Embed Size (px)
Citation preview
Author's Accepted Manuscript
This Cuff Tear Arthropathy is Best Treated with aReverse Total Shoulder Arthroplasty: Affirm
Matthew P. Baker MD, Lynn A. Crosby MD
PII: S1045-4527(14)00086-8DOI: http://dx.doi.org/10.1053/j.sart.2014.04.017Reference: YSART50606
To appear in:Semin Arthro
Cite this article as: Matthew P. Baker MD, Lynn A. Crosby MD, This Cuff TearArthropathy is Best Treated with a Reverse Total Shoulder Arthroplasty: Affirm,Semin Arthro , http://dx.doi.org/10.1053/j.sart.2014.04.017
This is a PDF file of an unedited manuscript that has been accepted for publication. As aservice to our customers we are providing this early version of the manuscript. Themanuscript will undergo copyediting, typesetting, and review of the resulting galley proofbefore it is published in its final citable form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers that applyto the journal pertain.
www.elsevier.com/locate/enganabound

This Cuff Tear Arthropathy is Best Treated with a Reverse Total Shoulder Arthroplasty: Affirm
Matthew P. Baker, MD Department of Orthopaedic Surgery, Medical College of Georgia, Georgia Regents University, Augusta, GA
Lynn A. Crosby, MD Department of Orthopaedic Surgery, Medical College of Georgia, Georgia Regents University, August, GA
Address reprint requests to: Lynn A. Crosby, MD Professor, Director of Shoulder Surgery, Department of Orthopaedic Surgery, Medical College of Georgia, Georgia Regents University, August, GA Contact: 1120 15th St., Dept of Orthopaedics, Augusta, GA 30912, [email protected]
From: Department of Orthopaedic Surgery, Medical College of Georgia, Georgia Regents University, Augusta, GA
ABSTRACT Cuff tear arthropathy is the arthritic eroded collapse of the glenohumeral
joint with progressive superior humeral migration in the setting of long standing
rotator cuff insufficiency. The ideal management of cuff tear arthropathy remains
elusive. Current arthroplasty options include hemiarthroplasty or reverse shoulder
arthroplasty. Proper clinical and radiographic evaluation are essential in decision
making in order to optimize outcomes. Acromiohumeral distance (AHD), as
measured on plain radiographs, as well as fatty degeneration of the rotator cuff
muscles on MRI are reliable tools for decision making. AHD < 7mm correlates
well with complete tear of the supraspinatus while AHD < 5mm indicates
infraspinatus involvement with significant muscular atrophy. Hemiarthroplasty

remains an option for providing pain relief; however, continued development of
superior migration and glenoid erosion remains a concern. The conversion to
reverse total shoulder arthroplasty after hemiarthroplasty can be difficult due to
glenoid bone loss. Recent literature supports the use of reverse total shoulder
arthroplasty over hemiarthroplasty for cuff tear arthropathy with significant
differences in functional outcome. Here, we discuss the radiographic evaluation of
cuff tear arthropathy and review the treatment options and why we advocate the
use of the reverse prosthesis.
Case Discussion:
This discussion was centered on the optimal treatment for the patient with the
radiographs in Figure 1. The patient was a sixty-nine year old male, a previous tennis
player, who has pain with activity and at rest. On physical examination, active range of
motion is limited to eighty degrees forward elevation and abduction, with evidence of
grade IV fatty infiltration on MRI.
The ideal management of cuff tear arthropathy remains a challenge despite an
abundance of recent literature addressing this issue. Cuff tear arthropathy, as described
by Neer and Craig1, is characterized by the arthritic eroded collapse of the glenohumeral
joint with superior migration of the humeral head after a massive rotator cuff tear. Other
characteristics include: erosive changes to the superior glenoid and acromion, humeral
head collapse, and subcutaneous effusion. Natural progression of cuff tear arthropathy
includes: progressive superior migration of the humeral head with progressive erosion of
the under surface of the acromion, loss of the capsular stabilizers, and ultimately anterior
superior escape of the humerus. Prior to the availability of the reverse prosthesis, surgical

treatment of patients with advanced rotator cuff arthropathy with anterior superior escape
was plagued with complications and poor outcomes. Current surgical management for
chronic irreparable rotator cuff tears with arthropathy has fallen into two categories:
hemiarthroplasty or reverse total shoulder replacement.
Hemiarthroplasty for cuff tear arthropathy was advocated in response to early
failures with standard and constrained total shoulder arthroplasty, particularly failure of
the glenoid component2,3. This was believed to be due largely to increased shear forces
across the glenoid with unopposed pull of the deltoid in cuff deficient shoulders.
Hemiarthroplasty has shown reliable results in terms of pain relief and function when
compared against early limited goals criteria. However, concern remains for subsequent
development of anterior superior escape after hemiarthroplasty, especially in patients
who have a history of previous subacromial decompression. Continued erosion of the
acromion with hemiarthroplasty also makes further conversion to a reverse difficult or
impossible.
Results with early designs of reverse total shoulder arthroplasty were met with
catastrophic failure. It wasn’t until Grammont introduced the Delta prosthesis that reverse
shoulder arthroplasty become a viable option in the treatment of cuff tear arthropathy4.
Reverse prosthesis can reliably provide pain relief and return of function; however,
concerns remain over reports of high complication rates and lack of good long term
outcome data.

