Embed Size (px)
Citation preview

A.C.TAccelerating
Change Today
F O R A M E R I C A ’ S H E A L T H
M A Y 2 0 0 2
T H E N A T I O N A L C O A L I T I O N O N H E A L T H C A R ET H E I N S T I T U T E F O R H E A L T H C A R E I M P R O V E M E N T
Stories of Change inChronic Illness Care
Curing the System

THE NATIONAL COALITION ON HEALTH CARE
NCHC is the nation’s most broadly representative alliance working to improve America’shealth and health care. It is comprised of 80 member organizations. They include someof the nation’s largest businesses, labor unions, health care providers, consumers groupsreligious organizations, foundations, and health and pension funds. The Coalition wasfounded in 1990. It is non-profit and non-partisan. Its members are united in the beliefthat America needs better, more affordable health care and that all Americans shouldhave health insurance. Former Presidents George Bush, Jimmy Carter, and Gerald R. Fordserve as the Coalition’s Honorary Co-Chairs. Former Iowa Governor Robert D. Ray andformer Congressman Paul G. Rogers of Florida are the Coalition’s Co-Chairmen. NCHCis in Washington, DC. Founder and President Henry E. Simmons, M.D., M.P.H., F.A.C.P.,is a widely respected pioneer in the field of health quality assessment and improvement.
THE INSTITUTE FOR HEALTHCARE IMPROVEMENT
IHI is an independent, non-profit education and research organization based in Boston,MA. It was founded in 1991 with the goal of fostering collaboration among health careorganizations to improve the quality of health care. IHI each year holds a wide arrayof educational forums, symposia and workshops, and demonstration projects for med-ical professionals and health care administrators. IHI’s co-founder and president, DonaldM. Berwick, M.D., M.P.P., a practicing pediatrician and clinical professor at HarvardMedical School, is one of the nation’s leading authorities on health care quality.
Accelerating Change Today (A.C.T.)F O R A M E R I C A ’ S H E A L T H
A.C.T. is a collaborative initiative of the National Coalition on
Health Care and the Institute for Healthcare Improvement. It
aims to improve the quality of health care in the United States
through the identification of “best practices” and administrative
and clinical innovations that are: (1) yielding better patient out-
comes; (2) making the delivery of care more efficient; (3) increas-
ing access to timely medical care; (4) making the health system
easier to use; (5) lowering costs, and (6) reducing medical errors
and inappropriate care. The initiative seeks to accelerate the
spread of best practices and innovations throughout the health
system by publishing them and through presentations at medical
meetings and health care and business symposia. A central pur-
pose is to make a broad range of health care stakeholders,
including consumers and those who pay the health care bill,
more aware of cutting-edge efforts to improve the quality of
health care. The initiative will actively encourage the replication
of best practices in health care facilities.
About This Publication
This report presents the stories of
individuals, institutions, and organi-
zations that made a commitment to
change and innovation to improve
chronic illness care. The profiles
reflect some of the most promising
pioneering efforts underway in this
field. The team of experts identified
in the Credits and Acknowledge-
ments developed selection criteria
and determined those to be profiled.
Their final choices represent the
larger group of meaningful and
laudable efforts underway nation-
wide to improve chronic disease
management.

Profiles of individuals,
institutions, and
organizations that
have demonstrated
excellence in chronic
disease care
A.C.TAccelerating
Change Today
F O R A M E R I C A ’ S H E A L T H
M A Y 2 0 0 2
Curing the System
T H E N A T I O N A L C O A L I T I O N O N H E A L T H C A R E
T H E I N S T I T U T E F O R H E A L T H C A R E I M P R O V E M E N T

Credits and AcknowledgementsTeam Co-Leader
EDWARD H. WAGNER, M.D. , M.P.H. , F.A .C .P.Dr. Wagner is a general internist/epidemiologist and Director of the W.A. MacColl Institutefor Healthcare Innovation at the Center for Health Studies (CHS), Group Health Cooperativeof Puget Sound. He is also Professor of Health Services at the University of Washington Schoolof Public Health and Community Medicine. He directs “Improving Chronic Illness Care” (ICIC),a national program of The Robert Wood Johnson Foundation. The overall goal of ICIC is toassist health systems improve their care of chronic illness through quality improvement andevaluation, research, and dissemination. More than 500 American and international healthcare organizations have been involved in ICIC-guided quality improvement programs.
Team Co-Leader
CONNIE DAVIS , M.N. , A .R .N.P.Connie Davis is a geriatric nurse practitioner at the Center for Health Studies, Group HealthCooperative of Puget Sound and the Associate Director for Clinical Improvement of“Improving Chronic Illness Care.” She is a member of the clinical faculty of the University ofWashington. She is the author or co-author of numerous publications on health promotionand chronic illness care and a frequent speaker regarding improving chronic illness care.
Team Member
CHARLES J . HOMER, M.D. , M.P.H.Dr. Homer is Executive Director of the National Initiative for Children’s Healthcare Quality,an education and research organization dedicated to improvement of the quality of children’shealth care. He is an associate professor of pediatrics and of public health at HarvardUniversity and is a member of the third U.S. Preventive Services Task Force. He currentlyserves as chair of the American Academy of Pediatrics Steering Committee on QualityImprovement and Management and is also principal investigator of several federally fundedstudies of quality improvement in child health.
Team Member
STEVEN D. HAGEDORN, M.D.Dr. Hagedorn, assistant professor of Family Medicine, is a member of the Mayo ClinicRochester Family Medicine staff. For 12 years he has been involved in numerous activitiesrelated to disease management and clinical quality improvement. From 1997 to 2001, heserved as Vice Chair of the Mayo Clinic Rochester Continuous Improvement Council and iscurrently its Acting Chair. He is studying complexity theory and its implications for healthcare through a doctorate program on organizational change at the Center for Complexity andManagement at the University of Hertfordshire, U.K.
Team Member
BRIAN AUSTINBrian Austin is Deputy Director of “Improving Chronic Illness Care,” with responsibility foroverall administrative leadership of the program. He is active in all aspects of ICIC, with aspecial interest in incorporating new technologies into the primary care setting and the devel-opment of expert systems and improved practice team communication methods to enhancecare delivery.
Writer
ABBI KAPLANAbbi Kaplan conducted the interviews and wrote this publication. An award-winning writer,Kaplan specializes in health care. She has authored numerous articles and publications on awide range of health care issues and has served as a spokesperson, consultant, and mediatrainer to leaders of regional, national, and international organizations. She is Of Counsel toPyramid Communications, a Seattle-based public affairs firm serving clients from the non-profit, advocacy, and philanthropic communities.
EDITORPatricia Q. Schoeni
ASSISTANT EDITORWhitney Lindahl
DESIGNPensaré Design Group, LTD
Support for the preparation andproduction of this report has beenprovided by the Robert WoodJohnson Foundation.
© 2002 by the National Coalitionon Health Care and the Institutefor Healthcare Improvement

Table of Contents
The Changing Face of Chronic Disease Careby Edward H. Wagner, M.D., M.P.H., F.A.C.P. 2
It’s a Team Sport: Delivering Unified Chronic Illness Care in Rural CommunitiesCareSouth Carolina, High Plains Community Health Center 6
Engaging the Patients: Private Practice Re-defined The Polyclinic, Natalie Roberts, D.O. 11
Rivaling Private Care: Community Health Centers Meet the Needs of the Urban PoorHill Health Center, Clinica Campesina 15
Full Court Press: An Integrated System Tackles Chronic Illness CarePremier Health Partners 20
Connecting the Dots: Health Plans’ Pivotal Role in Chronic Illness ImprovementUnivera Health Care, HealthPartners Medical Group, Rocky Mountain HMO 23
Primary Care in the Driver’s Seat: Re-configured Relationships in an Academic SettingVanderbilt Medical Center 28
Reversing the Trend: Chronically Ill Seniors’ Health Improves in Community ProgramSenior Wellness Project, Senior Services of Seattle/King County 32
Resources and Suggested Reading35
1

CHRONICDISEASE CARE
The Changing Face of
BY EDWARD H. WAGNER, M.D. , M.P.H . , F.A .C .P.
CHRONICDISEASE CARE
D I A B E T E S , C H I L D H O O D A S T H M A ,
D E P R E S S I O N , H Y P E R T E N S I O N , H E A R T
D I S E A S E , R H E U M A T O I D A R T H R I T I S
Some of these chronic illnesses affectadults, others children; some reduce lifeexpectancy, while others mostly causediscomfort. Yet, they have many com-monalities. These illnesses last for years,often for life; and cause major mor-bidity and mortality. Patients and theirfamilies play the central role in their suc-cessful management by appropriatelymonitoring their health, using medicalcare, adhering to treatment, regulatinglifestyle behaviors, and dealing effective-ly with the emotional and social stressesassociated with being chronically ill. All
these diseases are becoming increasinglyprevalent because the rapid aging of thepopulation increases the pool of suscep-tible older adults, advances in treatmentprolong life, and changes in the environ-ment increase risk.
Primary care practice, which used toinclude heavy doses of minor illnessesand the care of healthy younger people, isnow often dominated by care of chroni-cally ill older adults.
The good news is that care of mostmajor chronic illnesses has become sub-stantially more effective through recentprogress in clinical and behavioral treat-ments. When properly applied to well-informed patients, newer treatments canlead to major reductions in suffering andavoid complications, including death.
But the bad news is that studies showthat only a minority of people with theseconditions is receiving appropriate treat-ment. Especially lacking is support forpatients’ efforts to manage their ownhealth. These deficiencies in the quality ofchronic illness care have been found in all
types of medical settings—prepaid or fee-for-service, managed care and privatepractice, academic and community. Therecent Institute of Medicine (IOM) report,“Crossing the Quality Chasm,” highlight-ed this discrepancy (the “chasm”) betweenthe medical care made possible byadvances in clinical and behavioral ther-apies and the care received by the major-ity of Americans. The report recommend-ed that chronic illnesses, because of theirhuman and financial costs, are the placeto start working on improving the qualityof care. Until recently, deficiencies inquality of care were attributed to the failings of doctors and other health careproviders. The IOM report shifts the focusfrom the caregivers to the systems inwhich they work: “Current care systemscannot do the job. Trying harder will notwork. Changing systems of care will.”
What’s wrong with our current medicalcare system; isn’t it the finest in the world?
2

Simply put, the design of medicaloffice practice has not kept up with thechanging face of medical practice. Itstill relies heavily on the private officevisit, physician memory, written medicalrecords, and inadequate patient involve-ment, despite growing evidence of betterways of interacting with patients, assur-ing the application of appropriate treat-ments, and managing patient informa-tion. It is a “system” that developed inresponse to the then prevailing burden ofacute infectious diseases and injuries. Inpart because they are practicing in out-moded work settings, most clinicians areworking harder and harder, struggling tomeet the needs of an older and sickerpopulation. But can hardworking clini-cians and administrators redesign theircare system while still meeting the day-to-day needs of their patients?
Health care organizations around thecountry, large and small, are doing just that.
This report chronicles the experiencesof 12 very different organizations thathave redesigned systems so as to providebetter care to patients with diabetes, asth-ma, heart failure, depression, and otherchronic illnesses. Although the specificchanges made have varied, all of theorganizations used a similar recipe withthree major ingredients:
1. A clear definition of optimal care
2. A roadmap for changing the system
3. An effective improvement strategy.
INGREDIENT 1
A Clear Definitionof Optimal CareFirst, the organization determines thespecific clinical and behavioral interven-tions that characterize optimal care. Theseare the tests, medications, and behavioralmodifications proven by rigorous scien-tific evidence to improve the health andsatisfaction of patients. Prescribing theright tests and medications is only halfof the battle. Patients must also be ableto manage their health and treatments
and the thousands of decisions that con-front them with skill and confidence. Thedevelopment of self-management skillsand confidence can be assisted by sup-portive interventions
INGREDIENT 2
A Roadmap forChanging the SystemFor decades innovative clinicians andresearchers have been testing new waysto care for people with chronic condi-tions, and this experimentation has paidoff. We now have strong evidence thatan integrated set of system changes cansubstantially increase the likelihood thatoptimal care will be rendered and patienthealth and satisfaction improved.
Our Robert Wood Johnson Foundationnational program, Improving ChronicIllness Care (ICIC), tries to assist busyhealth systems to make these systemchanges through quality improvementinitiatives, dissemination, and by sup-porting relevant research.
The Chronic Care ModelProvides the RoadmapWe at ICIC have tried to summarize whatwe know about improving chronic illnesscare through system change in a singleframework—the Chronic Care Model. It isnot a quick fix or magic bullet; it is amulti-dimensional solution to a complexproblem. The Model distills the myriadimprovement activities that have shownsuccess into six interrelated elements.
THE CHALLENGESystem change must begin at the top.
THE SOLUTIONA supportive health careorganization.Given the challenges of packed
appointment schedules and tighter bud-gets, changes at the level of practice areunlikely to happen unless it is a priorityfor the organization and its leaders.Strong senior leadership plays an instru-mental role in providing motivation,securing resources, and removing thebarriers that may stall quality improve-ment activities.
THE CHALLENGERelying on the physician and 15-minute,acute care visits initiated by patientswith problems doesn’t lend itself toeffective chronic disease management.
THE SOLUTIONDelivery system design.Central to assuring high qualitychronic illness care are planned
visits and active follow-up. Planned visits(or other forms of interaction) use rele-vant patient information, evidence-basedguidelines, and organized approaches toassure that all patients receive recom-mended services. Such visits can be indi-vidual or in groups, and include attentionto self-management and preventive inter-ventions as well as acute problems. Highquality chronic illness care also entailsclose follow-up of the patient’s condition
3
T H E C H R O N I C
C A R E M O D E L
I S N O T A
Q U I C K F I X O R
A M A G I C B U L L E T ;
I T I S A M U L T I -
D I M E N S I O N A L
S O L U T I O N T O
A C O M P L E X
P R O B L E M .

4
and treatments. This can be done by tele-phone or e-mail as well as in person.Planned visits and close follow-up areteam sports, requiring planning and thecoordinated actions of multiple caregivers.Many of the critical tasks do not requireclinical training and could be most effi-ciently and consistently performed bynon-professional team members.
THE CHALLENGEThe practice team must have the in-formation needed to make appropriateclinical decisions at the time thosedecisions are made.
THE SOLUTIONDecision support.Data indicate that guidelinesbecome effective provider be-
havior change agents only when they arewoven into the fabric of patient carethrough effective professional education,reminders, and ongoing feedback andreinforcement. Incorporating guidelinesinto a registry, flow sheets, and patientassessment tools, coupled with education-al support from clinical opinion leaderssuch as medical specialists, increaseguideline adherence.
THE CHALLENGETimely access to critical clinical in-formation about individual patientsor their population of chronically illpatients makes it possible to deliverhigh quality chronic illness care.
THE SOLUTIONClinical information system.A registry or database of keyinformation on all patients with
a chronic condition is the glue that holdsan effective chronic care system togeth-er. Registries facilitate monitoring andplanning care for individual patients andfor the practice as a whole. An effectiveregistry reminds caregivers of neededservices and can generate materials forproviders and patients that support plan-
ned visits. To enhance the care for thepractice as a whole, an effective registryprovides feedback on performance andcan identify which patients are in partic-ular need of attention.
THE CHALLENGEPatients need to “own” their healthconditions and have the skills andconfidence to make the decisions andchanges that lead to better outcomes.
THE SOLUTIONSelf-management support.There is now considerable evi-dence that individual and group
interventions that promote patient em-powerment and the acquisition of self-management skills are effective in dia-betes, asthma, and other chronic condi-tions. They emphasize the crucial rolethat patients play in setting goals, estab-lishing action plans, identifying barriersto effective self-management, and prob-lem-solving to overcome the barriers. Theintegration of collaborative goal-setting,action planning, and problem-solvinginto routine care is a priority. The inclu-sion of self-management goals in a dis-ease registry has helped many organiza-tions maintain ongoing attention to self-management.
THE CHALLENGEMany practices simply cannot provideall of the services and supports thatpatients and families need for optimalchronic illness care.
THE SOLUTIONCommunity resources.With all that there is for clini-cian and patient alike to do,
there certainly is no reason to go it alone.Organizations large and small, in urbanand rural areas, in solo practices andintegrated health systems have foundthat community resources supplementand support their efforts to improve thecare of patients with chronic illnesses.
Chronically ill patients can benefit from avariety of services and resources that arenot available from their health careprovider—such as educational offerings,peer support groups, and exercise pro-grams. Many of these may be available intheir communities. Increasing access toeffective community resources throughlinkages with relevant organizations andagencies is a cost-effective way to opti-mize care, and, for small practices, maybe the only way.
INGREDIENT 3
An EffectiveImprovement StrategyIngredients 1 and 2 in the chronic careimprovement process provide the clinicaland system change ideas required toassure optimal care, but the ideas are ex-pressed generally to encourage flexibilityand local creativity in their implemen-tation. The 12 case studies in this reportillustrate the manifold ways in which theelements of the Chronic Care Model canbe put into practice. Thus, the third in-gredient in chronic disease improvementis to use an improvement strategy thatenables motivated organizations to “rein-vent” these ideas for effective clinicalmanagement and system change by tai-loring and testing them in their practice.Growing experience suggests that focus-ing on clear goals for improvement,designing measures to track the accom-plishment of the goals, and using briefpilot tests of change bring greater qualityimprovements than older models thatemphasize analysis and planning.

