Embed Size (px)
Citation preview
Central Annals of Sports Medicine and Research
Cite this article: Çetinkaya E, Özcan Ç, Gursu SS (2017) Current Concepts in Management of Femoroacetabuler Impingement. Ann Sports Med Res 4(1): 1100.
*Corresponding authorEngin Çetinkaya, Department of Orthopedics and Traumatology, Baltalimani Bone Diseases Training and Research Hospital, 34000, Istanbul, Turkey, Fax: 90 212 323 70 75; Tel: 90 506 328 58 58; Email:
Submitted: 03 February 2017
Accepted: 06 March 2017
Published: 08 March 2017
ISSN: 2379-0571
Copyright© 2017 Çetinkaya et al.
OPEN ACCESS
Keywords•Femoroacetabular impingment•FAI•Hip arthroscopy•Safe hip dislocation
Abstract
Femoroacetabular impingement (FAI) is a progressive pathology of hip joint affecting young adults causing hip pain and osteoarthritis. FAI results from contact secondary to abnormal morphology of proximal femur, femoral head-neck junction and acetabular rim. Two types of femoroacetabular impingement have been described: Pincer ve Cam impingement. Pincer impingement is caused by the overcoverage of the acetabulum. On the other hand, Cam impingement develops as the result of abnormal spherity of femoral head- neck junction which usually occurs at the anterosuperior part of femoral neck. This review will provide the framework fort he diagnosis and management of FAI from the perspectives of the practising ortopedic surgeon. Strategies for safe and succesful diagnosis and treatment of FAI are presented.
Review Article
Current Concepts in Management of Femoroacetabuler ImpingementEngin Çetinkaya*, Çagri Özcan, and Sukru Sarper GursuDepartment of Orthopedics and Traumatology, Baltalimani Bone Diseases Training and Research Hospital, Turkey
INTRODUCTIONFemoroacetabular impingement (FAI) is a progressive
pathology of hip joint affecting young adults causing hip pain and osteoarthritis. FAIresults from contact secondary to abnormal morphology of proximal femur, femoral head-neck junction and acetabular rim. The incidence of FAI is reported to be 10-15% in literature. Impingement was first described by Smith Peterson in 1936 [1]. Ganz et al. [2] described the FAI as the most common cause of premature major osteoarthritis. This hip pathology, with repetitive microtraumas, results with acetabular degeneration, labral tear and joint damage. Three types of femoroacetabular impingement have been described: Pincer lesions, Cam lesions and mixed tip lesions impingement.Pincer impingement is caused by the overcoverage of the acetabulum. On the other hand, Cam impingement develops as the result of abnormal spherity of femoral head- neck junction which usually occurs at the anterosuperior part of femoral neck [2,3]. In Cam impingement,therecurrent irritation of the anterosuperior part of acetabulumby the abnormal femoral head leads to acetabular cartilage damage with forced hip motions, especially flexion of the hip. In Pincer impingement, the labrum degenerates throughpinching between acetabular rim and femoral neck during flexion of the hip. This degenerating labrum may be ossified [4]. A combination of both forms (mixed pattern) can be detected in the same hip joint.Combination of Cam and pincer lesions can also ocur which actually is the most common presentation [3-7].
Pathology of FAI
FAI is essentially a dynamic problem. Normally, hip joint has a space between the femoral head neck junction and the acetabular rim provides unhindered hip movement. This is achieved with an offset. The normal head neck offset is 9 mm. If this offset is distorted, a mechanical blockage occurs in the hip joint. In addition, overexposure or retroversion of the acetabulum may cause mechanical blockage of the hip. Many diseases can lead to FAI due to these two pathological causes.
The Etiology of FAI
Various morphologic abnormalities of acetabulum and femoral neck may predispose to FAI. The most common predisposing factor of Cam impingement is delayed seperation of femoral head physis and trochanteric physis or abnormal pyhseal scar in femur neck after eccentric closure of femoral head epiphysis [5]. Other than these, subclinical SCFE, Perthes disease, coxa vara and posttraumatic deformity of femoral headmight contribute to Cam impingement [6]. The acetabular retroversion, coxa profunda, and acetabular protrusion have been found to be predisposing factors for Pincer impingement [6]. Genetic factors may also play a role, the frequency of Pincer or Cam impingement is much more higher in the siblings of the impingement patients with respect to normal population [7].
