Embed Size (px)
Citation preview

© 2003 Nature Publishing Group
Most people who die of cancer succumb to metastatictumours. Some of the most common tumour types,such as small-cell lung, ovarian, breast and stomachcancer, respond to chemotherapy, but the impact onsurvival is small or unproven1. Even when patients dorespond to chemotherapy, in most cases they relapsewith drug-resistant disease and few survive for morethan 5 years (TABLE 1). The tumours that can be curedwith chemotherapy are relatively rare, such as child-hood cancers, leukaemias, lymphomas and testiculargerm-cell tumours. Understanding the reason thatthese tumours are curable with chemotherapy couldlead to the development of more effective treatmentfor the estimated 6.2 million people who die of cancereach year, worldwide2.
Drug resistance has been studied extensively, andmany of the ways in which cancer cells can circumventthe cytotoxic influences of a drug are now understood.But the reasons that some cancers are successfully eradi-cated by drugs has not been studied in such detail, and itis not known whether the various types of cancer thatare curable all have the same underlying mechanisms ofdrug responsiveness. One of the greatest successes ofcancer chemotherapy is the introduction of cisplatin tothe treatment of testicular germ-cell tumours (TGCTs).Cisplatin-based combination chemotherapy cures morethan 80% of men with metastatic TGCTs. Cisplatin isbelieved to kill cancer cells by binding to and damagingDNA, leading to cell death. But what is the molecularbasis for the exquisite sensitivity of TGCTs to cisplatin,and how could it be applied to other types of cancer?
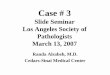
TGCTs occur mainly in young men, with a peakincidence between the ages of 15 and 34, and are themost frequently diagnosed cancers in this age group3.TGCTs develop from the germ cells, which give rise tothe sperm. There are two histopathological types ofTGCT — seminomas and non-seminomas (FIG. 1).About 20% of TGCTs contain a mixture of semino-mas and non-seminomas, indicating a common cellof origin.
Seminomas are homogenous, and consist of sheetsof cells with a clear cytoplasm. By contrast, non-semi-nomas are much more interesting in their appearance.In some classifications they are called ‘teratomas’,which is derived from the Greek word for ‘monster’.Because non-seminomas contain embryonal carci-noma cells, they have similarities to embryonic stemcells, and are capable of differentiating into virtuallyany tissue (FIG. 1). Consequently, they provide a modelof human embryonic development, despite the ‘mon-ster’ appearance. Studies of TGCTs led to theoriesconcerning the role of stem cells in normal develop-ment and cancer, and the concept of differentiationtherapy as an alternative to chemotherapy4,5.
TGCT therapyA series of clinical investigations called ‘staging’ are usedto estimate how far the cancer has spread. The extent ofthe spread dictates the treatment. In general, if a cancer isconfined to the site of origin (stage 1) it can be cured withsurgery or radiotherapy, but if it has spread, systemictreatment such as chemotherapy is needed.
CURING METASTATIC CANCER:LESSONS FROM TESTICULAR GERM-CELL TUMOURSJohn R.W. Masters* and Beate Köberle‡
Most metastatic cancers are fatal. More than 80% of patients with metastatic testicular germ-celltumours (TGCTs), however, can be cured using cisplatin-based combination chemotherapy. Whyare TGCTs more sensitive to chemotherapeutics than most other tumour types? Answers to thisquestion could lead to new treatments for metastatic cancers.
NATURE REVIEWS | CANCER VOLUME 3 | JULY 2003 | 517
*The Prostate CancerResearch Centre,Institute of Urology,University College London,3rd Floor,67 Riding House Street,London W1W 7EJ, UK.‡University of PittsburghCancer Institute,Hillman Cancer Center,Research Pavilion Suite263/2.1, 5117 Center Avenue, Pittsburgh,Pennsylvania 15213-1863,USA.e-mails: [email protected];[email protected]:10.1038/nrc1120
R E V I E W S

© 2003 Nature Publishing Group518 | JULY 2003 | VOLUME 3 www.nature.com/reviews/cancer
R E V I E W S
etoposide has increased response rates and reducedtoxicity. Further improvements have resulted frommore aggressive and better scheduling of chemother-apy, coupled with salvage surgery. Today, more than80% of men with metastatic TGCTs are cured8.
Most men with metastatic TGCTs can now expect anormal lifespan after they survive to 5 years. Most peoplewith other types of metastatic cancer, even if they arelucky enough to survive 5 years, will eventually succumbto the disease.
Why are metastatic TGCTs curable?So, are testis tumours curable because the cancer cellsare more sensitive to anticancer drugs, or is the hostresponse involved? To determine whether testis tumourcells are more sensitive to DNA-damaging agents thanother types of cancer cell, researchers have appliedchemotherapeutic drugs to cultured cancer cells andtested their response. Many studies have shown thattestis tumour cells are approximately 2–4-fold moresensitive (comparing the concentrations that arerequired to kill 50% of the cells) than other types ofcancer cells to various chemotherapeutic drugs9–12 orirradiation13. These findings indicate that the effect ofchemotherapy is not mediated by a host reaction, but isdue to a direct response of the testis tumour cells toDNA-damaging agents.
Do TGCT cell lines represent actual tumours? Whenmost types of cancer cell are selected for drug resistancein vitro, there can be a 1,000-fold or greater difference insensitivity between the parental cells and the resistantcells. So, can the 2–4-fold greater sensitivity of TGCTcells to cisplatin really make the difference between cureand failure in the clinic? There is no direct way toanswer this question, but it is possible to compare dataobtained in the laboratory with clinical observations.
One study compared the response of TGCT andbladder cancer cell lines to cisplatin10. Bladder cancercells were chosen for comparison because, like TGCT,cisplatin is the most active single agent used to treatthese tumours. But the response of bladder cancer tochemotherapy is usually of short duration (6–12months) and metastatic disease is rarely cured. Thestudy showed that five TGCT cell lines were more sen-sitive to cisplatin than five bladder cancer cell lines10.The dose responses of the TGCT and bladder cancercell lines can be extrapolated to 1012 cells, which isequivalent to a very large tumour in a patient —about 1 kg. The dose of cisplatin that is required to kill1012 testis cancer cells would only kill between 103 and104 bladder cancer cells. So, if the many assumptionsthat are used to make this extrapolation are correct,this relatively small difference in sensitivity is enoughto explain the difference between cure and failure.Although this dose is theoretically sufficient to eradi-cate TGCTs, and a bladder cancer might initiallyrespond to this therapy, the large number of survivingcells would allow the bladder cancer to continuegrowing, with fatal results. These studies also indicatethat despite the quality control problems associated
Men with TGCTs are treated with surgery, radio-therapy or chemotherapy — alone or in combination— depending on the stage of the disease3 (TABLE 2).Most TGCTs are restricted to the testis (stage 1) atdiagnosis, and can therefore be cured surgically. Stage1 seminomas are also treated with radiotherapy tothe para-aortic lymph nodes, which reduces the rateof relapse. Depending on the number and size oflymph nodes invaded, men with stage 2 non-semi-noma are treated with surgery and chemotherapy, orwith chemotherapy alone, whereas men with stage 2seminoma are treated with surgery and radiotherapy,or with chemotherapy alone. The standard treatmentfor men with more advanced disease (stage 3) of bothtypes is chemotherapy.