O R G A N I Z A T I O N O F H E A L T H C A R E
A health system’s business plan reflects its commitment to apply the Chronic Care Model
across the organization. Clinician leaders are visible, dedicated members of the team.
D E L I V E R Y S Y S T E M D E S I G N
Regular, proactive planned visits which incorporate patient goals help individuals main-
tain optimal health and allow health systems to better manage their time and resources.
The visits often utilize the skills of more than one member of the care team.
D E C I S I O N S U P P O R T
Clinicians have convenient access to the latest evidence-based guidelines for care for
each chronic condition. Continual educational outreach to clinicians reinforces utiliza-
tion of these standards.
C L I N I C A L I N F O R M A T I O N S Y S T E M S
Health systems harness technology to provide clinicians with a comprehensive list of
each of their patients with a given chronic disease. This list, also known as a patient reg-
istry, provides clinicians with the information they need to track their patients’ health
status and minimize complications.
P A T I E N T S E L F - M A N A G E M E N T
Patients are encouraged to set goals, identify barriers and challenges, and monitor their
own conditions. A variety of tools and resources provide patients with visual reminders
to manage their health.
C O M M U N I T Y R E S O U R C E S
Community resources, from schools to government, non-profits and faith-based organi-
zations, bolster health systems’ efforts to keep chronically ill patients supported,
involved and active.
THE CHRONIC CAREMODEL
5
The Institute for Healthcare Improve-ment has given life to this qualityimprovement strategy by using it in thecontext of a collaborative learning expe-rience called a Breakthrough Series. ABreakthrough Series brings together mul-tiple health care organizations to worktogether for 12–13 months with faculty toimprove care. Chronic Conditions Break-through Series work on care for one ormore chronic illnesses using the ChronicCare Model as the source of systemchange ideas. Several hundred health careorganizations have now used these threeingredients to improve chronic illnesscare in collaborative quality improve-ment programs.
The case studies that follow in thisreport largely document the experience ofa diverse group of health care organiza-tions that have participated in either aChronic Conditions Breakthrough Seriesor a similarly designed regional collabo-rative. Some had developed promisingprograms that were refined and improvedfurther by their involvement in a collab-orative. But most began only with avision of better care for their patients,reduced costs, and a more rewardingpractice for their beleaguered clinicians.All were guided by the Chronic CareModel and made changes in most of thesix elements. But several organizationsgave emphasis to one or two changes ofparticular relevance in their context—e.g., specialist support of primary care(Decision Support); planned group visits(Delivery System Design); electronicmonitoring of self-management goals(Clinical Information Systems). While the12 organizations featured are exceptional,their system changes and results are notatypical of the several hundred medicalorganizations (two-thirds of all partici-pating organizations in chronic illnesscollaboratives) that have demonstratedmeasurable improvements in the qualityof their care.
Edward H. Wagner, M.D., M.P.H., F.A.C.P.
Director, Improving Chronic Illness Care, NationalProgram, Robert Wood Johnson Foundation

If you don’t expect to find state-of-the-art chronic disease care in a rural com-munity health care setting, you’d be sur-prised if you visited any of the clinics ofHigh Plains Community Health Center inColorado or CareSouth Carolina.
Both community centers have enjoyedgreat success from adoption of theChronic Care Model, developed byImproving Chronic Illness Care, a nation-al program of the Robert Wood JohnsonFoundation.
CareSouth CarolinaCareSouth Carolina is a communityhealth center, operating four centers infour different rural communities in thePee Dee Region of South Carolina.CareSouth Carolina uses the Chronic CareModel to manage care for diabetes,depression, and asthma and plans to addcardiovascular disease and hypertension.
Ann Lewis, CareSouth Carolina’sExecutive Director, says clinicians are
6
It’s a
“Robbie had acted like he had been cornered for awhile. It started when he was in Junior High when he had a tough time
with bullies at school. One time, he became so frustrated, he put his fist through a wall. I began to think: ‘this child has
rage.’ It was right after Columbine and I tried to talk to the school about it, but they were no help at all.”
Janet Webster and her son Robbie, 16-years-old, were struggling with his mood disorder and didn’t know where to go
for help. “One day, we were taking a trip to the dentist to have his wisdom teeth pulled, and he went to pieces in the car.
I had to pull over. He was having so much anxiety over the surgery. We talked, and that was the point when I decided that
we really needed to do something about it,” she related. But fearing the stigma associated with mental health care, Janet
wasn’t sure on the best course. Then she took Robbie to CareSouth Carolina.
“Right off, the CareSouth Carolina counselor recognized Robbie was having a problem and identified exactly what it
was. The treatment has made a world of difference. Before we started participating in this, it was like my son saw every-
thing through a gray veil. Now, it’s like he sees things through a sunlit window. He’s just a few degrees happier and that
has made a big difference. He feels like he’s in control again. I’ve recommended this (program) to other people who are
having problems because it has made such a big difference in our lives,” Janet concluded.
CareSouth CarolinaPEE DEE REGION
SOUTH CAROLINA
High Plains CommunityHealth Center
COLORADO
DEL IVER ING UN IF I ED CHRONIC I L LNESS CARE
IN RURAL COMMUNIT I ES
TeamSport
•ORGANIZATIONOF HEALTH CARE
•DELIVERYSYSTEMDESIGN
•DECISIONSUPPORT
•CLINICAL INFORMATIONSYSTEMS
•PATIENTSELF-MANAGEMENT
•COMMUNITYRESOURCES

almost always surprised when they startworking to improve chronic conditions.“They usually think that they’re doing thebest they can. All of a sudden, they real-ize that the current level of thinking ismuch more advanced or has left thembehind a little bit. That’s not anythingagainst the clinicians. They’re in busyambulatory practices, and chronic caremanagement is usually last on the list forstaying on top of everything,” she added.
The second big surprise, according toLewis, is the difference between patienteducation and patient self-management.The former gives the patient informa-tion, the latter gets the patient involved.“A lot of what’s happened in health careis we think we know what’s best for thepatient. Wrong. We only know what ishappening in the office at that setting.They know what they’re doing 24 hoursa day. When they become engaged inthat process, they no longer have theexcuse not to improve their health,”Lewis said.
Whether for diabetes, depression, orasthma, CareSouth Carolina found eachof the Chronic Care Model’s six elements
provided critical success factors. Takentogether, their impact grew exponentially.
The Case for Data or How Will WeKnow When We Get There?
It would be a lot easier not tohave to deal with data, but asLewis pointed out, though
developing a patient registry and trackingoutcomes can be hard work, it pays off.“It’s the single most important thing youcan do. With data outcomes, you knowright away what’s working, and it keepsyou in intimate contact with yourpatients. You begin doing things proac-tively with your patients instead of reac-tively. You’re planning their care withthem ahead of time. You just can’t do thatif you don’t know that you have plannedcare visits,” she said.
Recognizing the importance of data,CareSouth Carolina decided to organizetheir disease management by investing inan electronic database that works off theelectronic medical records. That way,Lewis believes they’ll be most effective atincorporating additional conditions andmanaging all the patients’ needs.
Why Patient Education Isn’tEnough for Chronic Disease
Chances are, if you break abone, get hit by a car, or needsurgery, you’re going to fol-
low the doctor’s orders. But if you havebeen living with a chronic disease forawhile, you’ve had to adapt to the lim-itations it places on your life, and yousoldier on. As Lewis sees it, that’s oneof the big reasons why patient self-management plays such an importantrole in improving health for patientswith chronic disease.
“Our health care model has been oneof dictation. ‘Do this. Take this. Don’tdo that.’ That approach doesn’t work
7
• “Our depression outcomes were one of our biggest successes. In
national data for depression, follow up beyond eight to 12 weeks is
about 25% of the cases. In our program, 72% of our patients were in
follow up after six months.”
• “Of the clients receiving treatment, more than 73% reported a
decrease in depression symptoms after six months.”
• “Nine percent is the nationwide average HbA1c (measuring the
range of blood sugars for a three-month period, the main indicator
for how well diabetes is being controlled.) The average for our
patients is 7.5%, making an astounding impact on the quality of life
for these individuals.”
CareSouth CarolinaOutcomes Tell the Story
Making a difference for patients with asthma:Betty Railey, LPN at CareSouth CarolinaBishopville Center enjoys a hug from afive-year-old patient. (photo by Steve Roos)

in chronic care management,” Lewisremarked. “It’s behavior modification andlifestyle changes that achieve the results,and clinicians have to be willing to beparticipants in that.”
If patients aren’t engaged in thechange process, they’re probably notgoing to take the steps to improve theirhealth. They have to be willing to changetheir diet and to exercise regularly, totrack their blood sugars or check theirlung function, and they need to under-stand the difference that will make in theway they feel. Because the Chronic CareModel is patient-centered, patients actu-ally become involved in the managementof their own disease process.
Lewis related a group session sheattended with patients with diabetes wholive in a rural area. All the patients knewwhat their Hemoglobin A1c (blood glu-cose control) levels were. They knewwhere they started and they knew whattheir goals were. “They were charged up.They would say, ‘I know if I wasn’t doingthis that I would be gaining weight andfeeling bad.’ Many patients with chronicdisease are also severely depressed. Well,these patients aren’t,” Lewis enthused.
Lewis described the differences indepression as even more “staggering”than in diabetes. Clients are re-engagedin life, whether holding a job, going backto school or getting involved in thecommunity.
Why (Medical) Practice Doesn’tAlways Make Perfect
At the beginning of eachChronic Disease Collaborative,participants receive the most
recent evidence-based guidelines for care.Lewis said it’s a great way to make surethat clinicians are using the best informa-tion for treating their patients. “One ofthe first things we realized is that we hadto flag medical charts for chronic condi-tions,” she noted.
For patients with diabetes, the chartincludes an assessment and a flow sheet.For depression, the guidelines and theassessment were the same. For asthma,it’s an assessment which is conducted atevery visit.
Engaging the TeamPart of the major problem inour health care system today isthat physicians feel like they’re
on their own, responsible for managingthe health of their patients with acuteconditions and with chronic diseases.They have neither the systems to iden-tify patient conditions, nor the tools toimprove health, much less the supportfrom the other providers on their teamand the community. The Chronic CareModel paves the way for an organizedsystem of care.
“We did group visits for all threeconditions,” Lewis recalled. “That’s oneof your biggest payoffs. That’s wherepatients interact with each other andthat’s where once again the cliniciansbegin to understand they don’t have allthe answers. Patients share with eachother, and it’s very effective.”
Lewis believes that better chronic ill-ness care is compatible with high pro-ductivity. And she has the numbers toback it up, “The average productivity forCareSouth Carolina is one of the highestin the state, and we’ve participated inthree Collaboratives. The mental healthcounselors are saying the same thing.”
The national average is 4,100 encoun-ters per full-time provider per year. AtCareSouth Carolina, their productivitymeasures are at 6,572 encounters. Thedifference? A lot of little things, accord-ing to Lewis. Fifteen-minute visits don’tturn into disorganized 45-minute visits,because the clinicians are engaged inplanned care that’s proactive and doesn’tget side-tracked. An entire care team isinvolved in the comprehensive care ofchronically ill patients, not just the clini-cians. Patients are engaged in their visitsand come in energized. If a clinicianidentifies someone who is depressed,for example, the patient is immediatelyreferred to a mental health counselor.“The subsequent visits for that patientmedically are a lot less time consuming,”Lewis explained.
8
“I’ve had
diabetes for
four years
and nobody
has ever
told me
this stuff.”
The Rosa Lee Gerald Center, CareSouth Carolina’s $1.4 million state-of-the-art medical facili-ty, provides care to the underserved in the Society Hill community. (photo by Reid McBride)

Going forward, Lewis said CareSouthCarolina will expand its business plan toinclude staffing for certified chronic caremanagers who speak “both languages,”English and medical.
And their connections don’t stop atthe doors of their clinics. “Patients don’tlive in your clinic, they live in the com-munity. If you’re going to effect changewith them, you’ve got to be part of thecommunity,” Lewis said.
CareSouth Carolina’s community com-mitment is so strong that they have awhole division of community develop-ment that works both with the privatesector and with other agencies in thecommunity to sponsor programs andexpand the reach of their clinics.
“As a society we’re spending hugeamounts of money on medical education,and we don’t have a system that worksfor chronic care,” Lewis pointed out. “TheChronic Care Model works.”
High PlainsCommunity CenterHigh Plains Community Center in Lamar,Colorado, serves a population that’s 29percent uninsured, 43 percent privatelyinsured, with the remaining 28 percenton Medicare or Medicaid. Becauseapproximately 14% of their patients onlyspeak Spanish, all their materials andtheir care need to be provided in bothEnglish and Spanish.
The first evaluation of their pilot dia-betic population of 172 patients showedthat more than 98 percent had uncon-
trolled diabetes, with blood glucose lev-els averaging 9.5 percent, according toMonette Sutphin, Operations Officer. (Lessthan 7% is the goal.) Eighteen monthslater the average blood glucose was downto 8.4%.
Collaborative Helps Set the CourseDr. Hilton Ray, M.D., High PlainsMedical Director was so con-vinced that the Chronic Care
Model would elevate the clinic’s qualityof care that he persuaded the clinic’s lead-ership and Board to give it a try. By par-ticipating in a national Collaborative withteams from across the country, guided bythe expert staff from Improving ChronicIllness Care and the Institute of HealthCare Improvement, High Plains had theopportunity to learn and implement qual-ity chronic disease improvement quickly.
High Plains went to work develop-ing guidelines and protocols based on thelatest evidence. “The very first thing wedid was include standing lab orders sonurses could draw all the necessary labsfor our patients with diabetes,” Sutphinexplained. They also sent their nurses tostate training programs and specializedfoot assessment trainings.
Data Drive ImprovementIn order to track all of theirpatients with diabetes, and laterwith cardiovascular disease,
High Plains uses CVDEMS, a PC basedelectronic patient registry. The systemsimultaneously manages the patient data-base for both diabetes and cardiovasculardisease measures. It took a few years, but
the organization is now sold on budget-ing a data entry position, “because of allthe good that comes out of these num-bers, the feedback to patient charts andproviders,” Sutphin said.
“Early on, I said if we can’t get thisinformation on computer, we ought toforget it,” added Dr. Ray. “Once data entryis done, it’s not hard to pull out all therelevant information.”
“Hey doc, aren’t you going tocheck my feet today?”
The idea of patients as partnersin their health care is becomingpart of the health care zeitgeist,
bubbling up from policy circles, qualityimprovement programs and patientadvocates. It’s a timely trend, given theshortage of health care workers vis-a-vis the aging baby boomers, and theburgeoning increase in chronic condi-tions. Since most chronic conditions areheavily impacted by patient actions,emotions and lifestyle choices, themovement toward patient involvementin chronic disease is a potential matchmade in heaven with a sound basis.
To make sure their patients got a highdose of information and involvement,High Plains decided to jump-start theirdiabetes program by holding diabeticclinic days. The days were organized sothat about six patients at a time would bein the clinic for an hour and a half to twohours, with a team of providers availableto visit with each patient. The day wouldbegin with a nurse who conducted a footexam, showed patients how to check andclean their feet and recommended goodshoes. Patients then received bookletsthey could take home that reinforced theinformation given in the clinic. Next tocome in, a dietitian, who could offertraining tailored to the patient’s level ofneed and information. The third leg ofcare would come from a dental hygienistor dentist who would discuss the impor-tance of oral health for patients with dia-betes, and provide a referral to a dentist if
9
• 14% decrease in total mortality
• 21% decrease in diabetes-relateddeaths
• 14% decrease in myocardial infarction
• 12% decrease in strokes
• 43% decrease in amputations
• 24% decrease in renal failure
• $800 reduction in health care costs
Blood GlucoseReductions Pay Off
Longitudinal studies demonstrate that a one percentage point reduction inHemoglobin A1C (blood glucose) results in:

