Embed Size (px)
Citation preview

Current Drug Targets, 2010, 11, 1571-1585 1571
1389-4501/10 $55.00+.00 © 2010 Bentham Science Publishers Ltd.
The Heme-Heme Oxygenase System in Wound Healing; Implications for Scar Formation
Frank A.D.T.G. Wagener*,1,2,†, Alwin Scharstuhl2,†, Rex M. Tyrrell3, Johannes W. Von den Hoff1, Alicja Jozkowicz4, Jozef Dulak4, Frans G.M. Russel2 and Anne Marie Kuijpers-Jagtman1
1Department of Orthodontics and Oral Biology, 2Department of Pharmacology and Toxicology, Nijmegen Centre for Molecular Life Sciences, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands, 3Department of Pharmacy and Pharmacology, University of Bath, Bath, UK, 4Department of Medical Biotechnology, Faculty of Biochemistry, Biophysics and Biotechnology, Jagiellonian University, Krakow, Poland
Abstract: Wound healing is an intricate process requiring the concerted action of keratinocytes, fibroblasts, endothelial cells, and macrophages. Here, we review the literature on normal wound healing and the pathological forms of wound healing, such as hypertrophic or excessive scar formation, with special emphasis on the heme-heme oxygenase (HO) system and the versatile effector molecules that are formed after HO-mediated heme degradation. Excessive scar formation following wounding is thought to relate to prolonged oxidative and inflammatory stress in the skin. Evidence is accumulating that the heme-HO system forms a novel and important target in the control of wound healing. Heme-protein derived heme can act as a potent oxidative and inflammatory stress inducer, and excess levels of heme may thus contribute to delayed resolution of oxidative and inflammatory insults in the skin. This emphasizes the need for a timely reduction of the levels of heme. Heme-binding proteins, heme transporters, and the heme degrading protein, HO, form therefore a necessary defense. Deficiencies in these defense proteins or a disturbed redox status, as in diabetic patients, may render individuals more prone to heme-induced deleterious effects. A better understanding of the heme-heme oxygenase system as target during wound healing may result in novel strategies to reduce scar formation.
Keywords: Heme, wound healing, scar formation, inflammation, heme oxygenase, (myo)-fibroblasts.
INTRODUCTION
Wounds and other tissue injuries can be caused by a great variety of circumstances, including surgery, burns, and ischemia-reperfusion. The healing process varies depending on the severity of the causative agent. In this review we describe the physiological changes during the normal healing in the skin. Attention is also paid to pathological healing with special reference to excessive and hypertrophic scar formation and the role of heme as a possible pathological factor in this process. Special situations in this respect regarding diabetes and the role of angiogenesis are reviewed. Subsequently the possibility to counteract the process of excessive scarring by influencing the heme-heme-oxygenase (HO) system is considered.
PHYSIOLOGY OF WOUND HEALING
The skin consists of an epidermal and a dermal layer separated by the lamina basalis, and forms a versatile organ with highly adaptive properties. In addition to the various homeostatic mechanisms, the skin has to cope continuously with changes in the external environment, such as heat, cold, UV-radiation, oxidative stress, injury and wounds [1, 2]. Wounds are associated with hemorrhage, hemolysis and cell
*Address correspondence to this author at the Department of Orthodontics and Oral Biology, Nijmegen Centre for Molecular Life Sciences, Radboud University Nijmegen Medical Centre, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands; Tel: +31-24-3614082; Fax: +31-24-3540631; E-mail: [email protected]
(† contributed equally to the manuscript)
injury, and result in a local accumulation of free heme pro-teins and heme [3-5]. Wounding induces a complex cascade of events to stop and prevent blood loss, to kill possible intruding pathogens, which eventually results in restoration of the site of injury and homeostasis [6, 7]. Following injury the repair takes place in different, but overlapping phases: the inflammatory, proliferative and remodeling phase. The inflammatory phase is primarily intended to provide protection for the host and is characterized by classical clinical features, such as redness, swelling, heat, pain and loss of function. The skin microenvironment changes drama-tically after injury [7-9]. One of the earliest changes in the skin after wounding is the release of modified, denatured tissue proteins. In the wounded area a pro-oxidant micro-environment is created providing signals to generate an inflammatory process. Inflammation protects from pathogenic invaders, gets rid of damaged cells after injury, prevents further damage and prepares for tissue repair (reviewed in [3]). The inflamma-tory response involves several stages: 1) dilation of capilla-ries to increase blood flow; 2) microvascular structural chan-ges and escape of plasma proteins from the bloodstream; 3) the so-called “leukocyte-adhesion cascade”; 4) elimination of possible pathogens; and 5) the resolution of inflammation. The injury will firstly lead to disruption of blood vessels, thereby activating the coagulation cascade. Besides clot formation, coagulation induces the production of vasoactive, pro-inflammatory agents and activation of the complement cascade. Activation of the different cascade systems results

1572 Current Drug Targets, 2010, Vol. 11, No. 12 Wagener et al.
in the generation of bradykinin, C3a and C5a, and the active-tion of pro-inflammatory cytokines, such as TNF-α, IL-1, IL-6 and IL-8. Subsequently, there is increased blood vessel permeability, chemokine expression, adhesion molecule expression and recruitment of cells (granulocytes, macro-phages and lymphocytes) to the site of inflammation. The end of the inflammatory phase is marked by reduced levels of pro-inflammatory cytokines and decreased number of inflammatory cells, which in turn is the sign for the next stage in the wound healing process: the proliferative phase. This is characterized by processes such as re-epitheliali-zation, neovascularization, and wound contraction. Keratino-cytes, endothelial cells and fibroblasts start to migrate into the provisional extracellular matrix in the wound area, and start proliferating. Especially fibroblast activity is res-ponsible for the build-up of new extracellular matrix (ECM) to restore lost tissue. Finally, the remodeling phase takes place when the wound area is fully re-epithelialized. Fibroblasts will differ-rentiate into myofibroblasts and generate more ECM proteins. These cells are largely responsible for wound contraction. Wound contraction causes a rapid reduction of wound size, thereby reducing the chance of wound infection by infiltrating pathogens. This is the result of both myofibro-blast contraction and reorganization of ECM. The subse-
quent reorganization and synthesis of new ECM results in stronger fibers and increased tensile strength but this newly formed tissue never reaches the quality of normal uninjured skin. During this phase, myofibroblasts in the highly cellular granulation tissue disappear via programmed cell death (apoptosis), which ultimately results in a relatively acellular scar. However, during hypertrophic scar formation the myofibroblasts tend to persist, which lies at the base of the mechanism of excessive ECM production and wound con-traction as observed in this disorder [10-12]. Hypertrophic scars are not only disfiguring but are a well-known risk factor for scar contraction, which can lead to lifelong morbidity because of significant impairment of function [13].
PATHOLOGICAL WOUND HEALING: EXCESSIVE SCARRING
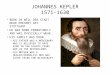
Wound contraction is important for wound closure, but under certain conditions such as following burns, deep dermal injuries and surgery related to cleft lip and palate, it may lead to excessive scar formation and pathological scar contracture [14, 15] (Fig. 1). Cleft lip and/or palate is a developmental disorder of the face that is characterized by a cleft in the upper lip and/or palate and alveolar bone.
A
B C Fig. (1). A. Patients with cleft lip and palate need to undergo various operations, which as adverse effect can result in the formation of scarring [187]. This can restrict maxillary growth and may lead to midfacial deficiency. B. and C. Also burn wounds can result in excessive or hypertrophic scars that are not only cosmetically disfiguring, but are also clearly hampering function. (Pictures of burn wounds were kindly provided by Prof. Dr. Esther Middelkoop, Association of Dutch Burn Centres, Beverwijk, The Netherlands).

The Heme-Heme Oxygenase System in Wound Healing Current Drug Targets, 2010, Vol. 11, No. 12 1573
Affected patients need multiple surgeries, which are often resulting in excessive scarring that can compromise normal growth of the maxilla and the development of the dentition (Fig. 1) [16]. Also burn patients often demonstrate large excessive scars following wound healing (Fig. 1) [13]. Thus, after major trauma to the skin, the formation of hypertrophic or excessive scars can lead to extensive functional and cosmetic morbidity, which is a major source of discomfort. Since (myo)fibroblasts are major producers of ECM, produce less matrix metalloproteinase (MMPs), and are over-represented in hypertrophic scars compared to normal skin and normotrophic scars, they are considered to be res-ponsible for the production of hypertrophic scars [13]. Nedelec and colleagues indicated that the development of hypertrophic scars and scar contractures may be the result of delayed or defective myofibroblast apoptosis [12]. The prolonged presence of fibroblasts and myofibroblasts results in abnormal ECM production and may lead to an imbalance of ECM turn-over, resulting in an excessive and rigid scar [14]. Accelerating the rate of apoptotic myofibroblast cell death was demonstrated to reduce the cell number, and may be a means for providing effective treatment of scar contracture [12]. Although a substantial amount of molecular and cellular data have been generated in order to better understand the process of wound contraction and scar contracture, the decisive and controlling mechanisms still remain to be elucidated. A major determinant of excessive scar formation is wound healing time; if a wound takes more than 21 days to heal, 78% of wound sites develop into excessive or hypertrophic scars [17]. The prolonged healing time, for example in an open or infected burn wound, is caused by overproduction of reactive oxygen species (ROS) and inflammatory mediators, which extend the proliferative phase via increased concentrations of growth factors known to stimulate fibroblast proliferation [18]. Moreover, excess amounts of ECM are produced, which interferes with normal tissue remodeling, and causes hypertrophic scar formation [19]. A tight control of inflammatory cell-derived ROS is important since excess of ROS, or a decreased expression of ROS-detoxifying proteins, corresponds with aberrant wound healing [20, 21]. Induction of ROS or inflammation can disrupt otherwise scarless fetal wound healing by increasing fibroblast proliferation and fibrosis [20, 22]. In contrast, overexpression of cytoprotective genes has demonstrated to restore delayed wound healing in diabetic mice [23]. Evidence is accumulating that the heme-HO system is involved in the oxidative and inflammatory processes leading to excessive scarring. Because this heme-HO system may be an important target to counteract hypertrophic scar formation the state of art in this field will be discussed in detail in the next part of this review.
HEME AS A PATHOLOGICAL FACTOR THAT MEDIATES OXIDATIVE AND INFLAMMATORY STRESS AND FIBROSIS
Heme (iron protoporphyrin IX) is a complex of an iron atom linked to the four ligand groups of porphyrin that is made in every mammalian nucleated cell via a series of enzymatic reactions. In response to excess levels of heme, δ-
aminolevulinate synthase (ALA-S), the rate-limiting enzyme for heme synthesis is, as a feedback, inhibited in non-erythroid cells [24]. The heme molecule provides a multitude of crucial biological functions and possesses several essential signaling properties as reviewed in Wagener et al. 2003 [3]. Heme can also interact with various inactive apo-heme proteins giving rise to functional heme proteins. For example, in hemoglobin and myoglobin it plays a critical role in oxygen transport and storage, respectively, while in cytochromes it is involved in electron transport, energy generation, and chemical transformation [3]. Furthermore, heme is indispensable for a wide array of other enzyme systems, such as cytochromes, cyclo-oxygenase (COX), and nitric oxide synthase (NOS) [25]. However, heme exerts a dual role: in small amounts it acts by itself or as the functional group of heme proteins providing diverse and indispensable cellular functions, whereas, in excessive amounts, free heme can cause severe tissue damage [26-28]. Cell damage results in a local accumulation of free heme proteins and heme. Previous data support a contribution of heme to wound healing since it can activate a wide array of processes, such as vasoconstriction, pro-coagulating effects of mononuclear-cells, activation of complement factors, platelet aggregation, and differentiation and proliferation of various cell types [29]. Heme has been shown to promote the formation of ROS via the Fenton reaction, and the (per)oxidation of biomolecules, like low density lipoprotein, which can result in cellular injury [28, 30]. This is further exemplified by studies of Nath and colleagues, who demonstrated that large amounts of heme (proteins) can cause severe kidney injury [31]. We and others demonstrated previously that free heme not only promotes oxidative stress, but also possesses pro-inflammatory properties both in vitro and in vivo [3]. Heme enhances vascular adhesion molecules ICAM-1, VCAM-1 and E-selectin, causes vascular permeability, and promotes leukocyte recruitment, and the induction of inflammatory cytokines [3, 4, 30, 32-39]. Moreover, strongly increased levels of ECM are found following exposure of mice to large amounts of heme, which may contribute to the development of fibrosis [35, 40]. It is therefore likely that free heme plays a role in the etiology of many inflammatory and pathological conditions and may function as a “molecular switch” [3, 4, 41, 42]. The important inflammatory mechanisms of heme have already been shown to affect a wide variety of conditions, including hemolytic diseases [43] and sickle cell disease [36, 41], and is thought to be involved in many more pathological processes. In recent studies, it was elegantly demonstrated that heme is the major culprit in the pathogenesis of malaria by promoting progression to cerebral malaria [42, 44, 45]. In addition, we and others also showed that heme is important in the process of wound healing [4, 5]. The sheer presence of heme is enough to recruit both macrophages and granulocytes [4]. Free heme activates granulocytes, causes granulocyte migration, and delays granulocyte apoptosis, by activating pro-survival signaling pathways (PI3K/AKT, ERK, and NF-κB), which results in prolonged presence of