The Clinical Findings of FAI
FAI is a disease of young and physically active patients. Clinical findings vary in sypmtomatic FAI; the most frequent

Central
Çetinkaya et al. (2017)Email:
Ann Sports Med Res 4(1): 1100 (2017) 2/6
complaint is groin pain. Patients with posterior impingement may experience gluteus medius and trochanteric bursitis pain [4]. Impingement type could be different according to sex. Posterior impingement is more common in middle-aged women whereas anterior impingement is more common in younger men [8,9]. It is also thought that genetic factors may be risk factors in the development of FAI [10] but in our knowledge there is no clear evidence of genetic transit. In the Pincer type impingment, the posterior impingement test the hip is flexed to 90 degrees, abducted and externally rotated (FABER) [6,11,12]. The patient experiences hip pain with femoral neck jamming against posterior acetabular margin. In patients with acetabulum labral lesion, painful hip clicking and locking may be detected. These complaints are aggrevated by ascending stairs, prolonged periods of sitting on chair, sports straining the hip flexion [13].
Anterior impingement occurs when the femur head sphericity is distorted and the diameter of the femur neck is increased pathologically, causing damage to the labrum of the acetabulum anterior wall during flexion and internal rotation of the hip joint. Anterior impingement test (FADIR) is performed by internally rotating and adducting the maximum flexed hip. This results in contact between femoral neck and anterosuperior acetabulum.
There are some physical examination procedures that are superior to others in differentiating FAI from other pathologies of the hip and lombar spine. Anterior impigment test are the most spesific test for this disease. FADIR sensitivity is %94-98 specificity %10-25 Posterior İmpigment test sensitivity (FABER)% 42-81, specificity %25-75. In some lomber spine pathology (sacroiliac joint disease and L5-S1 facet joint degeneration) FABER test can be seen as positive.
The Radiology of FAI
Radiological evaluation of FAI anteroposterior pelvis radiography, cross-table lateral radiography to visualize the proximal femur and an alternative Dunn view (45° flexion) to visualize the femoral neck [3]. Plain films give the chance to evaluate morphological abnormalities of femoral neck and acetabulum, to identify the lesions of cartilage and the labrum and to exclude the possible differential diagnoses such as avascular necrosis, acetabular dysplasia and stress fracture. Abnormal morphology may give rise to bilateral FAI imaging in the plain radiographs, however, majority of patients experience unilateral symptoms [3].
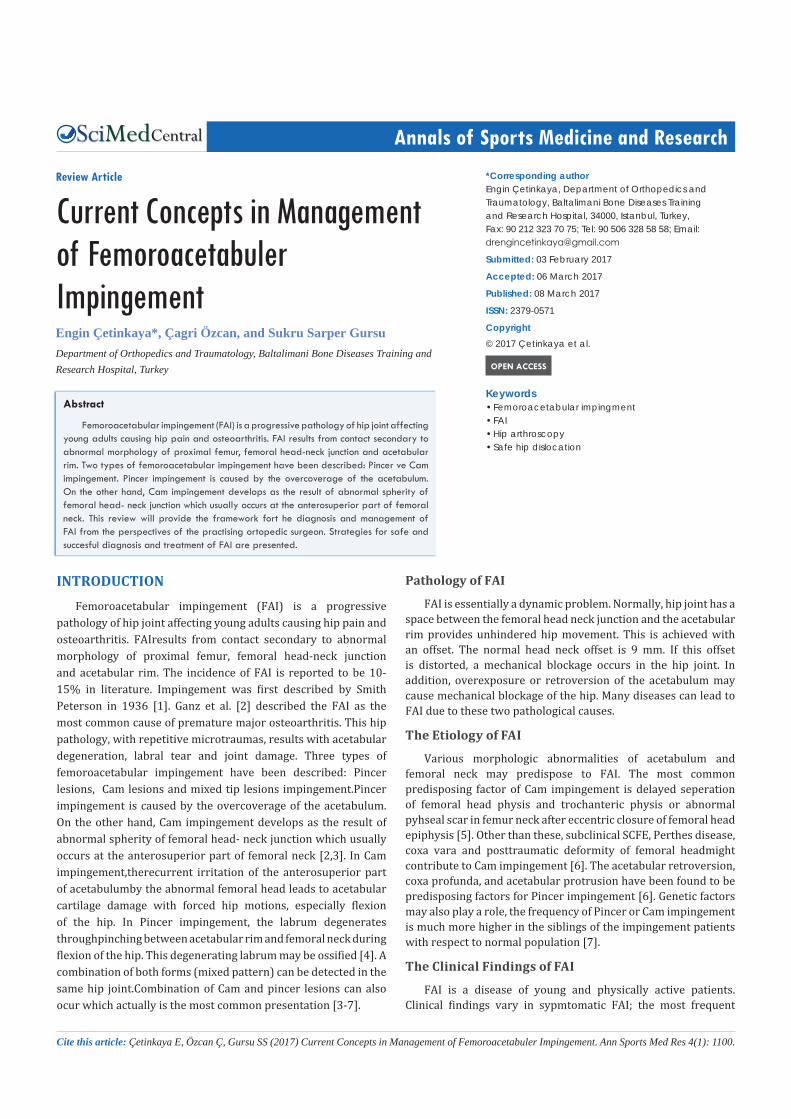
Acetabular overcoverage is measured by the lateral center edge (LCE) angle. . LCE angle is formed by a vertical line and a line connecting the femoral head center with the lateral edge of the acetabulum (Figure 1). The LCE angle makes the diagnosis of acetabular dysplasia and acetabular overcoverage if it is less than 25 degrees and above than 39 degrees, respectiveley. In Pincer impingement LCE angle is above normal [12,14]. The retroversion of Pincer type impingement can be diagnosedwith the ‘‘crossover sign’’ in anteroposterior plain radiography (Figure 1). The ‘‘crossover sign’’ is the result of misplacementof the anterior part of the acetabular margin more laterally with respect to the posterior part.Furthermore, the ischial prominences can be much more clearly defined on plain films. In coxa profunda and acetabular protrusion the surface of acetabular fossa extends beyond the medial of ilioischial line
