored. The central retinal artery is usually occluded by a thrombotic em-bolus (of internal carotid artery or cardiac origin, 15.5% of cases); a calcified embolus (commonly of diseased car-diac valve origin, 10.5% of cases); or cholesterol embolus (74.5% of cases) (Table 1).2,27,32 Other causes include sud-den narrowing of the arterial wall (hemorrhage into an atheromatous plaque) and inflammatory processes (arte-ritic CRAO) secondary to temporal arteritis.17 There is a
high association of CRAO with atherosclerosis, diabetes, and systemic hypertension.16
Epidemiology, Etiology, and PresentationThe true incidence of CRAO in the population is
unknown. One report estimated CRAO to occur in 1 per 10,000 outpatient visits.10 The department of ophthalmol-ogy at the Western Galilee–Nahariya Medical Center in Nahariya, Israel, estimated an incidence of acute CRAO (with a less than 48-hour onset) at that institution to be ap-proximately 0.85 per 100,000 per year or 1.13 per 10,000 outpatient visits.38 Of these patients, 1%–2% present with bilateral involvement. Men are more frequently affected than are women, and the average age at presentation is in the early 60s, with rare cases as early as in the 30s.1,38,40,42 Patients suffering from central retinal artery embolism have a 56% mortality rate over 9 years, compared with 27% for age-matched individuals without emboli.18 Life expectancy is 5.5 years postdiagnosis for patients with CRAO compared with 15.4 years for age-matched indi-viduals without CRAO.
Diagnosis is usually made based on clinical history and physical examination. Ninety percent of patients pre-sent with a complaint of acute, persistent, painless loss of vision. Some patients may report a history of amaurosis fugax lasting anywhere from seconds to several hours. Ophthalmoscopic examination may reveal diminished blood vasculature in the retina, retinal edema, pale optic disc, and a cherry red spot. Approximately 18.7% of the
Current endovascular treatment options for central retinal arterial occlusion: a review
NitiN AgArwAl, B.S.,1 NihAr B. gAlA, M.D.,1 rezA J. KAriMi, M.D.,1 roger e. turBiN, M.D.,2 ChirAg D. gANDhi, M.D.,1,3 AND ChArleS J. PreStigiACoMo, M.D.1,3,4
Departments of 1Neurological Surgery, 2Ophthalmology and Visual Science, 3Radiology, and 4Neurology and Neuroscience, Rutgers New Jersey Medical School, Newark, New Jersey
Central retinal artery occlusion, although relatively rare, is an ophthalmological emergency. If left untreated, complete blindness will ensue. Conventional therapies have not significantly improved outcomes compared with the natural history of the disease. Several case series of more recent endovascular approaches, such as intraarterial fibrinolysis, report successful outcomes. Still other studies regarding intraarterial fibrinolysis do not demonstrate any significantly better outcomes, with some even indicating increased complication rates. Therefore, the authors present a review of the current endovascular treatment options for central retinal artery occlusion.(http://thejns.org/doi/abs/10.3171/2013.11.FOCUS13331)
Key worDS • central retinal arterial occlusion • treatment • endovascular • fibrinolysis
1
Abbreviations used in this paper: CRAO = central retinal artery occlusion; EAGLE = European Assessment Group for Lysis in the Eye; IAF = intraarterial fibrinolysis; IOP = intraocular pressure; rt-PA = recombinant tissue plasminogen activator.