In 1970, 95% of men with metastatic TGCTs died oftheir disease. However, even before 1970 it was knownthat TGCTs were sensitive to a number of single agentsthat kill cells by damaging DNA, such as dactinomycin,vinblastine and bleomycin. A total of 25% of men whowere treated with bleomycin plus vinblastine achievedlong-term disease-free survival6. But the big break-through came in the mid-1970s with the introductionof cisplatin, which, in combination with vinblastineand bleomycin, cured more than half of the mentreated7. Since then, the replacement of vinblastine with
Summary
• Metastatic testicular germ-cell tumours (TGCTs), in contrast to nearly all other cancersin adults, can be cured with drugs (cisplatin-based combination chemotherapy).But why are metastatic TGCTs so curable?
• TGCT cells grown in the laboratory are 2–4 times more sensitive to cisplatin than mostother types of cancer cell, so they provide a representative model system with which tostudy the mechanisms that control cisplatin sensitivity.
• Testis tumour cells are deficient in one particular type of DNA repair — nucleotideexcision repair — and consequently have a reduced capacity to repair the DNAdamage caused by cisplatin.
• Testis tumour cells are also defective in other aspects of DNA repair and are primedfor apoptosis.
• Targeting DNA-repair proteins might sensitize other types of cancer to cisplatin.
Table 1 | Metastatic cancer survival rate
Cancer type 5-year survival rate
Pancreatic cancer 1.6%
Lung cancer 1.7%
Bladder cancer 5.9%
Colorectal cancer 6.9%
Cervical cancer 8.6%
Kidney cancer 9.2%
Melanoma 15.9%
Breast cancer 19.8%
Ovarian cancer 23.3%
Endometrial cancer 26.1%
Prostate cancer 29.8%
Adapted from REF. 77.

© 2003 Nature Publishing GroupNATURE REVIEWS | CANCER VOLUME 3 | JULY 2003 | 519
R E V I E W S
It is not known whether this greater sensitivity is asso-ciated with the difficulty of maintaining these cells in vitro. During the development of sperm from thegerm cells, there are changes in the sensitivity of thecells to drugs, so it is possible that seminomas andnon-seminomas are derived from cells at differentstages of germ-cell differentiation. Another interestingobservation is that when residual TGCTs remain afterchemotherapy, in about one-third of cases the tumourconsists of mature teratoma — a more differentiatedtumour type. More differentiated TGCT cells aretherefore more resistant to chemotherapy.
Do TGCT cells have a lower mutation frequency? Onepossible explanation for the sensitivity of TGCTs to cis-platin is that they have a reduced capacity to developdrug resistance. Tumours can become resistant to ther-apy by acquiring mutations in a variety of biochemicalpathways that enable the cells to circumvent the toxiceffects of the drugs. So, do TGCTs have a lower frequencyof mutations than other types of cancer?
The mutation frequencies of three bladder cancerand three TGCT cell lines were compared followingexposure to ethyl methanesulphonate (a potentmutagen) and cisplatin17. No difference was observedbetween either the spontaneous (no treatment) orthe induced frequency of mutations in the bladderand testis cancer cells. For example, in three bladderlines, the spontaneous mutation rate ranged from 2.3to 18.7 mutants per 106 cells. In three testis tumourlines, the mutation rate ranged from 6.2 to 8.2mutants per 106 cells17. So, testis tumour cells shouldbe able to develop drug resistance as readily as othertypes of cancer cell. But, compared with most othertypes of cancer, TGCTs rarely acquire drug resistance,perhaps because they are eradicated by the drugsbefore they have a chance to become resistant. So whyare TGCTs so sensitive to chemotherapeutics — tocisplatin, in particular?
Factors that influence chemosensitivityChemotherapeutic agents such as cisplatin kill cellsby damaging DNA. Four general processes determinethe sensitivity of cells to these types of chemothera-peutic agents (BOX 1). These include the transport ofthe drug across the cell membrane (into and out ofthe cytoplasm), drug activation and detoxification,the accessibility of the drug to DNA (BOX 2) and thecell’s response to the DNA damage. A number ofstudies have been performed to compare the effi-ciency of these processes between TGCTs and othercancer cell types.
When cancer cells become resistant to drugs, theytend to either disrupt one of these general mechanismsof chemosensitivity or modify the target in some way— often by mutation or gene amplification. However,it should not be assumed that because a tumourresponds to a drug by one mechanism, that the samemechanism will be altered during acquisition ofdrug resistance. Cancer cells modify any biochemical pathway that is at their disposal to avoid the cytotoxic
with cell lines14,15, many TGCT cell lines are sensitive tocisplatin and other drugs, providing a model systemthat can be used to study the mechanisms of TGCTdrug responsiveness. This is the reason that manystudies in this field are performed on TGCT cell lines.
One remarkable thing about TGCT cell lines is thatthey are almost all derived from non-seminomas. It hasbeen difficult to establish continuously growing celllines from seminomas — these cells tend to die in cul-ture16. Seminomas, however, are even more sensitive toradiotherapy and chemotherapy than non-seminomas.
Germ cell
Seminoma
Embryonal carcinoma
Extra-embryonic tissue
Embryonic tissue
Trophoblast Yolk sac
Carcinoma in situ
Ectoderm Mesoderm Endoderm
Choriocarcinoma Yolk-sac carcinoma
Teratoma
Non-seminoma
Combined tumour
Figure 1 | Theoretical histogenesis of testicular germ-celltumours. The origin of germ-cell tumours is a controversialsubject. There are two types of germ-cell tumours —seminomas and non-seminomas — which have differentappearances under the microscope. About 20% of TGCTs arecombined tumours that contain both seminoma and non-seminoma cells. It is generally thought that combined tumoursare derived from the same germ cell. During the development ofa germ-cell tumour, it is believed that the cells pass through acarcinoma in situ stage before differentiating into a seminoma ora non-seminoma. Non-seminomas can consist ofundifferentiated embryonal carcinoma cells, or can be a mixtureof undifferentiated and partially differentiated cells, or can, in rareinstances, consist of mature differentiated tissue. The embryonalcarcinoma cells can go through the various pathways ofdifferentiation to produce embryonic and extra-embryonictissues. The embryonic tissues can include primitive ectoderm,mesoderm and endoderm. On rare occassions, fullydifferentiated mature teratomas can arise from these tissues(sometimes the only tissue remaining after chemotherapy). Non-seminomas can also contain extra-embryonic tissues, such aschoriocarcinoma (trophoblastic cells) and yolk-sac cells.

