Embed Size (px)
Citation preview
O
Cfc
HHa
b
c
d
e
f
a
A
R
R
2
A
A
K
T
G
R
E
F1h
p r i m a r y c a r e d i a b e t e s 7 ( 2 0 1 3 ) 199–206
Contents lists available at ScienceDirect
Primary Care Diabetes
j o u r n a l h o m e p a g e : h t t p : / / w w w . e l s e v i e r . c o m / l o c a t e / p c d
riginal research
ulturally sensitive patient-centred educational programmeor self-management of type 2 diabetes: A randomizedontrolled trial
ashim Mohameda,b,∗, Badriya Al-Lenjawic, Paul Amunad,e, Francis Zotore,isham Elmahdi f
Weill Cornell Medical College - Qatar, QatarFamily Medicine, Primary Health Care Corporation, P.O. Box 7452, Doha, QatarNursing, Hamad Medical Corporation, Doha, QatarInternational Nutrition, Greenwich, United KingdomGreenwich University, Greenwich, United KingdomFamily Medicine, Primary Health Care Corporation, Doha, Qatar
r t i c l e i n f o
rticle history:
eceived 31 October 2012
eceived in revised form
2 April 2013
ccepted 30 May 2013
vailable online 3 July 2013
eywords:
ype 2 diabetes
roup-based diabetes education
andomized controlled trial
ffectiveness
a b s t r a c t
Objective: To assess the effectiveness of a culturally sensitive, structured education pro-
gramme (CSSEP) on biomedical, knowledge, attitude and practice measures among Arabs
with type two diabetes.
Research designs and methods: A total of 430 patients with type II diabetes mellitus living in
Doha, Qatar were enrolled in the study. They were randomized to either intervention (n = 215)
or a control group (n = 215). A baseline and one-year interval levels of biomedical variables
including HbA1C, lipid profile, urine for microalbuminuria; in addition to knowledge, atti-
tude and practice (KAP) scores were prospectively measured. The intervention was based
on theory of empowerment, health belief models and was culturally sensitive in relation to
language (Arabic), food habits and health beliefs. It consisted of four educational sessions
for each group of patients (10–20 patients per session), lasting for 3–4 h. The first session
discussed diabetes pathophysiology and complications; while the second session discussed
healthy life style incorporating the Idaho plate method; and the third session dealt with
exercise benefits and goal setting and the fourth session concentrated enhancing attitude
and practice using counselling techniques. Outcomes were assessed at base line and 12
months after intervention.
Results: After 12 months participation in the intervention was shown to have led to a
statistically significant reduction in HbA1C in the (CSSEP) group (−0.55 mmol/L, P = 0.012),
fasting blood sugar (−0.92 mmol/L, P = 0.022), body mass index (1.70, P = 0.001) and albu-
min/creatinine ratio (−3.09, P < 0.0001) but not in the control group. The intervention group
also had improvement in Diabetes knowledge (5.9%, P < 0.0001), attitude (6.56%, P < 0.0001),
and practice (6.52%, P = 0.0001).
∗ Corresponding author. Tel.: +974 55861008; fax: +974 44661226.E-mail addresses: [email protected] (H. Mohamed), [email protected] (B. Al-Lenjawi), [email protected] (P. Amuna),
[email protected] (F. Zotor), [email protected] (H. Elmahdi).751-9918/$ – see front matter © 2013 Primary Care Diabetes Europe. Published by Elsevier Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.pcd.2013.05.002
200 p r i m a r y c a r e d i a b e t e s 7 ( 2 0 1 3 ) 199–206
Conclusion: This study demonstrates the effectiveness of culturally sensitive, structured,
group-based diabetes education in enhancing biomedical and behavioural outcomes in
Diabetic patients.
ry Ca
© 2013 Prima1. Introduction
The prevalence of diabetes is rapidly increasing worldwide,especially in developing countries, thereby, representing amajor public health burden particularly in growing economies.This results in premature death, disability and reduced qualityof life at an escalating economic cost.
The prevalence of type II diabetes has recently esca-lated in the Arabian Peninsula. For example, Bahrain has anestimated prevalence of 22.1%; Kuwait 12.8%; Oman 16.1%;whilst the highest prevalence rate of 24% has been reportedin Qatar [1–3]. Arabian Gulf countries including Qatar arepart of a group of developing countries witnessing a rapidsocio-economic transition, where cardiovascular disease hasemerged as the leading cause of mortality in adults over thelast 20 years [4]. The high prevalence of Diabetes in Qatar cou-pled with obesity has led to increasing rates of morbidity andmortality due to Congestive Heart failure and Coronary Arterydisease [5].