Unauthenticated | Downloaded 06/01/20 07:10 PM UTC
N. Agarwal et al.
2 Neurosurg Focus / Volume 36 / January 2014
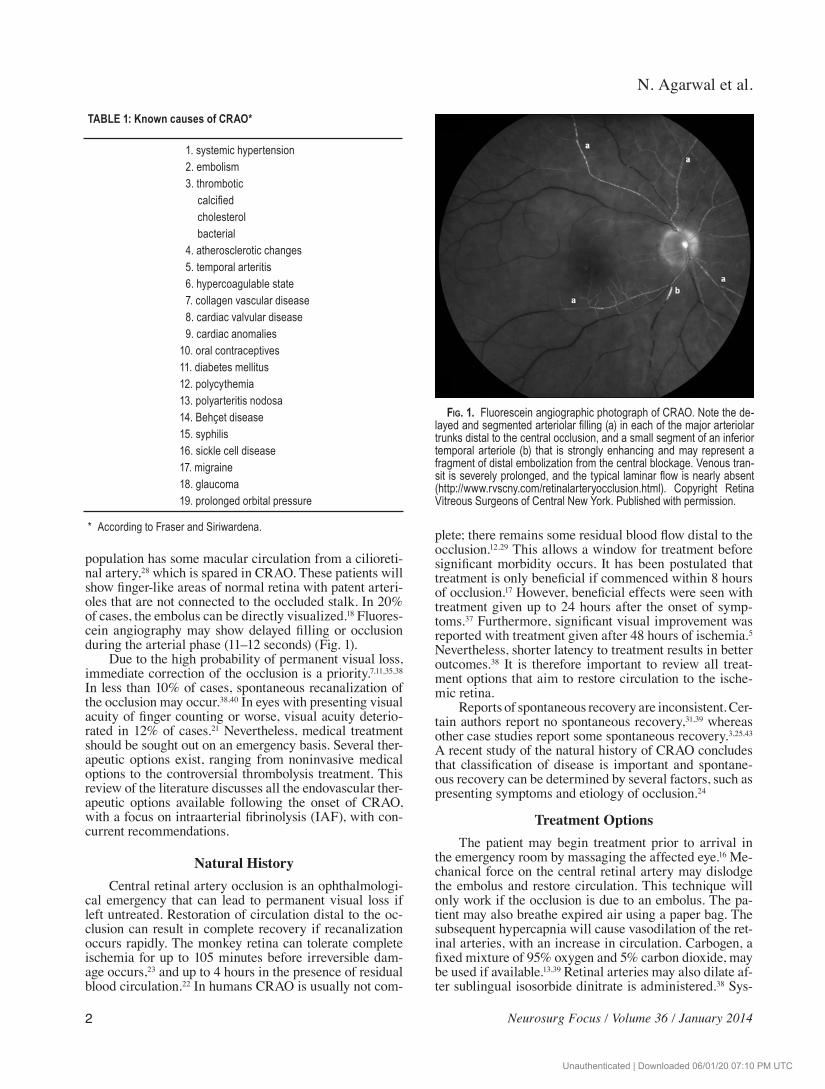
population has some macular circulation from a cilioreti-nal artery,28 which is spared in CRAO. These patients will show finger-like areas of normal retina with patent arteri-oles that are not connected to the occluded stalk. In 20% of cases, the embolus can be directly visualized.18 Fluores-cein angiography may show delayed filling or occlusion during the arterial phase (11–12 seconds) (Fig. 1).
Due to the high probability of permanent visual loss, immediate correction of the occlusion is a priority.7,11,35,38 In less than 10% of cases, spontaneous recanalization of the occlusion may occur.38,40 In eyes with presenting visual acuity of finger counting or worse, visual acuity deterio-rated in 12% of cases.21 Nevertheless, medical treatment should be sought out on an emergency basis. Several ther-apeutic options exist, ranging from noninvasive medical options to the controversial thrombolysis treatment. This review of the literature discusses all the endovascular ther-apeutic options available following the onset of CRAO, with a focus on intraarterial fibrinolysis (IAF), with con-current recommendations.