© 2003 Nature Publishing Group520 | JULY 2003 | VOLUME 3 www.nature.com/reviews/cancer
R E V I E W S
were detected in testis, bladder20 and colon cancercells21. These studies indicate that thiols are not likely tobe solely responsible for the sensitivity of testis cancercells to cisplatin.
Drug binding to DNA. The level of drug binding toDNA provides one means of distinguishing a cell’sresponse to DNA damage from the other processesthat control drug sensitivity (BOX 1). For example, ifdifferences in TGCT drug sensitivity can be accountedfor by one of the three early steps of drug activity(drug uptake or efflux, drug metabolism or drugbinding to DNA), then more cisplatin should bebound to the DNA of testis cancer cells than to DNAof other types of cancer cell. Studies show, however,that following exposure to cisplatin, there is a widerange in the number of cisplatin-DNA adducts mea-sured in different cancer cell types, and TGCT cells fallwithin this range11,19,22–24. These are key observations,because they indicate that the sensitivity of testis cancer cells must therefore lie downstream of DNAbinding — in the DNA-damage-response pathway —rather than in any of the upstream events that regulatethe access of cisplatin to DNA.
DNA-damage responseFour aspects of the response of testis tumour cells to cis-platin-induced DNA damage have been studied. Theseare the stress response, p53 activity, apoptosis inductionand DNA-repair efficacy.
The stress response. The stress response involves activation of heat-shock proteins (HSPs), which canprotect cells after exposure to chemotherapeuticdrugs. Overexpression of the stress-response proteinHSP27 in testis cancer cells caused a small increase inresistance to cisplatin25. However, measurement of thelevels of heat-shock proteins in TGCT cells, comparedwith bladder26 or colon cancer cells27, did not revealany consistent differences.
p53 expression. TGCTs have been shown in somestudies to express high levels of p53, and mutations inthis protein are rare in untreated TGCTs. p53 canactivate an apoptotic response in response to DNAdamage, and is an important factor in mediating
effects of chemotherapy. This review therefore focuseson the mechanisms that determine sensitivity ofTGCTs to cisplatin, rather than on the acquisition ofcisplatin resistance.
Transport across the cell membraneLittle is known about the mechanism by which cis-platin enters cells, although a recent study points tothe involvement of a copper transporter18. Comparisonof cisplatin accumulation in testis, colon19 and bladdercancer cell lines revealed no consistent differencesbetween cell types. These findings indicate that mem-brane transport is not the key factor that controls cisplatin sensitivity in testis tumour cells.
Drug activation and detoxificationResistance to cisplatin is frequently associated withchanges in the cellular levels of THIOL-containing com-pounds, such as glutathione. A comparison of threeTGCT (cisplatin-sensitive) and three colon cancer celllines (relatively insensitive to cisplatin) indicated thatmany factors are involved in the differential sensitivitybetween the two tumour types, including levels of thedetoxifying compound glutathione19. A comparison ofTGCT (cisplatin-sensitive) and bladder cancer cell lines(relatively insensitive to cisplatin) found that mean lev-els of glutathione were lower in the TGCT cells. Therewas not an association, however, between cisplatin sen-sitivity and levels of glutathione-S-transferase — theenzyme that catalyses the addition of glutathione tosubstrates during detoxification19,20 in cell lines or inclinical samples20. Metallothionein is an enzyme thatdetoxifies heavy metals, so low intracellular levels ofthis protein might also be associated with sensitivity tocisplatin. However, similar levels of metallothionein
THIOLS
Compounds that contain -SH as the principal group directlyattached to carbon, such asglutathione. Glutathione is themain endogenous antioxidantproduced by the cell. Itparticipates in the neutralizationof free radicals, reactive oxygencompounds, and maintainsexogenous antioxidants such asvitamins C and E in theirreduced (active) forms. Inaddition, through directconjugation by glutathione-S-transferase, glutathionedetoxifies many compounds.
Table 2 | Different stages of TGCTs
Stage Characterisitics 5-year survival rate
Stage 1 Within testicle >95%
Stage 2 Spread to local (pelvic or abdominal lymph nodes) >95%
Stage 3 Spread to distant lymph nodes in chest or higher, 74%very high levels of tumour markers, or spread to distant organs (such as lung)
Overall, more than 90% of newly diagnosed TGCTs are cured. Data provided by the AmericanCancer Society web site (http://www.cancer.org).
Box 1 | Factors that determine sensitivity to chemotherapeutic drugs
There are four general mechanisms that influence thecell’s response to chemotherapeutic drug agents. Thefirst is drug influx and efflux — drugs enter and leave thecell by various mechanisms through the plasmamembrane. They then can be metabolized — eitheractivated or detoxified within the cytoplasm.Accessibility of the DNA to the drug can also influencedrug efficacy. Finally, the response of the cell to DNAdamage will determine its fate. There are also many otherfactors that operate outside the cell that can alsoinfluence whether a cancer will respond to therapy, suchas route of administration and pharmacokinetics.
Accessibilityof DNA to drug
Cytoplasm
Nucleus
DNA
Drug activationand detoxification
Cell response toDNA damage
Drug influxand efflux
Cell membrane

© 2003 Nature Publishing GroupNATURE REVIEWS | CANCER VOLUME 3 | JULY 2003 | 521
R E V I E W S
59% of the drug-responsive tumours, compared with83% of the non-responsive tumours. These observationsindicate that the sensitivity of TGCTs to chemotherapy isnot determined by p53 levels.
These studies, however, only measured p53 levels,and not p53 function. It is possible that TP53 muta-tions33 or other alterations in the p53 pathway, suchas disruption of MDM2 function, could cause TGCTto become drug resistant. One study provided evi-dence in support of this hypothesis. Four of 23 cancerbiopsies from men who had relapsed following therapy were found to contain TP53 mutations33.Another study, however, showed that whereas TP53mutations were detected in only 1 of 17 TGCTs thatresponded to chemotherapy, there were no TP53mutations detected in the 18 TGCTs that were resistantto chemotherapy32.
In vitro studies were also performed in cell lineswith known p53 defects. In a comparison of 18human cell lines derived from various tumour typesthat express wild-type TP53 with 39 cancer cell linesthat contained TP53 mutations, the mutant lineswere found to be significantly more resistant to cis-platin, bleomycin and 5-fluorouracil than the wild-type lines34. In fact, the mutant lines tended to bemore resistant to most drugs, but were equally sensi-tive to some of the drugs that are commonly used totreat TGCT, including the antimitotic agents (such asvincristine, vinblastine and paclitaxel)34.
A cell line derived from a TGCT that had failedchemotherapy and also contained a p53 mutation wasfound to be relatively resistant to cisplatin33. By contrast,comparison of two TGCT cell lines — one with func-tional p53 and one without — revealed no differences indrug sensitivity35. Partial inactivation of p53 activity(using HPV16-E6) in a cisplatin-sensitive TGCT cellline did not make the cells resistant to cisplatin, whereasa cisplatin-resistant cell line was found to express func-tional p53 (REF. 32). Therefore, whereas p53 could medi-ate resistance of some TGCT to chemotherapy, it is notthe whole story.