Effective diabetes education leading to improved self-careactivities among patients can improve metabolic control,quality of life and prevent or delay complications. Currently,no single structured educational programme aimed at manag-ing Diabetes exists in the whole Gulf region, including Qatar.The intention of the present study is to conduct a cultur-ally targeted randomized controlled educational interventionemploying an RCT approach utilizing a structured groupbased educational programme based on empowerment andhealth belief model utilizing counselling techniques. Struc-tured group based education offers a unique opportunity forpatients to interact, be free of stigma; offer each other sup-port and an opportunity to exchange experience, feelings andinstil hope. This is unlikely to happen in a busy Diabetes clinicwhere patients are less likely to be forthcoming and doctorshave competing demands [6] resulting in information beingeither forgotten or ignored by patients.
2. Research design and methods
A total of 430 Arabic speaking adult patients with type IIdiabetes mellitus, attending 22 primary health care centresand hospital Diabetic clinics in Doha, Qatar were enrolledin this randomized controlled trial. Informed consent letterswere sent to all participants inviting them to participate. Thestudy conformed to the principles stated in the declaration ofHelsinki [7].
2.1. The nature and purpose of the study
The study was a multi-stage theory based randomized con-trolled study (see Fig. 1). The model used was based on two
re Diabetes Europe. Published by Elsevier Ltd. All rights reserved.
previous studies in the United Kingdom, one in England [8]and another one in Glasgow, Scotland [9].
2.2. Research protocol and ethical considerations
Approval for this study was granted by Hamad Medical Corpo-ration (HMC) Research Ethics Committee (Research Protocol#412/2006) and The University of Greenwich (U.K.) researchethics committee (UGREC).
2.3. Subject recruitment
2.3.1. Eligibility criteriaSubjects included in the study were Arab adults living in Qatarsuffering from type II diabetes mellitus and registered withprimary health care (PHC) centres and the Main General Hos-pital (HGH). Participants were excluded from the study if theywere diagnosed with Type 1 Diabetes Mellitus or had a docu-mented history of alcoholism or drug abuse.
A total of 800 subjects were enrolled, of these 430 sub-jects gave consent and returned the complete questionnaire,the remaining 370 declined to participate or gave incompleteinformation. The remaining 430 subjects were randomly allo-cated to either intervention or control groups with 215 subjectsin each arm. 109 patients in the intervention group attendedall four sessions. A further 49% drop out was noticed at sixmonths (106 out of 215) in the intervention arm and 16% (34out of 215) in the control group – see Fig. 2 This large drop outof participants was followed up by the main investigator andrespondents gave many reasons for non-attendance. Reasonsfor lack of follow up included: heavy traffic, lack of time on thepart of participants and the month of Ramadan where peopleare fasting during the day and going on leave.
Participants were recruited in the first stage by randomselection; the second stage involved sending a letter of invi-tation to the subjects and the third stage involved randomlyassigning participants to one of two groups using a randomnumber able [10]. Stratified randomization was used to ensurethat important characteristics were balanced approximately.This was done by producing a separate block randomizationlist for each group.
All participants (both in the control and in the inter-vention group) ultimately received the diabetes educationaltoolkit as it was deemed unethical to withhold the educa-tional tool kit from the control group. This was given tothe intervention group in addition to the education pro-gramme. Non-contamination of our subjects was insuredsince none had participated in any pharmacological or
behavioural interventions previously. The educational toolkitis a patient centred educational booklet for self-managementof diabetes mellitus which is written in simple layman’s lan-guage, coupled with coloured pictorial materials followed by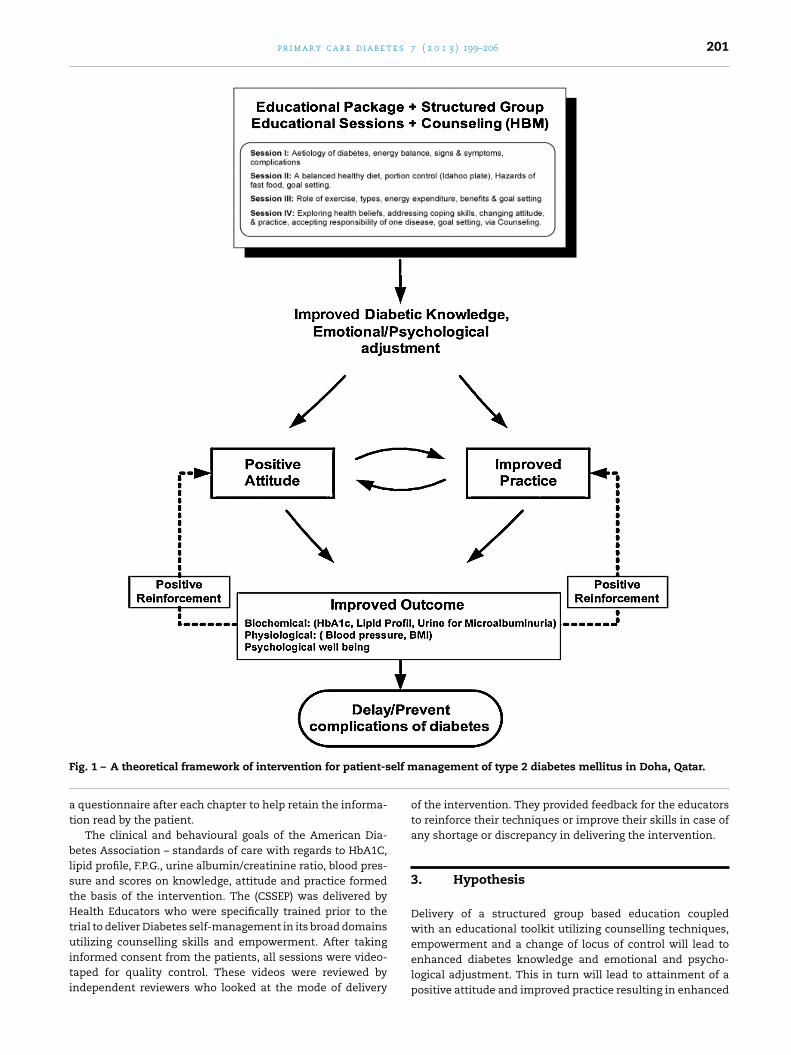
p r i m a r y c a r e d i a b e t e s 7 ( 2 0 1 3 ) 199–206 201
F elf m
at
blstHtuiti
ig. 1 – A theoretical framework of intervention for patient-s
questionnaire after each chapter to help retain the informa-ion read by the patient.