Making the Diagnosis:
Clinical findings of pain, with and without activity, loss of active and passive
range of motion, atrophy of infraspinatus and supraspinatus musculature, and
demonstratable weakness of elevation and external rotation are all findings that can be
associated with massive rotator cuff deficiency. Hamada5 described the classic
radiographic changes of rotator cuff arthropathy including superior migration of the
humeral head, joint space narrowing, wearing of the undersurface of the acromion,
superior wear of the glenoid, and a decrease in acromio-humeral distance. Of note, the
acromio-humeral distance has been shown to be an accurate predictor of rotator cuff
abnormalities. Saupe6 described the relationship between reduced acromio-humeral
distance with MRI findings of rotator cuff tear and fatty degeneration. Normal acromio-
humeral distance is typically from 7-14 mm and correlates with complete fill of the
supraspinatus fossa on sagittal MRI. Acromio-humeral distance < 7mm but >5mm on
radiographs has been shown to correlate well with full thickness tear of the supraspinatus
and fatty atrophy within the supraspinatus fossa on MRI. Figure 2 shows an example of
radiographs and MRI of these findings. Saupe found that 90% of patients with acromio-
humeral distance <7mm had full thickness supraspinatus tears with 67% also involving
the infraspinatus. Goutallier7 further showed that acromio-humeral distance < 6mm is
associated almost systematically with complete infraspinatus tear with advanced fatty
degeneration. It is important to distinguish these patients as an attempt at repairing the
rotator cuff is not recommended, and it has to be recognized that by replacing the
proximal humerus with a heimarthroplasty there will be continued erosion of the
undersurface of the acromial process.

Guiding Management:
Radiographic findings, including acromio-humeral distance (AHD) and fatty
atrophy on MRI or CT are useful in guiding surgical management of rotator cuff
deficiency. The Goutallier classification, based on computed tomography, of rotator cuff
fatty infiltration is an accepted standard8. Advanced atrophy is a negative predictive
factor for successful rotator cuff repair and functional outcome9. When evaluating for
surgical decision making, it is helpful to take into account not only tear size and
retraction on MRI, but also degree of fatty atrophy and acromio-humeral distance on
radiographs. Decision making based on MRI findings of a massive rotator cuff tear with
significant retraction of the supraspinatus tendon alone may lead to the conclusion that
this is an irreparable situation. However, in conjunction with plain radiographs that
demonstrate a humeral head that is still centered with a relatively normal AHD and lack
of significant fatty atrophy on MRI, primary repair may be warranted. When the AHD is
< 5mm then repair is unlikely to be successful and other treatment options should be
considered.
Non-arthroplasty options:
Conservative treatment with cortisone injections into the gleno-humeral joint and
subacromial bursae and physical therapy focused on improving deltoid function can be
attempted with the goal to decrease the pain and increase the range of motion. Surgical
options including arthroscopy with debridement and biceps tenotomy or tenodesis have
shown good results in pain relief, particularly in male patients with ROM above 100
degrees and good deltoid function10. Failure of these treatments leaves the options of
hemiarthroplasty or reverse total shoulder arthroplasty.
Visostky and Seebauer11 developed a classification scheme for progression of
rotator cuff arthropathy based on clinical and radiographic parameters. The four groups
are distinguished by degree of superior migration from the center of rotation and the
amount of instability present. Classically, in type IA and IB, the humeral head remains
centered and there is minimal superior migration due to an intact coracoacromial arch
(Figure 3). Traditionally, hemiarthroplasty was advocated in these groups. Type IIA and
IIB are characterized by a degree of anterior instability with loss of coracoacromial arch
stabilization and migration of the humeral head (Figure 4). Reverse total shoulder
arthroplasty was recommended in these groups due to loss of anterior restraints and an
incompetent coracoacromial arch.
Why Reverse Total Shoulder Arthroplasty
Although reliable pain relief can be achieved with hemiarthroplasty, concerns
remain about the development or continuation of superior glenoid and acromial erosion.
The incidence of continued superior migration after anatomic arthroplasty has been
reported as high as 55%12,13. Patients who have previously had subacromial
decompression with insufficiency of their coracoacromial arch, are particularly at risk.
Figure 5 demonstrates these findings in a patient with rotator cuff arthropathy treated
with hemiarthroplasty. Radiographs show anterior superior glenoid erosion after
continued superior migration of the humeral head. Ultimately, if this treatment fails,
reconstruction with reverse total shoulder arthroplasty is the only remaining salvage