appropriate. Finally, the physician wouldcome in and address things such as med-ication adjustments, foot problems, labtests and overall health. At the first clin-ic, the physician would also work with thepatient to set a self-management goal.
Follow up from the clinics wouldoccur, within one to three months,depending upon the patient’s condition.“When they returned, we’d review theirlabs and review their self-managementgoals,” Sutphin said.
While these planned visits may sounddaunting to organize, Dr. Ray said theydeveloped a model where they were ableto deliver 12 comprehensive visits in ahalf day. “We came out OK,” he said. Andthe patient surveys after the clinics wereuniformly positive. “I’ve had diabetes forfour years and nobody has ever told methis stuff,” one patient wrote.
The clinics were so popular with theirpatients, according to Dr. Ray, that a buzzstarted in the community with patientsfrom other practices calling to see if theycould enter the program. “I hear frompeople in the community that they be-lieve our patients are getting better carethan some people with private insurance,”Dr. Ray said.
Innovation DeliversWhat could lead to either theperception or the reality thatformerly underserved patients
are receiving superior care to patientswith private insurance? Dr. Ray believessuccess lies in taking a prevalent chronicdisease and finding an innovative way toapproach the delivery of care. Once youidentify all of your patients with a givenchronic condition, and begin to managethose patients as part of a unified sys-tem of care, “it changes the encounter. Wedidn’t have all the tools before. It changedthe way I practiced in terms of checkingthe data on each patient each time theycame in. The other providers and I startedtalking about population stats and data,rather than just talking about individ-ual cases. It meant people got individualattention, but they also got attention aspart of a larger group.”
Ironically, one of High Plains’ mostvocal critics of the approach early on wasso impressed that he’s now leading theeffort to manage patients with hyperten-sion using the Chronic Care Model. Thespread to hypertension was a natural,since many patients have both conditions.At the beginning of 2002, High Plainshad 218 patients in their diabetes registryand 114 people in their cardiovasculardisease registry.
Reaching Out to the CommunityBecause High Plains is in a ruralcommunity, there wasn’t accessto the plethora of programs and
organizations available in an urban area.However, High Plains took advantage ofpartnerships where they could find them.Contracts with home health agencies andlocal dental offices supplemented theirservices. “Both the Spanish and Englishnewspapers have published quite a fewthings about the program,” Sutphinadded. Reports are sent to the state’s Dia-betes Control Program monthly and theprogram received two grants for patientand staff education.
System Support for the Model“When you’re trying to controlsomebody’s blood glucose, youhave them come in more often,
once they’re in control you have the sav-ings,” Sutphin remarked. “For the longterm, it definitely keeps folks out of thehospital.”
Between Sutphin and Dr. Ray, theleadership of High Plains was kept regu-larly involved in the outcomes from theModel and the philosophy behind thechange. “This work gets to our mission ofproviding quality health care with partic-ular attention to the unserved and under-served,” explained Dr. Ray. •
10
“People got
individual
attention, but
they also got
attention
as part of a
larger group.”
INITIAL CURRENTTRACKING INDICATOR RATE RATE
Percentage of patients with blood pressure less than 140/90 35.3% 62%
Percentage of patients with documented blood pressurecheck twice a year 47.1% 87%
Percentage of patients with a documented self-management goal 34.1% 59%
Percentage of patients who smoke 16.5% 25%**
Percentage of patients with creatinine checked annually 81.2% 89%
Percentage of patients screened for hyperlipidemia (cholesterol) 69.4% 82%
* Results after seven months
** Additional smokers were identified during the process, as clinicians began asking all cardiovascularpatients if they smoked
High PlainsCardiovascular Sample Tracking Indicators*

If system changes guided by the ChronicCare Model improve care in settings asdiverse as community health centers,academic medical centers, integratedhealth systems and health plans, whatimpact does the model have on a regularprivate medical practice? The Polyclinicis an 85-physician multi-specialty clinicin urban Seattle, Washington. Dr. NatalieRoberts, D.O., operates a one-personpractice in Wasilla, Alaska, a 40-minutedrive from Anchorage. Both organiza-tions assert that there’s a lot to be gainedfrom this innovative approach to chronicdisease management.
The PolyclinicThe Polyclinic learned the chronic careropes at the 2001 regional collaborative ondiabetes, organized by the Washingtonstate Department of Health, PRO-West, aquality improvement organization, andImproving Chronic Illness Care. In anera of physician and nurse burnout andfrustration, working with the Chronic CareModel gave a renewed sense of enthusiasmand satisfaction to the entire care team,
according to Colette Rush, Coordinator ofDisease Management Programs. And thatenthusiasm and progress was mirrored bythe patients who were pleased to becomepartners in their own health care processand watch their conditions improve.
Self Management: New Rolesfor Patients and Providers
Mark Cordova, M.D., one of thecollaborative team members,acknowledged that establishing
self-management goals for patients hasbeen a very different concept for him asa physician. “When I first heard about it,I thought it meant I’d walk in and say, ‘Iwant your blood pressure to be this’ andthen walk out,” he chuckled. “Of coursethat’s not it at all. It’s their goal.”
Physicians are trained to have all theinformation and be the ones who pro-nounce what kind of care will be pro-vided and what the patients’ goalsshould be, according to Dr. Cordova.“This is much more collaborative withthe patient, investing them in theirown care and feedback about what’simportant to them. Through this process
11
The PolyclinicSEATTLE, WASHINGTON
Natalie Roberts, D.O.Solo PractitionerWASILLA, ALASKA
P R I V A T E P R A C T I C E R E - D E F I N E D
the PatientsEngaging
•ORGANIZATION
OF HEALTH CARE
•DELIVERY
SYSTEMDESIGN
•DECISIONSUPPORT
•PATIENT
SELF-MANAGEMENT

I learn that they may be most concern-ed about blindness or something that Ihaven’t even worried about.”
The self-management aspect of theChronic Care Model also provides newroles for nurses. Dr. Cordova found thatthe function brings nurses closer to thepatients in terms of their motivations andconcerns about their disease. “The nursesbecome partners in the team, with a muchmore proactive role,” he added.
The Polyclinic introduced patients tothe new concept with a letter, outliningsome of the practice changes they couldanticipate. At the first visit, patientswould discuss their ideas for self-man-agement goals and compare where theircondition was to target benchmarks. “Ithink the patients see a real difference inthe way our visits are structured and theway in which information is delivered,”Dr. Cordova said. “Some of my patientshave told me they’ve waited all their livesto get this kind of information.”
Not all patients are ready to set a self-management goal at their first visit, andnot every staff member has been trained
in the technique. The Polyclinic antici-pates that their progress in this area willcontinue to grow.
Rush said it’s important to have allthe tools ready for the visit. So eachexam room now has a file box filled witha variety of materials and tools—fromreferral forms to educational materials—
that providers need to give a visit thegreatest possible impact. Rush saidthey’ve designed the office around theconcept of organized systems of care andpatient involvement.
Guidelines and Information:New Systems for Providers
The Polyclinic developed amodel for the clinic to deliverdiabetes care derived from
evidence-based guidelines. While thatmay sound like an obvious step for themanagement of a chronic disease, Dr.Cordova, like others who’ve worked withthe Model, found that putting this kindof discipline into the practice improvesit significantly and consistently. Theclinic follows updated American Dia-betic Association guidelines for diabetesand also developed referral guidelinesfor specialists.
“Insurance companies are now comingto the physicians telling us we have apossibility of getting better reimburse-ment based on the confirmation thatwe’re providing better quality care. This isa system that allows us to do that,” Dr.Cordova said.
12
INITIAL IMPROVED PERCENTAGE, PERCENTAGE,
MEASURE JAN 2001 FEB 2002
Hemoglobin A1c (blood glucose) less than 9.5% 75% 90%
Blood pressure less than 140/90 38.5% 54.20%
LDL (cholesterol) less than 130 55.7% 81.00%
Percentage of patients who have had HbA1Cin previous six months 63% 85.80%
Percentage of patients with LDL checkedin previous 12 months 73% 92.12%
Patients whose kidney functions were checkedin previous 12 months 50.4% 84.70%
Patients with annual retinal exams 19.7% 50.00%
Percentage of patients with self management goals 0% 33.16%
The PolyclinicTracking Measures
100%
80%
60%
40%
20%
0
2/01 3/01 4/01 5/01 6/01 7/01 8/01 9/01 10/01 11/01 12/01 1/02 2/02 3/02 4/02
in last six monthsPatients with HbA1c testBy tracking patients with diabetes, the Polyclinic was able to dramatically increase the number
of patients whose blood glucose was being checked on a regular basis. The Polyclinic’s rate
of checking patients’ blood glucose levels every six months rose from 63% to almost 86%.
GOAL = 96%

The Polyclinic has 900 patients withdiabetes in their registry, a program thatnot only tracks who the patients are butalso what their clinical targets are andwhat labs they might need. “The reg-istry is the cornerstone of chronic dis-ease management and the Chronic CareModel,” noted Rush.
Planned Care Reaps BenefitsRush said patients with dia-betes now have planned visits.Before they leave the clinic,
they make appointments to return inthree months and the database ensuresthat the visits take place. Before thePolyclinic instituted the Chronic CareModel, patients were advised how soonto come back, but the responsibility formaking the appointment lay with thepatient. “People would have good inten-tions, but sometimes forget,” explainedGloria Dillon, M.A., one of the key mem-bers of the nursing staff at the start ofthe project. “This way, we don’t let themslip through the cracks.”
Another simple change that’s made a“huge impact” has been asking patientsto have their labs drawn in the week priorto their visit. “Staff review the labs andthey’re prepared to talk with the patientswhen they come in,” Rush noted.
The Polyclinic also had great successconvening group visits. Approximately20 patients replace one of their regularquarterly visits with a two-hour groupvisit. The visit begins with introductions,and then patients go around to differentstations. Patients have their labs drawn ifnecessary, go to the nurse’s station forvital signs and self management updates,foot exams, and vaccinations if they’redue. Then the doctor meets with themindividually and reviews their charts,their reports on self-management goalsand their labs. “In between the stations,the patients have an opportunity to pro-vide emotional support to each other, talk
to a pharmacist and review educationalmaterials,” described Rush.
In the second hour of the visit, theclinic organizes some type of clinical pre-sentation. Rush said that for somepatients this format works really well,“Different patients learn differently. Forthe right group, this is significant.”
Rush noted that they’ve actually in-creased revenues with the group visitswhile “providing better care.” The Poly-clinic plans to conduct group visits quar-terly and hopes to expand the number ofgroups they conduct.
The Chronic Care Model is now partof the Polyclinic’s strategic plan. Whilediabetes was the first target, plans are toadd cardiovascular disease in 2003.They’ll apply the same approach, begin-ning with a pilot group of physiciansand patients, then spreading the Modelto additional physicians and patients asthe program develops.
“Costs are so out of line,” Rush added,“Prevention makes sense.”
Natalie Roberts, D.O.The solo medical practice of NatalieRoberts, D.O., is located in Wasilla,Alaska, which offers a rural lifestyle withaccess to some of the most spectac-ular sites nature has to offer, includingthree mountain ranges, four state gamerefuges and six recreational rivers. Some30 percent of the population commutesto work in nearby Anchorage.
Easy to Change, Challengingto Implement
You may not have a lot of re-sources when you operate asolo practice, noted Dr. Roberts,
but “if I want to change things, I get themchanged in two days. It actually worksreally well, because you don’t have to dis-cuss it with 10,000 people.”
The team that worked with theChronic Care Model at Dr. Roberts’ prac-tice included the doctor, the officemanager Joyce Johnson, and a medicalassistant. The team participated in theregional Alaska collaborative, organizedby PRO-West and Improving ChronicIllness Care. Participating in an improve-ment effort was challenging for Dr.Roberts. Things that are normally diffi-cult for a single doctor practice, like staffturnover, take on a whole new level ofdifficulty during a collaborative. In addi-tion, in order for Dr. Roberts to attend alearning session, the office would haveto close for that day.
Incorporating evidence-based guide-lines wasn’t hard for Dr. Roberts, whoalready knew much of the information.However, she did learn a more focusedapproach to diabetes management andnew information about heart disease. “Iknew it was important to get patients’blood glucose levels down, but I didn’tspend as much time before getting themdown. I recently went to a lecture where Ilearned that everyone with diabetes
13
“Some of
my patients
have told
me they’ve
waited all
their lives
to get this
kind of
information.”

should be on ace inhibitors because itprevents heart disease.”
Education and a Whole Lot MoreGetting patients involved intheir own care means Dr.Roberts spends a good deal of
time educating her patients and givingthem options. For example, if patients’blood glucose level is above 7%, she’lllet them try to manage it with diet forthree months. In between visits, her staffwill call patients and reiterate the goal. Ifthere’s no improvement, she’ll add amedication.
In the meantime, patients go homewith graphs, generated by an electronicdatabase program, where they can charttheir progress on blood glucose, choles-terol, blood pressure, LDL and weight.“That’s part of our self-managementwork, to try to get them to see their num-bers to understand where they are and tochange because they want to see theirgraph improve,” explained Johnson,whose role includes managing the prac-tice’s registry of patients with diabetes.
Johnson recalled one patient who hadrefused to admit he had diabetes. Hiswife convinced him to come in when the
office started the Collaborative and “he’sbeen incredible. He loves his graphs; it’sjust something that’s really positive forhim. He lost 60 pounds in seven months.He was just not defeated anymore.When we started treating him like hecould make the change, it empoweredhim to take control and he did it.”
Johnson said for the most part, there’sbeen a very positive response frompatients who appreciate the extra “TLC.”
Dr. Roberts’ approach with herpatients has been, “Ok, here’s what I’mgoing to do, what are you going to do? Alot of my patients had been educated butwhen you survey them, they didn’t knowwhat they needed to know in order tomake a difference.”
Dr. Roberts said regular contact withpatients with a chronic disease is vital.“All my patients are scheduled for follow-up visits when they leave here. We do cri-sis care in between,” she noted. Patientsalso receive personal congratulationscards from the office if they meet thebasic measures.
Once their electronic database identi-fied all of their patients with diabetes,Johnson set up a system where all chartsare flagged with special stickers and
she enters information into the databaseafter every visit.
There aren’t extensive communityresources in Wasilla, Alaska, but the prac-tice takes advantage of what’s available.They work with the diabetes educatorat their local hospital and a statewideresource for smoking cessation. They alsorely heavily on pharmaceutical represen-tatives. “We get as many free materialsfrom them as we can,” said Johnson.
The practice now plans to extend theModel and its elements beyond the pilotpopulation of 74 patients. For example,the practice has adopted self-manage-ment goals across the board, in a varietyof conditions.
Dr. Roberts and Johnson both acknowl-edge that it’s more work to provide pa-tient care this way, but neither would haveit any other way. “High quality medicinekeeps your business booming,” said Dr.Roberts. “And you go home with a sense ofsatisfaction because you’re doing the rightthing for your patients.” •
14
“When we
started treating
him like he
could make
the change,
it empowered
him to take
control and
he did it.”
INITIAL IMPROVED PERCENTAGE, PERCENTAGE,
GOAL JAN 2001 DEC 2001
80% of patients with HbA1c (blood glucose) less than 8% 69% 78%
50% of patients with LDL (cholesterol) less than 100 33% 61%
90% of patients w/LDL less than 130 80% 89%
60% with blood pressure below 140/90 39% 50%
90% with annual foot exams 5% 94%
Percentage of patients with self-management goal 5% 64%
Dr. Roberts’Sample Tracking Measures