Part of the confusion about the role of p53 in thesensitivity of TGCT to chemotherapy might be due tothe use of short-term assays of apoptosis such as DNAcleavage assays36. These assays might not provide anaccurate reflection of the proportion of cells that sur-vive for the long term after drug treatment36. Forexample, in a mouse model of TGCT, tumour cells thatexpressed wild-type p53 underwent rapid apoptosis inresponse to cisplatin treatment. By contrast, Trp53-null tumour cells did not undergo apoptosis, butinstead underwent cell-cycle arrest with concomitantupregulation of p21 (REF. 37). However, when the cis-platin responses of the wild-type Trp53 and Trp53-nullTGCT cells were compared using CLONOGENIC ASSAYS,which provide a valid indication of the proportion ofcells that survive treatment, no significant difference insensitivity to cisplatin was observed37.
It has also been suggested that some of the disparitiesconcerning the role of p53 in the sensitivity of TGCTs tochemotherapy could be due to the partial reliance on
chemotherapy-induced cell death28,29. So, do p53 levels determine the sensitivity of TGCTs tochemotherapy drugs30,31?
About two-thirds of TGCTs contain cells that expressp53, as determined by immunohistochemistry, but mostof these tumours contain fewer than 30% p53-positivenuclei32. The same study compared p53 expression inclinical samples from 17 chemotherapy-responsiveTGCTs and 18 unresponsive TGCTs. p53 was detected in
CLONOGENIC ASSAY
Measures the proportion ofsingle cells that are able to formcolonies (minimum of 32 cells).It is used to estimate survivaland dose response to drugtreatment.
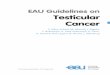
Box 2 | Cisplatin interactions with DNA
Cisplatin (Pt) is believed to kill cells through its interactions with DNA. The drug isgiven to patients intravenously in saline (sodium chloride solution) and enters thecells by either passive diffusion or facilitated uptake through an as yet unidentifiedpump. Once inside the cytoplasm, cisplatin undergoes hydrolysis. The chlorideligands are each replaced by a molecule of water, producing a positively chargedmolecule (the water molecules can also lose a proton to form various aquatedspecies). Hydrolysis occurs preferentially within cells, because cells have a muchlower concentration of chloride ions than the bloodstream.
Once hydrolysis has taken place, cisplatin can attach to DNA. Many types ofcisplatin–DNA complexes or adducts can be formed, which include intrastrandadducts. The most frequently observed adducts are intrastrand links between adjacentguanines (65%) or links between adenine and guanine (25%). Cisplatin can also stretchacross a base to join two guanines (GXG) on the same strand of DNA. The adductscause the DNA structure to become distorted, and can activate DNA-repairmechanisms. Cisplatin can also join bases across the two DNA strands (interstrandadducts). Although these are relatively infrequent (about 1% of adducts), they arethought to be highly cytotoxic. Cisplatin can also form monoadducts — in which onlyone of the active arms is joined to DNA and can also produce links between DNA andprotein — or adducts with other molecules such as glutathione or a protein.
H3N H3N
Cl Cl
Pt
Pt
H3N H3N
OH H20
Pt DNA
GG
Pt
GGX
Intrastrand adducts
Pt
G
PtG
GPt
PtG
G
Other types of adduct
Protein
Glutathione
(About 65%) (About 25%) (Rest of intrastrand adducts)
Monoadduct Intermolecular adductInterstrand adduct (<1%)
Pt
G A

© 2003 Nature Publishing Group522 | JULY 2003 | VOLUME 3 www.nature.com/reviews/cancer
R E V I E W S
However, NER (BOX 3) is the main mechanism bywhich cisplatin-induced damage is removed fromDNA in mammalian cells. NER can be subdivided intotranscription-coupled and global genome NER. Onerecent study has shown that the activity of transcrip-tion-coupled, but not global genome, NER is requiredfor cisplatin sensitivity in human cells50.
The first studies of DNA repair in testis tumour cellswere limited by available technologies. Repair of cis-platin-induced DNA damage in testis and bladder can-cer cells was originally compared using ATOMIC ABSORPTION
SPECTROSCOPY (which measures all cisplatin adducts),ALKALINE ELUTION (which measures interstrand crosslinks)and immunoassays (which measure various intrastrandadducts). These experiments indicated that followingtreatment with cisplatin, bladder cancer cells were ableto repair most or all of the DNA damage. By contrast,testis tumour cells removed little or none of the DNAdamage. So, it seems that TGCT cells have a reducedcapacity for NER51,52.
However, these assays measure DNA repairthroughout the genome, and as only about 2% of theDNA is actual coding sequence, much of this repaircould be irrelevant. Quantitative polymerase chainreaction (PCR) assays were eventually developed tomeasure repair within individual genes. In these assays,the amount of PCR product is inversely proportional tothe amount of DNA damage caused by cisplatin. Thistype of analysis showed that testis tumour cells retainDNA damage for a longer time interval than bladdercancer cells, and therefore have a reduced capacity forNER — not only in the whole genome, but also at thelevel of individual genes23,53. The reduced DNA-repaircapacity of TGCTs could underlie the sensitivity ofDNA-damaging drugs such as cisplatin.
But what aspect of NER is compromised in testistumour cells? NER is a complex process that involvesDNA-damage recognition, local unwinding of DNA,excision of the damaged region and, finally, repair of thedamaged region (BOX 3). Research into the relationbetween NER and the sensitivity of testis tumour cells tocisplatin has focused on two areas — DNA-damagerecognition and levels of individual NER proteins.
High mobility group (HMG) proteins are a largefamily of proteins that are characterized by twodomains (called HMG boxes) that facilitate their inter-action with DNA54. HMG proteins recognize DNAthat has been damaged by cisplatin55 and block repairof cisplatin-DNA adducts56,57.
Testicular cells express many tissue-specific HMG-domain proteins, including SRY (sex-determining fac-tor) and testis-specific HMG-domain protein (tsHMG— a nuclear isoform of the mitochondrial transcriptionfactor mtTFA). Both of these bind to cisplatin-damagedDNA with high affinity58,59. So, is the ability of tsHMGto block NER sufficient to mediate sensitivity to cis-platin60? The tsHMG gene was transfected into HeLacells (a cervical cancer cell line) under the control of aninducible promoter. Following exposure to cisplatin, thepercentage of apoptotic cells was greater among thetsHMG-expressing cells than the control cells at some
data from mouse models of TGCT32. In some respects,mice do not provide a fully representative model of human TGCT, due to differences in p53 expressionlevels, the absence of seminomatous components,the timing of cancer development and the diploid chromosomal constitution of the mouse tumours32.