and leads to the Cam impingement [14]. The alpha angle is used to measure the aspheric femoral head. It is between two lines from the centre of the femoral head through the middle of the femoral neck and through the point where the sphericity of the anterior femoral head is broken down to the center of femoral head (Figure 1) [11,15,16]. The normal level of alpha angle is 40°, it increases with Cam impingement, and with increasing degrees, the cartilage and labral damages also increase. The alpha angle is not related to the age.
The conventional radiography may reveal pistol grip deformity and synovial pitting in Cam impingement. (Figure 1). The pistol grip deformity is considered to be diagnostic [15].
Magnetic Resonance Imaging
MR arthrography is the gold standard method to evaluate the acetabular labrum and articular cartilage. The acetabular configuration, femoral neck contour and labral lesions can be well defined with the axial MRI sections. Femoral torsion can be assessed with CT or MRI images [12,14,17]. Femoral anteversion is much more pronounced in Pincer impingement with respect to Cam impingement.
The coronal MRI sections may reveal the alpha angle in Cam impingement. The anterosuperior labral tears are the most widely seen labral tears detected in Cam impingement. It can easily be diagnosed with MR arthrography.
The other MRI findings detected both in Cam and Pincer impingement are: paralabral cysts, subchondral edema, fibrocystic changes, labrum ossification, marginal osteophytes and subchondral sclerosis.
The Conservative Treatment of FAI
The conservative treatment options of FAI are limited. In addition, to our knowledge there is no high evidence-level study comparing conservative and surgical outcomes. The preservation of the muscle power, modification of activities and nonsteroidal antiinflammatory drugs are the treatment of choice [1]. The physiotheraphy concentrating on hip abductor and periarticular mucles should be conducted [18]. Increase in pelvic tilt results with postural deformities with advancing FAI. In advanced stages, the gait and posture should be analyzed, and the rehabilitation programme should be designed acorrdingly [18,19]. Although the rehabilitation programmes may help to preserve the functional level of the patient, it can not prevent the progression of the joint damage and the symptoms of FAI [2]. In the study conducted by Peter Wall et al. [13] analyzing 18 trials investigating conservative treatment of FAI, strengthening the hip musculature and the abdominal muscles has been proven to be effective in preservation of the patients’ functional activity and decrease the symptoms. These studies revealed that increase in passive range of motion could lead to labral tears and thus be harmful for the patient. The prevalence of FAI, which is asymptomatic in the community, is high.In the systematic rewiew of Frank et al.37% of patients had CAM deformities and 67% had pincer deformities with 2114 aseptomatic FAI patient. In the follow-up of 96 asymptomatic FAI hips monitored by Hartofilakidis et al.79 hips (82.3%) remained free of osteoarthritis for a mean of 18.5 years. In contrast, 17 hips (17.7%) developed osteoarthritis at a mean
Central
Çetinkaya et al. (2017)Email:
Ann Sports Med Res 4(1): 1100 (2017) 3/6
Figure 1 A: The image of impingement in the retroverted acetabulum, B: The radiographic image of Cam impingement (yellow arrow), C:Radiographic image of measured LCE Angle, D:Measurement of the alpha angle on axial section of MRI.