1574 Current Drug Targets, 2010, Vol. 11, No. 12 Wagener et al.
inflammatory cells in the wound area [46-48]. The presence of large amounts of heme induces the recruitment of leukocytes, which is indispensable for the elimination of pathogens and for the wound healing process [4, 35]. Macrophage-derived cytokines and growth factors are important in the transition from the inflammatory phase to tissue repair. However, since heme can also potentiate the injurious effects of agents as hydrogen peroxide [49], and TNF [50], it is likely that heme-induced recruitment of leukocytes will create an environment in which these injurious agents can interact with each other, thereby postponing resolution of inflammatory and oxidative stress in the skin. Our results demonstrated that the local release of heme functions as an early trigger to start inflammatory processes following injury, and we therefore postulated that heme could act as a danger signal [3, 4]. Moreover, it has recently been demonstrated that heme can indeed activate Toll-like receptor molecule-4 (TLR-4), and can promote TNF produc-tion in macrophages [51]. Also hemozoin, a crystallized aggregate of heme molecules formed by the malaria parasite may activate an alternative TLR ligand, suggesting a differential response [52]. Inflammation is normally a beneficial response to tissue injury, protects against invading pathogens, and prepares for the restoration of tissue. In the pathogenesis of a wide variety of diseases including rheumatoid arthritis and athero-
sclerosis, inflammation-mediated tissue injury plays an important role [53]. The prolonged presence of heme may be an important factor that skews normal wound healing via chronic inflammatory and oxidative stress in the skin towards pathological scarring (Fig. 2). Thus, heme-induced ROS and pro-inflammatory insults likely contribute to cellular damage when heme is present for too long. The recent advances in the study of heme as a pro-oxidative, pro-inflammatory and cytotoxic molecule, and its possible role in the etiology of pathological conditions underscores the need for a tight control of the levels of free heme [3].
MECHANISMS OF PROTECTION AGAINST HEME-INDUCED OXIDATIVE AND INFLAMMATORY STRESS AND FIBROSIS
Heme Binding Proteins
The heme- and hemoglobin (Hb)-scavenging molecules hemopexin and haptoglobin are thought to act as a first line of defense against the injurious actions of heme [3, 4, 54]. These scavengers have been demonstrated to protect against heme- and Hb-mediated insults such as lipid peroxidation [55]. Interestingly, reduction of heme-, and Hb-scavenging molecules like hemopexin and haptoglobin has demonstrated to also aggravate several of the pro-inflammatory charac-
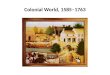
Fig. (2). Following wounding large amounts of heme are released locally that can initiate a wide range of pro-oxidative, pro-inflammatory and deleterious actions, including cytokine/chemokine production, adhesion molecule expression (inflammation), activation of the innate immune system, leukocyte recruitment, and fibrosis. We postulate that these properties of heme strongly contribute to excessive scar formation. Heme-binding proteins, heme transporters, heme-degrading proteins, and anti-oxidant systems protect us against these heme-induced insults. Since the levels of these protective mechanisms and/or effector molecules are differentially regulated in individuals, induction hereof in people with too little defense could possibly lead to amelioration of chronic wounds and prevent the formation of excessive scarring (See text for further details).

The Heme-Heme Oxygenase System in Wound Healing Current Drug Targets, 2010, Vol. 11, No. 12 1575
teristics of heme. For example, the group of Tolosano demonstrated elegantly that vaso-occlusion in the spleen, resulting in splenomegaly, was strongly enhanced in haptoglobin-hemopexin (HpHx) double knock-out mice following acute hemolysis, suggesting the involvement of plasma hemoglobin and heme [40]. Also, the single haptoglobin or hemopexin knock-out animals had increased levels of vaso-occlusion compared to wild-type animals, although less than in the double knock-out. This vaso-occlusion was likely the result of heme-induced vascular adhesion molecule expression, since ICAM-1 and VCAM-1 expression was even further enhanced following exposure to heme in hemopexin knock-out mice compared to wild-type mice [37]. The proinflammatory effects of Hb and heme were further substantiated by the analysis of acute hemolysis in splenectomized HpHx double knock-out mice. In these mice the liver took on the role of scavenging free Hb and heme from the circulation, and showed both strong inflammation and fibrosis [40]. This makes it tempting to speculate that hemoglobin and heme do not only contribute to oxidative stress and inflammation, but also to fibrosis (see Fig. 2) [35]. Also in patients with chronic venous ulcers large amounts of heme that are thought to contribute to injury, were found in ulcer fluid, plasma, and skin sections [5]. α1-Microglobulin, another heme scavenger, was found to protect against these heme-induced oxidative and inflamma-tory insults during skin wound healing [5]. Immenschuh and colleagues demonstrated that heme also induces the expres-sion of the heme-binding protein 23 (HBP23; peroxiredo-xin), an intracellular heme scavenger that is likely involved in protecting the intracellular environment from heme-induced ROS formation [56].
Heme Transporters
It was long thought that lipophilic heme can easily diffuse through the plasma membrane, however, recent studies cast doubt on this because of the anionic carboxylate side chains of the heme molecule, supporting a more important role for heme transporters in heme homeostasis [57]. Recently, a number of heme/porphyrin transport pro-teins have been identified, such as heme carrier protein 1 (HCP1), feline leukemia virus receptor C (FLVCR), breast cancer resistance protein (ABCG2/BCRP), and ABCB6. These proteins could be important to protect the cell from heme-mediated oxidative or inflammatory insults (thorou-ghly reviewed in Krishnamrthy 2007) [57]. FLVCR and BCRP can protect cells from heme-mediated insults by effluxing heme from the cells [58, 59], whereas HCP1 can shuttle heme into duodenum cells. BCRP, a member of the ABC transporter family, is a half transporter, and is believed to function as a homodimer [60]. BCRP contributes to the excretory processes of a diverse range of drugs and toxic substances, including porphyrins (e.g. heme) and flavonoids [59, 61, 62]. Moreover, heme accumulates in tissues of Bcrp knockout mice [58, 61, 62]. ABCB6 is important in mito-chondrial heme influx and could therefore also play a major role in apoptotic processes important in wound healing. It will therefore be of great interest to study the role of these heme transporters during wound healing in more detail.
Heme Oxygenase
During the resolution phase of inflammation, the pro-oxidative and pro-inflammatory properties of heme and cytokines need to be counteracted. Heme is degraded by the microsomal enzyme HO into the versatile effector molecules carbon monoxide (CO), biliverdin, and iron (Fig. 2) [63]. Biliverdin is directly converted by biliverdin reductase (BVR) into the antioxidant bilirubin. It has been demons-trated that HO-1 induction is accompanied by increased ferritin synthesis, whereas inhibition of HO activity causes a decrease in ferritin levels [64, 65]. Ferritin is a protein that can scavenge the pro-oxidant iron, rendering it inactive 66. This protective effect may be very important at sites with increased heme and iron, as in skin ulcers or after UV radiation [5, 65, 66]. HO expression represents an important mechanism of protective response in a wide variety of cellular stresses [67]. An overwhelming body of evidence indicates that the heme-HO-1 system is tightly involved in diverse (patho)physio-logical processes. HO-activity provides cytoprotection, inhi-bits apoptosis, and reduces oxidative stress and inflammation in a multitude of models, and is e.g. important for successful organ transplantation [3, 68-71]. These actions are probably mediated via its down-stream effector molecules [66]. Furthermore, biliverdin/bilirubin functions as a potent anti-oxidant, whereas CO induces cGMP-mediated vasodilatation and possesses several signaling properties [72]. At present, two HO-isoforms are known in humans. HO-1 is highly inducible by a variety of stimuli including oxidative stress, cytokines and its substrate heme, whereas HO-2 is mainly constitutively expressed [3]. HO-2 iso-enzymes probably function in normal heme capturing and metabolism [73, 74]. It is important to take into account that the heme-HO system has regulatory functions in a wide variety of processes that could be important in the resolution phase of wound healing, such as amelioration of inflamma-tion, protection against apoptosis, and proliferation [70, 75, 76]. We and others previously demonstrated that HO-1 overexpression can counteract the various cytotoxic, pro-oxidative and pro-inflammatory actions of heme [3, 43, 77]. HO-1 down-modulates inflammatory adhesion molecules and attenuates leukocyte adhesion to the vascular endothe-lium upon exposure to heme or other pro-inflammatory stimuli, whereas inhibition of HO-activity exacerbates heme-mediated oxidative and inflammatory injury both in vitro and in vivo [34, 35, 78-80]. Exposure of the skin to oxidative stress or to UV radiation promotes the release of the non-covalently bound prosthetic heme group from heme-proteins [81]. Recently, a simple but elegant mechanism by which CO protects against diseases was revealed: it prevents the release of the injurious heme from cell-free heme-proteins, by binding to the ferrous iron of the protoporphyrin IX ring [45]. This insight has already been shown to be important in diseases as malaria and atherosclerosis, but likely also plays a role in many more conditions, including wound healing. Moreover, it adds to the understanding of the protective actions of HO-activity. The important cytoprotective properties of HO-1 are further exemplified by a human case of HO-1 deficiency

