Embed Size (px)
Citation preview

Current Approaches and New Directions in Treating Bone
Metastases from Breast Cancer
Erica L. Mayer MD MPH
Dana-Farber Cancer Institute
May 16, 2009

Outline
• Biology
• Symptoms/Imaging
• Treatment
• New Directions

Bone Metastases in Breast Cancer• Up to 70% of women with advanced breast
cancer may develop bone metastases– Early site of spread– 20% of women have “bone only” disease– More common if tumor is hormone receptor positive
• Cancer cells target bones with an extensive blood supply: arms, legs, ribs, spine, pelvis. Tend not to travel to hands and feet.
• Breast cancer growth in bone is typically slow; therefore optimizing treatment is crucial

Normal Bone BiologyBone is always in an active state of
remodeling (build up/break down)
• Resorption: stimulated osteoclasts erode bone, creating a cavity
• Reversal: bone surface is prepared for osteoblasts to begin forming bone
• Formation: osteoblasts replace resorbed bone and fill the cavity with new bone
• Resting: bone surface rests until a new remodeling cycle begins
Adapted from Novert's Pharmaceuticals

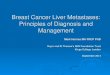
Bone Metastases: General Mechanism
Adapted from Guise and Mundy. Endocr Rev. 1998;19:18.
Primary cancerAngiogenesis Invasion Embolism
Multicell aggregates(lymphocytes, platelets)
Response tomicroenvironment
Tumor cellproliferation Bone
metastases
Extravasation Adherence Arrest in distantcapillary bed in bone
Tra
ns
po
rt

Osteolytic metastases
• Tumor cells produce growth factors that stimulate bone destruction• i.e. RANK ligand
• Osteoclasts are activated and break down bone
• Osteoblasts cannot build bone back fast enough
• Decreased bone density and strength; high risk for fracture
Patel, B. and DeGroot, H. Orthopedics Journal. 2001;24:612-7.

Osteoblastic Metastasis
• Osteoblasts are stimulated by tumors to lay down new bone
• Bone becomes abnormally dense and stiff
• Paradoxically bones are also at risk of breaking

Radiology: How to Evaluate
• Imaging tests– X-ray– Bone scan
• Sensitive, not specific. • False positives: trauma, arthritis,
infection– CT (“CAT” scan)– PET scan– MRI scan
• Bone biopsy – for confirmation
• Blood tests– Calcium, alkaline phosphatase
Bone Scan

MRI imaging
T1 T2

Symptoms/Complications Related to Bone Metastases
• Pain
• “Pathologic” fracture – broken bone after minimal trauma
• Bone marrow (“blood factory”) involvement -> low blood counts
• High calcium levels: confusion, drowsiness
• Nerve compression– Pain– Spinal cord compression
Goal is to use multidisciplinary management to reduce/eliminate all symptoms!

Treatment Options
• Goals:– Attack the cancer– Strengthen the bone– Reduce symptoms
• Includes:– Systemic therapy– Local therapy

Systemic Therapies
Anti-cancer therapy– Endocrine therapy
• Tamoxifen, aromatase inhibitors, ovarian suppression
– Chemotherapy• Many choices
– Biologic therapies• Herceptin, Tykerb, Avastin

Systemic Therapies
Pain control– Pain medication
• Tylenol, NSAIDs (ibuprofen), narcotics, steroids• Success can be limited by side effects
– Radiopharmaceuticals• Strontium-89 and samarium-153: radioactive
particles travel directly to tumor in bone• Can reduce pain refractory to other measures• Infrequently used

Systemic Therapies: Bisphosphonates
• Bind to and inhibit osteoclast action – Inhibit bone breakdown– Prevent bone damage– Improve bone density and strength
• Recommended for almost everyone with breast cancer bone metastases

Evidence Supporting Bisphosphonates in Breast Cancer
• Multiple clinical trials have demonstrated treatment with bisphosphonates can reduce:– Bone pain– Fractures– High calcium levels– Radiation therapy to bone– Surgery to bone
• May also significantly improve quality of life in women with breast cancer
Lipton. Clin Breast Cancer 2007

Oral Bisphosphonates: Clodronate
• Generally well tolerated
• Demonstrated benefits in clinical trials
• Issues for consideration– Not absorbed well from GI tract – may be less
effective than IV– Adherence to oral therapy a concern
• Not commercially available in US
Solomon et al. Arch Intern Med. 2005;165:2414.