What conclusions can be drawn concerning p53 andthe sensitivity of TGCTs to chemotherapy? High levelsof p53 expression could make the DNA of TGCTs moreaccessible for nucleotide excision repair (NER) or primethese cells for apoptosis. The hypothesis that overex-pression of wild-type p53 underlies the sensitivity ofTGCT to chemotherapy is attractive, simple and mightexplain their general sensitivity to almost all DNA-dam-aging agents. But the premise that TGCTs uniformlyoverexpress p53 is not correct32.
Apoptosis. If p53 is not responsible for TGCT sensitivityto cisplatin, could upregulation of one or more of themany proteins in the apoptotic pathways be responsible?Germ cells — the progenitors of sperm and TGCTs —are particularly susceptible to apoptosis38. Presumably, theapoptotic elimination of a high fraction of potentialsperm is the result of a quality control mechanism that isdesigned to reduce the risk of passing on genetic defectsto offspring. These cells could therefore be primed toundergo apoptosis, explaining the sensitivity of testistumour cells to cisplatin.
Testis tumour cells express high levels of the pro-apop-totic protein BAX, and low levels of the anti-apoptoticprotein BCL2 (REF. 39). However, when BCL2 was overex-pressed in TGCT cells, there was a reciprocal downregula-tion of another pro-apoptotic protein, BCL-X
L, resulting
in increased sensitivity to chemotherapeutic drugs40.Cisplatin resistance has been shown to be mediated by afailure to activate caspase-9 in a cisplatin-resistant TGCTcell line41.A number of proteins involved in regulation ofapoptosis (p53, BAX, BCL2 and BCL-X
L) and other path-
ways potentially involved in sensitivity to cisplatin wereexamined in a series of clinical samples from chemother-apy-resistant and -sensitive TGCTs, but no single factorseemed to be correlated with treatment response42.
The hypothesis that TGCTs are curable because anapoptotic pathway is upregulated is also attractive, sim-ple and might explain the general sensitivity to anti-cancer agents. However, the studies published on thismatter so far have yielded contradictory results.
DNA repair. Because cisplatin is a DNA-damagingagent, the ability of a cell to survive exposure coulddepend on the efficacy of its DNA-repair pathways —unrepaired DNA would lead to cell death. Correlationsbetween activation of mismatch-repair mecha-nisms43–45, recombinational repair mechanisms46,47 andcellular responses to cisplatin have been reported.Expression levels of DNA polymerases that can bypasssome cisplatin-induced DNA adducts could also beinvolved in mediating cisplatin sensitivity48. Human APendonuclease — a base excision repair enzyme — isexpressed at high levels in TGCTs, and overexpressionin a TGCT cell line caused resistance to bleomycin49.
ATOMIC ABSORPTION
SPECTROSCOPY
This technique uses lightabsorption to measure theconcentration of atoms in gasphase (usually followingvaporization of a solid or liquidin a furnace).
ALKALINE ELUTION
This technique measures the rateof DNA elution through a filtermembrane under alkalineconditions. The amount of DNAsingle-strand breaks (or otherlesions converted to single-strand breaks) is estimated onthe basis of the increase in therate of DNA elution.

© 2003 Nature Publishing GroupNATURE REVIEWS | CANCER VOLUME 3 | JULY 2003 | 523
R E V I E W S
time points. However, the survival of tsHMG-expressingHeLa cells in long-term clonogenic assays followingexposure to cisplatin was similar to that of thecontrols60. The results were difficult to explain, but it ispossible that the testis-specific expression of tsHMGcould explain the sensitivity of TGCTs to cisplatin60.
Levels of the NER proteins XPA, ERCC1 and XPFwere compared in six TGCT cell lines and 28 cell linesderived from a range of human cancers. The testistumour cells contain very low levels of theERCC1–XPF complex and of the XPA protein, and afew of the other cell lines also expressed either low lev-els of XPA or of ERCC1–XPF (B. K., unpublishedobservations). No immunohistochemical staining forXPA was observed in seminomas61. A reduced capacityfor NER in two TGCT cell lines was confirmed using in vitro assays, which measured the ability of cellextracts to repair an engineered cisplatin-DNA adduct62.Using a similar assay, it was shown that both mouse andhuman TGCT cells are deficient in the repair of a 1,2-d(GpG) cisplatin adduct, although not of a 1,3-d(GpG)adduct60. When XPA and ERCC1–XPF proteins wereadded to the testis tumour cell extracts, NER capacitywas restored to normal levels62. So, ERCC1–XPF andXPA are likely to be key determinants of cisplatin sensi-tivity in TGCTs. Further experiments are required todetermine whether overexpression of these proteinsconfers cisplatin resistance to TGCT cells.
But these cells could also be defective in other DNA-repair pathways that influence cisplatin sensitivity. Thegene encoding ligase III, which is involved in base excisionrepair through its interaction with the DNA-repairenzyme XRCC1, is alternatively spliced in the testis, elimi-nating its XRCC1-interacting exon63. The main damage-specific DNA polymerase of the XP variant group — polη — is also alternatively spliced in the testis, eliminatingthe exon that contains the ATG start codon64. It has there-fore been suggested that germ cells are ‘triple mutants’that lack significant functions of the main pathwaysinvolved in error-free processing of DNA damage64.
Future directionsThere could be one single mechanism, such as a defect inNER, that underlies the susceptibility of TGCTs to cis-platin. However, TGCTs respond to a wide range ofDNA-damaging agents that have different mechanisms ofaction. Therefore, it is more likely that a combination offactors interact to make TGCT a curable cancer.
The sensitivity of TGCTs to chemotherapy is associ-ated with defects in the DNA-repair machinery of thesecells, so it could be possible to sensitize other types ofcancer cells to chemotherapy by targeting DNA-repairmechanisms. Cells derived from people with xerodermapigmentosum — a disease associated with mutations inNER genes67 — can be hypersensitive to DNA-damag-ing agents such as cisplatin and ultraviolet (UV) light.Conversely, cells that overexpress ERCC1 (REFS 69–71) orXPA72,73 can be more resistant to DNA-damagingagents. So, disruption of NER activity in cancer cellsmight make them more sensitive to cisplatin and otherchemotherapeutic drugs.
Box 3 | Nucleotide excision repair
Nucleotide excision repair (NER) is the main mechanism by which cisplatin-induceddamage (red circle) is removed from DNA in mammalian cells. The recognition andincision step of the NER reaction requires the XPC–HR23B complex, XPA, RPA, TFIIH,XPG and the ERCC1–XPF complex. XPC–R23 binds to DNA, altering its structure andallowing other repair factors access. XPA, RPA and TFIIH next attach to the distortedDNA. The DNA is locally unwound by the helicase activities of TFIIH, which includesamong its subunits the DNA helicases XPB and XPD. Incisions are then made on thedamaged strand by nucleases. XPG cuts 3′ to the damage, whereas the ERCC1–XPFcomplex cuts 5′ of the lesion. This results in the release of the lesion within a 24–32-base-long oligonucleotide. The excised DNA is then replaced in a DNA-repair synthesisreaction that is catalysed by DNA polymerase (POL) δor ε holoenzyme with RFC andPCNA. The repair reaction is completed by a DNA ligase that reconnects the repairpatch of DNA to the original strand. Figure and legend adapted from REF. 68.