1576 Current Drug Targets, 2010, Vol. 11, No. 12 Wagener et al.
suffering from a wide variety of conditions including highly increased vascular adhesion molecule expression, severe inflammation, leukocytosis, and hyperlipidemia [3, 82-84]. This clinical observation is paralleled by similar data obtained from HO-1 knock-out mice [83, 84]. In addition, these mice have been shown to be extremely sensitive to oxidative injury. On the other hand, HO-1 transgenic mice are protected from oxidative stress, inflammation, and vascular dysfunction. Recent data suggest that also the HO-2 isoform has a crucial role in protection against inflammation [85, 86]. Since HO-2 harbors an extra heme-binding pocket [87], it may function as a first defense against heme-derived injury. Interestingly, we found a high HO-2 expression in uninjured skin, which may be a first line of defense against acute oxidative and inflammatory insults [4]. HO-1 on the other hand, is imported into the wound area by infiltrating cells, and initiates the resolution phase of inflammation [4, 88]. Our results demonstrate that the local release of heme may be a physiological trigger to start inflammation, whereas HO-1 antagonizes inflammation by attenuating adhesion and cellular infiltration [4].
UVA-INDUCED INJURY; AN INTERPLAY BE-TWEEN HEME, BACH1, AND HEME OXYGENASE ISOFORMS
The UVA waveband (320-400nm) is a major component of sunlight and is a powerful oxidizing carcinogen which generates various reactive oxygen species including singlet oxygen and hydroxyl radical in cells [89]. The identification of a 32kd protein that was strongly induced by UVA irradiation of human skin fibroblasts [90] as HO-1 [91] revealed this enzyme as the major oxidant stress-inducible pathway in mammalian cells. Interestingly, exposure of the skin to CO has also been demonstrated to protect against photocarcinogenesis [92]. Skin is the major target of sunlight and a puzzling observation from early studies, given that the epidermis is the first target reached by penetrating sunlight, was that while HO-1 was strongly induced in skin fibroblasts (and to some extent in melanocytes), there was almost no induction in epidermal keratinocytes [93]. In contrast, keratinocytes expressed high levels of the constitutive enzyme HO-2 [93] and it was postulated at the time that the lack of expression of induction of HO-1 reflected the low levels of free heme. Recently it has become clear that the activity of the HO-1 promoter is regulated by transcription factors typified by the Nrf2/MafK heterodimer. This transcriptional activating heterodimer competes in a dynamic fashion with negative regulatory proteins, such as the Bach1/MafK complex, for binding to the HO-1 promoter and determine together whether there is transcription of HO-1 [94]. Heme binding to the transcriptional inhibitor Bach1 releases its binding to the HO-1 promoter, stabilizes Nrf2, and enables Nrf2 to promote HO-1 transcription [95]. Low doses of UVA have been shown to release free heme in cells [96]. Recently it was observed that both Nrf2 [97] and Bach1 (Raval and colleagues, unpublished obser-vations) are involved in UVA-mediated up-regulation of HO-1 in fibroblasts. Using siRNA knock-down technology,
we have now shown that silencing of HO-2 expression allows a strong basal and UVA-induced expression of HO-1 in epidermal keratinocytes [98]. However , it is clear that Bach1 itself is the central factor suppressing HO-1 expres-sion in fibroblasts since knock-down of Bach1 leads to a strong constitutive expression of HO-1 which is not further enhanced by irradiation with UVA. These studies also strongly support the concepts that 1) it is the level of free heme that plays a key role in regulation of HO-1 expression and 2) levels of HO-2 expression strongly influence HO-1 expression (but not vice-versa) by determining the levels of heme that can interact with Bach1.
DIFFERENTIAL LEVELS OF PROTECTION AGAINST HEME
When large amounts of free heme proteins or heme (locally) accumulate, like in a blood clot, in a wound, or after extravascular deposition, their scavengers may get over-whelmed or are unable to reach them [3]. When the protective proteins against excess levels of heme in the skin are depleted, the skin may be more prone to heme-induced injurious effects, the formation of inflammatory and oxidative stress, and subsequently excessive scars. This is exemplified by the following: For haptoglobin, three major polymorphisms with diffe-rent hemoglobin-scavenging capacity have been described that are associated with different prevalence of many inflam-matory diseases [99]. The polymorphism with decreased hemoglobin binding is associated with a higher prevalence for cardiovascular diseases [100]. This is in line with our findings of heme-mediated oxidative and inflammatory effects [3]. Although genetic polymorphism of hemopexin has been reported for rabbits and pigs, possible human polymorphisms of hemopexin need further exploration [101]. Since albumin can bind heme to a lesser extent, it is possible that in case of such a deficiency in scavengers this plasma protein can also provide some protection [3]. Furthermore, the length of a guanine-thymidine (GT)n-repeat polymorphism in the promoter region of the HO-1 gene determines the level of HO induction, and corresponds clinically with differential susceptibility to various condi-tions [102, 103]. Since HO-activity protects against inflam-matory and oxidative injury, we expect that people carrying a HO1 promoter polymorphism leading to less HO1 induc-tion, have increased chance of developing heme-mediated excessive scarring. Thus, functional relevant polymorphisms for heme scavengers, like haptoglobin and hemopexin, and antioxidant enzymes like the heme-degrading enzyme HO could therefore determine the level of protection against heme, and possibly, the severity of scarring. This is especially impor-tant for people with increased risk of heme release or people with an already compromised redox balance, such as diabetes patients or people with glutathione deficiency [104]. In pathophysiological conditions, particularly those associated with diabetes, wound healing is also significantly disturbed [105, 106]. Interestingly, Quan and colleagues elegantly demonstrated that hyperglycemia decreases HO-

The Heme-Heme Oxygenase System in Wound Healing Current Drug Targets, 2010, Vol. 11, No. 12 1577
activity in the endothelium and increases the production of ROS [104, 107], suggesting that patients with hyperglycemia are deprived from the protecting effects of the HO-effector molecules CO, bilirubin and ferritin. Both investigations on animal models and clinical studies demonstrated that diabetic wounds are characterized by a dramatic reduction in the production of growth factors and their receptors playing an integral role in the process of skin repair [105, 106, 108]. Among those mediators the pivotal role of VEGF has been shown. Accordingly, growing evi-dence indicates that chronic wounds have decreased expres-sion of VEGF and fewer blood vessels in the granulation tissue when compared with physiologic wounds [109]. Particularly, in genetically diabetic mice the level of VEGF is severely reduced during the healing process [110]. Also the synthesis of stromal cell derived factor-1 (SDF-1) is dramatically attenuated in diabetic conditions [111]. We have determined the course of HO-1 induction in the injured skin of diabetic mice 1 during wound healing. Interestingly, the highest induction of HO-1 within the wound bed is observed during 1-3 days after insult, but in diabetic db/db mice it could be significantly delayed up to 8 days [112]. In order to determine whether this is associated with the impaired skin regeneration observed in those animals we have performed gene transfer of HO-1 using adenoviral vectors. Indeed, these experiments revealed that attenuation of the healing process can be partially reversed by HO-1 overexpression [112]. Additionally, attenuating the oxidative stress and the exaggerated inflammation in the wounds by overexpression of such concomitantly anti-inflammatory gene(s) can moderate the overall healing response driving it into the direction of proper tissue repair [113]. Noteworthy, the role of HO-1 may be particularly important, as in chronic wounds the expressions of other antioxidant genes, such as super-oxide dismutase, glutathione peroxidase, glutathione-S-transferase, or catalase, can be significantly decreased [114]. The same concerns the concentrations of antioxidants such as ascorbic acid, vitamin D, and glutathione [114]. Genetic variation and redox balance thus determine the differential protection against the injurious effects of heme between individuals.
WOUND HEALING AND MODULATION OF HEME-ENZYMES BY THE HEME-HEME OXYGENASE SYSTEM
Heme is the crucial part of many major enzymatic systems, such as nitric oxide synthase (NOS), and cyclo oxygenase (COX) [87]. HO controls the activity of these heme-proteins in two ways: directly, by regulating the availability of heme for the synthesis of heme-proteins (apo-enzyme vs holo-enzyme), or indirectly, via the generation of CO, which can bind to the heme moiety of heme-proteins and thereby affecting their enzymatic activity [115]. Moreover, CO binding would inhibit the release of heme from heme proteins [3, 45]. COX, NOS and arginase are important enzymes during the inflammatory phase of wound healing, but also in later processes such as wound contraction [116]. They exist in
several isoforms that can be constitutively expressed or inducible. Their products, COX-derived prostaglandins, NOS-derived NO, and arginase-derived ornithine and polyamines have been described as important mediators in skin repair [117, 118]. COX can convert arachidonic acid (AA) into PGE2, which is an important inflammatory mediator. Recent work with inducible NOS (iNOS)-deficient mice identified iNOS-derived NO as pivotal for wound healing [119]. This is further supported by the finding that inhibition of iNOS during repair leads to a potent effect of iNOS-derived NO on epithelial gene expression, which severely impaired re-epithelialization. L-arginine represents the only substrate for NOS, which results in the generation of citrulline and NO [120]. These observations may explain the observation that L-arginine improves wound healing in animal models and in humans, because it is the only substrate for NOS enzymatic activity. Alternatively, arginases, which convert L-arginine into ornithine and urea, may compete with NOS for their substrate at the wound site. Arginine levels in wound fluids remain low during healing [121]. Ornithine is the precursor for polyamines and proline. Polyamines are essential for cell proliferation whereas proline is necessary for collagen formation. Kampfer and colleagues [122] demonstrated that the arginase system is induced upon skin injury in mice, which paralleled the well-established expressional and activity kinetics of iNOS after injury. Furthermore, impaired healing was associated with a significantly increased arginase acti-vity, whereas improved healing showed to be characterized by a re-adjustment of iNOS and arginases at the wound site. Thus, a balanced presence of the iNOS and arginase acti-vities are crucial to drive an efficient skin repair. It is likely that the heme-heme oxygenase system is pivotal in modulating COX activity and the balance between NOS and arginase activity in fibroblasts and macrophages, and subsequently in the wound healing process.
MYOFIBROBLAST APOPTOSIS AND THE HEME-HEME OXYGENASE SYSTEM
The induction of myofibroblast apoptosis in hypertrophic scars has received considerable attention because of its obvious therapeutic significance. Fibroblasts derived from normal scars had a higher rate of apoptosis than cells from hypertrophic scars as was displayed by low levels of anti-apoptotic factors such as Bcl-2 and Bcl-xL and high levels of the pro-apoptotic factor Bax [123]. In a murine model of hypertrophic scar formation decreased fibroblast apoptosis was also detected, which was accompanied by enhanced levels of the pro-survival factor Akt [124]. This study also demonstrated that in p53-knock-out mice, with down-regu-lated apoptosis, hypertrophic scar formation was increased, whereas less scar hypertrophy was seen in pro-apoptotic Bcl-2 knock-out mice. Apoptosis can generally occur in either a caspase-dependent or -independent fashion. For caspase-dependent apoptosis two major pathways have been identified. The first is the extrinsic pathway, which involves activation of death receptors like tumor necrosis factor (TNF) receptor, FAS and