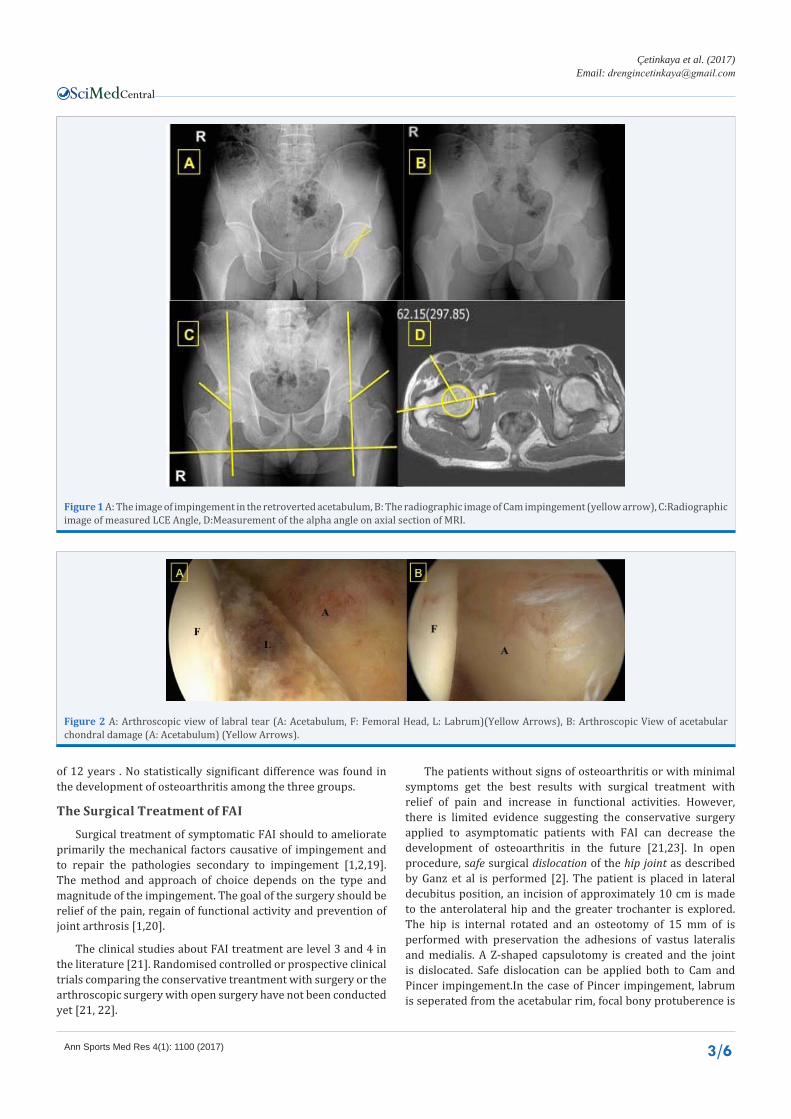
Figure 2 A: Arthroscopic view of labral tear (A: Acetabulum, F: Femoral Head, L: Labrum)(Yellow Arrows), B: Arthroscopic View of acetabular chondral damage (A: Acetabulum) (Yellow Arrows).
of 12 years . No statistically significant difference was found in the development of osteoarthritis among the three groups.
The Surgical Treatment of FAI
Surgical treatment of symptomatic FAI should to ameliorate primarily the mechanical factors causative of impingement and to repair the pathologies secondary to impingement [1,2,19]. The method and approach of choice depends on the type and magnitude of the impingement. The goal of the surgery should be relief of the pain, regain of functional activity and prevention of joint arthrosis [1,20].
The clinical studies about FAI treatment are level 3 and 4 in the literature [21]. Randomised controlled or prospective clinical trials comparing the conservative treantment with surgery or the arthroscopic surgery with open surgery have not been conducted yet [21, 22].
