Embed Size (px)
Citation preview

VIEWS
DECEMBER 2016�CANCER DISCOVERY | 1309
IN THE SPOTLIGHT
Culprit or Bystander ? The Role of the Fallopian Tube in “Ovarian” High-Grade Serous Carcinoma Elizabeth M. Swisher 1 , Rochelle L. Garcia 2 , Mark R. Kilgore 2 , and Barbara M. Norquist 1
“Ovarian” (pelvic) carcinomas comprise a heterogeneous
group of neoplasms, which may be unique among solid
tumors in the lack of consensus about the organ or origin.
Traditionally, nonuterine pelvic carcinomas have been labeled
as ovarian, fallopian tube (FT), or primary peritoneal based on
arbitrary assignations based on the volume of disease identi-
fi ed at different sites and the presumption that the ovary is
the most common site of origin. For example, Gynecologic
Oncology Group (GOG) criteria specify the ovary as the pri-
mary site of disease for any nonuterine high-grade serous car-
cinoma (HGSC) involving multiple intra-abdominal organs
with at least 0.5 cm of ovarian stromal involvement. Similarly,
if both the ovary and FT have bulky neoplasm, the primary
site is labeled ovary unless there is a clear transition from
intraepithelial neoplasm to invasive carcinoma in the FT.
However, no such transition is required to label nonuterine
HGSC as ovarian primary, and a similar precursor intraepi-
thelial neoplasm of the ovary has yet to be identifi ed. The
increased use of neoadjuvant chemotherapy, which affects
disease distribution, further increases the diffi culty of deter-
mining the site of origin. Understanding the origin and the
path of progression of these aggressive carcinomas directly
bears on strategies for risk assessment, early detection, and
prevention.
The ovary is primarily composed of stroma with a smaller
fraction consisting of germ cells and ovarian surface epithe-
lium, which is derived from primordial mesothelium. Pelvic
nonuterine carcinomas can be broken down into a number of
distinct histologic subtypes, including serous, clear cell, endo-
metrioid, mucinous, and those with mixed features. Each of
these subtypes is associated with distinct molecular pathways
and may arise from different organs and cells of origin. For
example, clear cell and endometrioid carcinomas probably
arise in endometriosis and share characteristic alterations in
1 Division of Gynecologic Oncology, Department of Obstetrics and Gyne-cology, University of Washington, Seattle, Washington . 2 Department of Pathology, University of Washington, Seattle, Washington.
Corresponding Author: Elizabeth M. Swisher , University of Washington, 1959 NE Pacifi c Street, Seattle, WA 98195. Phone: 206-543-3669; Fax: 206-543-8315; E-mail: [email protected]
doi: 10.1158/2159-8290.CD-16-1197
©2016 American Association for Cancer Research.
Summary: The concurrence of intraepithelial high-grade neoplasia in the fallopian tube with metastatic implants
has been taken as evidence of a tubal origin for high-grade serous pelvic carcinomas. In the current issue, Eckert
and colleagues perform detailed genomic phylogenetic analyses and demonstrate that some cases of high-grade
serous intraepithelial tubal neoplasia are metastatic implants and not precursor lesions. Cancer Discov; 6(12);
1309–11. ©2016 AACR.
See related article by Eckert and colleagues, p. 1342 (7).
PTEN, PIK3CA , and ARID1A . Serous carcinomas are divided
into low-grade and high-grade carcinomas. HGSC is the most
common form of nonuterine pelvic carcinoma, representing
approximately 70% of cases, and is characterized by near-
universal mutations in TP53 , genomic instability, and defects
in DNA repair, particularly homologous recombination repair.
Pelvic HGSC usually presents with metastatic and bulky multi-
focal disease, making the organ of origin diffi cult to determine.
It was recognized in the early 1980s that HGSC could be
multifocal and coexist with intraepithelial neoplasia in the
FT, and Bannatyne and Russell recommended more careful
pathologic evaluation of the entire FT in cases with HGSC
( 1 ). But it was the uptake of preventive surgeries in the late
1990s for genetic risk of “ovarian” carcinoma conferred by
inherited mutations in BRCA1 and BRCA2 ( BRCA1/2 ) that
provided a new window into the origin of HGSC ( 2, 3 ). Occult
neoplasms identifi ed at risk-reducing surgery in BRCA1/2
mutation carriers are almost always located in the FT and
not the ovary, including both microscopic invasive HGSC
and high-grade intraepithelial neoplasia [also termed serous
tubal intraepithelial carcinoma (STIC)]. The predominance
of the FT as the site of these early neoplasms led to the tubal
hypothesis: that the FT is the origin of nonuterine pelvic
HGSC. The practice of complete serial sectioning of the FTs
became standard of care for risk-reducing surgeries in high-
risk women, a practice essential to the identifi cation of micro-
scopic neoplasia in the FT ( 2, 3 ). The tubal origin of HGSC
was further supported by a series of studies that identifi ed
frequent occult tubal involvement in advanced-stage pelvic
HGSC if careful serial sectioning of the FT was performed ( 4 ).