Case in point: Hill Health Center’spediatric asthma program, Project AIR,(Asthma Improvement Resources) in NewHaven, Connecticut. “I think that ourkids with asthma are getting better carethan they are at a lot of places in thiscity because we’re providing comprehen-sive management,” explained GenevieveMack, Pediatric Nurse Practitioner andDirector of Hill Health’s pediatric asthmaprogram. “We’ve had patients who havetransferred here because their childwasn’t getting better and the parentsheard about our programs.”
Or Clinica Campesina, in Lafayette,Colorado, where both providers andpatients have gone from feeling “hope-less” about chronic conditions to feelingengaged and excited about the changesand improvements that are occurring dayin and day out, according to team leaderCory Sevin, R.N., M.S.N.
The driving force behind the successfor these clinics can be traced to a deci-sion made by the Department of Healthand Human Services’ Bureau of PrimaryHealth Care. The Bureau recognized thatproactive, organized chronic disease
management represented a key strategyfor reducing the disparities in healththat afflict low-income and ethni-cally diverse individuals around thecountry. Hill Health Center and ClinicaCampesina were two of the Bureau’s88 centers that participated in ground-breaking diabetes management effortsbeginning in 1998 using ImprovingChronic Illness Care’s Chronic CareModel and the Institute for HealthcareImprovement’s improvement model. Forboth centers, the diabetes work provideda springboard for organizing the care ofother chronic diseases as well.
Project AIRHILL HEALTH CENTER’S APPROACHTO ASTHMA IMPROVEMENT
Imagine, for a moment, that you’re apediatric provider. Your training, yourpractice and your health care system allare geared to handle acute health carecrises. A patient breaks a bone or getsstrep throat. You patch them up, prescribemedication and send them home untilthe next time something goes wrong. For
15
R IVALINGPRIVATE CARE
Hill Health CenterNEW HAVEN, CONNECTICUT
Clinica CampesinaLAFAYETTE, COLORADO
C O M M U N I T Y H E A L T H C E N T E R SM E E T T H E N E E D S O F T H EU R B A N P O O R
If there’s a startling trend in chronic disease management today, it’s this:Patients in a number of federally qualified community health centers arereceiving higher quality health care for their chronic conditions than manypatients with private insurance. These patients typically come from under-served populations, often have Medicaid, Medicare or no insurance and maybe combating challenging life issues on top of their chronic diseases.
•ORGANIZATION
OF HEALTH CARE
•DELIVERY
SYSTEMDESIGN
•CLINICAL
INFORMATIONSYSTEMS
•PATIENT
SELF-MANAGEMENT
•COMMUNITYRESOURCES

a portion of the population with onlyacute conditions, that kind of approachworks reasonably well. But when it comesto individuals with chronic disease, thatapproach leaves patients with little helpto personally manage their condition andavoid exacerbations.
Take asthma, for example. The Nation-al Institute of Health established guide-lines for asthma treatment in 1991. Butthe only way providers can be sure they’remeeting those guidelines is if they canidentify which patients have asthma. Andchances are, unless the clinic or systemhas established a mature disease manage-ment system, there’s no way to do that.That was one of the first things Hill HealthCenter discovered as practitioners beganworking on asthma improvement in 2000.
The pilot program was established ata school-based health center, with ser-vices provided by a nurse practitioner, asocial worker and a health educator. AsHill Health Center developed a patientregistry, identifying all their pediatric pa-tients with asthma out of the 500 middle
school students at the school-based cen-ter, Mack said they were able to track awide variety of measures both for indi-vidual patients and for the population asa whole. The registry can be used toschedule appointments and to identify thedevelopment of patterns. “For example, Ican query what children have winter astheir time period with greater triggers sothat we get to them ahead of time beforethey have problems and increase themedications that control their conditions.We use it to see if patients are slippingthrough the cracks. It helps us learn aboutour patients as a whole,” Mack explained.
As the program spread beyond thepilot population, the team found thatmore work needed to be done. Even whenpatients were identified, Mack said theteam still wasn’t conducting severityassessments, addressing asthma triggersand trigger avoidances, scheduling followups, appropriately referring to specialistsor utilizing community resources. “Whatwe needed to do was establish a structureand support that allowed our pediatricproviders to deliver that kind of care rou-tinely,” Mack explained. “You can’t expectpeople to jump ship and develop a newboat while they’re trying not to drown.You have to give them a new boat.”
DESIGNING A DIFFERENT KIND OF SYSTEMAs the program spread to HillHealth Center’s clinics, chang-ing the design of the delivery
system, one of the Chronic Care Model’ssix elements, was “critical,” according toMack. The Clinic established a division ofresponsibilities, so that physicians couldbegin relying on Community HealthWorkers and R.N.s to provide some of thekey functions that make comprehensivecare possible. Community Health Work-ers began taking the initial history andmade sure all of the necessary asthmatools—including guidelines and referralsources—were prominent in the patients’charts. The asthma nurses were trained toprovide more education ranging frommedication usage to trigger avoidance,environmental control and an emergencyplan. The pilot program that began withone clinician and 30 patients grew to
incorporate 10 Pediatric providers and aregistry of more than 900 patients in HillHealth Center’s main comprehensiveclinic and its eight school-based and pri-mary care satellite clinics.
16
“YOU CAN’TEXPECTPEOPLE TOJUMP SHIPANDDEVELOP ANEW BOATWHILETHEY’RETRYING NOTTO DROWN.YOU HAVETO GIVETHEM ANEW BOAT.”
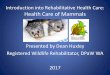
THE COLORSOF A
STOPLIGHTwill help you use your
asthma medicines
Project AIR uses color coding to help patientsunderstand their conditions, use the rightmedications, and seek appropriate treatment.
REDDANGER ZONEPATIENT’S ASTHMA ISGETTING WORSE FAST:
Medicine is not helpingBreathing is hard and fast
Nose opens wideRibs show
Can’t talk well
GET HELP FROMA DOCTOR
YELLOWCAUTION ZONEPATIENT HAS ANY ONE
OF THESE:First signs of a cold
Exposure to known triggerCough or mild wheeze
Coughing at night
ADD QUICK-RELIEFMEDICINE
GREENGO ZONE
PATIENT HAS ALLOF THESE:
Breathing is goodNo cough or wheeze
Sleep through the nightCan work and play
USE PREVENTIVEMEDICINE

Group education was another supple-ment to a physician-only model of healthcare. While the asthma team found therewas a lot of interest, there were also a lotof barriers to overcome, including timing,flexible scheduling and transportation.Two people would run the group; one withmedical expertise and another who couldprovide child care if that was an issuefor parents. The asthma team was able toenlist community and corporate support,ranging from supplying transportation todonations to providing food, door prizes,raffles and asthma equipment.
“In order to really make a change,education of our providers was vital,”Mack emphasized. Ongoing in-serviceswere used to reinforce use of the latestevidence-based guidelines and protocolsfor care, the Chronic Care Model elementknown as Decision Support.
Hill Health Center created a flow sheetthat guides the provider through an asth-ma assessment and treatment plan basedon guidelines which are printed in con-densed form on the back of the flowsheet. They also posted the guidelines incolor coded laminated charts at stationsand displayed user-friendly books inexam rooms.
PATIENT SELF-MANAGEMENT:SO WHAT HAVE I DONE FOR ME LATELY?
Another important aspect of theChronic Care Model lies in itsemphasis on patient self-man-
agement, or enlisting patients in improv-ing their own care. For this program ele-ment, Hill Health Center’s goal was thatevery patient with asthma be given anasthma action plan. Use of an action planwas one of Hill Health Center’s trackingindicators. Research shows an action plancontributes to reductions in asthma mor-bidity and deaths because it gives patientsa tool that includes guidelines for what todo if their health condition changes.“We’re giving patients a lot of informa-tion. Kids with moderate, persistent asth-ma may have three to five medications touse at different times. This can get veryconfusing,” Mack noted. “The action planhelps them track their symptoms andmanage their medications.”
Mack described the process of develop-ing the action plan as “patient-centered.”The clinic developed a format, tested itwith patients, got feedback and revised it.In addition to guidelines for medication,the action plan also incorporates a patientgoal. Does a patient want to play basket-ball, sleep well, miss less school, go tothe second floor of the house? Whateverthe goal the patient wants is included.“Sometimes kids are so adjusted to thechronicity of their disease that they can’tthink outside the box. We ask them, ‘whatcan’t you do because of your asthma thatyou’d like to be able to do?’”
Use of the action plan has been so suc-cessful—given to100 percent of the pilotpopulation and close to that in the spreadpopulation—that Hill Health Center’sinternal medicine department has begunto adopt it in order to meet their chroni-cally ill patients’ needs as well.
In addition to the action plan, self-management tools include kits for every
patient, videos, comic books, peak flowmeters and patient brochures.
The Chronic Care Model is such anintegral part of Hill Health Center that it’sreflected in the mission and businessplans as an absolute priority and focusin chronic care. That total commitmenthas given Mack the ability to negotiatewith HMOs to cover key medications anddurable medical equipment. “We used tohave problems getting reimbursement forcertain things and had to fight each andevery time. Once we developed more of arelationship with the claims administra-tor, we were able to say, ‘we’re reducingcosts here, these patients have fewer hos-pitalizations and emergency visits.’ Somemanaged care companies have been veryaccommodating, agreeing to cover thingson a group basis and taking out a lot ofthe administrative and bureaucratic stepsthat made it difficult,” Mack said.
Mack noted that while the clinics havenot tracked hospitalization rates, asthma
17
TRACKING INDICATOR RATE OF SUCCESS
CONTROLLER MEDICATION (daily 100%asthma medication that’s preventive or anti-inflammatory) used with mildor moderate asthma
SCHOOL ABSENTEEISM due to asthma Absenteeism less than one day per less than one day per two weeks two weeks since Jan. 2001
EMERGENCY VISITS due to asthma Less than 1% on average, per two weekssince Feb. 2001
PEAK FLOW RATE PERFORMANCE Greater than 80% in both the pilot(lung function test that patient can and spread populationsmonitor at home) average increased
ASTHMA ACTION PLAN given to patients Achieved and sustained 100% rate inpilot population, achieved 100% inJuly 2001 with spread population withslight drop subsequently
SYMPTOM-FREE DAYS 90% for two Started at 36% in January 2000; week periods (this was the collaborative’s reached almost 80% (the nationalonly long-term goal) standard is 70%)
TRACKINGINDICATORS
H I L L H E A L T H C E N T E R ’ S

used to be a very frequent reason for hos-pital admissions of their pediatric patients.“Now we get really upset when we have asingle patient who is hospitalized for asth-ma. We meet just to determine what wentwrong in our care,” Mack added.
HARNESSING COMMUNITY RESOURCESAs an urban community healthcenter addressing what can bean environmentally-triggered
disease, community resources haveplayed a significant role in Hill HealthCenter’s success. For example, close part-nerships with school nurses led to thedevelopment of comprehensive asthmamanagement plans for the schools. “Nomatter how high a standard of care youdeliver at the clinic, if the child is stillbeing exposed to asthma triggers at homeand at the school, medication and teach-ing are useless. We had to reach the com-munity to address these other issues,”Mack explained.
Other partnerships included a city-funded grant program with VisitingNurses Associations and local publicCommunity Action Agency, an organiza-tion that addresses issues affecting low-income residents with home environmentproblems. Mack said visiting nurses,under a pilot program, are conductinghome assessments for 20 families whohave children with asthma to review suchenvironmental issues as pest control,cockroaches, dust, mold, ventilation sys-tems, and carpets that need to be pulledup. The Community Action Agency thenactually makes those changes when indi-cated. “We’re hoping to demonstrate sig-nificant quality of life and lung functionimprovements so we can go back and tellthe insurance companies or other fundingsources this is something you shouldinvest in,” said Mack.
Hill Health Center has worked closelywith the American Lung Association interms of asthma camp, fairs and educa-tional materials. And pharmaceutical com-panies have donated “everything we’veneeded from educational materials to peakflow meters, patient samples and money tobuy equipment to set up a state-of-the-artasthma program,” Mack described.
Hill’s Mack doesn’t go a week withoutmultiple requests for information abouttheir program from the media, politiciansand other health care systems around thecountry. At a time when massive numbersof people are disillusioned with our healthcare system across the country, HillHealth Center’s staff is enjoying arenewed commitment to the practice ofmedicine. “We can actually change healthcare in this country if we support the useof this Model to change care.”
Changing RolesDIABETES IMPROVEMENTAT CLINICA CAMPESINA
THE CASE FOR QUALITY IMPROVEMENTThe proportion of patients withdiabetes is very small at ClinicaCampesina’s three community
health centers in urban Colorado, accord-ing to Cory Sevin, R.N., Vice President.“But diabetes ends up as one of the top10 reasons for a patient using a clinic,so these patients are high users of healthcare,” she explained, making it strategi-cally important to better manage thecourse of their illnesses.
A normal Hemoglobin A1c (HbA1c orblood glucose) level is around 6%. Butpatients with uncontrolled diabetes can
have HbA1c levels of 12% or higher.Before adapting the Chronic Care Model,the physicians would see patients withlevels above 10% and think, “No way amI going to get that down to 6%,” Sevinexplained. But at the same time the clin-ics began using the Model, a researchstudy was released indicating that evendropping the blood sugar level one per-cent, from 12 to 11 for example, makes adifference in terms of quality of life, mor-bidity and mortality.
“Now the whole organization waslined up to figure out what it would taketo help this patient and provider makeprogress,” Sevin said.
Coupled with the new approach tochronic disease management was therapid improvement process from theInstitute for Healthcare Improvement.Prior to the collaborative, it took twoyears to get consensus about a diabetesflow sheet. “Here was an expert saying,‘Try it on Tuesday. Try something differ-ent on Wednesday.’ It really changed thepractice of medicine for our providers,”Sevin said.
“We were definitely a provider orient-ed system,” acknowledged Sevin. “Veryfew of our providers had worked to getthe patients involved, it’s not somethingthey teach you in school. Providersunderstand now that there’s an expecta-
18
MEASURE INITIAL RATE IMPROVED RATE
Average HbA1c (Blood Glucose) 10.5% in Oct. 98 8.7% Sept. 01
Percentage of patients with two HbA1cs 14.7% in Oct. 98 45% Sept. 01measured three months apart, twice a year
Percentage of patients receiving eye exams 7% Feb. 99 27% Sept. 01
Percentage of patients receiving foot exams 15% Feb. 99 56% Sept. 01
Percentage of patients with a self-management 0% Feb 99 46% Sept. 01goal collaboratively set
TRACKINGINDICATORS
C L I N I C A C A M P E S I N A ’ S