The patients without signs of osteoarthritis or with minimal symptoms get the best results with surgical treatment with relief of pain and increase in functional activities. However, there is limited evidence suggesting the conservative surgery applied to asymptomatic patients with FAI can decrease the development of osteoarthritis in the future [21,23]. In open procedure, safe surgical dislocation of the hip joint as described by Ganz et al is performed [2]. The patient is placed in lateral decubitus position, an incision of approximately 10 cm is made to the anterolateral hip and the greater trochanter is explored. The hip is internal rotated and an osteotomy of 15 mm of is performed with preservation the adhesions of vastus lateralis and medialis. A Z-shaped capsulotomy is created and the joint is dislocated. Safe dislocation can be applied both to Cam and Pincer impingement.In the case of Pincer impingement, labrum is seperated from the acetabular rim, focal bony protuberence is

Central
Çetinkaya et al. (2017)Email:
Ann Sports Med Res 4(1): 1100 (2017) 4/6
removed and then anchors with sutures are attached to secure the labrum. In Cam impingement, the extra bone is removed from the femoral head and it is washed out. It is crucial to not to leave any fragments in the joint. After the surgical procedure, the trochanter majus is fixed with two cannulated screws [24]. Naal et al. [25], demonstrated that of 22 athletes with the symptoms of FAI treated with open surgery and safe dislocation, 21 got back to normal healthy sport life (19 of them in the professional league, 2 of them in the amateur league).18 of these patients were satisfied with the surgical procedure. Kockara et al. [24], showed the increase in Harris Hip Score from preoperative 54.3 levels to 70.6 in 22 patients safe dislocation performed in a follow up period of 27.5 months. One of those patient needed total hip replacement because of avascular necrosis. This method carries the disadvantages of the need for a larger incision, the risk of nonunion and irritation of the implant.The open surgery did not eventuate promising results in the patients with Tönnis grade 3 or 4 [25-27]. Sampson et al. [26] reported that the surgery created worser results than expected in patients with chondromalasia grades greater than 3 when detected during surgery. McCarthy et al. [27], showed 3 of 4 patients with grade 3 needed hip joint arthroplasty in 2 years of open surgery.
The other surgical treatment optionof FAI is mini-open surgery, developed first by Ribas et al. [28]. Mini open surgery, while debridement of cam impingement is performed, also enables to explore the labrum and acetabular rim with arthroscopy. Ribas et al. [28] applied mini open surgery to treat the FAI in 35 hips of 32 patients. During the follow up period of 2.4 years, a statistical difference in internal rotation and flexion of the hip was found and an improvement of Merle d’Aubign clinical hip scores from 13.8 to 16.9 points in one year was achieved. Laude et al. [29], demonstrated the improvement of non arthritic hip scores (NAHS) from preoperative 54.8 to 83.9 points in 5 years follow up period of 94 patients treated with mini open surgery. Total hip replacement was performed to 11 of these patients, whereas 13 of them needed to undergo additional surgical procedures. Only isolated acetabulum decompression and labrum repair can be performed due to the risks of femoral osteochondroplasty in combined type FAI patients.The clinical outcomes of isolated acetabular decompression in patients with combined type FAI are similar to those in patients undergoing combined decompression techniques. However, there are few studies on this subject in the literature. Mini open surgery has played a role of bridge between open surgery and arthroscopy in the treatment of FAI [30]. This procedure has the advantages of usage of mini incision, no need of traction for arthroscopy, however, carries the disadvantages of longer and more difficult surgery and 10-15 percentage of total hip replacement ratio after surgery [19]. Furthermore, injury to the posterior branch of lateral femoral cutaneous nerve is reported to be 17.1% after mini open surgery [19,29]. Therefore, arthroscopic treatment is favored agaist mini open surgery today. Arthroscopic hip surgery is one of the most widely used techniques to correct FAI. In order to perform the arthroscopic hip surgery, the patient is placed in supine position on the traction table and hip joint is tracted to expand the joint space 15-20 mm. Since excessive traction may result with pudendal nerve neuropraxis, the genital region should be suspende with pads and sponges and excessive traction longer
than 2 hours should be avoided [31,32]. The portals should be placed when the leg is maximally internal rotated. Anterior, anterolateral and posterolateral portals are frequently used as described by Byrd et al. [33,34]. After surgerey is completed, the traction is relieved, the hip is internally rotated and flexed to 900. In the case of any signs of impingement, open debridement of the remnant in the femoral neck can be performed [34]. Postoperative physiorehabilitation may include tolerable weight bearing by the axillary crutches for the first 2 weeks. After 4-6 weeks forced hip flexion exercises(e.g. bicycling) can be started.