Natural HistoryCentral retinal artery occlusion is an ophthalmologi-
cal emergency that can lead to permanent visual loss if left untreated. Restoration of circulation distal to the oc-clusion can result in complete recovery if recanalization occurs rapidly. The monkey retina can tolerate complete ischemia for up to 105 minutes before irreversible dam-age occurs,23 and up to 4 hours in the presence of residual blood circulation.22 In humans CRAO is usually not com-
plete; there remains some residual blood flow distal to the occlusion.12,29 This allows a window for treatment before significant morbidity occurs. It has been postulated that treatment is only beneficial if commenced within 8 hours of occlusion.17 However, beneficial effects were seen with treatment given up to 24 hours after the onset of symp-toms.37 Furthermore, significant visual improvement was reported with treatment given after 48 hours of ischemia.5 Nevertheless, shorter latency to treatment results in better outcomes.38 It is therefore important to review all treat-ment options that aim to restore circulation to the ische-mic retina.
Reports of spontaneous recovery are inconsistent. Cer-tain authors report no spontaneous recovery,31,39 where as other case studies report some spontaneous recov ery.3,25,43 A recent study of the natural history of CRAO concludes that classification of disease is important and spontane-ous recovery can be determined by several factors, such as presenting symptoms and etiology of occlusion.24
Treatment OptionsThe patient may begin treatment prior to arrival in
the emergency room by massaging the affected eye.16 Me-chanical force on the central retinal artery may dislodge the embolus and restore circulation. This technique will only work if the occlusion is due to an embolus. The pa-tient may also breathe expired air using a paper bag. The subsequent hypercapnia will cause vasodilation of the ret-inal arteries, with an increase in circulation. Carbogen, a fixed mixture of 95% oxygen and 5% carbon dioxide, may be used if available.13,39 Retinal arteries may also dilate af-ter sublingual isosorbide dinitrate is administered.38 Sys-
TABLE 1: Known causes of CRAO*
1. systemic hypertension 2. embolism 3. thrombotic calcified cholesterol bacterial 4. atherosclerotic changes 5. temporal arteritis 6. hypercoagulable state 7. collagen vascular disease 8. cardiac valvular disease 9. cardiac anomalies10. oral contraceptives11. diabetes mellitus12. polycythemia13. polyarteritis nodosa14. Behçet disease15. syphilis16. sickle cell disease17. migraine18. glaucoma19. prolonged orbital pressure
* According to Fraser and Siriwardena.
Fig. 1. Fluorescein angiographic photograph of CRAO. Note the de-layed and segmented arteriolar filling (a) in each of the major arteriolar trunks distal to the central occlusion, and a small segment of an inferior temporal arteriole (b) that is strongly enhancing and may represent a fragment of distal embolization from the central blockage. Venous tran-sit is severely prolonged, and the typical laminar flow is nearly absent (http://www.rvscny.com/retinalarteryocclusion.html). Copyright Retina Vi treous Surgeons of Central New York. Published with permission.
Unauthenticated | Downloaded 06/01/20 07:10 PM UTC

Neurosurg Focus / Volume 36 / January 2014
Central retinal arterial occlusion treatments
3
temic vasodilation may occur, causing decreased blood pressure.
Immediate reduction of intraocular pressure (IOP) may cause an increase in ocular perfusion pressure and therefore circulation as well. This may be attempted with intravenous or oral acetazolamide, a carbonic anhydrase inhibitor.36 Mannitol may act as an osmotic diuretic and may also be used to reduce IOP. Anterior chamber para-centesis of aqueous humor3 and trabeculectomy19 are al-ternative methods for reducing IOP. Systemic steroids may be used to reduce vascular endothelial edema.20 Pentoxifylline has been shown to increase red blood cell deformability, allowing easier passage through capillaries and less ischemia in CRAO.26,30
Despite the various options, a retrospective study of 178 patients showed no significant benefit in conventional conservative methods.41 Several other series suggest a low success rate with conservative treatment.5,14,31 The current thrombolytic approach, known as IAF, consists of local infusion of urokinase or recombinant tissue plasminogen activator (rt-PA) at the site of occlusion via catheteriza-tion of the ophthalmic artery. The thrombolytic agent of choice is rt-PA, due to the shorter half-life and lower risks for complications. A meta-analysis of all previous litera-ture regarding IAF in cases of CRAO from 2000 suggests marginal visual benefit compared with conventional ther-apy (Table 2).6 However, the evidence was not enough to recommend IAF in the treatment of CRAO. In the afore-mentioned retrospective study of 178 patients, 62 patients with CRAO were treated with IAF in which urokinase or rt-PA was used, and were compared with 116 controls treated using conservative methods.41 Those treated with IAF had a greater chance of better outcome than those treated conservatively. Another series of 56 patients con-cluded that IAF enhanced the chances of improvement compared with conservative treatment.1 In that study, 8 of 37 patients treated with IAF regained visual acuity of greater than 0.6 compared with none in the control group.