1578 Current Drug Targets, 2010, Vol. 11, No. 12 Wagener et al.
TRAIL. Fas-associated death domain and TNF-receptor-associated death domain can recruit and activate caspase-8 to form a death-inducing signaling complex (DISC) [125]. DISC can generally propagate the death signal either by splicing Bid, which upon translocation to the mitochondria can cause mitochondrial outer membrane permeabilization (MOMP) or it can lead to the release of pro-apoptotic proteins, such as cytochrome c [126]. Cytochrome c in turn can form an apoptosome by interacting with apoptotic protease activating factor-1 (Apaf-1) and procaspase 9. This complex is able to activate caspase 9, which in turn activates the effector caspases 3, 6 and 7, leading to apoptosis [127]. Alternatively, DISC can also directly activate these effector caspases [128]. Secondly, caspase-dependent apoptosis can occur via the intrinsic pathway, which is regulated by the mitochondrion, and characterized by MOMP [129], that is controlled by the family of Bcl-2 proteins [130]. These Bcl-2 proteins are either anti- or pro-apoptotic and a shift in balance between these two groups ultimately determines cell survival or cell death. The pro-apoptotic Bcl-2 family mem-bers Bax and Bak probably contribute to MOMP by facilitating the release of cytochrome c from the mitochon-drial intermembrane space [131, 132]. Caspase-independent cell death relies on the Bax-mediated release of pro-apoptogenic factors like apoptosis inducing factor (AIF) and EndoG from the mitochondria, which subsequently trans-locate to the nucleus and contribute to chromatin condensa-tion and DNA damage [133]. Heme oxygenase is considered to be a cytoprotective enzyme and numerous publications show that it affords protection against apoptosis (refs. in [134, 135]). Since oxidative stress is clearly involved in apoptosis, the protective effect of HO-activity most likely depends on the antioxidant properties of HO-derived reaction products. For instance, the antioxidant actions of bilirubin can protect cultured cells from cell death caused by oxidative stress [136]. Iron released from heme-break down by HO can have pro-oxidant actions via the Fenton reaction and could therefore be considered to be deleterious. However, as men-tioned previously, iron can also upregulate the expression of the sequestering protein ferritin, which protect cells from iron released from HO-activity following induction of oxidative stress by ultraviolet A radiation [65]. The exposure of cells to exogenous CO potently inhibited TNFα-induced apoptosis in mouse fibroblasts, indicating the anti-apoptotic potential of CO [137]. In addition, HO-1-derived CO protected endothelial cells from TNFα-induced apoptosis [138]. This effect was shown to depend on the activation of p38 MAPK and the expression of NF-κB-responsive anti-apoptotic genes. On the contrary, HO and CO can induce Fas-mediated apoptosis in Jurkat T-cells [139, 140], and CO can also induce apoptosis in endothelial cells [141]. We previously showed that the polyphenol curcumin is a potent inducer of dermal fibroblast apoptosis and that the concomitant induction of HO-1 protects against curcumin-induced apoptosis [142]. Curcumin-induced apoptosis of human dermal fibroblasts turned out to be completely caspase-independent but relies on the mitochondrial generation of ROS and subsequent mitochondrial release of apoptosis inducing factor through translocation of the pro-apoptotic factors p53 and Bax [143]. The enhanced levels of HO-1 induced by curcumin protects fibroblasts against the
deleterious effects of curcumin and, therefore, HO or its effector molecules could enable the fine-tuning of the balance between acellular and hypertrophic wound healing.
FIBROSIS AND THE HEME-HEME OXYGENASE SYSTEM
Fibroblasts are responsible for the production and deposition of several ECM proteins such as collagens and fibronectin, proteins which are essential for tissue repair after injury. These products give the tissue strength, integrity and flexibility. However, sometimes, especially after burns, and sometimes following surgery related to cleft lip and palate, this healing process derails and a pathological situa-tion is formed (Fig. 1) were fibroblasts number dramatically increases by enhanced proliferation and/or failure to go into apoptosis, resulting in fibrosis/hypertrophy. Moreover, the increased number of myofibroblasts produce excessive amounts of ECM proteins, leading to an inferior repair tissue. As described above, increased heme levels have been associated with the formation of fibrosis [40]. The possible protective role of HO in skin has been the subject of only few studies, and evidence for a role for HO in dermal fibrosis is therefore scarce. In systemic sclerosis patients (SSC) it was found that fibroblasts are extra vulnerable to apoptosis induced by curcumin. It was concluded that, in these patients, the expression of phase 2 detoxification enzymes HO-1 and glutathione S-transferase P1 could not be upregulated [144]. In a psoriasis model, upregulation of HO-1 by CoPP dramatically reduced psoriasis skin lesions by preventing keratinocyte hyperproliferation [145]. However, in several other organ systems such as lung, heart, kidney, and liver, a clear relation between HO, its effector mole-cules, and fibrosis has been described. In the bleomycin-induced model of pulmonary fibrosis the systemic inhibition of HO-activity by Zn-deuteropor-phyrin-IX-2,4-bisethylene glycol caused reduced levels of transforming growth factor-β (TGFβ) accompanied by signi-ficantly less collagen accumulation, which ultimately resul-ted in less fibrosis [146]. Additionally, viral overexpression of HO-1 in the lung prevented bleomycin-induced fibrosis [147]. Besides HO, also its effector molecule CO has been shown to prevent bleomycin-induced lung fibrosis as was shown by decreased fibroblast proliferation and decreased expression of the ECM molecules collagen-1 and fibronectin [148]. Very recently, the same group showed that CO protects against fibrosis, and that it suppresses alpha-smooth muscle actin (αSMA) expression, which was dependent on ERK signaling [149]. Also for the HO effector molecule bilirubin, evidence exists in support of an antifibrotic effect. Wang and colleagues showed in rats that the development of bleomycin-induced pulmonary fibrosis was attenuated in hyperbilirubinemic animals as shown by improved lung histology and reduced levels of TGFβ [150]. The antifibrotic properties of 15-d-PGJ2 in liver fibrosis, such as growth inhibition, inhibition of collagen synthesis, and induction of apoptosis could be attributed to the activity of HO, and more specifically, to the HO-effector molecule bilirubin and not CO [151]. Recombinant adeno-associated-virus-mediated in vivo overexpression of HO-1 in hepatic

The Heme-Heme Oxygenase System in Wound Healing Current Drug Targets, 2010, Vol. 11, No. 12 1579
stellate cells resulted in a reduced expression of type 1 collagen, impaired proliferation, and reduced levels of pro-fibrotic TGFβ [152]. Recently, it was shown that increased endogenous HO-1 by administration of the HO-inducer CoPP could reduce hepatic fibrosis in an immune liver fibrosis model of rat [153]. Upregulation of the HO-system by systemic treatment with heme resulted in decreased cardiac fibrosis/hyper-trophy, whereas inhibition of HO activity by CrMP exacer-bated fibrosis in spontaneously hypertensive rats [154]. Interestingly, this reduction in fibrosis was accompanied by HO-mediated upregulation of cGMP levels, which could explain the reduced levels of NF-kB and AP-1, transcription factors well known to be involved in the fibrotic process. The same group recently reported that the beneficial effects of hemin therapy on several fibrotic parameters could be abolished by the HO-activity inhibitor CrMP [155]. Furthermore, hemin-induced HO-1 attenuated TGFβ and ECM proteins such as collagen and fibronectin. Post myo-cardial infarction was inhibited by viral overexpression of HO-1 in the left ventricle [156]. Although extensive myocar-dial scarring and fibrosis, associated with elevated levels of collagen-1 and -3 and MMP-2 activity, was observed in the LacZ-control group, these effects were strongly reduced in HO-1-treated animals. Moreover, virally overexpressed HO-1 caused a reduction in proliferation of isolated cardiac fibroblasts. Curcumin is a well-known antifibrotic agent and a known upregulator of HO-1. In a glomerular model of fibrosis, curcumin-induced HO-1 was able to reduce several markers of fibrosis, such as expression of fibronectin, TGFβ, PAS and PAI-1, and these effects could be blocked by co-administration of curcumin with the HO-activity inhibitor ZnPP [157]. Further evidence of an antifibrotic effect of HO is given by the study of Kie et al. in which mice deficient in HO-1 demonstrated more fibrosis after kidney obstruction compared to wild type mice [158]. Obstructed kidneys of HO-1 deficient mice also presented with greater infiltration of inflammatory cells, tubular TGFβ expression and αSMA expression. In a murine model of arthritis HO-1 was strongly induced by the systemic treatment with CoPP, which aside from inhi-biting cartilage erosion, unexpectedly resulted in extensive fibrosis of the joint. Treatment with the HO-inhibitor SnPP also reduced arthritis severity but did not result in fibrosis [159]. These data clearly demonstrate that HO can act as an anti-fibrotic agent in several organs and, therefore, modula-tion of HO-activity could also be beneficial to treat patho-logical scar formation in the skin and oral mucosa. MMPs are the natural enzymes responsible for the degradation of the ECM and since HO seems to be a protective factor against fibrosis, a likely target of HO-activity could be the expression/activity of MMPs. Indeed, several studies show that overexpression or induction of HO affects expression and activity of several MMPs. Hemin-induced HO-1 expression was able to inhibit breast cancer invasion through the suppression of MMP-9 expression [160]. This effect could be blocked by the HO-activity inhibitor SnPP and mimicked by addition of CO but not by
BV/BR, indicating that this effect was mediated by HO. In contrast, it was shown that in breast cancer cells 15d-PGJ2, in addition to CoPP and hemin, induces HO-1 expression, which subsequently resulted in the induction of MMP-1 [161]. Addition of iron chelators and antioxidants abrogated HO-mediated MMP-1 induction, indicating the involvement of free iron and ROS in this process. In osteoarthritis, the pharmacological induction of HO-1 by CoPP resulted in inhibition of MMP-1 and MMP-13 expression [162], whereas HO-induction decreased MMP-9 activity in a model of acute arthritis [163]. In lung epithelial cells, CO was able to block expression and activity of MMP-1 and -2, indicating that also the products of HO-activity can affect MMPs [164]. So, targeting HO-activity could be a novel approach to modulate MMP-activity and thereby improve the outcome of pathological wound healing.
WOUNDS, ANGIOGENESIS AND HEME OXYGE-NASE
Vascularization of the wound, achieved by angiogenesis (formation of new blood vessels from preexisting capillaries) or by vasculogenesis (formation of new blood vessels from endothelial progenitor cells), is necessary for proper tissue repair. Factors stimulating the formation of new blood ves-sels are mainly secreted by keratinocytes and macrophages in the inflammatory phase, and include vascular endothelial growth factor (VEGF), fibroblast growth factors (FGFs), keratinocyte growth factor (KGF) and insulin-like growth factor (IGF) (for review see: Gurtner and colleagues [106]). Numerous conditions affect the process of wound heal-ing. Several genetic models have demonstrated the signi-ficance of various genes for the proper regeneration of the skin [165, 166]. Among them are crucial genes influencing inflammation and the formation of blood vessels such as HO-1. Indeed, involvement of HO-1 in blood vessel formation has been previously revealed, and so far numerous studies demonstrated its significance for the synthesis of VEGF-A in vascular smooth muscle cells [167], endothelial cells [168, 169], keratinocytes [170] and cardiomyocytes [171]. Also the production of SDF-1 was upregulated by HO-1 overexpression in myocardium [171]. Moreover, HO-1 works also downstream of both VEGF [168, 172] and SDF-1 [173] in endothelial cells and endothelial progenitor cells stimulated with those growth factors. In contrast, prostate cancer cells overexpressing HO-1 reduced VEGF-A levels [174]. Thus, under certain conditions HO-1 does not promote but inhibits angiogenesis, suggesting a more complex relationship between HO-1 and angiogenesis. This is described in more detail in the excellent review of Was et al. in this issue of Current Drug Targets [175]. Hence, the role of HO-1 in vascularization during the regenerative processes can be important for the healing of either skin or other injured tissues, but may be more complex than initially thought. Of particular importance was the demonstration that the level of HO-1 expression in the skin significantly influenced the tissue vascularization. Accordingly, the number of CD31-positive capillaries was similar in wild type mice and in animals lacking one Hmox-1 allele. However, in homozygous Hmox-1 knockout individuals the number of