Arthroscopic FAI surgery enables to visualize the the central and peripheric chondral damage of the joint, to repair the labrum and treat both two types of impingement. The chondral damage on the joint surface can be observed and properly treated (Figure 2A, 2B) [35].
The studies that focused on hip arthroscopy for the treatment of FAI have been published since 2006. In the study conduvted by Philippon et al. [33] 112 patients who had undergone hip arthroscopy with a mean follow up period of 2.3 years, the mean Harris Hip Scores of patients improved from the preoperative 58 to postoperative 84.Total hip replacement was indicated in 10 patients in the postopreative period. They have shown the scores of patients adminestered labral repair were much more higher than those of labral excision applied [33]. Fabricant et al. [35] treated 21 athletes with FAI below 19 years of age with hip arthroscopy. The mean follow-up period was 1.5 yaers. They showed that the Harris Hip Scores improved significantly after operation with a mean of 21 points. The mean alpha angle decreased from 64+/- 16 to 40+/- 5 degrees [35].
The results of hip arthroscopy in the treatment of FAI depends largely on the experience of the surgeon, with increasing experience the results are promising. Büchler et al. [36] evaluated the patients operated for FAI between 2006-2010 years according to the years. In patients operated in first 2 years, there was no statistical difference between preoperative and postoperative alpha angles. However, the postoperative alpha angles of the patients operated in the third and fourth years decreased more significantly than those operated in first two years [36]. This study also demonstrated the alpha angles of patients to whom safe dislocation applied were statistically less than those treated with arthroscopy.
Hip arthroscopy is a difficult treatment method that requires experience. The minor risks and complications are; Traction –related injuries, Iatrogenic chondral and labrum damage, painful skar, instrument breakage, fluid extravasation. Majör risks and complications are; femur head avaskuler necrosis, femur neck fracture, infection Possibility of norovascular injuries when entering portals [37-41].
R. Seijas et al. Showed 14% [37]) total complications in 258 patients in the literature review. 3 patients show traumatic pudendal neuropathy and were resolved within 6 weeks, In 6 patients, Lateral femoral Cutaneous nerve ınjury due to portal entrance were observed.4 patients had improvement within 8 weeks and 2 patients had sequelae.In 2 patients had painful skar at the portal entrance and treated with scar excision under local anesthesia. 5 patients had instrumental breakage and were

Central
Çetinkaya et al. (2017)Email:
Ann Sports Med Res 4(1): 1100 (2017) 5/6
removed without any problems during operation. In 9 patients ilitibial band syndrome developed on the same side after a mean 6 weeks after surgery. Physical therapy was started for all patients and Z-plasties were applied to 3 patients who did not pass the pain. İn 4 patients developed heterotopic ossification but they were followed up for not having any complaints.Stress fracture occurred in one patient with a Cam Type lesion. Although fracture was non – displaced the patient was treated conservatively.One patient had debridement due to infection. Capsular adhesions developed in 3 patients. Arthroscopic capsularrelease was applied to this patient again.AVN developed in 1 patient. This patient was fully recovered after 6 months. The total number of patients remaining sequential was %0.7(2/258) [38-43].
CONCLUSIONThe arthroscopic treatment of FAI is more advantageous
compared to open surgery, due ton o need of osteotomy, no risk of nonunion, being less invasive and easier postoperative physiorehabilitation. Longer learning curves and neuropraxis after traction constitute the disadvantages [6,19]. The success rates of arthroscopic FAI treatmentincreases with the learning curve and give rise to promising results as much as safe dislocation. Still, we believe that further randomized controlled trials are required as studies proving that arthroscopic treatment is better than conservative methods are lacking.
REFERENCES1. Bedi A, Kelly BT. Femoroacetabular impingement. J Bone Joint Surg
Am. 2013; 95: 82-92.
2. Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003; 112-120.
3. Simon Dimmick, Kathryn J. Stevens, David Brazier, Suzanne E. Anderson, F Femoroacetabular impingement Radiol Clin N Am. 2013; 51:337- 352.
4. Leunig M, Robertson WJ, Ganz R. Femoroacetabular Impingement: Diagnosis and Management, Including Open Surgical Technique. Oper Tech Sports Med.2007; 15:178-188.
5. Sebastian A, Trousdale R. Femoroacetabular impingement: Avoiding arthroplasty Seminars in arthroplasty. Arthroplasty.2013; 24: 50-55.