Although IAF seemed very promising with such abundant support in the literature, randomized controlled clinical trials were needed before recommendations re-garding the use of IAF in treatment of acute CRAO could be made. The European Assessment Group for Lysis in the Eye (EAGLE) started a prospective and randomized multicenter study in 2002 to evaluate the efficacy of IAF.15 Patients between the ages of 18 and 75 years who had acute CRAO of less than 20 hours’ onset and presenting visual acuity of less than 0.32 were included in the study. Exclu-
sion criteria included presence of branched retinal artery occlusion, cilioretinal artery, elevated IOP greater than 30 mm Hg, or severe general medical disease. Patients were randomly assigned into IAF treatment or control groups. Patients in the treatment group received a total of 50 mg rt-PA injected locally into the ophthalmic artery. Control patients received conservative therapy including massage of the eye, topical beta-blocker, acetazolamide, aspirin, heparin, and isovolemic hemodilution. All patients were treated with heparin postprocedure for 5 days. The pri-mary end point was the best corrected visual acuity as-sessed 1 month after the procedure. A recent European article states that the study was halted after the first inter-im analysis because similar outcomes were seen in both groups, with an increased risk of complication in the IAF group.46 The investigators concluded that IAF cannot be recommended in treatment of acute CRAO. Of 37 patients treated with IAF, 3 (2 with transient ischemic attacks and 1 with stroke) developed periprocedural cerebrovascular ischemic events.1 Another study reports 2 patients endur-ing complications (transient aphasia and hemiparesis) with IAF treatment.41
For IAF to prove its role in the treatment of acute CRAO, the risk of complications must be reduced. This may be done through more optimal thrombolytic infusion methods, use of a thrombolytic agent with shorter half-life, or with a more experienced neurointerventionalist. Although discouraging, the hope for better results with the EAGLE study lies in the improvement of the IAF pro-tocol.
Future DirectionsClearly, the risk of complications of IAF in the treat-
ment of acute CRAO must be reduced. Still, a study by Margo and Mack33 revealed that 39% and 37% of sur-veyed adults would accept some risk of stroke and death, respectively, to triple the chances of recovering 20/100 vi-sual acuity in one eye when binocular. Even more (80%) would accept these risks if they were monocular. A survey by Atkins et al.4 demonstrated that despite limited evi-dence, a majority of US neuroophthalmologists continue to administer various conservative treatments, includ-ing ocular massage, topical drops to reduce IOP, anterior chamber paracentesis, antiplatelet agents, and anticoagu-lation. Moreover, thrombolytic agents were recommended by 23% of physicians.
Therefore, despite potential complications, the need for a well-designed randomized, controlled, double-blind
TABLE 2: Studies regarding efficacy of IAF in CRAO
Authors & Year No. of Patients Thrombolytic Therapy Outcome Study Type
Beatty & Au Eong, 2000 100 urokinase, streptoki- nase, rt-PA
final acuity 20/20 in 14%; 10/20 in 27%; 1/20 or worse in 60.6%
meta-analysis of 16 studies
Schmidt et al., 2002 178 urokinase, rt-PA partial or greater improvement seen in 58% treated w/ IAF compared to 29% treated conservatively
case series
Arnold et al., 2005 56 urokinase final acuity 12/20 or greater in 22% treated w/ IAF compared to 0% treated conservatively
case series
Unauthenticated | Downloaded 06/01/20 07:10 PM UTC