XPA
TFIIH XPGXPC–HR23B
XPC–HR23B
XPC–HR23B
XPC–HR23B
XPA
TFIIHRPA
XPA
TFIIHRPA
XPG
Distortion recognition and partial opening
Formation of open structure and recognition of damaged strand
Dual incision by structure-specific endonucleases
ERCC1–XPF
ERCC1–XPF
Excision and DNA-repair synthesis
RPA
RFC
PCNA LigasePOL δ/ε
3′
5′
3′
5′
3′
5′
3′
5′
3′
5′
3′
5′
3′
5′
5′
3′
5′
3′
5′
3′
5′
3′
5′
3′
5′
3′
5′
3′
RPA
XPG

© 2003 Nature Publishing Group524 | JULY 2003 | VOLUME 3 www.nature.com/reviews/cancer
R E V I E W S
These observations indicate that ERCC1–XPF andXPA are potential targets for sensitizing human cancer cells to chemotherapy. The downside is thatdrugs that inhibit NER could also sensitize individu-als to other DNA-damaging agents, such as sunlight,or increase the risk of other cancers. So, it will be necessary to find ways to target anti-NER treat-ment to tumour cells and to avoid collateral damageto normal tissues74. For example, drugs that inactivateanother DNA-repair enzyme — ATase — have been shown to damage the bone marrow to theextent that no therapeutic benefit is gained66. In targeting the DNA-repair pathways of cancer cells,there are significant technical problems to over-come — particularly in tumour-specific targeting of these reagents. But it makes sense to try to build on success, as most of the individuals whomight benefit have only a few months to live — 30years ago that was true of most young men withmetastatic TGCTs.
There are a number of drugs and other agents thatare being developed to target the NER pathway75 .Thecell-cycle checkpoint inhibitor UCN-01 increases bind-ing of cisplatin to DNA, reducing the capacity of thecells to repair the damaged DNA. UCN-01 reduces thebinding of ERCC1 to XPA in cell extracts and reducesthe amount of NER incision76. Antisense RNA has alsobeen used to downregulate expression levels of DNA-repair protein. Ovarian cancer cells were sensitized to cisplatin in vitro using ERCC1 antisense RNA.Furthermore, immunocompromised mice thatreceived transplanted cells that expressed antisenseERCC1 survived longer than control mice after expo-sure to cisplatin77. Another approach involved adenovi-ral-vector-induced expression of truncated XPA, whichwas predicted to impair NER and sensitize cells to UVlight and cisplatin73. In a human lung cancer cell line,expression of this dominant-negative form of XPAsequestered ERCC1 and made the cells more sensitiveto UV-light-induced damage and cisplatin73.
1. Souhami, R. & Tobias, J. Cancer and its Management 3rdedn (Blackwell Science, Oxford, 1998).
2. Parkin, D. M., Bray, F., Ferlay, J. & Pisani, P. Estimating theworld cancer burden: Globocan 2000. Int. J. Cancer 94,153–156 (2001).
3. Bosl, G. J. & Motzer, R. J. Testicular germ-cell cancer. N. Engl. J. Med. 337, 242–253 (1997).A clearly written review that summarizes most of theclinical aspects of TGCTs.
4. Pierce, G. B. & Speers, W. C. Tumors as caricatures of theprocess of tissue renewal: prospects for therapy by directingdifferentiation. Cancer Res. 48, 1996–2004 (1988).
5. Sell, S. & Pierce, G. B. Maturation arrest of stem celldifferentiation is a common pathway for the cellular origin ofteratocarcinoma and epithelial cancers. Lab. Invest. 70,6–22 (1994).
6. Samuels, M. L., Lanzotti, V. J., Holoye, P. Y., Boyle, L. E. &Johnson, D. E. Combination chemotherapy in germinal celltumors. Cancer Treat. Rev. 3, 185–204 (1976).
7. Einhorn, L. H. Curing metastatic testicular cancer. Proc. NatlAcad. Sci. USA 99, 4592–4595 (2002).
8. Einhorn, L. H. & Donohue, J. Cis-diamminedicloroplatinum,vinblastine and bleomycin combination chemotherapy indisseminated testicular cancer. Ann. Intern. Med. 87,293–298 (1977).The landmark clinical study that demonstrated thatTGCTs are curable with cisplatin.
9. Oosterhuis, J. W., Andrews, P. W., Knowles, B. B. &Damjanov, I. Effects of cis-platinum on embryonalcarcinoma cell lines in vitro. Int. J. Cancer 34, 133–139(1984).
10. Walker, M. C., Parris, C. N. & Masters, J. R. W. Differentialsensitivities to chemotherapeutic drugs between testicularand bladder cancer cells. J. Natl Cancer Inst. 79, 213–216(1987).
11. Pera, M. F., Friedlos, F., Mills, J. & Roberts, J. J. Inherentsensitivity of cultured human embryonal carcinoma cells toadducts of cis-diamminedichloroplatinum(II) on DNA.Cancer Res. 47, 6810–6813 (1987).
12. Fry, A. M. et al. Relationship between topoisomerase II leveland chemosensitivity in human tumor cell lines. Cancer Res.51, 6592–6595 (1991).
13. Parris, C. N., Arlett, C. F., Lehmann, A. R., Green, M. H. L. &Masters, J. R. W. Differential sensitivities to gamma radiationof human bladder and testicular tumour cell lines. Int. J.Radiat. Biol. 53, 599–608 (1988).
14. Masters, J. R. Human cancer cell lines: fact and fantasy.Nature Rev. Mol. Cell Biol. 1, 233–236 (2000).
15. Masters, J. R. HeLa cells 50 years on: the good, the badand the ugly. Nature Rev. Cancer 2, 315–319 (2002).
16. Olie, R. A. et al. Apoptosis of human seminoma cells upondisruption of their microenvironment. Br. J. Cancer 73,1031–1036 (1996).
17. Parris, C. N., Walker, M. C., Masters, J. R. W. & Arlett, C. F.Inherent sensitivity and induced resistance tochemotherapeutic drugs and irradiation in human cancer
cell lines: relationship to mutation frequencies. Cancer Res.50, 7513–7518 (1990).
18. Ishida, S., Lee, J., Thiele, D. J. & Herskowitz, I. Uptake of theanticancer drug cisplatin mediated by the coppertransporter Ctr1 in yeast and mammals. Proc. Natl Acad.Sci. USA 99, 14298–14302 (2002).
19. Sark, M. W. J. et al. Cellular basis for differential sensitivity tocisplatin in human germ cell tumour and colon carcinomacell lines. Br. J. Cancer 71, 684–690 (1995).
20. Masters, J. R. W. et al. Sensitivity of testis tumour cells tochemotherapeutic drugs: role of detoxifying pathways. Eur.J. Cancer 32A, 1248–1253 (1996).