However, these studies showed an association between neo-
plastic lesions in the FT and elsewhere, without proving the
site of origin. The relative role of the FT in sporadic HGSC
may also have been confused by not distinguishing sporadic
from inherited pelvic HGSC in most studies.
Nevertheless, the paradigm shift toward a tubal origin of
nonuterine HGSC was so complete that the tubal hypothesis
was featured by Dr. Oz in 2009 and discussed widely on blogs.
High-risk women wondered why they needed to remove their
ovaries and suffer the consequences of surgical menopause if
the real culprit was the FT. The clinical implications are great;
risk-reducing salpingo-oophorectomy reduces mortality of
BRCA1/2 mutation carriers ( 5 ). The safety for high-risk women
Research. on November 26, 2020. © 2016 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from

VIEWS
1310 | CANCER DISCOVERY�DECEMBER 2016 www.aacrjournals.org
of retaining the ovaries is unknown, and a randomized trial
comparing bilateral salpingectomy to salpingo-oophorectomy
would be unethical. For women at normal risk of “ovarian”
cancer, some experts have suggested that bilateral salpingec-
tomy should be the preferred method of female sterilization
and should be performed with every hysterectomy when ova-
ries are retained (called opportunistic salpingectomy; ref. 6 ).
The study by Eckert and colleagues provides new insights
into this thorny problem ( 7 ). The diminutive size of STIC
lesions in the FT provides challenges for detailed molecular
characterization. Nevertheless, the authors isolated neoplastic
cells using laser-capture microdissection and applied whole-
exome sequencing to STIC paired with metastatic deposits
from the same patient. They then used phylogenetic analyses
to postulate the primary site. Among eight women with STIC
and multifocal HGSC, mutational profi ling identifi ed the
STIC as the precursor lesion in half. But notably, in at least
two cases, the STIC appeared to be a metastatic implant.
They experimentally supported the plausibility of intramu-
cosal spread to the FT by demonstrating that HGSC sphe-
roids can implant into the epithelium of e x vivo FT explants
and attain a similar appearance to STIC (Fig. 4E of ref. 7 ).
The potential for intramucosal metastatic implants is not
unique to this scenario, as it is a well-documented fi nding in
bronchial epithelium from lung carcinomas and even in FT
epithelium from nongynecologic sources ( 8, 9 ). Previous evi-
dence for the possibility of metastatic spread to the FT from
HGSC came from the observation of multifocal STIC present
in some advanced HGSC cases and the presence of STIC in
some cases of uterine serous carcinomas.
These fi ndings call into question previous assumptions
that the fi nding of synchronous STIC and metastatic HGSC
implicates the FT as the organ of origin. The best evidence
for a FT origin for HGSC remains the location of the early
microscopic cancers identifi ed in women with increased gen-
etic risk. When only microscopic cancer is identifi ed, FTs are
serially sectioned, and cases with multifocal disease or elevated
serum CA125 (implying macroscopic disease) are excluded,
the FT is the location in 90% of HGSC in BRCA1/2 mutation
carriers. The role of the FT in sporadic HGSC is less well
defi ned. Eckert and colleagues evaluated only cases without
BRCA1/2 mutations and provide some answers. In half of
the cases, STIC was the presumed precursor lesion, so the FT
remains the likely origin for many sporadic “ovarian” HGSCs.
But these cases were specifi cally chosen because they had
identifi able STIC, and many women with sporadic ovarian
and peritoneal HGSC have no such identifi able lesions. There-
fore, the fraction of unselected sporadic HGSCs that have an
FT origin remains unknown. Larger phylogenetic studies of
HGSC genotyped for inherited risk are needed to answer this
question. These data will be critical in understanding the effi -
cacy of opportunistic salpingectomy in reducing cancer risk.
The origin of HGSC that is labeled primary peritoneal
carcinoma is another interesting mystery on which the work
by Eckert and colleagues sheds light and raises important
questions. In BRCA1/2 mutation carriers who have undergone
bilateral salpingo-oophorectomy, the majority of primary per-
itoneal carcinomas occur in the fi rst 5 years after risk-reducing
surgery with only rare cases reported after that ( 10 ). These
data suggest that an occult FT or ovarian carcinoma missed at
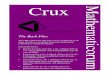
Figure 1. Spread patterns of HGSC (blue deposits). In some cases of sporadic pelvic HGSC, the high-grade intraepithelial neoplasia (also called STIC) is the precursor lesion, spreading to the ovary and omentum in parallel or sequentially. In other cases, HGSC from other sites spreads to the FT as a metastatic intraepithelial lesion histologically indistinguishable from intraepithelial neoplasia originating in the FT .
Fallopiantube
Bladder
Intraepithelialneoplasia
Smallintestine
Colon
PeritoneumUterus
Cancer
Ovary
Omentum
Research. on November 26, 2020. © 2016 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from

VIEWS
DECEMBER 2016�CANCER DISCOVERY | 1311
time of risk-reducing surgery might be the actual source of the
majority of “primary peritoneal” carcinomas in women with
BRCA1/2 mutations. The omentum is typically the anatomic
site of bulkiest tumor in “primary peritoneal” carcinoma. In
the two cases in which the STIC was secondary to metastatic
spread, Eckert and colleagues identifi ed the omentum as the
most “basal” of the sampled tumor sites ( 7 ). In women with-
out cancer, the omentum is a common site of endosalpingi-
osis, non-neoplastic FT-like epithelium occurring outside the
FT. Possibly, endosalpingiosis in the omentum was the site
of origin, though endosalpingiosis is more often associated
with low-grade serous neoplasms. Alternatively, the primary
site may not have been sampled for these 2 patients, and the
omentum represented an early site of metastasis with further
metastasis occurring from the omentum to FT mucosa.