tion that they engage the patient andinvolve them in their own care in more ofa patient-focused way.”
By the time Clinica Campesina workedthrough the diabetes collaborative, thesepatients with previously unmet needs hadnew roles, as did their care teams.
ORGANIZING CAREUsing a patient registry, pro-viders would regularly learnwhich of their patients have
diabetes and receive updated informationon all of the tracking indicators. “Wecould look at who we weren’t reachingand determine their biggest need. Thatinformation became the impetus fordeveloping diabetes fairs, for example,because we found we weren’t impactingthe whole population,” Sevin explained.“You can’t do the Chronic Care Modelwithout a registry.”
Clinica Campesina hosted diabetesfairs twice a year at two clinics, withmore than 130 patient visits, includingrepeat customers. The fairs providedpatients with a broad range of informa-tion, from managing blood glucose toeating healthy and getting eye checks.Sevin recalled one patient who hadn’tbeen able to take off from work to getregular check ups who was able to takeadvantage of a dilated eye exam at thefair. It turned out that he had retinaldamage. “It was a great way to reachpatients who have a hard time makingregular visits and it really makes themfeel supported,” she said.
Using the latest evidence-basedguidelines, Clinica Campesina developeda flow sheet with simple algorithms ofcare for the providers. According toSevin, the flow sheet guides the provider,step by step, through a series of deci-sions. “For example, if there’s protein inthe urine, then the flow sheet providesguidelines for treatment. Another exam-ple is guidelines for putting patients withhigh blood pressure on the right medica-tions,” she described.
Developing the guidelines and makingsure they’re utilized can be two separatetasks, so the guidelines were reinforced atclinician meetings once a month.
TEAM BUILDINGThe team also worked to identi-fy who besides the physicianscould perform key tasks. How
could medical assistants become part ofthe team? “We found many things theycan do. For example, they can review thediabetes flow sheet for needed tests andbegin the progress notes with things thatare needed. They also are able to conductfoot exams and check in with patientsregarding their self-management goals,”Sevin added.
What it came down to, Sevin related,was creating a team approach so thatmore people are able to cover all thebases. And the patient response? “Wefound that engaging them differently waseffecting their blood glucose control. Wealso got verbal feedback that they weremore hopeful and more involved withtheir care,” said Sevin.
Clinica Campesina’s commitment tothe Chronic Care Model is long term and
lasting. “We’re looking at how to institu-tionalize it so it’s not dependent on a par-ticular person. You need champions, butit has to be institutionalized enough tocontinue,” Sevin said.
EMPOWERING THE PATIENTSBased on prior experience, pro-viders knew that they weren’tgoing to be able to shift their
patients’ health care without involvingthem in the process. When the clinicsbegan measuring the number of patientswith documented self-management goals,they started at zero and the physicianswould get a report once a month wherethey’d see that. “We didn’t say you’rebad because you don’t know how to dothis,” Sevin emphasized. “After a coupleof months, we started educating smallgroups of providers on things they coulddo in 15-minute visits that wouldn’t beoverwhelming for them or their patients.Part of it was learning to ask questionsdifferently.”
Sevin noted that evidence shows ifproviders and patients collaboratively setself-management goals, a follow-upphone call in two weeks really reinforcesthe goal. “It doesn’t have to be theprovider, just someone with reasonableskill in communicating.”
In addition to raising the issuewith providers, Clinica Campesina wentstraight to the patients. Patients receivedseries of guidelines on a regular basis toengage them on what their care shouldlook like so they come to each visit witha different set of expectations. They knowtheir feet should be examined at everyvisit and their eyes checked once a year.
They learned what their blood glucoselevels were and how often they should bemeasured.
In an era of cutting corners, how doesClinica Campesina justify taking on thislevel of systemic change? “We did itbecause our primary goal is quality forour patients. And in a sense we’re man-aged care because no one else is going totake care of our patients. This kind of careprovides patient and provider satisfactionand in the end our quality of care doeshelp us financially,” Sevin added. •
19
“WE STARTEDEDUCATINGSMALLGROUPS OFPROVIDERSON THINGSTHEY COULDDO IN15-MINUTEVISITS.…PART OFIT WASLEARNINGTO ASKQUESTIONSDIFFERENTLY.”

Full Court
Premier Health Partners in Dayton, Ohio,is a complex integrated health systemwith two hospitals, 100 physician prac-tices, a long-term care facility and ahome health agency. When the systemdecided to tackle comprehensive diabetesimprovement, the team recognized that itwould take a “full court press”, accordingto Evan Steffens, R.N., M.S., Director ofClinical and Quality Systems, PrimaryCare Physicians Network, part of PremierHealth Partners.
Like many pioneers in systemic qual-ity improvement, Premier Health Part-ners launched their improvement processwith a small, committed core team.Steffens’ counsel to other health sys-tems: make sure you give physicians theright tools and enough training. “Youcan’t just hand them a standard, beatthem over the head, and say ‘bad doc.’
You have to give them the tools and say,‘great doc, crummy system.’”
Before signing up for the diabetes col-laborative that got underway at the endof 1998, Premier Health Partners hadtackled diabetes improvement by dissem-inating care standards to their physicians.But the team quickly recognized that sim-ply distributing more forms to physicianswith busy practices wasn’t going toachieve their goal. A better strategy: usethe Chronic Care Model to identify healthsystem changes needed to manage chron-ic illness more effectively and improvepatient outcomes. Because the Modelfocuses on involving patients and givingpractice teams the right systems and theright tools to proactively manage theconditions, it delivers greater results.
“We dramatically shifted our focus fromprocess to outcomes,” Steffens explained.
20
You’re a primary care physician with a busy practice, under pressure to see more patients.
You don’t have enough time.
You’re a patient with uncontrolled diabetes and you are not sure how to manage your
condition. You don’t have the right skills.
You’re an administrator wanting your health system to deliver care that improves health
and follows best practices. You don’t have the right system.
Premier Health PartnersDAYTON, OHIO
PressAN INTEGRATED SYSTEM TACKLES CHRONIC ILLNESS CARE
•ORGANIZATIONOF HEALTH CARE
•DECISIONSUPPORT

Plan Your WorkThe first order of business wasdeveloping ambulatory diabetestreatment guidelines. The next
step was developing Premier’s DiabetesInnovation Tool Kit, which contained avariety of tools and a range of options.Materials for physicians included:
• Diabetes Documentation Flow Sheets
• Adult Summary of Care Forms, thatincluded problem list, preventive inter-ventions and a mechanism to customizethe form with stickers for multiple chron-ic disease conditions
• Chart stickers for diabetes and smoking
• Patient visit cards
• Nursing visit documentation forms
• Standing laboratory order forms
• Foot exam documentation forms
• Pertinent diabetes research articles
• Guidelines for planned visits
• Patient information and reminder letters
They also made sure that physicianshad guidelines for specialist referrals andmonofilaments in exam rooms so thatthey could easily conduct critical footexams. Physicians were taught to usethese tools in planned visits and torestructure how they supported patientsin their self-care.
Materials for patients included:
• Patient education posters for exam rooms
• Blood sugar home forms
• Diabetes checklists
Work Your PlanSteffens and Meenakshi Patel,M.D., Chair, Quality Committee,Miami Valley Hospital, another
part of the Premier system, individuallyvisited every office in the pilot project,
and over time, every office in the rest ofthe organization. “We took the physicianschart review results, and the tool kit. Wetalked about what we were trying to doand we offered them the tools to helpthem get to targets,” Steffens said. “Weunderstand that there’s no way everyphysician can remember everything she orhe should do for patients with diabetes.”
Steffens continued the “academicdetailing” of the physicians’ practices ona quarterly basis to learn what was andwasn’t working. The response to theChronic Care Model was strong initiallybecause the pilot team consisted of vol-unteers. However, the team also recruit-ed a couple of physicians who tend tobe “skeptics,” and Steffens reported theyalso did very well. “I think they respond-ed positively to the concept of a menuof ideas. We didn’t dictate, but suggest-ed that the tools might help their out-comes,” she said.
The team’s philosophy was to help theclinicians figure out how to do the workin the context of very busy practicesunder pressure to see more patients, more
quickly. Steffens found that once the first20 percent of physicians were successful,the remaining 80 percent would follow.
Premier’s team started working withone physician and over the course of sixto nine months, added 18 practices.Eventually, the entire network of 100physician practices incorporated theChronic Care Model in their approach todiabetes care, with each physician caringfor between 100 and 200 patients withdiabetes. With diabetes appropriatelymanaged, the network is adapting theModel to the full range of chronic illness-es, including cardiac disease, asthma, aswell as to preventive care.
Steffens said the entire Premier orga-nization received American DiabetesAssociation certification so that theycould get reimbursement for all theirteaching programs in order to supporteducation. They were successful at nego-tiating with one of the local HMOs topay for diabetes education that supple-ments the formal, hospital-based educa-tion programs with a two-hour “survivalskills” curriculum delivered to patientsindividually. According to Steffens, thenurses that provide the survival skillsprogram undergo more than 16 hours ofadditional education in diabetes andadult education. “They teach the basicsto patients who, for whatever reason, areunable to get into the formal educationprogram at the main hospital in a timelymanner,” Steffens explained.
Organizing a health system to supportquality improvement work is a key ele-ment to the Model. Disease managementhas been part of Premier’s business plansince 1999, and in 2001 meeting certaindisease management criteria became partof the executive bonus structure. Steffensalso notes a growing trend among em-ployers to provide bonuses to healthplans that meet certain quality targets.The health plans in turn are beginning topartner with the physicians to help meetthose targets.
21
“You can’t just hand
them a standard,
beat them over the
head, and say ‘bad
doc.’ You have to
give them the tools
and say, ‘great doc,
crummy system.’”

“In order to make gains in diabetesmanagement, we must shift from the cur-rent model of a random event in the mid-dle of a busy day to a planned event in amanaged day.”
In 2002 Steffens is looking forward tothe implementation of a disease manage-ment registry and reminder system thatwill print sheets showing what patientsneed to have done. This will mark the firsttime Premier has had a registry in morethan a handful of practices and the firsttime the registry will be electronic. Thenetwork received grant money to pur-chase an enhancement to their billingsystem with a new clinical module.
Measuring successThe tracking indicators for successinclude:
• Hemoglobin A1c (HbA1c—blood glu-cose) checked twice each year
• HbA1c less than 7 percent
• Weight and blood pressure checked atevery visit
22
MEASURE BEFORE AFTER
HbA1c (blood glucose) under 7% 1999: 42% 2001: 70%
HbA1c checked twice a year 1997: 67% 2001: 90%
Foot exams using monofilament testing 1997: 61% 2001: 78%
Annual urine protein measures 1997: 52% 2001: 78%
Ace inhibitors with positive urine protein 1999: 38% 2001: 80%
actually making a difference in people’slives and they have a process that some-one is helping them with.”
In addition to improving the care andhealth of patients with chronic diseaseand providing a more rewarding systemfor clinicians, Steffens believes a strongbusiness case can be made for employingthe Chronic Care Model. At the beginningof the project, she reviewed approxi-mately 200 patients with diabetes fromone practice. Of all of the patients, lessthan 10 percent were up to speed with alltheir quality criteria. They’d been in tosee the doctor frequently, as many as 35times the previous year, typically for anacute condition. But the diabetes carenever took place. “If the patient wouldcome in twice a year for intense diabetesvisits, with the right documentation tobe coded at an appropriate level for acomprehensive visit, it would drasticallychange the nature of the physician’sbilling,” Steffens said.
“You have to change the system,”Steffens emphasized. “The delivery ofmedicine is not just about what Dr. Smithdoes in his practice. You have to re-thinkevery aspect of how you deliver care,from how you make appointments to howyou put your charts together, to how youput patients in the room to what you doin the visit.” •
• Blood pressures below 130/80
• Diet counseling provided on an annualbasis
• Eye exam, foot exam, urine protein,conducted annually
• Patients with positive urine proteingiven ACE inhibitors
• LDLs (cholesterol) less than 100
• Evidence that home glucose testing isbeing performed (as evidenced by docu-mented home charts).
For patients, one of the most com-pelling aspects of this approach to care isthat they’re empowered to make changesand improve their health. Collabora-tive member Dr. Patel told of one patientwho came to her with uncontrolled dia-betes and a leg already amputated. “Weswitched her to an oral regimen and thencounseled her on diet, exercise, the im-portance of foot and eye exams and shejust took off. Her HbA1c is around 6.1%and every visit she brings me beautifulcharts of her blood sugar mapped out.Her quality of life has improved dramat-ically and she feels 100 percent better,”Dr. Patel added.
For physicians, the Model has thesame effect, according to Dr. Patel. “Theyabsolutely feel empowered that they are
This chart, displayed in all of the examrooms, gives patients a visual reminderof how to manage their diabetes.
ResultsSample

D O T SHealth plans can play a significant rolein the management of chronic disease,from reimbursing for quality outcomesto providing sophisticated case manage-ment to bolster providers’ services.
Univera Health Care, an ExcellusCompany, in New York State, Health-Partners, in Minnesota, and RockyMountain HMO in Colorado, are verydifferent kinds of plans, yet all threeare committed to proactive disease man-agement. Univera originated as a staff-model HMO using employed physicians,merged with another plan and is nowpart of Blue Cross Blue Shield, cover-ing most of New York State, outside ofthe city. HealthPartners, both a healthplan and a health care delivery sys-tem, includes the HealthPartners MedicalGroup and Clinics, a set of clinics thatserves between one-quarter and one-thirdof the population of the health plan’s660,000 enrollees. Rocky Mountain HMOis an independent, non-profit IPA-model
health maintenance organization that wasfounded by physicians in 1974.
All three plans have employed theChronic Care Model to support care oftheir patients and enrollees, all with sig-nificant results.
Univera Focus:CONGESTIVE HEART FAILURE
Univera’s initial foray into dis-ease management using theChronic Care Model began in
1999 with congestive heart failure, a con-dition that is responsible for a significantportion of overall health care costs in theU.S. According to Peggy Calogero, R.N.,Manager for Univera’s Chronic IllnessProgram, there are a variety of reasonsfor spiraling costs for congestive heartfailure, including lack of coordination inthe delivery of care and a wide variationin the application of care. “Heart failuredisease management programs have been
23
H E A L T H P L A N S ’ P I V O T A L R O L E I N C H R O N I C
I L L N E S S I M P R O V E M E N T
Univera Health CareAN EXCELLUS COMPANYNEW YORK
HealthPartnersMedical GroupMINNESOTA
Rocky Mountain HMOCOLORADO
Connecting the
•ORGANIZATION
OF HEALTH CARE
•DELIVERY
SYSTEMDESIGN
•DECISIONSUPPORT
•CLINICAL
INFORMATIONSYSTEMS
•PATIENT
SELF-MANAGEMENT

shown to improve the quality of caredelivered to patients by coordinating andfocusing an effective managementapproach which results in improvedpatient outcomes and decreased hospitaladmissions,” Calogero explained. “Thatinevitably leads to lower costs.”
Using the Chronic Care Model,Univera’s approach boils down to this:Shifting the focus of care away from cri-sis management to prevention by:
• Concentrating on patients’ self manage-ment of their conditions
• Making sure appropriate levels of med-ications are prescribed
• Providing critical nutritional counseling
• Ensuring consistent contact with ahealth care professional.
Calogero admits that these are not thetypes of services providers are used togetting from health plans. “You have to
be very gentle when you’re working withthe doctors,” she acknowledged.
To minimize the built-in tensionbetween the plan and the providers,Univera’s program was strictly volun-tary, requiring consent both from theproviders and the patients. “It’s not arequired service for all members withheart failure,” Calogero noted. Univera’sapproach was built around two strate-gies, the first a series of eight care callsto patients, the second, a comprehensivecase management program, with a one-on-one relationship between a Univeranurse case manager and a patient, andinvolving their physicians.
PATIENT IN THE DRIVER’S SEATThe development of two sepa-rate approaches evolved fromclose consultation with the staff
at Improving Chronic Illness Care. “Theyreally helped us realize that it’s the personwith the condition that’s in the driver’s
seat. You can educate till you’re blue in theface, but if the patient is not ready to takesteps, it doesn’t work,” Calogero related.
After trying out a couple of differentways to identify patients for the program,Univera settled on targeting their mem-bers who had been hospitalized for heartfailure along with accepting referralsfrom clinicians or patients themselves.“We have had very positive feedbackfrom doctors and patients because it’sanother set of eyes and ears reinforcingtheir self-management,” Calogero added.
The Care Calls Program is tailored tothe individual, so, for example, if a patientis knowledgeable about their heart med-ications, but needs to learn more aboutmanaging their diet or incorporatingexercise, the nurse will spend more timeon that. “The service is delivered over thephone. For some people, that anonymityis a good thing. It’s really been very wellreceived,” Calogero said.
Univera worked with private practicephysicians in advisory teams to developguidelines for the case management pro-gram, beginning with congestive heartfailure, and later incorporating diabetes,asthma and depression. Each teamapproves all the materials Univera useswith patients and sees the outcomes mea-sures and reporting.
Case managers have a wide range ofresponsibilities including:
• Maintaining the database and reportingoutcomes
• Providing telephonic follow up using anassessment tool
• Adjusting medications over the tele-phone using protocols approved by theHeart Failure Team, as long as they havestanding authorization from the physician
• Communicating with physicians using astandard form
• Organizing patient education activitiesthrough home care or teaching sessions
• Monitoring and encouraging diet andmedication compliance
24
For the 12 months prior to instituting the congestive heart failure disease managementprogram, 33 out of the 81 continuously enrolled members were hospitalized. For the 12months after the program was instituted, hospitalizations declined to 12 members.
Sigma level = 3 N = 32/81
CHF AdmissionsHospitalizations Before/After Enrollment
0.5
0.4
0.3
0.2
0.1
0
-Q4 -Q2 -Q1 Q1 Q2 Q3 Q4
ME
AN
NU
MB
ER
OF
HO
SP
ITA
LIZ
AT
ION
S
-Q3