The clinical and behavioural goals of the American Dia-etes Association – standards of care with regards to HbA1C,
ipid profile, F.P.G., urine albumin/creatinine ratio, blood pres-ure and scores on knowledge, attitude and practice formedhe basis of the intervention. The (CSSEP) was delivered byealth Educators who were specifically trained prior to the
rial to deliver Diabetes self-management in its broad domains
tilizing counselling skills and empowerment. After takingnformed consent from the patients, all sessions were video-aped for quality control. These videos were reviewed byndependent reviewers who looked at the mode of delivery
anagement of type 2 diabetes mellitus in Doha, Qatar.
of the intervention. They provided feedback for the educatorsto reinforce their techniques or improve their skills in case ofany shortage or discrepancy in delivering the intervention.
3. Hypothesis
Delivery of a structured group based education coupledwith an educational toolkit utilizing counselling techniques,
empowerment and a change of locus of control will lead toenhanced diabetes knowledge and emotional and psycho-logical adjustment. This in turn will lead to attainment of apositive attitude and improved practice resulting in enhanced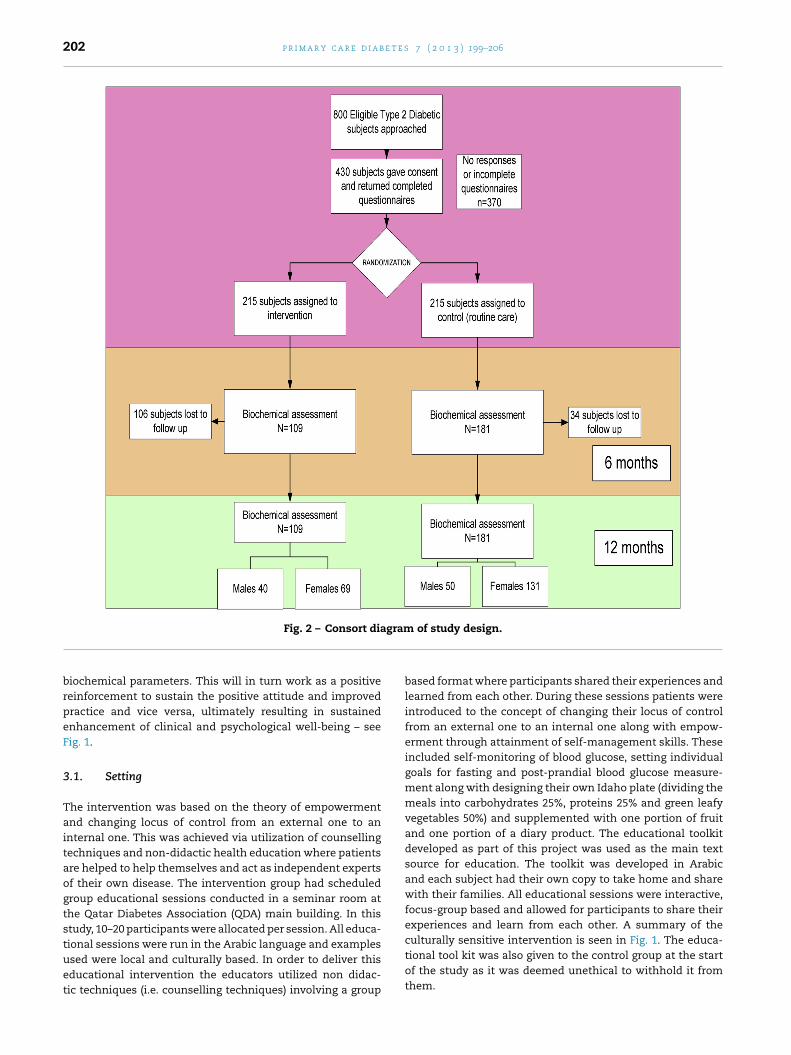
202 p r i m a r y c a r e d i a b e t e s 7 ( 2 0 1 3 ) 199–206
gram
Fig. 2 – Consort diabiochemical parameters. This will in turn work as a positivereinforcement to sustain the positive attitude and improvedpractice and vice versa, ultimately resulting in sustainedenhancement of clinical and psychological well-being – seeFig. 1.