1580 Current Drug Targets, 2010, Vol. 11, No. 12 Wagener et al.
blood vessels was significantly lower, by about two-fold, while in the skin of transgenic mice, having additionally the human Hmox-1 gene expressed in keratinocytes, the number of capillaries was doubled in comparison to the wild type counterparts. It is well known that the skin of hyperglycemic db/db mice, which are used as a model of human type 2 diabetes, have a less dense network of vasculature in the injured skin [176]. The same was observed in our studies. However, adenoviral gene transfer of HO-1 increased the number of capillaries in the skin of diabetic mice while this did not occur in animals injected with control vector [112]. Various experimental models have demonstrated the improvement of wound healing after topical application of proangiogenic proteins or transfer of their genes. Indeed, delivery of VEGF protein [177, 178] or overexpression of VEGF-A or VEGF-C [179, 180] accelerated blood vessel formation and reduced the time of wound closure in various models. Similar results have been achieved in mice undergoing PDGF-BB [181], FGF-1 [182], FGF-2 [181], SDF-1 [183], IGF and KGF [184] or angiopoietin-1 [185] protein treatment or gene transfer. However, despite some beneficial effects of therapy with growth factors, most of the animal experiments and clinical trials have reported only modest improvements in wound closure [186, 187]. As wound healing is a complicated process, requiring the orchestration of actions of several cell types and numerous mediators, one can therefore presume that upregulation of gene(s) working upstream the angiogenic cytokines, and regulating the expression of several of them, can be better than augmenting the production of only one factor.
WOUND HEALING TIME AND HEME OXYGENASE
Because of the reduced risk of infection, a fast wound closure and a short healing time have always been thought of as beneficial. However, accelerated wound contraction can exacerbate scar formation [12]. Nowadays, antibiotics/anti-mycotics are very efficient in combating infections and consequently allow for slower wound closure. In an in vitro study we showed that curcumin can block fibroblast-mediated collagen gel contraction, and that restoration of HO-activity can protect against this effect [142]. The first approach to demonstrate the role of HO-1 in wound healing time was performed in an excisional wound healing model in mice devoid of the Hmox-1 gene [173]. We revealed that lack of both Hmox-1 alleles in 3-month old animals significantly attenuated skin closure. Moreover, while in wild type mice application of SDF-1 accelerated wound healing, the effect of this growth factor was impaired in HO-1 knockout mice [173]. In our recent study [112] a comprehensive approach was undertaken to investigate the significance of HO-1 for effects on wound healing time. To this end we have employed several animal models, investigating the effect of pharmacological inhibition of HO-1 expression, genetic knockout of either one or two Hmox-1 alleles as well as transgenic overexpression of HO-1 in keratinocytes [112]. Our study has revealed that pharmacological inhibition by local or systemic treatment of mice with SnPPIX or knockout of both Hmox-1 alleles significantly impaired
closure of cutaneous wounds in 3 month old animals. Importantly, in the aging, 6 month old mice the lack of even one Hmox-1 allele significantly affected skin closure and in such older specimens the total absence of HO-1 could result in complete abrogation of repair [112]. Further, the absence of HO-1-activity reduced angiogenesis and had an inhibitory effect on keratinocyte migration and survival. Importantly, our observations are supported by other recent studies which demonstrated that pharmacological induction of HO-1 with tin chloride significantly accelerated wound healing time and decreased inflammation in injured corneal epithelium [177]. Additionally, we showed that in HO-2 knock-out mice wound closure was also delayed compared to WT animals and that this was related to increased inflammation [86]. Interestingly, in hyperbilirubinemic rats, wound closure time was shorter than in wild-type controls, indicating that high levels of bilirubin accelerate wound healing [86]. Of note, clinical data from sickle cell anemia patients, which are characterized by elevated serum bilirubin, as a result of a higher rate of heme degradation, indicate that they are better protected against leg ulcers, again suggesting a role for HO-1 in wound healing [178]. Combined, these results clearly show that HO-activity is intimately involved in the later stages of wound healing and is not only important in the resolution of inflammation. However, more research is required to assess the effects of HO-mediated acceleration of wound healing on scar formation.
CONCLUSIONS AND FUTURE THERAPEUTIC POSSIBILITIES
Summarizing, we expect that heme can play a central role in the pathogenesis of excessive scarring. The prolonged presence of heme-induced pro-oxidative, pro-inflammatory, and deleterious insults in the skin may initiate the formation of fibrosis and excessive scar formation. Heme-binding proteins, heme transporters, heme-degrading proteins, and anti-oxidant systems protect us against these heme-induced insults. Since the levels of these protective mechanisms or effector molecules are differentially regulated in individuals, induction hereof in patients with an impaired defense could possibly lead to amelioration of chronic wounds and prevent the formation of excessive scarring. Small concentrations of heme act cytoprotective by the swift up-regulation of HO-1 via the release of Bach1 from the HO-1 promoter, whereas large amounts of heme present for prolonged periods of time may act deleterious on tissue via its pro-oxidative and pro-inflammatory functions [3, 35, 179], which cannot be neutra-lized anymore by the anti-oxidative and anti-inflammatory properties of the HO-1 end-products. HO-1, working both as a factor limiting the extent of uncontrolled inflammation-driven angiogenesis while induc-ing the non-inflammatory vascularization [172, 180] may be a good candidate for therapeutic approaches based on either gene transfer or augmentation of the endogenous expression of HO-1. Various small molecular compounds, activating the Nrf2 transcription factor and inducing the expression of not only HO-1 but also other anti-oxidant and protective genes (for review see [104, 181]) can be tested for this purpose.

The Heme-Heme Oxygenase System in Wound Healing Current Drug Targets, 2010, Vol. 11, No. 12 1581
The possibility of HO-1 augmentation can also be consi-dered in those clinical approaches which involve the application of cultured keratinocytes for treatment of severe burns. Such isolated keratinocytes can be relatively easily modified with gene transfer or endogenous HO-1 can be enhanced by pharmacological treatment. Our data [112] indicate that HO-1 may enhance the migration of keratino-cytes, improving also their survival in stressful conditions and augmenting their proliferation, as has been also sug-gested by previous studies [182]. The application of the end-products of HO-1 activity can be additionally tested, as both CO and biliverdin can enhance VEGF synthesis in endo-thelial cells [183] and keratinocytes [170, 184], respectively. Importantly, it is also possible that compounds already known to play a beneficial role in wound healing act via HO-1 induction. RegranexTM, the recombinant PDGF-BB protein is the only one growth factor registered for the clinical treatment of diabetic ulcers [185]. Interestingly, PDGF-BB is a potent inducer of HO-1 expression [186]. Therefore, it is tempting to suggest that the beneficial effects of this biological, as demonstrated in some diabetic patients involve HO-1 induction. Further research to the deleterious effects of heme and the protecting effects of heme-neutralizing mechanisms in wound healing and scarring is warranted, and is likely to result in novel strategies to prevent or attenuate excessive scarring.
ACKNOWLEDGEMENTS
We thank our coworkers who contributed to the experi-ments described in this review. The research of the group of Wagener is supported by grants from the Dutch Burns Foundation (Grants # 05.104 and # 09.110), the Radboud University Nijmegen Medical Centre, and the Dutch Diabetes Research Foundation (Grant # 2006.00.055). The research of the groups of Dulak and Jozkowicz, and of the Faculty of Biochemistry, Biophysics and Biotechno-logy of the Jagiellonian University are supported by grants from the European Union (EU) structural funds (grants No. POIG 01.02-00-109/09, POIG.02.01.00-12-064/08, and 02.02.00-00-014/08), and grants No. N301 08032/3156; N301 3148/37 from the Ministry of Science and Higher Education. Jozkowicz is a recipient of the Wellcome Trust Senior Research Fellowship in Basic Biomedical Science. The department of Medical Biotechnology participates in the EU COST CM0602 Action (ANGIOKEM). The recent work of the Tyrrell group has been supported by the UK Biotechnology and Biological Sciences Council (BBSRC, project code BB/D521530/1).
REFERENCES [1] Cross CE, van der Vliet A, Louie S, Thiele JJ, Halliwell B.
Oxidative stress and antioxidants at biosurfaces: plants, skin, and respiratory tract surfaces. Environ Health Perspect 1998; 106 (Suppl 5): 1241-51.
[2] Dubertret L. [Skin and environment]. C R Acad Sci III 2000; 323: 629-32.
[3] Wagener FA, Volk HD, Willis D, et al. Different faces of the heme-heme oxygenase system in inflammation. Pharmacol Rev 2003; 55: 551-71.
[4] Wagener FA, van Beurden HE, von den Hoff JW, Adema GJ, Figdor CG. The heme-heme oxygenase system: a molecular switch in wound healing. Blood 2003; 102:521-8.
[5] Allhorn M, Lundqvist K, Schmidtchen A, Akerstrom B. Heme-scavenging role of alpha1-microglobulin in chronic ulcers. J Invest Dermatol 2003; 121: 640-6.
[6] Hunt TK, Hopf H, Hussain Z. Physiology of wound healing. Adv Skin Wound Care 2000; 13: 6-11.
[7] Chettibi S, Ferguson WJ. Wound repair: an overview. In: Gallin JL, Snyderman R, eds. Inflammation: basic principles and clinical correlates. 3 ed. Philadelphia: Lippincott Williams & Wilkins 1999: 865-81.
[8] Cooper DM. Wound healing: new understandings. Nurse Pract Forum 1999; 10: 74-86.
[9] Dressler J, Bachmann L, Strejc P, Koch R, Muller E. Expression of adhesion molecules in skin wounds: diagnostic value in legal medicine. Forensic Sci Int 2000; 113: 173-6.
[10] Greenhalgh DG. The role of apoptosis in wound healing. Int J Biochem Cell Biol 1998; 30: 1019-30.
[11] Linge C, Richardson J, Vigor C, et al. Hypertrophic scar cells fail to undergo a form of apoptosis specific to contractile collagen-the role of tissue transglutaminase. J Invest Dermatol 2005; 125: 72-82.
[12] Nedelec B, Shankowsky H, Scott PG, Ghahary A, Tredget EE. Myofibroblasts and apoptosis in human hypertrophic scars: the effect of interferon-alpha2b. Surgery 2001; 130: 798-808.
[13] Kwan P, Hori K, Ding J, Tredget EE. Scar and contracture: biological principles. Hand Clin 2009; 25: 511-28.
[14] Nedelec B, Ghahary A, Scott PG, Tredget EE. Control of wound contraction. Basic and clinical features. Hand Clin 2000; 16: 289-302.
[15] Park JS, Kim JY, Cho JY, Kang JS, Yu YH. Epidermal growth factor (EGF) antagonizes transforming growth factor (TGF)-beta1-induced collagen lattice contraction by human skin fibroblasts. Biol Pharm Bull 2000; 23: 1517-20.
[16] Wilson AD, Mercer N. Dermabond tissue adhesive versus Steri-Strips in unilateral cleft lip repair: an audit of infection and hypertrophic scar rates. Cleft Palate Craniofac J 2008; 45: 614-9.
[17] Deitch EA, Wheelahan TM, Rose MP, Clothier J, Cotter J. Hypertrophic burn scars: analysis of variables. J Trauma 1983; 23: 895-8.
[18] Singer AJ, Clark RA. Cutaneous wound healing. N Engl J Med 1999; 341: 738-46.
[19] Aarabi S, Longaker MT, Gurtner GC. Hypertrophic scar formation following burns and trauma: new approaches to treatment. PLoS Med 2007; 4: e234.
[20] Frantz FW, Bettinger DA, Haynes JH, et al. Biology of fetal repair: the presence of bacteria in fetal wounds induces an adult-like healing response. Journal of pediatric surgery 1993; 28: 428-33; discussion 33-4.
[21] Steiling H, Munz B, Werner S, Brauchle M. Different types of ROS-scavenging enzymes are expressed during cutaneous wound repair. Exp Cell Res 1999; 247: 484-94.
[22] Wilgus TA, Bergdall VK, Dipietro LA, Oberyszyn TM. Hydrogen peroxide disrupts scarless fetal wound repair. Wound Repair Regen 2005; 13: 513-9.
[23] Luo JD, Wang YY, Fu WL, Wu J, Chen AF. Gene therapy of endothelial nitric oxide synthase and manganese superoxide dismutase restores delayed wound healing in type 1 diabetic mice. Circulation 2004; 110: 2484-93.
[24] Sassa S. Regulation of the genes for heme pathway enzymes in erythroid and in non-erythroid cells. Int J Cell Cloning 1990; 8: 10-26.
[25] Seed MP, Willoughby DA. COX-2, HO NO! Cyclooxygenase-2, heme oxygenase and nitric oxide synthase: their role and interactions in inflammation. BIRAs Symposium, Saint Bartholomew's Hospital, London, 26 April 1996. Inflamm Res 1997; 46: 279-81.
[26] Balla J, Balla G, Jeney V, et al. Ferriporphyrins and endothelium: a 2-edged sword-promotion of oxidation and induction of cytoprotectants. Blood 2000; 95: 3442-50.
[27] Ryter SW, Tyrrell RM. The heme synthesis and degradation pathways: role in oxidant sensitivity. Heme oxygenase has both pro- and antioxidant properties. Free Radic Biol Med 2000; 28: 289-309.