6. De Sa D, Cargnelli S, Catapano M, Bedi A, Simunovic N, Burrow S. Femoroacetabular impingement in skeletally immature patients: a systematic review examining indications, outcomes, and complications of open and arthroscopic treatment. Arthroscopy. 2015; 31:373-384.
7. Pollard TC, Villar RN, Norton MR, Fern ED, Williams MR, Murray DW. Genetic influences in the aetiology of femoroacetabular impingement. J Bone Joint Surg Br. 2010: 209-216.
8. Parvizi J, Leunig M, Ganz R. Femoroacetabular impingement. J Am Acad Orthop Surg. 2007; 15: 561-70.
9. Parvizi J, Campfield A, Clohisy JC, Rothman RH, Mont MA. Management of arthritis of the hip in the young adult. J Bone Joint Surg Br. 2006; 88: 1279-1285.
10. Packer JD, Safran MR. The etiology of primary femoroacetabular impingement: genetics or acquired deformity. 2015; 10:10-27.
11. Boone GR, Pagnotto MR, Walker JA, Trousdale RT, Sierra RJ. Caution should be taken in performing surgical hip dislocation for the treatment of femoroacetabular impingement in patients over the age of 40. HSS J 2012; 8: 230-234.
12. Wall PD, Fernandez M, Griffin DR, Foster NE. Griffin, Nonoperative Treatment for Femoroacetabular Impingement: A Systematic Review of the Literature American Academy of Physical Medicine and Rehabilitation. PM R. 2013; 5: 418-426.
13. Nicholls RA. Intra-articular disorders of the hip in athletes. Physical Therapy in Sport. 2004; 5:17-26.
14. Wright AA, Naze GS, Kavchak AE, Paul D, Kenison B, Hegedus EJ. Naze, Alicia Emerson Kavchak Radiological variables associated with progression of femoroacetabular impingement of the hip: A systematic review. J Sci Med Sport. 2015; 18: 122-127.
15. Ersan O, Yıldız Y, Ateş Y. Femoroacetabular impingement TOTBID Dergisi. 2010; 9: 107-114.
16. Craig S. Mauro, James E. Voos, and Bryan T. Kelly Femoroacetabular Impingement Surgical Techniques. Oper Tech Orthop. 2010; 20: 223-230.
17. Miriam A. Bredella, Erika J. Ulbrich, David W. Stoller, Suzanne E. Anderson, Femoroacetabular Impingement Magn Reson Imaging. Clin N Am. 2013; 21: 45-64.
18. Bathala EA, Bancroft LW, Peterson JJ, Ortiguera CJ. Radiologic case study. Femoroacetabular impingement. Orthopedics. 2007; 30: 986: 1061-1064.
19. Matsuda DK, Carlisle JC, Arthurs SC, Wierks CH, Philippon MJ. Comparative systematic review of the open dislocation, mini-open, and arthroscopic surgeries for femoroacetabular impingement. Arthroscopy. 2011; 27: 252-269.
20. Bedi A, Dolan M, Leunig M, Kelly BT. Static and dynamic mechanical causes of hip pain. Arthroscopy. 2011; 27: 235-251.
21. Clohisy JC, St John LC, Schutz AL. Surgical treatment of femoroacetabular impingement: a systematic review of the literature. Clin Orthop Relat Res. 2010; 468: 555-564.
22. Matsuda DK, Gupta N, Hanami D Hip arthroscopy for challenging deformities: global pincer femoroacetabular impingement. Arthrosc Tech. 2014; 27:197-204.
23. Impellizzeri FM, Mannion AF, Naal FD, Hersche O, Leunig M. Naal The early outcome of surgical treatment for femoroacetabular impingement: success depends on how you measure it Osteoarthritis and Cartilage. 2012; 20: 638-645.
24. Koçkara N, Bursali A, Issin A, Gürsu SS, Yildirim T, Sahin V. Is open surgery effective in early-term in patients with femoroacetabular impingement syndrome Eklem Hastalik Cerrahisi. 2012; 23: 72-76.
25. Naal FD, Miozzari HH, Wyss TF, Nötzli HP. Surgical hip dislocation for the treatment of femoroacetabular impingement in high-level athletes. Am J Sports Med. 2011; 39: 544-550.
26. Sampson TG. Arthroscopic treatment of femoroacetabular impingement: a proposed technique with clinical experience. Instr Course Lect. 2006; 55: 337-346.