3.1. Setting
The intervention was based on the theory of empowermentand changing locus of control from an external one to aninternal one. This was achieved via utilization of counsellingtechniques and non-didactic health education where patientsare helped to help themselves and act as independent expertsof their own disease. The intervention group had scheduledgroup educational sessions conducted in a seminar room atthe Qatar Diabetes Association (QDA) main building. In thisstudy, 10–20 participants were allocated per session. All educa-
tional sessions were run in the Arabic language and examplesused were local and culturally based. In order to deliver thiseducational intervention the educators utilized non didac-tic techniques (i.e. counselling techniques) involving a groupof study design.
based format where participants shared their experiences andlearned from each other. During these sessions patients wereintroduced to the concept of changing their locus of controlfrom an external one to an internal one along with empow-erment through attainment of self-management skills. Theseincluded self-monitoring of blood glucose, setting individualgoals for fasting and post-prandial blood glucose measure-ment along with designing their own Idaho plate (dividing themeals into carbohydrates 25%, proteins 25% and green leafyvegetables 50%) and supplemented with one portion of fruitand one portion of a diary product. The educational toolkitdeveloped as part of this project was used as the main textsource for education. The toolkit was developed in Arabicand each subject had their own copy to take home and sharewith their families. All educational sessions were interactive,focus-group based and allowed for participants to share theirexperiences and learn from each other. A summary of theculturally sensitive intervention is seen in Fig. 1. The educa-
tional tool kit was also given to the control group at the startof the study as it was deemed unethical to withhold it fromthem.
e s 7
3
AatagaekfStdPpf
3Hd
3Bp
3BiClb
3
Timok
3
Ays(tlbefwUaoswdp
p r i m a r y c a r e d i a b e t
.2. Measures
ssessment of knowledge, attitudes and current practices wasscertained by using a modified previously validated ques-ionnaire used in a similarly designed study [9] and modifiednd translated into Arabic to suit the requirements of the tar-et population. The questionnaire consisted of 36 items using
likert scale scoring system. Questions assessing knowl-dge comprised 12 items designed to determine subjects’nowledge about Diabetes, its complications, correct diet toollow, proper management decisions and exercise habits.imilarly, attitude appraisal questions assessed subjects atti-ude towards their disease, life-style issues, diet, controllingiabetes and having confidence in declaring having diabetes.ractice questions on the other hand concentrated on theatient’s compliance with treatment, diet adherence, exercise,oot examination and regular follow-up.
.2.1. Height and weight measurementseight measurements was carried out using a portable sta-iometer.
.2.2. Blood pressure measurementslood pressure measurements were taken using a digital bloodressure monitor applying accepted methods [10].
.2.3. Biochemical and haematological measurementsiochemical and haematological measurements were taken
n accordance with the aligned method used in the Diabetesontrol and Complications Trial (DCCT) [11] and recent guide-
ines reports were used to determine acceptable ranges foriochemical and biomedical data [12].
.3. Study outcomes
he primary outcomes of the intervention at 12 monthsncluded reduction in HbA1C, F.P.G., lipid profile, albu-
in/creatinine ratio, BMI and blood pressure. Secondaryutcomes for the intervention were improvement in diabetesnowledge, attitude and practice.