21. Meijer, C. et al. Role of metallothionein in cisplatinsensitivity of germ-cell tumours. Int. J. Cancer 85,777–781 (2000).
22. Walker, M. C. Inherent Sensitivity and Acquired Resistancein Human Testicular Germ Cell Tumours In Vitro. PhD Thesis,Univ. London (1990).
23. Köberle, B. et al. DNA repair capacity and cisplatin sensitivity ofhuman testis tumour cells. Int. J. Cancer 70, 551–555 (1997).
24. Burger, H., Nooter, K., Boersma, A. W. M., Kortland, C. J. &Stoter, G. Lack of correlation between cisplatin-inducedapoptosis, p53 status and expression of Bcl-2 familyproteins in testicular germ cell tumour cell lines. Int. J.Cancer 73, 592–599 (1997).
25. Richards, E. H., Hickey, E., Weber, L. & Masters, J. R. W.Effects of overexpression of the small heat shock proteinHSP27 on the heat and drug sensitivities of human testistumor cells. Cancer Res. 56, 2446–2451 (1996).
26. Richards, E. H., Hickman, J. A. & Masters, J. R. W. Heatshock protein expression in testis and bladder cancer celllines exhibiting differential sensitivity to heat. Br. J. Cancer72, 620–626 (1995).
27. Hettinga, J. V. E. et al. Heat-shock protein expression incisplatin-sensitive and-resistant human tumor cells. Int. J.Cancer 67, 800–807 (1996).
28. Lowe, S. W., Schmitt, E. M., Smith, S. W., Osborne, B. A.& Jacks, T. p53 is required for radiation-induced apoptosisin mouse thymocytes. Nature 362, 847–849 (1993).
29. Lowe, S. W., Ruley, H. E., Jacks, T. & Housman, D. E. p53-dependent apoptosis modulates the cytotoxicity ofanticancer agents. Cell 74, 957–967 (1993).
30. Lutzker, S. G. & Levine, A. J. A functionally inactive p53 proteinin teratocarcinoma cells is activated by either DNA damage orcellular differentiation. Nature Med. 2, 804–810 (1996).
31. Lutzker, S. G., Mathew, R. & Taller, D. R. A p53 dose-response relationship for sensitivity to DNA damage inisogenic teratocarcinoma cells. Oncogene 20, 2982–2986(2001).
32. Kersemaekers, A. M. F. et al. Role of p53 and MDM2 intreatment response of human germ cell tumors. J. Clin.Oncol. 20, 1551–1561 (2002).A comprehensive analysis of the role of p53 in germ-cell tumours in relation to both cisplatin sensitivityand cisplatin resistance, plus a helpful review of p53expression and some in vitro data.
33. Houldsworth, J. et al. Human male germ cell tumorresistance to cisplatin is linked to TP53 gene mutation.Oncogene 16, 2345–2349 (1998).
34. O’Connor, P. M. et al. Characterization of the p53 tumorsuppressor pathway in cell lines of the National CancerInstitute anticancer drug screen and correlations with thegrowth-inhibitory potency of 123 anticancer agents. CancerRes. 57, 4825–4300 (1997).
35. Burger, A. M. et al. Distinct p53-independent apoptotic celldeath signalling pathways in testicular germ cell tumour celllines. Int. J. Cancer 81, 620–628 (1999).
36. Brown, J. M. & Wouters, B. G. Apoptosis, p53, and tumorcell sensitivity to anticancer agents. Cancer Res. 59,1391–1399 (1999).
37. Zamble, D. B., Jacks, T. & Lippard, S. J. p53-dependentand-independent responses to cisplatin in mouse testicularteratocarcinoma cells. Proc. Natl Acad. Sci. USA 95,6163–6168 (1998).
38. Braun, R. E. Every sperm is sacred — or is it? Nature Genet.18, 202–204 (1998).
39. Chresta, C. M., Masters, J. R. W. & Hickman, J. A.Hypersensitivity of human testicular tumors to etoposide-induced apoptosis is associated with functional p53 anda high Bax:Bcl-2 ratio. Cancer Res. 56, 1834–1841(1996).
40. Arriola, E. L., Rodriguez-Lopez, A. M., Hickman, J. A. &Chresta, C. M. Bcl-2 overexpression results in reciprocaldownregulation of Bcl-XL and sensitizes human testiculargerm cell tumours to chemotherapy-induced apoptosis.Oncogene 18, 1457–1464 (1999).
41. Mueller, T. et al. Failure of activation of caspase-9 induces ahigher threshold for apoptosis and cisplatin resistance intesticular cancer. Cancer Res. 63, 513–521 (2003).
42. Mayer, F. et al. Molecular determinants of treatmentresponse in human germ cell tumors. Clin. Cancer Res. 9,767–773 (2003).
43. Fink, D. et al. The role of DNA mismatch repair in platinumdrug resistance. Cancer Res. 56, 4881–4886 (1996).
44. Mello, J. A., Acharya, S., Fishel, R. & Essigmann, J. M. Themismatch-repair protein hMSH2 binds selectively to DNAadducts of the anticancer drug cisplatin. Chem. Biol. 3,579–589 (1996).
45. Massey, A., Offman, J., Macpherson, P. & Karran, P. DNAmismatch repair and acquired cisplatin resistance in E. coliand human ovarian carcinoma cells. DNA Repair 2, 73–89(2003).
46. Zdraveski, Z. Z., Mello, J. A., Marinus, M. G. & Essigmann, J. M.Multiple pathways of recombination define cellularresponses to cisplatin. Chem. Biol. 7, 39–50 (2000).
47. Takata, M. et al. Chromosome instability and defectiverecombinational repair in knockout mutants of the fiveRad51 paralogs. Mol. Cell. Biol. 21, 2858–2866 (2001).
48. Vaisman, A., Masutani, C., Hanaoka, F. & Chaney, S. G.Efficient translesion replication past oxaliplatin and cisplatinGpG adducts by human DNA polymerase η. Biochemistry39, 4574–4580 (2000).

© 2003 Nature Publishing GroupNATURE REVIEWS | CANCER VOLUME 3 | JULY 2003 | 525
R E V I E W S
49. Robertson, K. A. et al. Altered expression of Ape1/ref-1 ingerm cell tumors and overexpression in NT2 cells confersresistance to bleomycin and radiation. Cancer Res. 61,2220–2225 (2001).
50. Furuta, T. et al. Transcription-coupled nucleotide excisionrepair as a determinant of cisplatin sensitivity of human cells.Cancer Res. 62, 4899–4902 (2002).
51. Bedford, P., Fichtinger-Schepman, A. M., Walker, M. C.,Masters, J. R. W. & Hill, B. T. Differential repair of platinum-DNA adducts in human bladder and testicular tumorcontinuous cell lines. Cancer Res. 48, 3019–3024 (1988).The first indication that NER was defective in TGCTcells.