N. Agarwal et al.
4 Neurosurg Focus / Volume 36 / January 2014
clinical trial evaluating the effect of thrombolysis in CRAO continues to be considered. However, as echoed by Biousse,8 the first step toward a multicenter trial may be forming a consensus on treatment protocols. Evaluations of patients with acute CRAO before and after intervention must be conducted, with organization of pilot data into an international registry. Meanwhile, alternative thera-peutic strategies for CRAO should also be considered. To this end, given the efficacy of intravenous rt-Pa for fibrin-platelet clot lysis in ischemic stroke and myocardial in-farction, the role of systemic rt-Pa has also been explored for CRAO.34 In a systematic review of 103 cases of acute CRAO, Biousse et al.9 reported a 48.5% improvement of at least 3 lines of visual acuity. Ultimately, given that the treatment window probably does not exceed 6–12 hours, developing quick transportation modalities for patients to emergency departments is essential. For now, heightened patient awareness and physician collaboration with emer-gency rooms, stroke units, and interventionists is encour-aged.
ConclusionsThere is an abundance of literature regarding treat-
ment options for CRAO. Conservative therapy has been used for decades with variable success, but it has not been shown to improve outcomes significantly compared with no treatment. A recent endovascular approach involved IAF with urokinase or rt-PA. Several series report suc-cessful outcomes in patients treated with IAF; however, a recent prospective randomized controlled multicenter clinical study has not yet shown significantly better out-comes. Attention must be given to reduction and/or better management of complications associated with IAF as well as more optimal infusion methods. Given the current evi-dence, IAF cannot yet be recommended for the treatment of acute CRAO.
Disclosure
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
Author contributions to the study and manuscript prepara-tion include the following. Conception and design: Prestigiacomo, Agarwal, Gala. Acquisition of data: Agarwal, Gala. Analysis and interpretation of data: Agarwal, Gala. Drafting the article: Agarwal, Gala. Critically revising the article: Agarwal, Gala, Karimi, Turbin, Gandhi. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Pres tigiacomo. Statistical analysis: Agarwal. Administrative/tech-nical/material support: Prestigiacomo, Gandhi. Study supervision: Pres tigiacomo.
References
1. Arnold M, Koerner U, Remonda L, Nedeltchev K, Mattle HP, Schroth G, et al: Comparison of intra-arterial thrombolysis with conventional treatment in patients with acute central reti-nal artery occlusion. J Neurol Neurosurg Psychiatry 76:196–199, 2005
2. Arruga J, Sanders MD: Ophthalmologic findings in 70 patients with evidence of retinal embolism. Ophthalmology 89:1336–1347, 1982
3. Atebara NH, Brown GC, Cater J: Efficacy of anterior chamber paracentesis and Carbogen in treating acute nonarteritic cen-
tral retinal artery occlusion. Ophthalmology 102:2029–2035, 1995
4. Atkins EJ, Bruce BB, Newman NJ, Biousse V: Translation of clinical studies to clinical practice: survey on the treatment of central retinal artery occlusion. Am J Ophthalmol 148:172–173, 2009
5. Augsburger JJ, Magargal LE: Visual prognosis following treat-ment of acute central retinal artery obstruction. Br J Ophthal-mol 64:913–917, 1980