.4. Statistics analysis
n intention to treat basis was used during statistical anal-sis. The primary outcome measures were used to test thetudy hypotheses by calculating means, standard deviationsSD) and standard errors of means (SEM). Mean differences andheir equivalent 95% confidence intervals (95% CI) were calcu-ated e.g. for HbA1c to allow for further statistical comparisonsetween control and intervention groups similar to methodsmployed in previous studies [13]. Quantitative data collectedrom physical, physiological and biochemical measurementsere also grouped as mean (±SD) values. The Mann–Whitney-test was employed in statistical analysis to compare means,s the data did not appear to fit (or obey completely the rulesf) a normal distribution pattern. A series of univariant analy-
is of covariance at different time (6 and 12 months) intervalsas conducted to find out if there is any statistically significantifferences between the two arms with regard to biochemicalrofiles, knowledge, attitude and practice.( 2 0 1 3 ) 199–206 203
4. Results
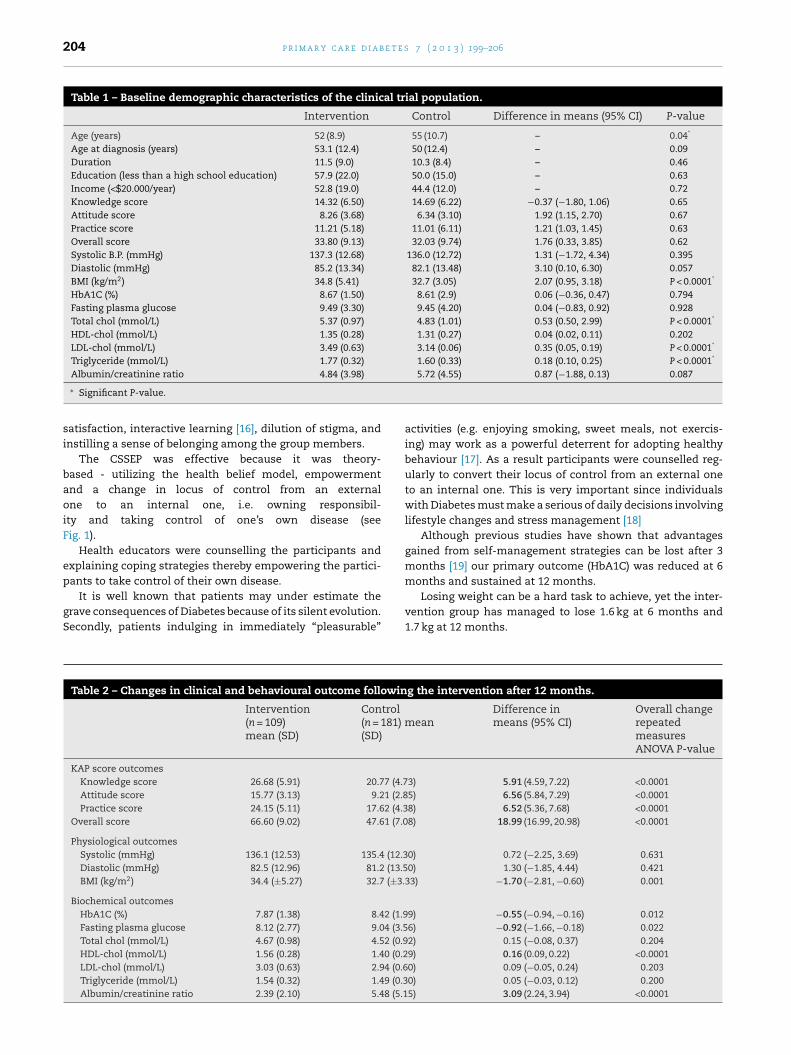
The majority of subjects was obese females with poormetabolic control and had elevated FBS, HbA1C, LDL choles-terol and a high albumin/creatinine ratio at baseline (seeTable 1). At baseline there were no statistically significant dif-ferences between the intervention and control groups withregards to F.P.G., HbA1C, HDL cholesterol, albumin/creatinineratio and blood pressure. However, statistically significantchanges in metabolic parameters were evident at baselinebetween the intervention and control group in few outcomemeasures including total cholesterol, LDL cholesterol andtriglycerides and BMI (see Table 1). On the other hand, withregards to knowledge, attitude and practice there were no sta-tistically significant changes between intervention and controlgroup except on the attitude scale (see Table 1).
4.1. Biomedical outcomes
By 12 months the intervention group compared with thecontrol group had: greater HbA1C reduction (−0.55 mmol/L,P < 0.0001); greater reduction in F.P.G. (−0.92 mmol/L), P = 0.015);greater reduction in B.M.I. (−1.70 kg, P = 0.001); and greaterreduction in albumin/creatinine ratio (−3.09, P < 0.0001).However, there were no statistically significant differencesbetween the groups with regards to total cholesterol, LDL–Ccholesterol, triglycerides and systolic blood pressure (seeTable 2).
4.2. Life style outcomes (KAP)
The intervention group had improvement in diabetes knowl-edge (5.9%, P < 0.0001), attitude (6.56%, P < 0.0001) and practice(6.25%, P = 0.0001) (see Table 2).
5. Discussion
Enrolment in the CSSEP led to significantly improved glycemiccontrol, lower lipid profile, reduced BMI and an improvementin the albumin/creatinine ratio. Psychosocial adjustmentand well-being was evident from the statistically significantimprovement seen in the domains of diabetes knowledge,attaining a positive attitude towards diabetes and improvedpractice.
Although the control group had a higher baseline attitudescore than the intervention group, this could have been dueto over estimation, or false perception of one’s own attitude.This is supported by the fact that practice score was not signif-icantly different between the two groups at baseline, and thispositive attitude was not maintained at the end of the study.
Knowledge, attitude and practice were all significantlyimproved in the intervention group at the conclusion of thestudy and not in the control group.
Knowledge alone is not sufficient in enabling patients tomanage their Diabetes safely and effectively [14,15].
Improvements in KAP score could be related to the useof a group-based approach which leads to higher patient
204 p r i m a r y c a r e d i a b e t e s 7 ( 2 0 1 3 ) 199–206
Table 1 – Baseline demographic characteristics of the clinical trial population.