Understanding the origin of pelvic carcinomas is critically
important for optimizing cancer prevention strategies at both
the individual and population levels. In studying the origin of
HGSC, it remains important to separate cases driven by germline
mutations in BRCA1/2 or other ovarian cancer susceptibility
genes from sporadic carcinomas. Eckert and colleagues have
made a seminal contribution to our understanding by providing
genomic and experimental data supporting the ability of at least
some sporadic HGSC to secondarily implant into the FT mucosa
( Fig. 1 ). We congratulate the authors and look forward to further
revelations on the molecular progression of pelvic HGSC.
Disclosure of Potential Confl icts of Interest No potential confl icts of interest were disclosed .
Grant Support B.M. Norquist is supported by a Liz Tilberis Career Development
Award from the Ovarian Cancer Research Fund Alliance.
Published online December 5, 2016.
REFERENCES 1. Bannatyne P , Russell P . Early adenocarcinoma of the fallopian
tubes. A case for multifocal tumorigenesis . Diagn Gynecol Obstet
1981 ; 3 : 49 – 60 .
2. Lamb JD , Garcia RL , Goff BA , Paley PJ , Swisher EM . Predictors
of occult neoplasia in women undergoing risk-reducing salpingo-
oophorectomy . Am J Obstet Gynecol 2006 ; 194 : 1702 – 9 .
3. Powell CB , Kenley E , Chen LM , Crawford B , McLennan J , Zaloudek C ,
et al. Risk-reducing salpingo-oophorectomy in BRCA mutation car-
riers: Role of serial sectioning in the detection of occult malignancy .
J Clin Oncol 2005 ; 23 : 127 – 32 .
4. Kindelberger DW , Lee Y , Miron A , Hirsch MS , Feltmate C , Medeiros F ,
et al. Intraepithelial carcinoma of the fi mbria and pelvic serous car-
cinoma: Evidence for a causal relationship . Am J Surg Pathol 2007 ;
31 : 161 – 9 .
5. Domchek SM , Friebel TM , Singer CF , Evans DG , Lynch HT ,
Isaacs C , et al. Association of risk-reducing surgery in BRCA1 or
BRCA2 mutation carriers with cancer risk and mortality . JAMA
2010 ; 304 : 967 – 75 .
6. McAlpine JN , Hanley GE , Woo MM , Tone AA , Rozenberg N , Swen-
erton KD , et al. Opportunistic salpingectomy: uptake, risks, and
complications of a regional initiative for ovarian cancer prevention .
Am J Obstet Gynecol 2014 ; 210 : 471 e1–11 .
7. Eckert MA , Pan S , Hernandez KM , Loth RM , Andrade J , Volchenboum
SL , et al. Genomics of ovarian cancer progression reveals diverse
metastatic trajectories including intraepithelial metastasis to the fal-
lopian tube . Cancer Discov 2016;6:1342–51 .
8. Rabban JT , Vohra P , Zaloudek CJ . Nongynecologic metastases to fal-
lopian tube mucosa: A potential mimic of tubal high-grade serous
carcinoma and benign tubal mucinous metaplasia or nonmucinous
hyperplasia . Am J Surg Pathol 2015 ; 39 : 35 – 51.
9. Stewart CJ , Leung YC , Whitehouse A . Fallopian tube metastases of
non-gynaecological origin: A series of 20 cases emphasizing patterns
of involvement including intra-epithelial spread . Histopathology
2012 ; 60 : E106 – 14.
10. Finch A , Beiner M , Lubinski J , Lynch HT , Moller P , Rosen B ,
et al. Salpingo-oophorectomy and the risk of ovarian, fallopian tube,
and peritoneal cancers in women with a BRCA1 or BRCA2 Mutation .
JAMA 2006 ; 296 : 185 – 92 .
Research. on November 26, 2020. © 2016 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from

2016;6:1309-1311. Cancer Discov Elizabeth M. Swisher, Rochelle L. Garcia, Mark R. Kilgore, et al. High-Grade Serous CarcinomaCulprit or Bystander? The Role of the Fallopian Tube in ''Ovarian''
Updated version
http://cancerdiscovery.aacrjournals.org/content/6/12/1309
Access the most recent version of this article at:
Cited articles
http://cancerdiscovery.aacrjournals.org/content/6/12/1309.full#ref-list-1
This article cites 10 articles, 2 of which you can access for free at:
Citing articles
http://cancerdiscovery.aacrjournals.org/content/6/12/1309.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerdiscovery.aacrjournals.org/content/6/12/1309To request permission to re-use all or part of this article, use this link
Research. on November 26, 2020. © 2016 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from