52. Hill, B. T. et al. Deficient repair of cisplatin-DNA adducts inhuman testicular teratoma cell lines established fromtumours from untreated patients. Eur. J. Cancer 30A,832–837 (1994).
53. Köberle, B., Payne, J., Grimaldi, K., Hartley, J. & Masters, J.R. W. DNA repair in cisplatin-sensitive and resistant humancell lines measured in specific genes by Q-PCR. Biochem.Pharmacol. 52, 1729–1734 (1996).
54. Baxevanis, A. D. & Landsman, D. The HMG-1 box proteinfamily: classification and functional relationships. NucleicAcids Res. 23, 1604–1613 (1995).
55. Ohndorf, U. M., Rould, M. A., He, Q., Pabo, C. O. & Lippard, S. J.Basis for recognition of cisplatin-modified DNA by high-mobility-group proteins. Nature 399, 708–712 (1999).A key study showing the recognition of cisplatin-damaged DNA by high mobility group proteins.
56. Huang, J. C., Zamble, D. B., Reardon, J. T., Lippard, S. J. &Sancar, A. HMG-domain proteins specifically inhibit therepair of the major DNA adduct of the anticancer drugcisplatin by human excision nuclease. Proc. Natl Acad. Sci.USA 91, 10394–10398 (1994).
57. Zamble, D. B., Mu, D., Reardon, J. T., Sancar, A. &Lippard, S. J. Repair of cisplatin-DNA adducts by themammalian excision nuclease. Biochemistry 35,10004–10013 (1996).
58. Ohndorf, U. M., Whitehead, J. P., Raju, N. L. & Lippard, S. J.Binding of tsHMG, a mouse testis-specific HMG-domainprotein, to cisplatin-DNA adducts. Biochemistry 36,14807–14815 (1997).
59. Trimmer, E. E., Zamble, D. B., Lippard, S. J. & Essigmann, J. M.Human testis-determining factor SRY binds to the majoradduct of cisplatin and a putative target sequence withcomparable affinities. Biochemistry 37, 352–362 (1998).
60. Zamble, D. B., Mikata, Y., Eng, C. H., Sandman, K. E. &Lippard, S. J. Testis-specific HMG-domain protein alters theresponses of cells to cisplatin. J. Inorg. Biochem. 91,451–462 (2002).
61. Stoop, H. et al. Reactivity of germ cell maturation stage-specific markers in spermatocytic seminoma: diagnosticand etiological implications. Lab. Invest. 81, 919–928(2001).
62. Köberle, B., Masters, J. R. W., Hartley, J. A. & Wood, R. D.Reduced repair of cisplatin-induced DNA damage intesticular germ cell tumours due to a specific protein defect.Curr. Biol. 9, 273–276 (1999).First unequivocal proof that NER is defective in TGCTs(earlier studies had used assays that requiredsupralethal concentrations of cisplatin).
63. Chew, S. L., Baginsky, L. & Eperon, I. C. An exonic splicingsilencer in the testis-specific DNA ligase III beta exon.Nucleic Acids Res. 28, 402–410 (2000).
64. Cleaver, J. E., Karplus, K., Kashani-Sabet, M. & Limoli, C. L.Nucleotide excision repair ‘a legacy of creativity’. Mutat.Res. 485, 23–36 (2001).
65. Cree, I. A., Knight, L., di Nicolantonio, F., Sharma, S. &Gulliford, T. Chemosensitization of solid tumors bymodulation of resistance mechanisms. Curr. Opin. Invest.Drugs 3, 634–640 (2002).
66. Middleton, M. R. & Margison, G. P. Improvement ofchemotherapy efficacy by inactivation of a DNA-repairpathway. Lancet Oncol. 4, 37–44 (2003).
67. de Boer, J. & Hoeijmakers, J. H. J. Nucleotide excisionrepair and human syndromes. Carcinogenesis 21, 453–460(2000).
68. Friedberg, E. C. How nucleotide excision repair protectsagainst cancer. Nature Rev. Cancer 1, 22–33 (2001).Comprehensive review relating NER defects to cancerpredisposition syndromes.
69. Bramson, J. & Panasci, L. C. Effect of ERCC-1overexpression on sensitivity of Chinese Hamster Ovary cellsto DNA damaging agents. Cancer Res. 53, 3237–3240(1993).
70. Larminat, F. & Bohr, V. A. Role of the human ERCC-1 gene ingene-specific repair of cisplatin-induced DNA damage.Nucleic Acids Res. 22, 3005–3010 (1994).
71. Ferry, K. V., Hamilton, T. C. & Johnson, S. W. Increasednucleotide excision repair in cisplatin-resistant ovariancancer cells. Biochem. Pharmacol. 60, 1305–1313(2000).
72. Cleaver, J. E., Charles, W. C., McDowell, M. L., Sadinski, W. J.& Mitchell, D. L. Overexpression of the XPA repair geneincreases resistance to ultraviolet radiation in human cells byselective repair of DNA damage. Cancer Res. 55,6152–6160 (1995).
73. Rosenberg, E., Taher, M. M., Kuemmerle, N. B., Farnsworth,J. & Valerie, K. A truncated human xerodermapigmentosum complementation group A proteinexpressed from an adenovirus sensitizes human tumorcells to ultraviolet light and cisplatin. Cancer Res. 61,764–770 (2001).
74. Reference deleted in proof.75. Barret, J. M., Cadou, M. & Hill, B. T. Inhibition of nucleotide
excision repair and sensitization of cells to DNA cross-linking anticancer agents by F 11782, a novel fluorinatedepipodophylloid. Biochem. Pharmacol. 63, 251–258(2002).Example of a new drug that targets NER.
76. Jiang, H. & Yang, L. Y. Cell cycle checkpoint abrogatorUCN-01 inhibits DNA repair: association with attenuation ofthe interaction of XPA and ERCC1 nucleotide excision repairproteins. Cancer Res. 59, 4529–4534 (1999).
77. Fact Sheet. Twelve major cancers. Sci. Am. 275, 92–98(1996).
Online links
DATABASESThe following terms in this article are linked online to:Cancer.gov: http://www.cancer.gov/cancer_information/bladder cancer | breast cancer | colon cancer | ovarian cancer |small-cell lung cancer | stomach cancer | testicular cancerLocusLink: http://www.ncbi.nih.gov/LocusLink/AP endonuclease | ATase | BAX | BCL2 | BCL-XL | caspase-9 |ERCC1 | HR23B | HSP27 | MDM2 | p53 | PCNA | RFC | RPA |Trp53 | XPA | XPB | XPC | XPD | XPF | XPG | XRCC1OMIM: http://www.ncbi.nlm.nih.gov/Omim/xeroderma pigmentosum
FURTHER INFORMATIONCancer UK: http://www.cancerhelp.org.ukHuman DNA repair genes:http://www.cgal.icnet.uk/DNA_Repair_Genes.htmlNational Cancer Institute: http://www.nci.nih.gov/cancerinfoAccess to this interactive links box is free online.