Intervention Control Difference in means (95% CI) P-value
Age (years) 52 (8.9) 55 (10.7) – 0.04*
Age at diagnosis (years) 53.1 (12.4) 50 (12.4) – 0.09Duration 11.5 (9.0) 10.3 (8.4) – 0.46Education (less than a high school education) 57.9 (22.0) 50.0 (15.0) – 0.63Income (<$20.000/year) 52.8 (19.0) 44.4 (12.0) – 0.72Knowledge score 14.32 (6.50) 14.69 (6.22) −0.37 (−1.80, 1.06) 0.65Attitude score 8.26 (3.68) 6.34 (3.10) 1.92 (1.15, 2.70) 0.67Practice score 11.21 (5.18) 11.01 (6.11) 1.21 (1.03, 1.45) 0.63Overall score 33.80 (9.13) 32.03 (9.74) 1.76 (0.33, 3.85) 0.62Systolic B.P. (mmHg) 137.3 (12.68) 136.0 (12.72) 1.31 (−1.72, 4.34) 0.395Diastolic (mmHg) 85.2 (13.34) 82.1 (13.48) 3.10 (0.10, 6.30) 0.057BMI (kg/m2) 34.8 (5.41) 32.7 (3.05) 2.07 (0.95, 3.18) P < 0.0001*
HbA1C (%) 8.67 (1.50) 8.61 (2.9) 0.06 (−0.36, 0.47) 0.794Fasting plasma glucose 9.49 (3.30) 9.45 (4.20) 0.04 (−0.83, 0.92) 0.928Total chol (mmol/L) 5.37 (0.97) 4.83 (1.01) 0.53 (0.50, 2.99) P < 0.0001*
HDL-chol (mmol/L) 1.35 (0.28) 1.31 (0.27) 0.04 (0.02, 0.11) 0.202LDL-chol (mmol/L) 3.49 (0.63) 3.14 (0.06) 0.35 (0.05, 0.19) P < 0.0001*
Triglyceride (mmol/L) 1.77 (0.32) 1.60 (0.33) 0.18 (0.10, 0.25) P < 0.0001*
Albumin/creatinine ratio 4.84 (3.98)
∗ Significant P-value.
satisfaction, interactive learning [16], dilution of stigma, andinstilling a sense of belonging among the group members.
The CSSEP was effective because it was theory-based - utilizing the health belief model, empowermentand a change in locus of control from an externalone to an internal one, i.e. owning responsibil-ity and taking control of one’s own disease (seeFig. 1).
Health educators were counselling the participants andexplaining coping strategies thereby empowering the partici-pants to take control of their own disease.
It is well known that patients may under estimate thegrave consequences of Diabetes because of its silent evolution.Secondly, patients indulging in immediately “pleasurable”
Table 2 – Changes in clinical and behavioural outcome followin
Intervention(n = 109)mean (SD)
Control(n = 181)(SD)
KAP score outcomesKnowledge score 26.68 (5.91) 20.77 (4.7Attitude score 15.77 (3.13) 9.21 (2.8Practice score 24.15 (5.11) 17.62 (4.3
Overall score 66.60 (9.02) 47.61 (7.0
Physiological outcomesSystolic (mmHg) 136.1 (12.53) 135.4 (12.3Diastolic (mmHg) 82.5 (12.96) 81.2 (13.5BMI (kg/m2) 34.4 (±5.27) 32.7 (±3.
Biochemical outcomesHbA1C (%) 7.87 (1.38) 8.42 (1.9Fasting plasma glucose 8.12 (2.77) 9.04 (3.5Total chol (mmol/L) 4.67 (0.98) 4.52 (0.9HDL-chol (mmol/L) 1.56 (0.28) 1.40 (0.2LDL-chol (mmol/L) 3.03 (0.63) 2.94 (0.6Triglyceride (mmol/L) 1.54 (0.32) 1.49 (0.3Albumin/creatinine ratio 2.39 (2.10) 5.48 (5.1
5.72 (4.55) 0.87 (−1.88, 0.13) 0.087
activities (e.g. enjoying smoking, sweet meals, not exercis-ing) may work as a powerful deterrent for adopting healthybehaviour [17]. As a result participants were counselled reg-ularly to convert their locus of control from an external oneto an internal one. This is very important since individualswith Diabetes must make a serious of daily decisions involvinglifestyle changes and stress management [18]
Although previous studies have shown that advantagesgained from self-management strategies can be lost after 3months [19] our primary outcome (HbA1C) was reduced at 6months and sustained at 12 months.