• Assisting with identifying barriers andchallenges and helping patients plan cop-ing strategies.
By the time Univera completed theChronic Disease Collaborative with theInstitute of Healthcare Improvement andImproving Chronic Illness Care, therewere around 100 patients participating inthe program and a reduction in hospitaladmission rates for heart failure. “Evenwith the increase in pharmacy costs, sav-ings in hospitalization alone still createdoverall savings,” Calogero said.
The impact of the program and itspromise for the future is undeniable. In1997, Univera provided care to 729 con-gestive heart failure patients requiringapproximately $10 million in medicalexpenses, $1.3 million of which were forcongestive heart failure related services.With membership growth in the plan’ssenior population, Univera anticipatesthat the number of over-65 congestive
heart failure patients will double, requir-ing approximately $2.4 million in con-gestive heart failure-related expenses.The medical literature suggests that casemanagement, applied in these popu-lations can produce 30% savings oninpatient expenses, which could conserv-atively represent $400,000 for Univera.
Arthur Orlick, M.D., Univera’s Med-ical Director during the Collaborative,believes that even if the program is costneutral, it offers great value. “It’s whathealth plans should be doing, instead ofmanaging cost, managing care,” he said.
With a firm understanding of theChronic Care Model and the one-yearexperience with the Collaborative underits belt, Univera was able to develop dis-ease management programs for diabetes,asthma and depression. “When you’ve
done it once, it transfers fairly easily toother disease states, as long as you havethe right indicators,” said Dr. Orlick.
HealthPartners Focus:DIABETES AND HEART DISEASEThe HealthPartners Medical Group, withmore than 570 physicians practicing inover 31 primary clinics, including morethan 35 medical and surgical special-ties, has a long, rich history of qualityimprovement innovations.
The HealthPartners Medical Groupbegan working on the diabetes collabo-rative in 1998, focusing on the medicalclinics. Recognizing that heart diseaseoften occurs along with diabetes andthat it can develop with little or nowarning, HealthPartners Medical Group
25
“Even with
the increase
in pharmacy
costs, savings in
hospitalization
alone still
created overall
savings.”
GOAL 1999 RATE 2000 RATE
HbA1c (Blood Glucose) Screening 87.6% 91.6%during the reporting year
HbA1c less than or equal to 8% 58.1% 67.2%
LDL Screening 72.6% 75.5%
LDL (Cholesterol) less than 130 44.6% 51.4%
Blood Pressure Control (less than 130/85) 32.5% 37.4%
Aspirin Use (for those 40 and above) 38.4% 44.5%
Tobacco Assessment 82% 83%
Tobacco Advice 33.2% 49.4%
*The results are based upon an annual chart audit of more than 1,400 patients
JANUARY — DECEMBER 20007,000 PATIENTS
HealthPartners Medical GroupTracking Indicators*

incorporated appropriate managementof cardiovascular disease risk factorsinto their measures. So in addition to themanagement of blood sugar levels andthe range of preventive diabetes checks,the HealthPartners Medical Group addedin blood pressure control, lipid manage-ment, controlling LDL (the bad choles-terol), use of aspirin, and reduction insmoking to their outcomes measures.
ADVANCING THE USE OFDATA THROUGH INFORMATIONTECHNOLOGY
The HealthPartners MedicalGroup relied on its InformationSystems (IS) and Health Services
Analysis and Reporting Team to developa registry of diabetes patients. “In 1998,we started providing a list of registrypatients to providers that identified theirpatients with diabetes and stratified theirrisk based on available lab values andother diagnostic codes,” explained TerryCrowson, M.D., HealthPartners MedicalDirector for Disease Management. “Thisbecame a tool for clinicians to managetheir patients with diabetes.”
Dr. Crowson said this population-based approach makes sure that the high-est priority patients are visible to theprovider team so that appropriate carecan be delivered.
DECISION-MAKING SUPPORT:A ROADMAP FOR CARE TEAMSAND PATIENTS
The next building block is mak-ing sure physicians have accessto the latest guidelines. Health-
Partners Medical Group had played a sub-stantial role in helping to develop commu-nity-based practice guidelines, taking intoaccount national recommendations, scien-tific evidence and local practitioner input.They provided the medical groups witheducation, distributed the guidelines, pro-vided ongoing continuing medical educa-tion and implemented a program calledStaged Diabetes Management. Dr. Crowsondescribed the program as decision-making
support for care teams, developed by theInternational Diabetes Center in Minne-apolis. “It’s like a roadmap for care teamsand patients to follow,” he said.
EMPOWERING PATIENTS INSELF-MANAGEMENT
When it comes to gettingpatients involved in their owncare, the HealthPartners Medical
Group’s one- stop-shopping model offersan ideal platform. “The medical group hasan American Diabetes Association-recog-nized diabetes education program. We’vegot the educational support. Each clinichas a designated diabetes resource nursespending time with patients on self-man-agement,” Crowson explained. “The med-ical group has a structure to make surepatients are getting access to programs.Registered dietitians are available andinvolved, offering classes, or one-on-onevisits as necessary. Educators and coun-selors help patients understand what theyneed to do daily on meal planning. Wehave on-site mental health professionals
who participate in diabetes classes and/orindividual counseling.”
HealthPartners also designed handywallet cards to help patients track resultsand remind them of the kinds of thingsthey should be doing for their care. Thecard lists everything from targeted bloodglucose range, goals and dates for bloodglucose checks, weight checks, blood pres-sure readings, cholesterol checks, annualfoot, urine, eye and dental exams, flu andpneumonia shots. It lists the key indicatorspatients should track, such as daily footchecks, avoidance of tobacco and mainte-nance of a low-fat diet. It even lists ques-tions to ask the health care team andoffers a chart for tracking medications.The card includes the number to a phoneline, which offers health experts trainedto support and teach patients. “Our healthplan offers this phone-based healthcounseling to all members, and the med-ical group has fully utilized this service,”said Jan Wuorenma, R.N., B.S.N., SeniorDirector for Disease Management. “Theprogram offers health counseling on stressmanagement, healthy eating, increasedphysical activity, all the lifestyle manage-ment options that patients can use tobring their diabetes under control.”
RE-ORGANIZING HEALTH CARE“Our leadership is committed toquality improvement,” addedWuorenma. “Everybody is tar-
geted and focused on the same thing.When we pay attention, things improve.”
At the health plan level, Health-Partners has decided to align outcomesand income. “The organization sets tar-gets for care improvement for medicalgroups and if they hit their targets, there’sa substantial financial reward,” explainedDr. Crowson.
Because of the commitment to quality,HealthPartners is now managing heartdisease using the Chronic Care Model andis evaluating its use for depression. “Wehave 13,000 patients with coronary arterydisease, and between 3,000 and 4,000with congestive heart failure. We’ve seen
26
“If there’s
anyone who
will slip
through the
cracks, it’s
someone with
depression.”

a decrease in hospital and emergencyadmissions in the population with con-gestive heart failure over the last threeyears,” said Dr. Crowson.
Rocky MountainHMO Focus:DEPRESSION
“Chronic illness takes a lot ofmoney out of the coffers anddecreases quality of life for peo-
ple,” said Lori Stephenson, Director ofQuality Improvement for Rocky MountainHMO. “As a health plan, we are commit-ted to significant chronic disease man-agement.”
With quality medical care a primaryobjective, the pieces were in place tolaunch an innovative quality improve-ment project on depression. Stephensonsaid their team chose to focus on depres-sion because it often accompanies otherchronic illnesses. “We like to screen every-one we have in our diabetes or asthmaprograms for depression. If you get thedepression treated, it may be easier, forexample, to bring blood sugar under con-trol in patients with diabetes,” she said.
Dr. Gregg Omura, of Rocky MountainHMO’s depression team, said using theChronic Care Model improved care in anumber of ways. First, it provided thebasis for a training program for physi-cians and nurses, increasing their com-fort in working with depression. Second,it encouraged use of patient educationhandouts, a critical component in caringfor patients with depression. Third, “ifthere’s anyone who will slip through thecracks of the health care system, it’ssomeone with depression. By using aregistry of all patients with depression,we can monitor improvement in careand identify patients who are notresponding well or who are missingappointments. We can then make phonecontact and encourage them to continuetreatment,” added Dr. Omura.
“The majority of our patients don’t
know they’re depressed. Eight to ninepercent of the population is being treatedfor depression. The real number is doublethat,” Dr. Omura explained. “A lot ofpatients out there have fatigue or backpain that’s actually caused by depression.If you treat depression, maybe their backpain or their heart palpitations will goaway or get better.”
Dr. Omura said his team uses PHQ-9,a depression assessment tool that includesthe nine most common symptoms ofdepression. The tool is quick and simpleto administer. It is used at every visit andprovides the physician with an objec-tive measure of the patient’s progress. Dr.Omura’s team showed over a 50 percentimprovement among patients identifiedwith depression at 12 weeks and ulti-mately a much higher improvement atsix months.
The key to success with this approachis motivated clinical staff, according toboth Stephenson and Dr. Omura. “It’simportant to collaborate with physicianswho are eager to work with this. Oncethose physicians enjoy success, theybecome champions with other physi-cians,” Stephenson said.
With 16 physicians and more than450 patients in the depression registry,Rocky Mountain HMO hopes soon tohave strong clinical outcome data tomake a persuasive business case for clin-ics to add case managers.
RE-ORGANIZING HEALTH CAREDr. Omura employs three full-time nurses and says his prac-tice approach revolves around a
care team, one of the key Chronic CareModel elements. And his practice is morecost effective than it’s ever been. One ofthe more encouraging indicators: his reg-istry of depressed patients is decreasing.“After nine months to a year, you’re ter-minating treatment as much as you’repicking it up. If patients are doing well, wediscontinue all interventions with instruc-tions to be cautious if symptoms return.”
With six months of experience discon-tinuing treatment, so far Dr. Omura’spatients have not experienced recurrentdepression. “We’re catching it earlier and atthis point, we may have tapped into mostpeople in the practice with depression.”
Rocky Mountain HMO is convincedthat approaching chronic disease in thissystematic way will save money overtime. But Stephenson acknowledged thatit’s an investment for the long haul.“When you think about chronic illnesscare, programs that take care of peoplewhen they are the sickest cost the mostmoney,” she noted. “Rather than spend-ing all your resources when the popula-tion is in crisis, proactively treating thechronically ill when their symptoms canbe better managed will keep peoplehealthier and save resources over time,”according to Stephenson. •
27
GOAL RATE OF SUCCESS
50% reduction in depression symptoms at 12 weeks 52%
Making contact with the patient by phone or in a follow-up visit 32%within two weeks of initiating treatment
Use of antidepressant medications for a minimum of six months 98%
AUGUST 2000 – OCTOBER 2001684 PATIENTS
Rocky Mountain HMO’sTracking Indicators

First, The ProblemAlan Graber, M.D., Professor ofMedicine, Division of Endocrin-ology, Vanderbilt Medical Center
identified the problem. After develop-ing and analyzing a patient database,he realized that a significant populationof patients with diabetes at VanderbiltMedical Center wasn’t being managedproperly. Dr. Graber had developed a 12-week Diabetes Improvement Programdesigned for patients newly diagnosedwith diabetes, or patients whose diseaseprocess was out of control. At Vanderbilt,as elsewhere, most patients with diabeteswere cared for by primary care physi-cians and endocrinologists. But the right
patients weren’t getting referred to theprogram, while some of the patients whowere being referred really didn’t needspecialty care.
Enter into the equation, Doris Quinn,Ph.D., Director of Improvement Educationand Measurement, part of Vanderbilt’sCenter for Clinical Improvement. The goalwas to discover a way to get the primarycare physicians to reflect on their ownpopulation of patients with diabetes.“Without data, individual patients cometo a physician who opens the chart andmay see the blood sugar is up. But thatdoesn’t tell the clinician that out of 200patients with diabetes, 10 are out of con-trol. The clinicians were managing charts,one at a time,” Quinn noted.
28
Vanderbilt Medical CenterNASHVILLE, TENNESSEE
Profile Vanderbilt: Vanderbilt University Medical Center is a 658-bed acute care facility with almost 30,000
annual admissions. With the area’s only Level I Trauma Center, Vanderbilt has 92 specialties with approximately
650,000 visits per year. The primary care practices consist of 25 academic internists who provide care for
approximately 30,000 patients. Around 12 percent of all primary care visits are made for diabetes.
in the Driver’s SeatR E - C O N F I G U R E D R E L A T I O N S H I P SI N A N A C A D E M I C S E T T I N G
PrimaryCare
•DECISIONSUPPORT
•CLINICAL INFORMATIONSYSTEMS
•PATIENTSELF-MANAGEMENT

In January of 1998, Quinn facilitateda meeting of the primary care physicians(PCPs), Dr. Graber and the nurse instruc-tors. They shared Dr. Graber’s data,showing that patients weren’t beingmanaged as well as they could be,acknowledged the difficulty of the PCPs’range of responsibilities and proposedworking together. “As the PCPs talkedthrough their relationship with Endo-crinology, I would draw pictures. Whenwe started, the links between primarycare and Endocrinology were iffy. Some
patients found their way to a good pro-gram, some didn’t. The system for diabet-ic patients was weak. Every meeting wehad, they’d say ‘how do we work togeth-er?’” Quinn explained.
As the meetings progressed, the pic-tures began to change. The visual de-piction of the relationships between thetwo disciplines began with side by sideor parallel boxes. The “ah-ha moment”arrived with the visual image of the PCPsas the dominant box, with Endocrinologysupporting their work.
Creating a New FrameworkAt that point, Dr. Graber offeredto give the primary care physi-cians a report on their panel of
patients, highlighting those whose dia-betes was out of control. The new con-cept was tested with a pilot group of fourprimary care physicians. Eventually all ofVanderbilt’s PCPs would be invited toparticipate.
The group worked through criteriafor referring patients to the DiabetesImprovement Program and agreed whatfeedback the Program would supply tothe referring PCPs.
The goals at first included:
• Creating a shared model of care thatworked for the pilot group of PCPs and anendocrinology practice
• Spreading the model to all PCPs in theAdult Primary Care Center
29
“A physician who
opens the chart may
see the blood sugar
is up. But that doesn’t
tell the clinician that
out of 200 patients
with diabetes, 10 are
out of control.”
Diabetes
ManagementDisease
D I A B E T E S D I S E A S EI M P R O V E M E N T P R O G R A M
Assess
P R I M A R Y C A R E
Diagnose Treat Follow-Up
Criteria forReferral
GenerateData
MonitorData
Process forSupport
Vanderbilt positioned Primary Care as the dominant focus of care for patients with diabetes,with the Department of Endocrinology in a support function.