6. Beatty S, Au Eong KG: Local intra-arterial fibrinolysis for acute occlusion of the central retinal artery: a meta-analysis of the published data. Br J Ophthalmol 84:914–916, 2000
7. Beiran I, Reissman P, Scharf J, Nahum Z, Miller B: Hyperbaric oxygenation combined with nifedipine treatment for recent-onset retinal artery occlusion. Eur J Ophthalmol 3:89–94, 1993
8. Biousse V: Thrombolysis for acute central retinal artery occlu-sion: is it time? Am J Ophthalmol 146:631–634, 2008
9. Biousse V, Calvetti O, Bruce BB, Newman NJ: Thrombolysis for central retinal artery occlusion. J Neuroophthalmol 27: 215–230, 2007
10. Brown GC: Retinal arterial obstructive disease, in Schachat AP, Murphy RB, Patz A (eds): Medical Retina. Retina, Vol 2. St. Louis: CV Mosby, 1989, pp 1361–1377
11. Chen JC, Cheema D: Repeated anterior chamber paracentesis for the treatment of central retinal artery occlusion. Can J Ophthalmol 29:207–209, 1994
12. David NJ, Norton EW, Gass JD, Beauchamp J: Fluorescein an-giography in central retinal artery occlusion. Arch Ophthal-mol 77:619–629, 1967
13. Deutsch TA, Read JS, Ernest JT, Goldstick TK: Effects of oxy-gen and carbon dioxide on the retinal vasculature in humans. Arch Ophthalmol 101:1278–1280, 1983
14. Duker JS, Sivalingam A, Brown GC, Reber R: A prospective study of acute central retinal artery obstruction. The incidence of secondary ocular neovascularization. Arch Ophthalmol 109:339–342, 1991
15. Feltgen N, Neubauer A, Jurklies B, Schmoor C, Schmidt D, Wanke J, et al: Multicenter study of the European Assessment Group for Lysis in the Eye (EAGLE) for the treatment of cen-tral retinal artery occlusion: design issues and implications. EAGLE Study report no. 1: EAGLE Study report no. 1. Grae-fes Arch Clin Exp Ophthalmol 244:950–956, 2006
16. Ffytche TJ: A rationalization of treatment of central retinal ar-tery occlusion. Trans Ophthalmol Soc U K 94:468–479, 1974
17. Fraser S, Siriwardena D: Interventions for acute non-arteritic central retinal artery occlusion. Cochrane Database Syst Rev (1):CD001989, 2002
18. Graham RH, Ebrahim SA: Central retinal artery occlusion. Medscape. (http://emedicine.medscape.com/article/1223625-overview) [Accessed November 20, 2013]
19. Harvey PA, Winder S, Talbot JF: Trabeculectomy for central retinal artery occlusion. Eye (Lond) 14:256–257, 2000
20. Hausmann N, Richard G: Effect of high dose steroid bolus on occlusion of ocular central artery: angiographic study. BMJ 303:1445–1446, 1991
21. Hayreh SS: Acute retinal arterial occlusive disorders. Prog Re-tin Eye Res 30:359–394, 2011
22. Hayreh SS: Retinal arterial occlusion with LIF using rTPA. Ophthalmology 106:1236–1239, 1999
23. Hayreh SS, Kolder HE, Weingeist TA: Central retinal artery occlusion and retinal tolerance time. Ophthalmology 87:75–78, 1980
24. Hayreh SS, Zimmerman MB: Central retinal artery occlusion: visual outcome. Am J Ophthalmol 140:376–391, 2005
25. Humphrey WT: Central retinal artery spasm. Ann Ophthal-mol 11:877–881, 1979
26. Iwafune Y, Yoshimoto H: Clinical use of pentoxifylline in haemorrhagic disorders of the retina. Pharmatherapeutica 2: 429–438, 1980
Unauthenticated | Downloaded 06/01/20 07:10 PM UTC

Neurosurg Focus / Volume 36 / January 2014
Central retinal arterial occlusion treatments
5
27. Jenkins HS, Marcus DF: Central retinal artery occlusion. JA-CEP 8:363–367, 1979