Losing weight can be a hard task to achieve, yet the inter-vention group has managed to lose 1.6 kg at 6 months and1.7 kg at 12 months.
g the intervention after 12 months.
meanDifference inmeans (95% CI)
Overall changerepeatedmeasuresANOVA P-value
3) 5.91 (4.59, 7.22) <0.00015) 6.56 (5.84, 7.29) <0.00018) 6.52 (5.36, 7.68) <0.00018) 18.99 (16.99, 20.98) <0.0001
0) 0.72 (−2.25, 3.69) 0.6310) 1.30 (−1.85, 4.44) 0.421
33) −1.70 (−2.81, −0.60) 0.001
9) −0.55 (−0.94, −0.16) 0.0126) −0.92 (−1.66, −0.18) 0.0222) 0.15 (−0.08, 0.37) 0.2049) 0.16 (0.09, 0.22) <0.00010) 0.09 (−0.05, 0.24) 0.2030) 0.05 (−0.03, 0.12) 0.2005) 3.09 (2.24, 3.94) <0.0001
e s 7
csnomp
otict
pca
5
Trsmi
p r i m a r y c a r e d i a b e t
Furthermore, albumin/creatinine ratio improvement at theonclusion of the study could be attributed to the specific mes-age transmitted throughout the sessions that extra protein isephrotoxic. This is quite true since the average consumptionf protein intake in a typical Arabic diet in a one day meal planay exceed 300 g. This is in contrast to the average 80–100 g
rotein consumed by an average American.Although, group based educations are more effective than
ne-to-one education [20], the active ingredient (S) is difficulto define [21]. However, in our study the effectiveness of thentervention may be attributed to several factors includingounselling, empowering patients and forming a psycho-herapeutic alliance.
Furthermore, diet was approached by utilizing the Idaho-late method in a culturally acceptable way where localuisine was reinforced and portion control was explained andpplied using live demonstrations.
.1. Strengths and limitations the study
he study has several strengths: Firstly, the sample size wasepresentative. Secondly, the small number 10–20 patients per
ession makes it a feasible option to be applied in all pri-ary health care centres in Qatar since each health centres equipped with a conference Thirdly, the utilization of the
1 Insulin raises your blood sugar level2 Food is not an essential part of my life and I can accept cha3 I examine my feet on a regular basis4 I should immediately eat or drink something sweet when f5 Diabetes is an embarrassing disease to tell people about6 When I have blurred vision I see my doctor7 Rice is mainly protein8 I find it difficult to control my weight9 Loss of sensation in the feet is a normal occurrence in diab10 The normal range of blood glucose is (20–30 mmol/L) 370–511 Diabetes is the most unpleasant thing happened in my life12 I often eat fast food13 Fibrous food is good as it absorbs sugar more efficiently14 Adjusting my life to diabetes is quiet difficult15 I exercise regularly16 Being overweight does not worsen Blood sugar control.17 Most people do not know what it feels like to live with diab18 I do not take my diabetic medication on time (oral or insuli19 Heart, eyes, kidneys and feet can be damaged in uncontrol20 It is essential to involve a family member in managing my21 I eat at least one plate full of rice every day22 Smoking does not have any complications on diabetic subj23 Controlling diabetes seems to be a very hard goal to achiev24 I use butter instead of vegetable oil in the house25 Diabetic patients should avoid physical exercise26 I know everything about diabetes
( 2 0 1 3 ) 199–206 205
“culturally sensitive Idaho-plate” method makes it an attrac-tive and pragmatic way of cutting down on calories withoutthe feeling of hunger or the need to use exchange lists anddiet sheets.
Fourthly, the intervention is likely to be generalized toneighbouring Arab countries. However, there are severallimitations. Firstly, the high attrition rate encountered inthe course of the trial may represent a setback. Secondly,dietary intake, physical activities, and medication changewere not accounted for. Thirdly, complementary and alterna-tive medicine usage was not assessed as many patients useherbal medicine to treat their diabetes without divulging theinformation to their treating physicians.
In spite of these limitations to the present study, the signifi-cant improvement in biomedical and psychosocial parametersprovides a great opportunity for the study to be replicated inthe Arabian countries. This is particularly important since nostructured group based education currently exists or is appliedin the region.
Disclosure statement
The authors declare that they have no competing interests.
Appendix A. Knowledge, Attitude, Practice(KAP) Questionnaire
Agree Disagree
1 2 3 4 5 6 7
� � � � � � �nges � � � � � � �
� � � � � � �eeling hungry, dizzy and weak � � � � � � �
� � � � � � �� � � � � � �� � � � � � �� � � � � � �
etics and should be ignored � � � � � � �55 mg/DL � � � � � � �
� � � � � � �� � � � � � �� � � � � � �� � � � � � �� � � � � � �� � � � � � �
etes � � � � � � �n) � � � � � � �led diabetes mellitus � � � � � � �diabetes. � � � � � � �
� � � � � � �ects � � � � � � �e � � � � � � �
� � � � � � �� � � � � � �� � � � � � �

206 p r i m a r y c a r e d i a b e t e s 7 ( 2 0 1 3 ) 199–206
Agree Disagree
1 2 3 4 5 6 7
27 Separate type of food is being prepared for me at home � � � � � � �28 The diabetic patients can eat fruits but not too often � � � � � � �29 Having diabetes makes me feel different to the rest of the people � � � � � � �30 I often take soft drinks with my meals � � � � � � �31 Type II diabetes is due to lack of insulin and insulin resistance � � � � � � �32 I feel quite confident in controlling my diabetes with little help from doctors � � � � � � �33 I eat fruits daily � � � � � � �34 The presence of glucose in urine is a bad sign. � � � � � � �
rol � � � � � � �t sweets � � � � � � �
r
35 I feel happy being told that my diabetes is under cont36 When I feel dizzy, weak and hungry, I immediately ea
e f e r e n c e s
[1] J.A. Al-Lawati, A.L. Riyami, A.M. Mohammed, A.J.P. Jousilahti,Increasing prevalence of diabetes mellitus in Oman, DiabeticMedicine 19 (2002) 954–957.