1582 Current Drug Targets, 2010, Vol. 11, No. 12 Wagener et al.
[28] Jeney V, Balla J, Yachie A, et al. Pro-oxidant and cytotoxic effects of circulating heme. Blood 2002; 100: 879-87.
[29] Nakajima O, Takahashi S, Harigae H, et al. Heme deficiency in erythroid lineage causes differentiation arrest and cytoplasmic iron overload. EMBO J 1999; 18: 6282-9.
[30] Balla G, Jacob HS, Eaton JW, Belcher JD, Vercellotti GM. Hemin: a possible physiological mediator of low density lipoprotein oxidation and endothelial injury. Arterioscler Thromb 1991; 11: 1700-11.
[31] Nath KA, Balla J, Croatt AJ, Vercellotti GM. Heme protein-mediated renal injury: a protective role for 21-aminosteroids in vitro and in vivo. Kidney Int 1995; 47: 592-602.
[32] Green D, Ts'ao CH. Hematin: effects on hemostasis. J Lab Clin Med 1990; 115: 144-7.
[33] Wagener FA, Feldman E, de Witte T, Abraham NG. Heme induces the expression of adhesion molecules ICAM-1, VCAM-1, and E selectin in vascular endothelial cells. Proc Soc Exp Biol Med 1997; 216: 456-63.
[34] Wagener FA, da Silva JL, Farley T, et al. Differential effects of heme oxygenase isoforms on heme mediated endothelial ICAM-1 expression. J Pharmacol Exp Ther 1999; 291: 416-23.
[35] Wagener FA, Eggert A, Boerman OC, et al. Heme is a potent inducer of inflammation in mice and is counteracted by heme oxygenase. Blood 2001; 98: 1802-11.
[36] Belcher JD, Mahaseth H, Welch TE, et al. Heme oxygenase-1 is a modulator of inflammation and vaso-occlusion in transgenic sickle mice. J Clin Invest 2006; 116: 808-16.
[37] Vinchi F, Gastaldi S, Silengo L, Altruda F, Tolosano E. Hemopexin prevents endothelial damage and liver congestion in a mouse model of heme overload. Am J Pathol 2008; 173: 289-99.
[38] Lavrovsky Y, Chatterjee B, Clark RA, Roy AK. Role of redox-regulated transcription factors in inflammation, aging and age-related diseases. Exp Gerontol 2000; 35: 521-32.
[39] Hancock WW, Buelow R, Sayegh MH, Turka LA. Antibody-induced transplant arteriosclerosis is prevented by graft expression of anti-oxidant and anti-apoptotic genes. Nat Med 1998; 4: 1392-6.
[40] Tolosano E, Fagoonee S, Hirsch E, et al. Enhanced splenomegaly and severe liver inflammation in haptoglobin/hemopexin double-null mice after acute hemolysis. Blood 2002; 100: 4201-8.
[41] Wagener FA, Abraham NG, van Kooyk Y, de Witte T, Figdor CG. Heme-induced cell adhesion in the pathogenesis of sickle-cell disease and inflammation. Trends Pharmacol Sci 2001; 22: 52-4.
[42] Pamplona A, Hanscheid T, Epiphanio S, Mota MM, Vigario AM. Cerebral malaria and the hemolysis/methemoglobin/heme hypothesis: shedding new light on an old disease. Int J Biochem Cell Biol 2009; 41: 711-6.
[43] Takahashi T, Shimizu H, Morimatsu H, et al. Heme oxygenase-1: a fundamental guardian against oxidative tissue injuries in acute inflammation. Mini reviews in medicinal chemistry 2007; 7: 745-53.
[44] Ferreira A, Balla J, Jeney V, Balla G, Soares MP. A central role for free heme in the pathogenesis of severe malaria: the missing link? J Mol Med 2008; 86: 1097-111.
[45] Pamplona A, Ferreira A, Balla J, et al. Heme oxygenase-1 and carbon monoxide suppress the pathogenesis of experimental cerebral malaria. Nat Med 2007; 13: 703-10.
[46] Porto BN, Alves LS, Fernandez PL, et al. Heme induces neutrophil migration and reactive oxygen species generation through signaling pathways characteristic of chemotactic receptors. J Biol Chem 2007; 282: 24430-6.
[47] Arruda MA, Rossi AG, de Freitas MS, Barja-Fidalgo C, Graca-Souza AV. Heme inhibits human neutrophil apoptosis: involvement of phosphoinositide 3-kinase, MAPK, and NF-kappaB. J Immunol 2004; 173: 2023-30.
[48] Graca-Souza AV, Arruda MA, de Freitas MS, Barja-Fidalgo C, Oliveira PL. Neutrophil activation by heme: implications for inflammatory processes. Blood 2002; 99: 4160-5.
[49] Balla G, Vercellotti G, Eaton JW, Jacob HS. Heme uptake by endothelium synergizes polymorphonuclear granulocyte-mediated damage. Trans Assoc Am Phys 1990; 103: 174-9.
[50] Seixas E, Gozzelino R, Chora A, et al. Heme oxygenase-1 affords protection against noncerebral forms of severe malaria. Proc Natl Acad Sci USA 2009; 106: 15837-42.
[51] Figueiredo RT, Fernandez PL, Mourao-Sa DS, et al. Characterization of heme as activator of Toll-like receptor 4. J Biol Chem 2007; 282: 20221-9.
[52] Parroche P, Lauw FN, Goutagny N, et al. Malaria hemozoin is immunologically inert but radically enhances innate responses by presenting malaria DNA to Toll-like receptor 9. Proc Natl Acad Sci USA 2007; 104: 1919-24.
[53] Cotran RS, Mayadas-Norton T. Endothelial adhesion molecules in health and disease. Pathol Biol (Paris) 1998; 46: 164-70.
[54] Taketani S, Immenschuh S, Go S, et al. Hemopexin from four species inhibits the association of heme with cultured hepatoma cells or primary rat hepatocytes exhibiting a small number of species specific hemopexin receptors. Hepatology 1998; 27: 808-14.
[55] Tolosano E, Hirsch E, Patrucco E, et al. Defective recovery and severe renal damage after acute hemolysis in hemopexin-deficient mice. Blood 1999; 94: 3906-14.
[56] Immenschuh S, Iwahara S, Satoh H, et al. Expression of the mRNA of heme-binding protein 23 is coordinated with that of heme oxygenase-1 by heme and heavy metals in primary rat hepatocytes and hepatoma cells. Biochemistry 1995; 34: 13407-11.
[57] Krishnamurthy P, Xie T, Schuetz JD. The role of transporters in cellular heme and porphyrin homeostasis. Pharmacol Ther 2007; 114: 345-58.
[58] Krishnamurthy P, Schuetz JD. The ABC transporter Abcg2/Bcrp: role in hypoxia mediated survival. Biometals 2005; 18: 349-58.
[59] Van Summeren F, Russel FG, Masereeuw R, Wagener FA. Heme oxygenase-1 and breast cancer resistance protein as modulators of heme-induced cytotoxicity. Naunyn-Schmiedebergs Archives of Pharmacology 2009; 380: 262.
[60] Staud F, Pavek P. Breast cancer resistance protein (BCRP/ ABCG2). The international journal of biochemistry & cell biology 2005; 37: 720-5.
[61] Krishnamurthy P, Schuetz JD. Role of ABCG2/BCRP in biology and medicine. Annual review of pharmacology and toxicology 2006; 46: 381-410.
[62] Krishnamurthy P, Ross DD, Nakanishi T, et al. The stem cell marker Bcrp/ABCG2 enhances hypoxic cell survival through interactions with heme. J Biol Chem 2004; 279: 24218-25.
[63] Tenhunen R, Marver HS, Schmid R. The enzymatic conversion of heme to bilirubin by microsomal heme oxygenase. Proc Natl Acad Sci USA 1968; 61: 748-55.
[64] Eisenstein RS, Garcia-Mayol D, Pettingell W, Munro HN. Regulation of ferritin and heme oxygenase synthesis in rat fibroblasts by different forms of iron. Proc Natl Acad Sci USA 1991; 88: 688-92.
[65] Vile GF, Basu-Modak S, Waltner C, Tyrrell RM. Heme oxygenase 1 mediates an adaptive response to oxidative stress in human skin fibroblasts. Proc Natl Acad Sci USA 1994; 91: 2607-10.
[66] Balla G, Jacob HS, Balla J, et al. Ferritin: a cytoprotective antioxidant strategem of endothelium. J Biol Chem 1992; 267: 18148-53.
[67] Abraham NG, Lin JH, Schwartzman ML, Levere RD, Shibahara S. The physiological significance of heme oxygenase. Int J Biochem 1988; 20: 543-58.
[68] Willis D, Moore AR, Frederick R, Willoughby DA. Heme oxygenase: a novel target for the modulation of the inflammatory response. Nat Med 1996; 2: 87-90.
[69] Soares MP, Lin Y, Anrather J, et al. Expression of heme oxygenase-1 can determine cardiac xenograft survival. Nat Med 1998; 4: 1073-7.
[70] Brouard S, Otterbein LE, Anrather J, et al. Carbon monoxide generated by heme oxygenase 1 suppresses endothelial cell apoptosis. J Exp Med 2000; 192: 1015-26.
[71] Otterbein LE, Soares MP, Yamashita K, Bach FH. Heme oxygenase-1: unleashing the protective properties of heme. Trends Immunol 2003; 24: 449-55.
[72] Siow RC, Sato H, Mann GE. Heme oxygenase-carbon monoxide signalling pathway in atherosclerosis: anti-atherogenic actions of bilirubin and carbon monoxide? Cardiovasc Res 1999; 41: 385-94.
[73] Braggins PE, Trakshel GM, Kutty RK, Maines MD. Characterization of two heme oxygenase isoforms in rat spleen: comparison with the hematin-induced and constitutive isoforms of the liver. Biochem Biophys Res Commun 1986; 141: 528-33.
[74] McCoubrey WK, Jr., Huang TJ, Maines MD. Isolation and characterization of a cDNA from the rat brain that encodes hemoprotein heme oxygenase-3. Eur J Biochem 1997; 247: 725-32.
[75] Willis D. Expression and modulatory effects of heme oxygenase in acute inflammation in the rat. Inflamm Res 1995; 44: S218-20.