27. McCarthy JC, Noble PC, Schuck MR, Wright J, Lee J. The Otto E. Aufranc Award: The role of labral lesions to development of early degenerative hip disease. Clin Orthop Relat Res. 2001; 25-37.
28. Ribas M, Marin-Pena OR, Regenbrecht B, Torre BDL, Vilarrubias JM. Hip osteoplasty by an anterior minimally invasive approach for active patients with femoroacetabular impingement. Hip Int. 2007; 17: 91-98.
29. Laude F, Sariali E, Nogier A. Femoroacetabular impingement treatment using arthroscopy and anterior approach. Clin Orthop Relat Res. 2009; 467: 747-752.
30. Lincoln M, Johnston K, Muldoon M, Santore R. Combined arthroscopic and modified open approach for cam femoroacetabular impingement:

Central
Çetinkaya et al. (2017)Email:
Ann Sports Med Res 4(1): 1100 (2017) 6/6
Çetinkaya E, Özcan Ç, Gursu SS (2017) Current Concepts in Management of Femoroacetabuler Impingement. Ann Sports Med Res 4(1): 1100.
Cite this article
A preliminary experience. Arthroscopy. 2009; 25: 392-399.
31. Clarke MT, Arora A, Villar RN. Hip arthroscopy: complications in 1054 cases. Clin Orthop Relat Res. 2003; 84-88.
32. Ilizaliturri VM Jr, Orozco-Rodriguez L, Acosta-Rodríguez E, Camacho-Galindo J. Arthroscopic treatment of cam-type femoroacetabular impingement: Preliminary report at 2 years minimum follow-up. J Arthroplasty. 2008; 23: 226-234.
33. Philippon MJ, Briggs KK, Yen YM, Kuppersmith DA. Outcomes following hip arthroscopy for femoroacetabular impingement with associated chondrolabral dysfunction: Minimum two-year follow-up. J Bone Joint Surg Br 2009; 91:16-23.
34. Byrd JW, Jones KS. Arthroscopic femoroplasty in the management of cam-type femoroacetabular impingement. Clin Orthop Relat Res. 2009; 467: 739-746.
35. Fabricant PD, Heyworth BE, Kelly BT. Hip arthroscopy improves symptoms associated with FAI in selected adolescent athletes. Clin Orthop Relat Res. 2012; 470: 261-269.
36. Büchler L, Neumann M, Schwab JM, Iselin L, Tannast M, Beck M. Arthroscopic versus open cam resection in the treatment of femoroacetabular impingement. Arthroscopy. 2013; 29:653-660.
37. Byrd JW. Femoroacetabular impingement in athletes: current
concepts. Am J Sports Med. 2014; 42: 737-51.
38. Frank JM, Harris JD, Erickson BJ, Slikker W 3rd, Bush-Joseph CA, Salata MJ, et al. Prevalence of Femoroacetabular Impingement Imaging Findings in Asymptomatic Volunteers: A Systematic Review. Arthroscopy. 2015; 31: 1199-204.
39. Hartofilakidis G, Bardakos NV, Babis GC, Georgiades G. An examination of the association between different morphotypes of femoroacetabular impingement in asymptomatic subjects and the development of osteoarthritis of the hip. J Bone Joint Surg Br. 2011; 93: 580-586.
40. Reiman MP, Goode AP, Hegedus EJ, Cook CE, Wright AA. Diagnostic accuracy of clinical tests of the hip: a systematic review with meta-analysis. Br J Sports Med. 2013; 47: 893-902.
41. Papavasiliou AV, Bardakos NV. Complications of arthroscopic surgery of the hip. Bone Joint Res. 2012; 1: 131-44.
42. Tjong VK, Gombera MM, Kahlenberg CA, Patel RM, Brian Han B, Deshmane P. Isolated Acetabuloplasty and Labral Repair for Combined-Type Femoroacetabular Impingement: Are We Doing Too Much Arthroscopy. 2017.
43. Seijas O R, Ares A. SallentHip arthroscopy complications regarding surgery and early postoperative care: retrospective study and review of literature. Musculoskelet Surg. 2016: 1-6.
















![Marcin SZAREK, Gözde ÖZCAN [Biped Robot]](https://img.pdfslide.us/doc/110x75/577cc4671a28aba711992e3b/marcin-szarek-goezde-oezcan-biped-robot.jpg)