[2] G. Lberti, P. Zimmet, J. SHAW, Z. Bloomgarden, F. Kaufman,M. Silink, Type 2 diabetes in the young: the evolvingepidemic: the international diabetes federation consensusworkshop, Diabetes Care 27 (2004) 1798–1811.
[3] International Diabetes Federation, e-Atlas-DiabetesPrevalence. Diabetes Prevalence, 2003www.idf.org/e-atlashome/index.cfm?node=79
[4] F. Al-Mahroos, Diabetes Mellitus in the Arabian Peninsula,Annals of Saudi Medicine 20 (2000) 111–112.
[5] A. Bener, M. Zirie, R. Al-Rikabi, Genetics, obesity andenvironmental risk factors associated with type 2 diabetes,Croatian Medical Journal 46 (2) (2005) 302–307.
[6] M. Trento, P. Passera, M. Tomalino, M. Bajardi, Pomero f, A.Allione, P. Vaccari, G.M. Molinati, M. Porta, Group visitsimprove metabolic control in type 2 diabetes. A 2 – yearfollow up, Diabetes Care 24 (June (6)) (2001) P995–P1000.
[7] World Medical Association, Declaration of Helsinki, JAMA277 (1998) 925–926.
[8] J.P. O’hare, N.T. Raymond, S. Mughal, et al., Evaluation ofdelivery of enhanced diabetes care to patients of SouthAsian ethnicity: the United Kingdom Asian Diabetes Study(UKADS), Diabetic Medicine 21 (2004) 1357–1365.
[9] H.R. Baradaran, R.P. Knill-Jones, A.S. Walli, S.A. Roger,controlled trial of the effectiveness of a diabetes educationprogram in a multi-ethnic community in Glasgow[ISRCT28317455], BMC Public Health 6 (2006) 134–143.
[10] L. Ramsay, B. Williams, G. Johnson, G. Mac Gregor, J. Potter, N.Poulter, et al., Guidelines for management of hypertension:report of the third working part of the British Hypertension
Society, Journal of Human Hypertension 13 (1999) 569–592.[11] C.L. Rolfing, H.M. Wiedmeyer, R.R. Little, J.D. England, A.Tennill, D.E. Goldstein, et al., Defining the relationshipbetween plasma glucose and HbA1C: analysis of glucose
profiles and HbA1C in the Diabetes Control andComplications Trial, Diabetes Care 25 (2002) 275–278.
[12] NICE, Management Type 2 Diabetes: Management of BloodPressure and Blood Lipids, Ref. No. 167, National Institute forClinical Excellence, London, 2002.
[13] T.A. Deakin, C. Mcshane, J.E. Cade, R. Williams, Group basedself- 285 management education in adults with type 2diabetes mellitus. Cochrane systematic review, Diabetes 53(2005) A515.
[14] T.J. Lockinton, S. Farrant, K.A. Meadows, et al., Knowledgeprofile and control in diabetic patients, Diabetic Medicine 5(1988) 381–386.
[15] R. Ambigapathy, S. Amigapathy, H.M. Ling, A knowledge,attitude and practice (KAP) study of diabetes mellitus amongpatients attending Llinik Kesihatan Seri Manjung, NCDMalaysia 2 (2) (2003) 6–16.
[16] C.R. Mensing, S.L. Norris, Group education in diabetes:effectiveness and implementation, Diabetes Spectrum 16(2003) 96–103.
[17] C. Silagy, J. Muir, A. Coulter, M. Thorogood, L. Roe,Cardiovascular risk and attitudes to lifestyle: what dopatients think? BMJ 306 (1993) 1657–1660.
[18] R.M. Anderson, M.M. Funnell, J.T. Fitzgerald, D.G. Marrero,The diabetes empowerment scale, a measure ofpsychosocial self-efficacy, Diabetes Care 23 (June (6)) (2000)739–743.
[19] S.L. Norris, J. Lau, S.J. Smith, C.H. Schmid, M.M. Engelgau,Self Management education for adults with type 2 diabetes:a met analysis of the effect on glycemic control, DiabetesCare 25 (2002) 1159–1171.
[20] P.L. Rickheim, T.W. Weaver, J.L. Flader, D.M. Kendall,Assessment of group versus individual diabetes education: arandomized study, Diabetes Care 25 (2002) 269–274.
[21] Medical Research Council, A Framework for Developmentand Evaluation of RCTs for Complex Interventions toImproves Health, Medical Research Council, London,2000.