The Heme-Heme Oxygenase System in Wound Healing Current Drug Targets, 2010, Vol. 11, No. 12 1583
[76] Duckers HJ, Boehm M, True AL, et al. Heme oxygenase-1 protects against vascular constriction and proliferation. Nat Med 2001; 7: 693-8.
[77] Takahashi T, Shimizu H, Morimatsu H, et al. Heme Oxygenase-1 is an Essential Cytoprotective Component in Oxidative Tissue Injury Induced by Hemorrhagic Shock. J Clin Biochem Nut 2009; 44: 28-40.
[78] Hayashi S, Takamiya R, Yamaguchi T, et al. Induction of heme oxygenase-1 suppresses venular leukocyte adhesion elicited by oxidative stress: role of bilirubin generated by the enzyme. Circ Res 1999; 85: 663-71.
[79] Vachharajani TJ, Work J, Issekutz AC, Granger DN. Heme oxygenase modulates selectin expression in different regional vascular beds. Am J Physiol Heart Circ Physiol 2000; 278: H1613-7.
[80] Rucker M, Schafer T, Roesken F, et al. Reduction of inflammatory response in composite flap transfer by local stress conditioning-induced heat-shock protein 32. Surgery 2001; 129: 292-301.
[81] Zhong JL, Raval C, Edwards GP, Tyrrell RM. A role for Bach1 and HO-2 in suppression of basal and UVA-induced HO-1 expression in human keratinocytes. Free Radic Biol Med 2010; 48: 196-206.
[82] Kartikasari AE, Wagener FA, Yachie A, et al. Hepcidin suppression and defective iron recycling account for dysregulation of iron homeostasis in heme oxygenase-1 deficiency. J Cell Mol Med 2009; 13: 23091-102.
[83] Kawashima A, Oda Y, Yachie A, Koizumi S, Nakanishi I. Heme oxygenase-1 deficiency: The first autopsy case. Hum Pathol 2002; 33: 125-30.
[84] Yachie A, Niida Y, Wada T, et al. Oxidative stress causes enhanced endothelial cell injury in human heme oxygenase-1 deficiency. J Clin Invest 1999; 103: 129-35.
[85] Seta F, Bellner L, Rezzani R, et al. Heme oxygenase-2 is a critical determinant for execution of an acute inflammatory and reparative response. Am J Pathol 2006; 169: 1612-23.
[86] Scharstuhl A, Pennings SW, Te Paske J, et al. Dermal wound contraction is delayed in heme oxygenase-2 knock-out mice, but increased in hyperbilirubinemic rats. Wound Repair Regen 2010; in press.
[87] Maines MD. The heme oxygenase system: a regulator of second messenger gases. Annu Rev Pharmacol Toxicol 1997; 37: 517-54.
[88] Hanselmann C, Mauch C, Werner S. Haem oxygenase-1: a novel player in cutaneous wound repair and psoriasis? Biochem J 2001; 353: 459-66.
[89] Tyrrell RM. UVA (320-380 nm) radiation as an oxidative stress London: Academic Press 1991.
[90] Keyse SM, Tyrrell RM. Both near ultraviolet radiation and the oxidizing agent hydrogen peroxide induce a 32-kDa stress protein in normal human skin fibroblasts. J Biol Chem 1987; 262: 14821-5.
[91] Keyse SM, Tyrrell RM. Heme oxygenase is the major 32-kDa stress protein induced in human skin fibroblasts by UVA radiation, hydrogen peroxide, and sodium arsenite. Proc Natl Acad Sci U S A 1989; 86: 99-103.
[92] Allanson M, Reeve VE. Carbon monoxide signalling reduces photocarcinogenesis in the hairless mouse. Cancer Immunol Immunother 2007; 56: 1807-15.
[93] Applegate LA, Noel A, Vile G, Frenk E, Tyrrell RM. Two genes contribute to different extents to the heme oxygenase enzyme activity measured in cultured human skin fibroblasts and keratinocytes: implications for protection against oxidant stress. Photochem Photobiol 1995; 61: 285-91.
[94] Sun J, Brand M, Zenke Y, et al. Heme regulates the dynamic exchange of Bach1 and NF-E2-related factors in the Maf transcription factor network. Proc Natl Acad Sci U S A 2004; 101: 1461-6.
[95] Zenke-Kawasaki Y, Dohi Y, Katoh Y, et al. Heme induces ubiquitination and degradation of the transcription factor Bach1. Mol Cell Biol 2007; 27: 6962-71.
[96] Kvam E, Noel A, Basu-Modak S, Tyrrell RM. Cyclooxygenase dependent release of heme from microsomal hemeproteins correlates with induction of heme oxygenase 1 transcription in human fibroblasts. Free Radic Biol Med 1999; 26: 511-7.
[97] Zhong JL, Edwards GP, Raval C, Li H, Tyrrell RM. The role of Nrf2 in ultraviolet A mediated heme oxygenase 1 induction in human skin fibroblasts. Photochem Photobiol Sci 2010; 9: 18-24.
[98] Zhong JL, Raval C, Edwards GP, Tyrrell RM. A role for Bach1 and HO-2 in suppression of basal and UVA-induced HO-1 expression in human keratinocytes. Free Radic Biol Med 2010; 48: 196-206.
[99] Langlois MR, Delanghe JR. Biological and clinical significance of haptoglobin polymorphism in humans. Clin Chem 1996; 42: 1589-600.
[100] Braeckman L, De Bacquer D, Delanghe J, Claeys L, De Backer G. Associations between haptoglobin polymorphism, lipids, lipoproteins and inflammatory variables. Atherosclerosis 1999; 143: 383-8.
[101] Muller Eberhard U, Liem HH. Hemopexin, the heme-binding serum beta-glycoprotein. La Ricerca Clin Lab 1975; 5: 275-91.
[102] Wagener FA, Toonen EJ, Wigman L, et al. HMOX1 promoter polymorphism modulates the relationship between disease activity and joint damage in rheumatoid arthritis. Arthritis Rheum 2008; 58: 3388-93.
[103] Exner M, Schillinger M, Minar E, et al. Heme oxygenase-1 gene promoter microsatellite polymorphism is associated with restenosis after percutaneous transluminal angioplasty. J Endovasc Ther 2001; 8: 433-40.
[104] Wagener FA, Dekker D, Berden JH, Scharstuhl A, van der Vlag J. The role of reactive oxygen species in apoptosis of the diabetic kidney. Apoptosis 2009; 14: 1451-8.
[105] Falanga V. Wound healing and its impairment in the diabetic foot. Lancet 2005; 366: 1736-43.
[106] Gurtner GC, Werner S, Barrandon Y, Longaker MT. Wound repair and regeneration. Nature 2008; 453: 314-21.
[107] Quan S, Kaminski PM, Yang L, et al. Heme oxygenase-1 prevents superoxide anion-associated endothelial cell sloughing in diabetic rats. Biochem Biophys Res Commun 2004; 315: 509-16.
[108] Lerman OZ, Galiano RD, Armour M, Levine JP, Gurtner GC. Cellular dysfunction in the diabetic fibroblast: impairment in migration, vascular endothelial growth factor production, and response to hypoxia. Am J Pathol 2003; 162: 303-12.
[109] Swift ME, Kleinman HK, DiPietro LA. Impaired wound repair and delayed angiogenesis in aged mice. Lab Invest 1999; 79: 1479-87.
[110] Goren I, Muller E, Schiefelbein D, et al. Akt1 controls insulin-driven VEGF biosynthesis from keratinocytes: implications for normal and diabetes-impaired skin repair in mice. J Invest Dermatol 2009; 129: 752-64.
[111] Liu ZJ, Velazquez OC. Hyperoxia, endothelial progenitor cell mobilization, and diabetic wound healing. Antioxid Redox Signal 2008; 10: 1869-82.
[112] Grochot-Przeczek A, Lach R, Mis J, et al. Heme oxygenase-1 accelerates cutaneous wound healing in mice. PloS One 2009; 4: e5803.
[113] Altavilla D, Saitta A, Cucinotta D, et al. Inhibition of lipid peroxidation restores impaired vascular endothelial growth factor expression and stimulates wound healing and angiogenesis in the genetically diabetic mouse. Diabetes 2001; 50: 667-74.
[114] Shukla A, Rasik AM, Patnaik GK. Depletion of reduced glutathione, ascorbic acid, vitamin E and antioxidant defence enzymes in a healing cutaneous wound. Free Radic Res 1997; 26: 93-101.
[115] Haider A, Olszanecki R, Gryglewski R, et al. Regulation of cyclooxygenase by the heme-heme oxygenase system in microvessel endothelial cells. J Pharmacol Exp Ther 2002; 300: 188-94.
[116] Witte MB, Barbul A. Role of nitric oxide in wound repair. Am J Surg 2002; 183: 406-12.
[117] Frank S, Kampfer H, Wetzler C, Pfeilschifter J. Nitric oxide drives skin repair: novel functions of an established mediator. Kidney Int 2002; 61: 882-8.
[118] Kampfer H, Brautigam L, Geisslinger G, Pfeilschifter J, Frank S. Cyclooxygenase-1-coupled prostaglandin biosynthesis constitutes an essential prerequisite for skin repair. J Invest Dermatol 2003; 120: 880-90.
[119] Yamasaki K, Edington HD, McClosky C, et al. Reversal of impaired wound repair in iNOS-deficient mice by topical adenoviral-mediated iNOS gene transfer. J Clin Invest 1998; 101: 967-71.
[120] Moncada S, Palmer RM, Higgs EA. Nitric oxide: physiology, pathophysiology, and pharmacology. Pharmacol Rev 1991; 43: 109-42.