28. Justice J Jr, Lehmann RP: Cilioretinal arteries. A study based on review of stereo fundus photographs and fluorescein angio-graphic findings. Arch Ophthalmol 94:1355–1358, 1976
29. Karjalainen K: Occlusion of the central retinal artery and reti-nal branch arterioles. A clinical, tonographic and fluorescein angiographic study of 175 patients. Acta Ophthalmol Suppl 109:1–95, 1971
30. Kieswetter H, Körber N, Jung F, Reim M: Rheologic findings in patients with acute central retinal artery occlusion. Graefes Arch Clin Exp Ophthalmol 220:92–95, 1983
31. Lorentzen SE: Occlusion of the central retinal artery. A follow-up. Acta Ophthalmol (Copenh) 47:690–703, 1969
32. Mangat HS: Retinal artery occlusion. Surv Ophthalmol 40: 145–156, 1995
33. Margo CE, Mack WP: Therapeutic decisions involving dispa-rate clinical outcomes: patient preference survey for treatment of central retinal artery occlusion. Ophthalmology 103:691–696, 1996
34. National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group: Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 333:1581–1587, 1995
35. Perkins SA, Magargal LE, Augsburger JJ, Sanborn GE: The idling retina: reversible visual loss in central retinal artery ob-struction. Ann Ophthalmol 19:3–6, 1987
36. Rassam SM, Patel V, Kohner EM: The effect of acetazolamide on the retinal circulation. Eye (Lond) 7:697–702, 1993
37. Richard G, Lerche RC, Knospe V, Zeumer H: Treatment of retinal arterial occlusion with local fibrinolysis using recombi-nant tissue plasminogen activator. Ophthalmology 106:768–773, 1999
38. Rumelt S, Dorenboim Y, Rehany U: Aggressive systematic treatment for central retinal artery occlusion. Am J Ophthal-mol 128:733–738, 1999
39. Schmetterer L, Lexer F, Findl O, Graselli U, Eichler HG, Wolzt M: The effect of inhalation of different mixtures of O2 and
CO2 on ocular fundus pulsations. Exp Eye Res 63:351–355, 1996
40. Schmidt D, Schumacher M, Wakhloo AK: Microcatheter uro-kinase infusion in central retinal artery occlusion. Am J Oph-thalmol 113:429–434, 1992
41. Schmidt DP, Schulte-Mönting J, Schumacher M: Prognosis of central retinal artery occlusion: local intraarterial fibrinolysis versus conservative treatment. AJNR Am J Neuroradiol 23: 1301–1307, 2002
42. Schumacher M, Schmidt D, Wakhloo AK: Intra-arterial fibri-nolytic therapy in central retinal artery occlusion. Neuroradi-ology 35:600–605, 1993
43. Shimizu K, Numaga J, Takahashi M, Matsunaga T: [A case of Sneddon syndrome.] Nippon Ganka Gakkai Zasshi 99:104–108, 1995 (Jpn)
44. Von Graefe A: Über Embolie der Arteria centralis retinae als Ursache plötzlicher Erblindung. Graefes Arch Ophthalmol 5:136–185, 1859
45. Weber J, Remonda L, Mattle HP, Koerner U, Baumgartner RW, Sturzenegger M, et al: Selective intra-arterial fibrinolysis of acute central retinal artery occlusion. Stroke 29:2076–2079, 1998
46. Wolf A, Schumacher M, Neubauer AS, Schmoor C, Gall C, Jurklies B, et al: [Comparison of superselective intraarterial fi-brinolysis with conservative therapy. Use in patients with acute non-arteritic central retinal artery occlusion.] Ophthalmologe 107:799–805, 2010 (Ger)
Manuscript submitted August 11, 2013.Accepted November 6, 2013.Please include this information when citing this paper: DOI:
10.3171/2013.11.FOCUS13331.Address correspondence to: Charles J. Prestigiacomo, M.D., 90
Bergen St., Ste. 8100, P.O. Box 1709, Newark, NJ 07101-1709. email: [email protected].
Unauthenticated | Downloaded 06/01/20 07:10 PM UTC





