• Increasing the number of appropriatereferrals to the Diabetes ImprovementProgram and the endocrinologist
• Decreasing the mean Hemoglobin A1C(HbA1c—Blood Glucose) levels of patientsof the participating PCPs
• Improving physician and patient satis-faction.
The timing was right for Dr. Graber toprovide reports to the PCPs, as well as let-ters addressed to their patients over theirsignatures. The PCPs then had the optionof sending the letter or discarding it if itwas inappropriate.
Six months into the pilot project, inJanuary of 1999, the team joined theInstitute of Healthcare Improvement’s
Breakthrough Series Collaborative onChronic Disease and adopted ImprovingChronic Illness Care’s Chronic Care Model.“The Chronic Care Model provided a goodunifying system for us,” Quinn noted. “It’sthe little things that make a difference,like marking the chart and getting patientsto take off their shoes and socks.”
Decision Support:Common Definitions
One of the interesting findingsthat emerged from the meetingsbetween the endocrinologist and
the PCPs was their difference in definitionof “out of control” for a patient with dia-betes. The endocrinologist wanted HbA1c
levels below 7%, while the PCPs werelooking for HbA1c levels below 8%. Areview of current research helped them toidentify common ground. They agreed torefer patients to the outpatient treatmenteducation program if HbA1c levels werehigher than 8% for longer than six monthsand were not responding to action takenby the PCP. The process helped the physi-cians build trust with one another, one ofthe key goals of Vanderbilt’s approach.
Dr. Graber developed a template forthe medical records of each patient withdiabetes, which included a handy pull-down check sheet, providing remindersfor the routine, preventive care for thingslike foot and eye checks.
With the new Model, those patientswho do need a higher level of care arereferred to the 12-week Diabetes Im-provement Program, which is managedby the Department of Endocrinology. Thenurses in the program give instructions,start and stop medications, and adjustinsulin. Patients will share their homeblood sugar readings with the nurse atleast once a week and the nurse in turnlets the patients know if they need toadjust their medications. And one of thebest aspects of the program is that thePCPs never lose touch with their patients.“It’s comprehensive care and it’s all donein one place,” concluded Dr. Graber.
Clinical InformationSystems: ManagingComprehensively
Developing a patient registry, ordatabase, was another key com-ponent in Vanderbilt’s success.
“The whole notion of having a databasewas critical,” said Quinn. “Without data,you don’t know how well you’re doing.”
30
SATISFACTION (%) EXCELLENT VERY GOOD GOOD FAIR/ POOR
Overall health 17.6 58.8 11.8 0
Diabetes care received 82.4 11.8 5.9 0
Information presented 82.4 11.8 5.9 0
Questions answered 82.4 17.6 0 0
Lab test results shared 82.4 11.8 5.9 0
Lab test explained 70.6 5.8 17.6 0
Concern, courtesy 88.2 5.9 5.9 0
Patient
SurveySatisfaction
SATISFACTION SURVEY TO PATIENTS COMPLETINGDIABETES IMPROVEMENT PROGRAM IN JUNE 2000(N = 31)

Once all the patients were gathered inone database, they were able to stratifypatients into three groups, based on theirHbA1c levels. One group was doing fine,one was borderline and sent to DiabetesImprovement Program classes, and thosewho were truly complex, with levelsabove 10%, generally were sent to theendocrinologist.
The Results Are InThe approach was a win from allangles. Both PCP and patientsatisfaction surveys were excel-
lent. The physicians felt like they had thesupport they needed to provide the bestpossible care for their patients and a placeclose by to send their patients for morecomprehensive treatment, should the
need arise. Patients in the improvementprogram expressed satisfaction becausethey had the tools and the knowledge tomanage their own care.
More than 1,000 patients have com-pleted the Diabetes Improvement Prog-ram at Vanderbilt. The mean HbA1c forpatients going into the program was 9.3%.After three months, the average was 7%.
Dr. Graber thoroughly subscribes tothe PCP-managed approach to diabetescare and views supporting primary careas an appropriate use of an endocrin-ologist’s time, “One endocrinologist,with proper support from nurses anddieticians and a proper organizationalframework can support several PCPs.The endocrinologist doesn’t have to seeall the patients, but can train and super-vise the nurses and just see the selecteddifficult patients in consultation. It’sbetter than trying to compete with aPCP and there aren’t enough endocri-nologists to see all the patients in anyevent.” Dr. Graber said.
“What we’re trying to develop here isa model that could be used in the privatesector,” Dr. Graber added. “The patientscome from the same environment andhave the same type of insurance. We justhappen to have a group of 25-30 PCPson site.”
Quinn and Dr. Graber both acknowl-edge that it’s not always easy to get reim-bursed for providing this kind of care, butbelieve there’s a strong business case tobe made. “We know that it costs a lotmore to care for a diabetic who is not ingood control. A patient who goes to theemergency room and ends up in the hos-pital is a lot more expensive to the systemthan somebody you’ve been managing,where problems can be nipped in the bud.That’s not even mentioning the patients’quality of life,” Quinn explained.
“In a capitated environment, youmight as well shoot yourself in the footif you don’t manage diabetic patients,”Quinn said. “If you’re in fee-for-serviceand you want to grow your practice, youwant to take better care of your patients.With a program like this, we can showhow well our patients are cared for, andthat’s not a bad thing to take to the nego-tiating table with a health plan.”
The overall success of the programmeans other chronic diseases are onthe drawing board at Vanderbilt. “Thismethod would work for any conditionthat requires PCPs and specialists to worktogether, from congestive heart failure tolow back pain,” noted Dr. Graber. •
31
“What we’re trying
to develop here is a
model that could be
used in the private
sector. The patients
come from the same
environment and
have the same type
of insurance.”Patients in Vanderbilt’s Diabetes ImprovementProgram are satisfied because they have theinformation they need to manage their ownhealth conditions and the vast majority ratethe care they receive as excellent.

Marianne LoGerfo, M.S.W.,Director of the Northshore Sen-ior Center in Northeast Seattle,
realized that there was a vacuum ofservices for older adults who were be-coming more frail and needed to bettermanage their health on their own. In1996, Northshore joined forces with twohealth maintenance organizations and theUniversity of Washington and developeda one-year, senior center-based chronicillness self-management and disabilityprevention program. Their project focusedon health, the ability to function, and theutilization of health care services amongfrail older adults.
When the program was evaluated by arandomized controlled study, the resultswere astonishing. The 100 program par-ticipants, age 70 and over, with one ormore chronic conditions, decreased their
hospitalization by 38%, compared to anincrease of 69% in the control populationthat didn’t participate in the program.
“The study results confirmed our beliefthat a program like this could be extremelyeffective,” noted Susan Snyder, M.S., Pro-ject Director for the Senior Wellness Project,Senior Services of Seattle/King County.
Clearly, it was time to extend the pro-gram to additional facilities.
Since the mid-90s, the Senior WellnessProject has evolved and spread to 32 sites inWashington state, four each in California,Maryland and Michigan and two each inMaine and New York, and Sweden. The pro-ject features three main components:
• Health Enhancement Program
• Living a Healthy Life with ChronicConditions Workshop
• Lifetime Fitness Program.
32
People clearly are living longer these days but with the increased incidence of chronic disease, the goal
of the Senior Wellness Project is to make sure that they’re also living better. The brainchild of one of
the senior centers of Senior Services of Seattle/King County, the Senior Wellness Project embodies two
of the Chronic Care Model’s key elements: patient self-management and community resources.
Senior Wellness ProjectSENIOR SERVICES OF SEATTLE/
KING COUNTY, WASHINGTON
ReversingC H R O N I C A L L Y I L L S E N I O R S ’H E A L T H I M P R O V E S I NC O M M U N I T Y P R O G R A M
the Trend
•ORGANIZATIONOF HEALTH CARE
•PATIENTSELF-MANAGEMENT
•COMMUNITYRESOURCES

Health EnhancementProgramThe one-year Health Enhancement Pro-gram, the core of the Senior WellnessProject, is offered in senior centers andpublic housing facilities. Characterizing itas a health behavior change program,Snyder said the key is putting individualsin the driver’s seat and letting themchoose their own goals. That’s a hallmarkof the self-management approach of theChronic Care Model, and it’s one thatoften takes some re-thinking on the partof providers.
But the payoffs can be great.In her four years of experience
staffing the Health Enhancement Pro-gram, Sabina Kane, R.N., Senior WellnessProject Clinical Supervisor, learned tohonor people’s choices. If a participantwas an alcoholic and wanted to workon exercise, she went with that. “OnceI figured out that the issues belonged tothe participants and not to me, I sleptbetter. Moving the power to change theirhealth from me to them was a very goodthing,” she noted.
And an important lesson she learnedwas that if changes don’t happen in peo-ple’s lives, it’s because they don’t own thechanges. Over the course of her work onthe program, Kane learned from partici-pants that they had good reasons formaking the choices they made and thatover time, more progress was made whenher relationship with them developed outof mutual trust and respect.
The Health Enhancement Programbegins with a comprehensive healthscreening to determine actual and poten-tial health risks. The nurse then workswith participants to select areas wherethey want to improve. Patients typicallypick one or two goals and from thosegoals a computerized action plan is devel-oped. The plan outlines participants’baseline scores and details the steps theywant to take to achieve their goals. Theyreceive health assessment questionnairesinitially, at six months and at the end ofthe one-year program.
The nurse is available as support, anda social worker is on call for short-termindividual counseling or to facilitate sup-
port groups. Patient choices generallycenter on physical and social activity,chronic disease self-management, griefand loss, and depression.
“We found that this program is aresource for older adults in the commu-nity and for physicians who may nothave the time to spend with participants.We can supplement what the doctor isdoing by providing additional time to lis-ten to the participants. We help olderadults learn to improve their health andto better manage their health on theirown,” said Snyder.
Social connections, disease self-man-agement and physical health are theHealth Enhancement Program’s threemain areas of focus. That makes thesenior centers and public housing facili-ties ideal venues, since a variety of pro-grams typically are available. “If peopledon’t want to sign up for a group exer-cise class, they can participate in a walk-ing program, or follow an exercise pro-gram on television,” Snyder noted. “Wewant them to learn that there areresources in the centers and in the com-munity that can help them maintain andalso improve their health as they age.”
A special feature of the HealthEnhancement Program is peer healthmentors. Snyder said mentors are olderadults, typically managing their ownchronic conditions, who volunteer to bematched up with participants in theprogram. They provide support and en-
couragement in helping participantsreach their health goals.
Kane pointed out that mentoring canbe good for both parties. She rememberedone participant who had a stroke, walkedwith a cane and was having difficultywith her memory. Her family was close toplacing her in an assisted living facility,but the woman didn’t want to move outof her own home. Then, she joined theHealth Enhancement Program. “Shedecided to attend the Lifetime Fitnessexercise class,” Kane said. “She was sucha magnet that four or five other peoplejoined the exercise program with her.”
The woman ended up impacting notonly her own life, but also those of five orsix other people. Kane said she’s still liv-ing on her own and lends a welcominghand to new people in the group.
Another eventual mentor started theprogram with such an acute anxiety dis-order that he couldn’t even sit still in achair. New to the area, he hooked up witha volunteer mentor and began going toexercise classes. He and his wife bothmade friends in the class. Kane said heblossomed so much that he began men-toring people with memory problems. “Hespoke to a small group of nurses aboutthe value of being a mentor. He’s nowable to go on trips, which he hadn’t beenable to do for years. He attributes that tothe program,” she concluded.
“The Health Enhancement Program isthe most rewarding job I have had in my30-year career,” Kane added.
Living a Healthy Lifewith Chronic ConditionsWorkshop
The Living a Healthy Life withChronic Conditions Workshop,the second component of the
Senior Wellness Project, consists of groupclasses that zero in on self-managementtechniques. Led by trained volunteers,the six-session workshop originated atStanford University’s Patient EducationResearch Center. A program to helpseniors with chronic conditions cope withissues including lifestyle changes, fatigue,medications, communication skills, pain
33
“A lot of older people
are living on their own
with no support system.
The Senior Wellness
Project is a low-cost
complement to a
physician’s practice.”

and depression, the impacts it can haveon participants’ lives can be remarkable.
“When I entered the class, I was onoxygen 24 hours per day,” related pro-gram participant Edna Olsen, a residentof Vashon Island, outside of Seattle. “Ihad started working on managing mycondition, but I didn’t have a well-planned program. The action plans andproblem-solving techniques we learnedin the class really helped.”
One big change for Olsen was learninghow to improve communications with herdoctor. “Before I took the class, when Iwent to visit my doctor, he would sayhow are you, and I would say, fine. I wasso flustered.” Now she goes to doctor vis-its prepared, and their relationship isvastly improved.
One of the keys to the workshops isthat they are always run by two trainedleaders, at least one of whom has achronic disease and isn’t a health profes-sional. The goal is to create an environ-ment in which participants provide sup-port to one another and build confidencein their ability to manage their health andstay active. Subject areas include:
• Ways to handle frustration, fatigue,pain and isolation
• Appropriate exercises for enhancingstrength, flexibility and endurance
• Appropriate use of medications
• Communicating effectively with family,friends and health professionals
• Nutrition
• Evaluating new treatments.
“The Living a Healthy Life withChronic Conditions class built my selfworth. This class gave me the tools notonly to take control of my health but totake control of my life,” added Olsen. Shenow co-leads the Living a Healthy Lifeworkshops herself.
Lifetime Fitness ProgramThe final aspect of the SeniorWellness Project is a tested exer-cise program, which works well
in conjunction with the other two partsof the Project.
For example, the six-week chronicconditions workshop motivated partici-pant Olsen to join The Lifetime FitnessProgram, where she began riding her sta-tionary bicycle and walking two or threetimes a week. Olsen went on to lose 50pounds, bring her blood pressure undercontrol, and no longer need supplementaloxygen. Her life is now filled with socialand community activities.
The Lifetime Fitness Program is an evi-dence-based, low-cost program designedto improve physical conditioning levelsand to decrease the risk of falling.Sessions run for five weeks, three classesper week and offer exercises to improvestrength, balance and range of motion.
Exercise instructors are specificallytrained to work with seniors, and nation-ally recognized senior exercise expertsregularly review the program. It’s designedso that seniors with a wide range ofphysical abilities are able to participate.The program is a partnership betweenSenior Services, Group Health Coopera-tive, and the University of Washington’sHealth Promotion Research Center.
Spreading the SeniorWellness Project
Snyder continues to work withthe physician community tohighlight the Senior Wellness
Project and the three components of theprogram to generate more referrals.“Once physicians have participants inour program, they’re happy. They see theprogram has a positive impact on theirparticipants’ health.”
Obtaining funding for the program hasbeen challenging, and over the yearsSnyder has pursued a variety of grants.The Robert Wood Johnson Foundationand local foundations have been majorfunding partners over the past threeyears. The program now has a strongpartnership with the University of Wash-ington’s Health Promotion ResearchCenter, and its staff is helping them eval-uate the program’s effectiveness. As theSenior Wellness Project sends data to theUniversity, they learn from the physi-cian’s viewpoint what they need to beincorporating to make it a stronger pro-gram in the view of health care providers.The Senior Wellness Project also receiveda grant from the Robert Wood JohnsonFoundation to support evaluation anddissemination of the project. “They feelthat it’s a strong project because of ourinterventions, and they want to know if itworks as well in other populations andsettings,” Snyder said.
In the meantime, thousands of partici-pants have improved their function andtheir outlook on life. “A lot of older peo-ple are living on their own with no sup-port system. The Senior Wellness Projectis a low-cost complement to a physician’spractice,” Snyder pointed out. •
34
The Lifetime Fitness Classes are designedfor older adults with a wide range ofphysical abilities. (photo by Susan Snyder)
“This class gave me
the tools not only to
take control of my
health, but to take
control of my life.”