1584 Current Drug Targets, 2010, Vol. 11, No. 12 Wagener et al.
[121] Albina JE, Mills CD, Henry WL, Jr., Caldwell MD. Temporal expression of different pathways of 1-arginine metabolism in healing wounds. J Immunol 1990; 144: 3877-80.
[122] Kampfer H, Pfeilschifter J, Frank S. Expression and activity of arginase isoenzymes during normal and diabetes-impaired skin repair. J Invest Dermatol 2003; 121: 1544-51.
[123] Moulin V, Larochelle S, Langlois C, et al. Normal skin wound and hypertrophic scar myofibroblasts have differential responses to apoptotic inductors. J Cell Physiol 2004; 198: 350-8.
[124] Aarabi S, Bhatt KA, Shi Y, et al. Mechanical load initiates hypertrophic scar formation through decreased cellular apoptosis. FASEB J 2007; 21: 3250-61.
[125] Walczak H, Krammer PH. The CD95 (APO-1/Fas) and the TRAIL (APO-2L) apoptosis systems. Exp Cell Res 2000; 256: 58-66.
[126] Li H, Zhu H, Xu CJ, Yuan J. Cleavage of BID by caspase 8 mediates the mitochondrial damage in the Fas pathway of apoptosis. Cell 1998; 94: 491-501.
[127] Zou H, Henzel WJ, Liu X, Lutschg A, Wang X. Apaf-1, a human protein homologous to C. elegans CED-4, participates in cytochrome c-dependent activation of caspase-3. Cell 1997; 90: 405-13.
[128] Ashkenazi A, Dixit VM. Death receptors: signaling and modulation. Science 1998; 281: 1305-8.
[129] Jin Z, El-Deiry WS. Overview of cell death signaling pathways. Cancer Biol Ther 2005; 4: 139-63.
[130] Green DR, Kroemer G. The pathophysiology of mitochondrial cell death. Science 2004; 305: 626-9.
[131] Crompton M. Bax, Bid and the permeabilization of the mitochondrial outer membrane in apoptosis. Curr Opin Cell Biol 2000; 12: 414-9.
[132] Shimizu S, Narita M, Tsujimoto Y. Bcl-2 family proteins regulate the release of apoptogenic cytochrome c by the mitochondrial channel VDAC. Nature 1999; 399: 483-7.
[133] Kroemer G, Martin SJ. Caspase-independent cell death. Nat Med 2005; 11: 725-30.
[134] Ryter SW, Choi AM. Heme oxygenase-1/carbon monoxide: from metabolism to molecular therapy. Am J Respir Cell Mol Biol 2009; 41: 251-60.
[135] Gozzelino R, Jeney V, Soares MP. Mechanisms of cell protection by heme oxygenase-1. Annu Rev Pharmacol Toxicol 2010; 50: 323-54.
[136] Foresti R, Green CJ, Motterlini R. Generation of bile pigments by haem oxygenase: a refined cellular strategy in response to stressful insults. Biochem Soc Symp 2004; 71: 177-92.
[137] Petrache I, Otterbein LE, Alam J, Wiegand GW, Choi AM. Heme oxygenase-1 inhibits TNF-alpha-induced apoptosis in cultured fibroblasts. Am J Physiol Lung Cell Mol Physiol 2000; 278: L312-9.
[138] Brouard S, Berberat PO, Tobiasch E, et al. Heme oxygenase-1-derived carbon monoxide requires the activation of transcription factor NF-kappa B to protect endothelial cells from tumor necrosis factor-alpha-mediated apoptosis. J Biol Chem 2002; 277: 17950-61.
[139] McDaid J, Yamashita K, Chora A, et al. Heme oxygenase-1 modulates the allo-immune response by promoting activation-induced cell death of T cells. FASEB J 2005; 19: 458-60.
[140] Song R, Zhou Z, Kim PK, et al. Carbon monoxide promotes Fas/CD95-induced apoptosis in Jurkat cells. J Biol Chem 2004; 279: 44327-34.
[141] Thom SR, Fisher D, Xu YA, Notarfrancesco K, Ischiropoulos H. Adaptive responses and apoptosis in endothelial cells exposed to carbon monoxide. Proc Natl Acad Sci USA 2000; 97: 1305-10.
[142] Scharstuhl A, Mutsaers HA, Pennings SW, et al. Curcumin-induced fibroblast apoptosis and in vitro wound contraction are regulated by antioxidants and heme oxygenase: implications for scar formation. J Cell Mol Med 2009; 13: 712-25.
[143] Scharstuhl A, Mutsaers HA, Pennings SW, Russel FG, Wagener FA. Involvement of VDAC, Bax and ceramides in the efflux of AIF from mitochondria during curcumin-induced apoptosis. PloS One 2009; 4: e6688.
[144] Tourkina E, Gooz P, Oates JC, et al. Curcumin-induced apoptosis in scleroderma lung fibroblasts: role of protein kinase cepsilon. Am J Respir Cell Mol Biol 2004; 31: 28-35.
[145] Ma LJ, You Y, Bai BX, Li YZ. Therapeutic effects of heme oxygenase-1 on psoriasiform skin lesions in guinea pigs. Arch Dermatol Res 2009; 301: 459-66.
[146] Atzori L, Chua F, Dunsmore SE, et al. Attenuation of bleomycin induced pulmonary fibrosis in mice using the heme oxygenase inhibitor Zn-deuteroporphyrin IX-2,4-bisethylene glycol. Thorax 2004; 59: 217-23.
[147] Tsuburai T, Suzuki M, Nagashima Y, et al. Adenovirus-mediated transfer and overexpression of heme oxygenase 1 cDNA in lung prevents bleomycin-induced pulmonary fibrosis via a Fas-Fas ligand-independent pathway. Hum Gene Ther 2002; 13: 1945-60.
[148] Zhou Z, Song R, Fattman CL, et al. Carbon monoxide suppresses bleomycin-induced lung fibrosis. Am J Pathol 2005; 166: 27-37.
[149] Zheng L, Zhou Z, Lin L, et al. Carbon monoxide modulates alpha-smooth muscle actin and small proline rich-1a expression in fibrosis. Am J Respir Cell Mol Biol 2009; 41: 85-92.
[150] Wang HD, Yamaya M, Okinaga S, et al. Bilirubin ameliorates bleomycin-induced pulmonary fibrosis in rats. Am J Respir Crit Care Med 2002; 165: 406-11.
[151] Li L, Grenard P, Nhieu JT, et al. Heme oxygenase-1 is an antifibrogenic protein in human hepatic myofibroblasts. Gastroenterology 2003; 125: 460-9.
[152] Tsui TY, Lau CK, Ma J, et al. rAAV-mediated stable expression of heme oxygenase-1 in stellate cells: a new approach to attenuate liver fibrosis in rats. Hepatology 2005; 42: 335-42.
[153] Wang F, Duan ZJ, Sun YJ. Influence of heme oxygenase-1 expression on immune liver fibrosis induced by cobalt protoporphyrin in rats. World J Gastroenterol 2009; 15: 3009-14.
[154] Ndisang JF, Jadhav A. Upregulating the heme oxygenase system suppresses left ventricular hypertrophy in adult spontaneously hypertensive rats for 3 months. J Cardiac Failure 2009; 15: 616-28.
[155] Jadhav A, Torlakovic E, Ndisang JF. Interaction among heme oxygenase, nuclear factor-kappaB, and transcription activating factors in cardiac hypertrophy in hypertension. Hypertension 2008; 52: 910-7.
[156] Liu X, Pachori AS, Ward CA, et al. Heme oxygenase-1 (HO-1) inhibits postmyocardial infarct remodeling and restores ventricular function. FASEB J 2006; 20: 207-16.
[157] Gaedeke J, Noble NA, Border WA. Curcumin blocks fibrosis in anti-Thy 1 glomerulonephritis through up-regulation of heme oxygenase 1. Kidney Int 2005; 68: 2042-9.
[158] Kie JH, Kapturczak MH, Traylor A, Agarwal A, Hill-Kapturczak N. Heme oxygenase-1 deficiency promotes epithelial-mesenchymal transition and renal fibrosis. J Am Soc Nephrol 2008; 19: 1681-91.
[159] Devesa I, Ferrandiz ML, Terencio MC, et al. Influence of heme oxygenase 1 modulation on the progression of murine collagen-induced arthritis. Arthritis Rheum 2005; 52: 3230-8.
[160] Lin CW, Shen SC, Hou WC, Yang LY, Chen YC. Heme oxygenase-1 inhibits breast cancer invasion via suppressing the expression of matrix metalloproteinase-9. Mol Cancer Ther 2008; 7: 1195-206.
[161] Kim DH, Kim JH, Kim EH, et al. 15-Deoxy-Delta12,14-prostaglandin J2 upregulates the expression of heme oxygenase-1 and subsequently matrix metalloproteinase-1 in human breast cancer cells: possible roles of iron and ROS. Carcinogenesis 2009; 30: 645-54.
[162] Guillen M, Megias J, Gomar F, Alcaraz M. Haem oxygenase-1 regulates catabolic and anabolic processes in osteoarthritic chondrocytes. J Pathol 2008; 214: 515-22.
[163] Benallaoua M, Francois M, Batteux F, et al. Pharmacologic induction of heme oxygenase 1 reduces acute inflammatory arthritis in mice. Arthritis Rheu m 2007; 56: 2585-94.
[164] Desmard M, Amara N, Lanone S, Motterlini R, Boczkowski J. Carbon monoxide reduces the expression and activity of matrix metalloproteinases 1 and 2 in alveolar epithelial cells. Cell Mol Biol (Noisy-le-grand) 2005; 51: 403-8.
[165] Rossiter H, Barresi C, Pammer J, et al. Loss of vascular endothelial growth factor a activity in murine epidermal keratinocytes delays wound healing and inhibits tumor formation. Cancer Res 2004; 64: 3508-16.
[166] Zamboni P, Gemmati D. Clinical implications of gene polymorphisms in venous leg ulcer: a model in tissue injury and reparative process. Thromb Haemost 2007; 98: 131-7.
[167] Dulak J, Jozkowicz A, Foresti R, et al. Heme oxygenase activity modulates vascular endothelial growth factor synthesis in vascular smooth muscle cells. Antioxid Redox Signal 2002; 4: 229-40.
[168] Jozkowicz A, Huk I, Nigisch A, et al. Effect of prostaglandin-J(2) on VEGF synthesis depends on the induction of heme oxygenase-1. Antioxid Redox Signal 2002; 4: 577-85.

The Heme-Heme Oxygenase System in Wound Healing Current Drug Targets, 2010, Vol. 11, No. 12 1585
[169] Cisowski J, Loboda A, Jozkowicz A, et al. Role of heme oxygenase-1 in hydrogen peroxide-induced VEGF synthesis: effect of HO-1 knockout. Biochem Biophys Res Commun 2005; 326: 670-6.
[170] Jazwa A, Loboda A, Golda S, et al. Effect of heme and heme oxygenase-1 on vascular endothelial growth factor synthesis and angiogenic potency of human keratinocytes. Free Radic Biol Med 2006; 40: 1250-63.
[171] Lin HH, Chen YH, Chang PF, et al. Heme oxygenase-1 promotes neovascularization in ischemic heart by coinduction of VEGF and SDF-1. J Mol Cell Cardiol 2008; 45: 44-55.
[172] Bussolati B, Ahmed A, Pemberton H, et al. Bifunctional role for VEGF-induced heme oxygenase-1 in vivo: induction of angiogenesis and inhibition of leukocytic infiltration. Blood 2004; 103: 761-6.
[173] Deshane J, Chen S, Caballero S, et al. Stromal cell-derived factor 1 promotes angiogenesis via a heme oxygenase 1-dependent mechanism. J Exp Med 2007; 204: 605-18.
[174] Gueron G, De Siervi A, Ferrando M, et al. Critical role of endogenous heme oxygenase 1 as a tuner of the invasive potential of prostate cancer cells. Mol Cancer Res 2009; 7: 1745-55.
[175] Was H, Dulak J, Jozkowicz A. Heme oxygenase-1 in tumor biology and therapy. Curr Drug Targets 2010; 11(12): 1551-70.
[176] Michaels Jt, Churgin SS, Blechman KM, et al. db/db mice exhibit severe wound-healing impairments compared with other murine diabetic strains in a silicone-splinted excisional wound model. Wound Repair Regen 2007; 15: 665-70.
[177] Patil K, Bellner L, Cullaro G, et al. Heme oxygenase-1 induction attenuates corneal inflammation and accelerates wound healing after epithelial injury. Invest Ophthalmol Vis Sci 2008; 49: 3379-86.
[178] Nolan VG, Adewoye A, Baldwin C, et al. Sickle cell leg ulcers: associations with haemolysis and SNPs in Klotho, TEK and genes of the TGF-beta/BMP pathway. Br J Haematol 2006; 133: 570-8.
[179] Nath KA, Vercellotti GM, Grande JP, et al. Heme protein-induced chronic renal inflammation: suppressive effect of induced heme oxygenase-1. Kidney Int 2001; 59: 106-17.
[180] Bussolati B, Mason JC. Dual role of VEGF-induced heme-oxygenase-1 in angiogenesis. Antioxid Redox Signal 2006; 8: 1153-63.
[181] Dulak J, Loboda A, Jozkowicz A. Effect of heme oxygenase-1 on vascular function and disease. Curr Opin Lipidol 2008; 19: 505-12.
[182] Clark JE, Green CJ, Motterlini R. Involvement of the heme oxygenase-carbon monoxide pathway in keratinocyte proliferation. Biochem Biophys Res Commun 1997; 241: 215-20.
[183] Jozkowicz A, Huk I, Nigisch A, et al. Heme oxygenase and angiogenic activity of endothelial cells: stimulation by carbon monoxide and inhibition by tin protoporphyrin-IX. Antioxid Redox Signal 2003; 5: 155-62.
[184] Loboda A, Jazwa A, Grochot-Przeczek A, et al. Heme oxygenase-1 and the vascular bed: from molecular mechanisms to therapeutic opportunities. Antioxid Redox Signal 2008; 10: 1767-812.
[185] Nagai MK, Embil JM. Becaplermin: recombinant platelet derived growth factor, a new treatment for healing diabetic foot ulcers. Expert Opin Biol Ther 2002; 2: 211-8.
[186] Durante W, Peyton KJ, Schafer AI. Platelet-derived growth factor stimulates heme oxygenase-1 gene expression and carbon monoxide production in vascular smooth muscle cells. Arterioscler Thromb Vasc Biol 1999; 19: 2666-72.
[187] Lorenz HP, Longaker MT. In utero surgery for cleft lip/palate: minimizing the "Ripple Effect" of scarring. J Craniofac Surg 2003; 14: 504-11.
Received: January 28, 2010 Revised: March 18, 2010 Accepted: May 31, 2010