IV Bisphosphonates
• More potent than oral bisphosphonates
• Improved adherence in clinic setting; given once every 4 weeks
• Side events– Flu-like symptoms– Injection-site reactions– Renal toxicity – need to check kidney function before giving– Long-term use
• Osteonecrosis of the jaw• Electrolyte abnormalities (low calcium)
Conte et al. Oncologist. 2004;9(suppl 4):28.

Theriault, R. L. et al. J Clin Oncol; 17:846 1999
Available IV bisphosphonates
Pamidronate (Aredia™) • In placebo-controlled trials
significantly reduced fracture, radiation, pain
Zoledronic Acid (Zometa™)• More potent agent; equally
effective in trials• Shorter infusion time (15
min vs 3 hours)

Newest Bisphosphonate: Ibandronate
• Both oral and IV forms
• Prevents bone events (fractures, radiation, surgery ) compared with placebo
• Can relieve bone pain when given with a loading dose (but takes up to 12 weeks)
• May have less kidney toxicity
• Ongoing comparisons to zoledronic acid are underway
Cameron et al, The Oncologist, 2006

Osteonecrosis of the jaw (ONJ)• What is ONJ?
– Exposed jawbone that does not heal
– Treated with surgery, antibiotics– Rare side effect: about 5% in
breast cancer population
• Who could get ONJ?– Risk related to cumulative
exposure – Recent invasive dental procedure
or poor oral health are risk factors• Tooth extraction
• Dental implant

ONJ Prevention
• Potential benefits of bisphosphonates typically outweigh small risks of ONJ
• How to prevent:– See dentist before beginning
bisphosphonate– Pursue optimal preventative dental care– Practice good oral hygiene
• In those with stable disease after prolonged therapy, can consider reducing frequency of treatment

New Systemic Therapy: Denosumab
• Denosumab: antibody against RANK ligand, the stimulator for osteoclasts
• Once-a-month subcutaneous injection
• Promising results as osteoporosis treatment in clinical trials
• Emerging role in the treatment of bone metastases
Ellis SABCS 2007; Lipton ASCO breast 2008; McClung et al, NEJM 2006

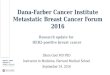
Blocking RANK ligand in a mouse can fill in a mouse bone metastases
OPG
Control Treated
Morony et al. Cancer Res. 2001;61:4432.

Ellis, G. K. et al. J Clin Oncol; 26:4875-4882 2008
Denosumab prevents osteoporosis in women receiving aromatase inhibitors
• 250 patients receiving placebo or denosumab• Results: increased bone density with
denosumab• Side effects: joint pain, body ache, fatigue

Denosumab vs Zoledronic Acid
• Phase 2 trial of first-line denosumab vs zoledronic acid– 255 women enrolled– Equivalent reduction in bone breakdown– Equivalent prevention of bone events (fracture, radiation,
surgery)
• Phase 3 trials underway comparing denosumab and zoledronic acid head to head
Lipton et al, CCR 2008

Denosumab after Zoledronic Acid
• Phase 2 trial of denosumab vs zoledronic acid after prior bisphosphonate therapy
• 111 patients enrolled with bone breakdown despite zoledronic acid
– Denosumab reduced markers of bone breakdown
– Less fracture, radiation, surgery in those receiving denosumab
Fizazi, JCO 2009
A future role may exist for denosumab for bisphosphonate-refractory disease