Web Sites to WatchFEDERAL AGENCIES
National Library of Medicineat the National Institutes ofHealth (NLM) MEDLINEplushttp://www.nlm.nih.gov/medlineplus/
MEDLINEplus brings together, by health topic,authoritative information from NLM, theNational Institutes of Health (NIH), other gov-ernment, non-profit and other health-relatedorganizations. Preformulated MEDLINEsearches are included in MEDLINEplus andgive easy access to the medical research liter-ature. It also provides a database of full-textdrug information and an illustrated medicalencyclopedia.
National Center for ChronicDisease Prevention and HealthPromotion at the Centers forDisease Controlhttp://www.cdc.gov/nccdphp/index.htm
The CDC web site contains information aboutchronic diseases and conditions, lists of publi-cations from the National Institutes of Healthand links to other sources of health informa-tion, health and education agencies, majorvoluntary associations, the private sector andother federal agencies.
In a field as dynamic as that of chronic illness care, any written
resource guide faces the threat of obsolescence almost as soon as
it is published. In the entries below we have included some of the
seminal published works in chronic illness care and a few of the
key web sites to watch as the field evolves. Web sites included
range from Federal agencies active in this area to groups with a
commitment to chronic illness improvement, and sites oriented to
the patient. As the field evolves and the publications and useful
web sites grow, we will continue to provide updated information
on the web site for Improving Chronic Illness Care:
http://www.improvingchroniccare.org
HOW TO USE THE ICIC WEB SITE
Improving Chronic Illness Care’s web site is designed to help health care professionals
improve care for patients with chronic illness. It provides an in-depth model of health
system change that re-orients practice to chronic illness management within the current
acute care setting. There are quality improvement resources to accelerate this system
change and practical clinical tools for managing multiple chronic illness populations.
To get started, go to the link above and click on first-time user.
35
Resources andSuggested Reading

GROUPS COMMITTED TOQUALITY IMPROVEMENTIN HEALTH CARE
Picker Institutehttp://www.picker.org/
Although designed primarily for professionalhealth care providers, Picker’s web site offersinsightful ideas for quality care that areequally useful to consumers. Check out Newvisions: ideas worth sharing.
Institute for HealthcareImprovementhttp://www.ihi.org
The Institute for Healthcare Improvement (IHI)is a not-for-profit organization created to helplead the improvement of health care systems.Their web site features their public events,such as health care forums and educationalofferings, collaborative improvement efforts,and redesigning the health care system.
Health Disparities Collaborativeshttp://www.healthdisparities.net
The Health Disparity Collaboratives are aneffort of the Health Resources ServicesAdministration to reduce disparities in healthoutcomes for poor, minority, and other under-served people. The web site includes informa-tion about current collaboratives, assistancefor clinicians and senior leaders, as well aslinks to sites for patients. As of December2001, the Health Disparity Collaboratives havereached over 300 community health centersand 38,000 patients.
PATIENT INFORMATION
Johns Hopkins Library,Evaluating information onthe internethttp://www.library.jhu.edu/elp/useit/evaluate/index.html
This site contains a tutorial on evaluatinginformation on the internet. It covers author-ship, bias, propaganda, misinformation, dis-information, verifiability, and currency ofmaterial.
National Institutes of Health,Health Informationhttp://www.nih.gov/health/
The NIH page contains health information,research opportunities, drug information,health literature, links to other governmentagencies and information on special pro-grams, such as minority health and alterna-tive and complementary medicine.
InfoNet http://infonet.welch.jhu.edu/advocacy.html
InfoNet from Johns Hopkins MedicalInstitutions offers an extensive list of advoca-cy and self-help organizations. It includesdirect links to many advocacy and informa-tion groups, such as the American CancerSociety, American Heart Association,American Diabetes Association and others.
Internet Resources for HealthEducation and Health Promotionhttp://www.gwumc.edu/library/Hpdp.htm
This site contains a selected bibliography ofInternet resources on health education andpromotion. It was compiled by the GeorgeWashington University Medical Center.
National Guideline Clearinghousehttp://www.ahcpr.gov/1-800-359-9295 (Publication Clearinghouse)
Consumer information on specific health con-ditions, surgery, prescriptions, heath plansand other health care issues. From main page,click on “consumer health.”
healthfinder®http://www.healthfinder.gov/
healthfinder® is a free guide to reliable con-sumer health and human services informa-tion, developed by the U.S. Department ofHealth and Human Services. healthfinder®can lead you to selected online publications,clearinghouses, databases, web sites, andsupport and self-help groups, as well asgovernment agencies and not-for-profitorganizations that produce reliableinformation for the public.
36

Published Literature
Calkins E, Boult C, Wagner EH,Pacala JT, editors. New ways to carefor older people: building systemsbased on evidence. New York, NewYork: Springer Publishing Company,Inc., 1998.
This book describes innovations in care of theelderly, including programs for prevention,health promotion, and frail elders. Chaptersinclude application of the Chronic Care Modelto elder care, the role of the older person inmanaging illness, caring for older persons inboth acute and long-term settings and inte-gration of care across settings, as well as carefor the dying. Quality assurance in health careand Medicare and changes in health systeminfrastructure are also addressed.
Clark NM, Gong M. Managementof chronic disease by practitionersand patients: are we teaching thewrong things? BMJ. 2000 Feb26;320(7234):572-5.
Using asthma as an example, Clark and Gongdescribe the quality of education that under-lies bridging the gap between research andpractice in managing chronic illnesses. Theauthors depict the quality of partnershipbetween patient and physician that is neces-sary for disease control, discuss the self-regu-lation model that has successfully changedpatient behavior and outcomes, and suggesttechniques providers can employ to establishsuch partnerships.
Committee on Quality of HealthCare in America: Institute ofMedicine. Crossing the QualityChasm: A New Health System forthe 21st Century. Washington, DC:National Academy Press, 2001.
This report from the Institute of Medicinefocuses on how the health care delivery sys-tem can be redesigned to improve care. Itoffers a new perspective on the purpose andaims of health care systems and describeshow patients and their clinicians shouldrelate, and how care processes can bedesigned to optimize responsiveness topatient needs. It offers principles and guid-ance for redesign that represent fundamentalchanges in the way the system meets theneeds of people it serves, focusing not onlyon health care organizations, but the envi-ronment in which these organizations func-tion. It proposes six aims for improvement tooccur that address key dimensions in whichtoday’s health care system functions at farlower levels that it can. Health care should besafe, effective, patient-centered, timely, effi-cient, and equitable. Finally, it makes a seriesof recommendations regarding optimal care.
Langley GJ, Nolan KM, NolanTW, Norman CL, Provost LP. TheImprovement Guide: A PracticalApproach to EnhancingOrganizational Performance.San Francisco: Jossey-BassPublishers, 1996.
This book describes the Model forImprovement that has been the basis forquality improvement in the BreakthroughSeries Collaboratives. It illustrates the funda-mental questions for achieving improvementin a variety of settings and outlines skills tosupport improvement. These skills includeusing data for improvement, developing andtesting change concepts, implementingchange and working with others to make thechange system-wide. It contains case studiesas examples of improvement efforts, andguidance for both implementers and leadersin establishing an environment conducive tobuilding a culture of improvement.
Lorig KR, Sobel DS, Stewart AL,Brown BW Jr, Bandura A, Ritter P,Gonzalez VM, Laurent DD, andHolman HR. Evidence suggestingthat a chronic disease self-manage-ment program can improve healthstatus while reducing hospitaliza-tion: a randomized trial. Med Care.1999 Jan; 37(1):5-14.
This is the definitive randomized controlledtrial of a lay-led self-management programdesigned for a heterogeneous group of chron-ic disease patients. Participants who receivedthe six-week intervention, when comparedwith wait list controls, showed improvementin health behaviors such as frequency of exer-cise and improved communication withphysicians, as well as improved health statusand reduced hospitalization.
37

Renders CM, Valk GD, GriffenSJ, Wagner EH, van Eijk JT, andAssendelft WJJ. Interventionsto Improve the Management ofDiabetes in Primary Care, Outpatientand Community Settings. DiabetesCare. 2001 Oct; 24(10):1821-33.
This review summarizes effective interven-tions in office practice for patients with dia-betes. Interventions were characterized astargeted at health professionals, reorganiza-tion of care, or patient education. Findingsindicated that postgraduate education com-bined with organizational strategies thatincrease structured recall arrangements forfollow-up improves the process of diabetescare. The addition of patient education or amore enhanced role of the nurse were criticalaspects of programs that improved patientoutcomes.
Rich MW. Heart failure diseasemanagement: a critical review. JCard Fail. 1999 Mar; 5(1):64-75.
Heart failure hospitalization rates remainhigh despite effective pharmacotherapy. Thisarticle reviews the literature on multidiscipli-nary disease management programs toimprove the psychosocial, behavioral andfinancial factors that impede effective com-pliance with prescribed treatment. There isconvincing evidence that such programs areeffective in reducing hospital admissions anddays, improving quality of life, functionalcapacity and patient satisfaction, as well asenhancing patient knowledge and adherencewith medications and diet. Limited cost dataalso suggest that such programs are highlycost-effective and in some cases cost-saving.
Wagner EH, Austin BT, and VonKorff M. Organizing care forpatients with chronic illness. MilQuarterly 1996; 74(4): 511-544.
This article was the genesis for the develop-ment of the chronic care model. It discussesthe differences between the acute care-ori-ented health care system and the needs ofpeople with chronic conditions and offers ananalysis of the system components thatunderlie good chronic care.
Wagner EH, Glasgow RE, Davis C,Bonomi AE, Provost L, McCulloch D,Carver P, Sixta C. Quality improve-ment in chronic illness care: A col-laborative approach. Joint CommisJ Qual Improve 2001; 27: 63-80.
This article describes the first Chronic IllnessBreakthrough Series Collaborative includingthe Chronic Care Model, the Model forImprovement, and the results received fromthe first collaborative. It gives examples ofthe most common and especially innovativechanges attempted by the participatinghealth care teams and reports on successesand challenges they experienced in trying todeliver truly patient-centered, evidence-based care.
38

The Changing Face ofChronic Disease Care
Ed Wagner, M.D., M.P.H, F.A.C.P.Director
Connie Davis, M.N., A.R.N.P.Associate Director for Clinical Improvement
Center for Health StudiesMacColl Institute for Healthcare InnovationImproving Chronic Illness Care1730 Minor Avenue, Suite MPE-1600Seattle, WA 98101-1448PHONE 206-287-2704FAX 206-287-2138EMAIL [email protected]
It’s a Team SportDelivering Unified Chronic IllnessCare in Rural Communities
Ann LewisExecutive Director
CareSouth Carolina, Inc.P.O. Box 1090Hartsville, SC 29551PHONE 843-857-0111FAX 843-857-0150EMAIL [email protected]
Monette SutphinOperations Officer
Hilton C. Ray, M.D.Medical Director
High Plains Community Health Center201 Kendall DriveLamar, CO 81052PHONE 719-336-0261 FAX 719-336-0265EMAIL [email protected]
Engaging the PatientsPrivate Practice Re-defined
Colette Rush, R.N., B.S.N., C.C.M.Coordinator of Disease Management Programs
The Polyclinic1145 BroadwaySeattle, WA 98122PHONE 206-860-5416 FAX 206-860-4432 EMAIL [email protected]
Marc Cordova, M.D.
The Polyclinic1145 BroadwaySeattle, WA 98122PHONE 206-329-1760 FAX 206-325-6910 EMAIL [email protected]
Natalie Roberts, D.O.
935 West Point Drive, Suite 103Wasilla, AK 99654PHONE 907-373-4135FAX 907-373-0205
Rivaling Private CareCommunity Health Centers Meetthe Needs of the Urban Poor
Genevieve Mack, M.S.N., P.N.P.Director, Project AIR
Hill Health Center428 Columbus AvenueNew Haven, CT 06519PHONE 203-503-3030FAX 203-503-3183EMAIL [email protected]
Cory Sevin, R.N., M.S.N.Vice President
Clinica Campesina1345 Plaza Court NorthLafayette, CO 80026 PHONE 303-665-3192, ext 212 FAX 303-665-4459EMAIL [email protected]
Full Court PressAn Integrated System TacklesChronic Illness Care
Evan Steffens, R.N., M.S.Director of Clinical and Quality Systems
Primary Care Networks ofPremier Health Partners40 West Fourth Street, Suite 1700Dayton, OH 45402PHONE 937-208-8215FAX 933-208-8201EMAIL [email protected]
Connecting the DotsHealth Plans’ Pivotal Role in ChronicIllness Improvement
Kathleen CurtinVice President Quality ManagementAdministration
Peggy D. CalogeroSenior Manager Quality ManagementAdministration, Western New York
Univera HealthCare205 Park Club LaneBuffalo, NY 14221PHONE 716-857-6204 OR 716-857-6214FAX 716-857-6355EMAIL [email protected] [email protected]
Jan Wuorenma, R.N., B.S.N.Sr. Director, Disease Management
HealthPartners, Inc.8100 34th Avenue South, P.O. Box 1309Minneapolis, MN 55440-1309PHONE 952-883-7176FAX 952-883-7399EMAIL [email protected]
Lori Stephenson, R.N.Director of Quality Improvement
Rocky Mountain HMO2775 Crossroads Blvd, P.O. Box 10600Grand Junction, CO 81502PHONE 970-248-5124FAX 970-244-7880EMAIL [email protected]
Primary Care in theDriver’s SeatRe-configured Relationshipsin an Academic Setting
Doris Quinn, Ph.D.Director of Improvement Educationand Measurement
Center for Clinical ImprovementVanderbilt University Medical CenterA1220 MCN 21st Avenue SouthNashville, TN 37232-2668PHONE 615-343-6393FAX 615-343-3398EMAIL [email protected]
Reversing the TrendChronically Ill Seniors’ HealthImproves in Community Program
Susan Snyder, M.S.Director, Senior Wellness Project
Senior Services of Seattle/King County1601 Second Avenue, Suite 800Seattle, WA 98101PHONE 206-727-6297FAX 206-448-5766EMAIL [email protected]
FOR ADDIT IONAL INFORMATION ON THE QUALITY IMPROVEMENT PROJECTS
PROFILED IN THIS REPORT PLEASE CONTACT:

The National Coalition on Health Care1200 G Street NW, Suite 750Washington, DC 20005
PHONE 202-638-7151FAX 202-638-7166
EMAIL [email protected] www.nchc.org
The Institute for Healthcare Improvement375 Longwood Avenue, Fourth FloorBoston, MA 02215
PHONE 617-754-4800FAX 617-754-4848
EMAIL [email protected] www.ihi.org
Improving Chronic Illness Care1730 Minor Avenue, Suite MPE-1600Seattle, WA 98101-1448
PHONE 206-287-2704FAX 206-287-2138
EMAIL [email protected] www.improvingchroniccare.org