Systemic Agents in Development
• Cathepsin K inhibitors– Cathepsin K degrades the bone– An oral inhibitor reduced bone turnover from breast
cancer bone metastases (ASCO 2009 poster)
• SRC kinase inhibitors (dasatinib)– SRC necessary for osteoclast bone breakdown– Dasatinib is oral, approved for chronic leukemia, may
have activity against breast cancer as well
• Ongoing trials are using these drugs after, with, or instead of zoledronic acid

Local Therapies• Local therapies treat a limited number of
locations; do not treat the whole body
• Types:– Radiotherapy– Interventional Radiology– Surgery
• Goals:– Relieve pain– Prevent fracture– Enhance mobility and function– Preserve quality of life

Radiation Therapy
• Radiation therapy can be used to treat painful bone metastases refractory to systemic therapies
– 80-90% of breast cancer patients experience relief of symptoms
– 40-46% experience full relief
– 70% never have pain in that region again
– May take months before full pain relief is realizedTong et al, Cancer 1982

Radiation Therapy: Specifics
• Can take 1-4 weeks; 2 weeks is most common
• Chemotherapy is usually on hold during RT
• Side effects: nausea, diarrhea, low blood counts, fatigue
• Typically radiation is not used again in the same place

Interventional Radiology
• What is it?– Minimally invasive procedures performed by
specialized radiologists to treat symptoms from bone metastases
• Indications:– To treat bone pain refractory to other
conservative pain control measures– Specialized technique for metastatic cancer to
spine bones• Stabilize broken bone

Interventional Radiology: Techniques
• Vertebroplasty: – Injection of bone cement to
support weakened bones – Provides immediate and
substantial pain relief
• Kyphoplasty: – Balloon inflation of
compressed spine bone is performed before cement injection
– Used for compression fractures

Positioning in Interventional Radiology

Example: Vertebroplasty

Example: Vertebroplasty

Concept of kyphoplasty

Concept of kyphoplasty

Other Local Techniques• Radiofrequency Ablation (RFA) and
cryoablation– Minimally invasive procedures to “burn”
or “freeze” a tumor– Desensitizes by killing nerve endings
near the metastasis
• Most commonly used for cancer in the spine
• Techniques can achieve excellent pain control
• Use may expand with further data

Surgical Joint Stabilization
• Indications for surgery for bone metastases:
– Prevention of bone fracture (“prophylactic”)• Risk depends on location of metastasis, type, size, and
presence of symptoms
– Alleviation of pain
– Maintain ability to walk (for hip metastases)
– Stabilize broken bone after pathologic fracture
Beals et al, Cancer 1971

Surgical Joint Stabilization
• Benefits of surgery– Procedures designed for rapid recovery
• Simple pin placement to full hip replacement
– Most are walking again soon after hip surgery– Most have good to excellent pain relief– Can dramatically improve healing after fracture
• Typically performed in combination with radiotherapy
Ryan et al. J Bone Joint Surg Am, 1976

Future Directions
• Can we prevent bone or other metastases by using bone medicines earlier on?
• Increasing evidence suggests bisphosphonates may have anti-cancer activity

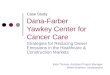
ABCSG 12ABCSG 12
Ovarian suppression +
tamoxifen
Ovarian suppression +
anastrozole
Zoledronic Acid (Zometa) 4 mg IV, Every 6 Months for 3 years
No Rx
All patients premenopausal, HR+
No adjuvant chemo
Stage I-II breast cancer- 30% with T2 tumors- 25% with positive nodes
N = 1803

At 5 years, 36% reduction in risk of recurrence in those taking Zometa



Conclusions• Bone metastases are common in advanced breast cancer,
and can cause significant symptoms
• Multiple systemic and local therapies are available; standard therapy includes monthly zoledronic acid
• Better understanding of toxicities can improve the safety of treatment
• New agents take advantage of increased understanding of the biology of bone turnover
• Women with advanced breast cancer may live with bone metastases for many years, therefore optimizing therapy is crucial