option. In these cases, you are often dealing with significant glenoid bone deficiency. The
use of augments or grafting may be necessary in order to achieve proper glenoid
positioning, which is critical in restoring optimal function as well as limiting
complications such as scapular notching (Figure 5). Recent studies support the use of
reverse total shoulder arthroplasty for cuff tear arthropathy and suggest improved pain
and function compared to hemiarthroplasty. Leung14 retrospectively compared
differences in pain, function, and ROM in rotator cuff arthropathy patients treated with
reverse total shoulder arthroplasty versus hemiarthroplasty. Significant differences in
pain and function were found at 2 years follow-up favoring reverse total shoulder
arthroplasty. In 25% of the hemiarthroplasty group, severe anterior superior escape was
noted. Young15 et al similarly compared results between reverse total shoulder
arthroplasty and hemiarthroplasty and revealed significant differences in functional
outcomes at 6 months in favor of reverse total shoulder arthroplasty.
In the patient presented, the radiographs demonstrate well preserved glenoid bone
with a well centered humeral head, an AHD < 5mm, and MRI findings of Grade IV fatty
atrophy. We would recommend to this patient, after a trial of non operative care, a
reverse total shoulder arthroplasty which can provide both pain relief and reliable
functional improvement (Figure 6).
Disclosures: Lynn A. Crosby, MD is a consultant for Exactech Bibliography:
1. Neer CS, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 65:1232-1244, 1983.
2. Jensen KL, Williams GR, Russell IJ, Rockwood CA: Rotator cuff tear arthropathy.
J Bone Joint Surg Am 81:1312-1324, 1999.

3. Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear
arthropathy. J Shoulder Elbow Surg 9(3):169-72, 2000.
4. Grammont OM, Baulot E: Delta shoulder prosthesis for rotator cuff rupture. Orthopedics 16:65-69, 1993.
5. Hamada K, Fukuda H, Mikasa M, Kobayashi Y: Roentgenographic findings in massive rotator cuff tears. A long-term observation. Clin Orthop Relat Res 254: 92-96, 1990.
6. Saupe N, Pfirrmann CW, Schmid MR, et al: Association between rotator cuff abnormalities and reduced acromiohumeral distance. Am J Roentgenol 187: 376-382, 2006
7. Goutallier D, Guilloux PL, Postel JM, et al: Acromio humeral distance less than
six millimeter: Its meaning in full-thickness rotator cuff tear. Orthopaedics & traumatology: Surgery & Research 97:246-251, 2011
8. Goutallier D, Postel JM, Bernageau J, et al: Fatty muscle degeneration in cuff
ruptures. Pre- and postoperative evaluation by CT scan. Clin Orthop Relat Res. 304: 78-83, 1994
9. Goutallier D, Postel JM, Gleyze P, et al: Influence of cuff muscle fatty
degeneration on anatomic and functional outcomes after simple suture of full thickness tears. J Shoulder Elbow Surg 12(6): 550-554, 2003.
10. Boileau P, Baque F, Valerio L, et al: Isolated arthroscopic biceps tenotmy or
tenodesis improves symptoms in patients with massive irreparable rotator cuff tears. J Bone Joint Surg Am 89:747-57, 2007.
11. Visotsky JL, Basamania C, Seebauer L, et al: Cuff tear arthropathy: Pathogenesis,
classification, and algorithm for treatment. J Bone Joint Surg Am 86:35-40 (suppl 2)
12. Boyd AD, Aliabadi P, Thornhill TS: Postoperative proximal migration in total
shoulder arthroplasty: Incidence and significance. J Arthroplasty 6(1):31-37, 1991.
13. Koorevaar RC, Merkies ND, Waal-Malefijt MC, et al: Shoulder hemiarthroplasty in rheumatoid arthritis 19 cases reexamined after 1-17 years. Acta Orthop Scand 68:243-245, 1997.
14. Leung B, Horodyski M, Struck AM, et al: Functional outcome of
hemiarthroplasty compared with reverse total shoulder arthroplasty in the treatment of rotator cuff tear arthropathy. J Shoulder Elbow Surg 21:319-323, 2012.

15. Young, SW, Zhu M, Walker CG, et al: Comparison of functional outcomes of
reverse shoulder arthroplasty with those of hemiarthroplasty in the treatment of cuff-tear arthropathy. J Bone Joint Surg Am 95: 910-5, 2013.
16. Ecklund KJ, Lee TQ, Tibone J, et al: Rotator cuff tear arthropathy. J Am Acad
Orthop Surg 15(6):340-349, 2007.
17. Gerber C, Pennington SD, Nyffeler RW, Eng D: Reverse Total Shoulder Arthroplasty. J Am Acad Orthop Surg 17(5):284-295, 2009.
18. Keener JD, Wei AS, Kim HM, et al: Proximal humeral migration in shoulders
with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 91(6):1405-13, 2009.
Figure 1 demonstrates AP radiograph of a 69 y/o M with centered humeral head with significant decrease in AHD.

Figure 2 shows AP radiograph showing decreased AHD with corresponding fatty atropthy of supraspinatus on MRI
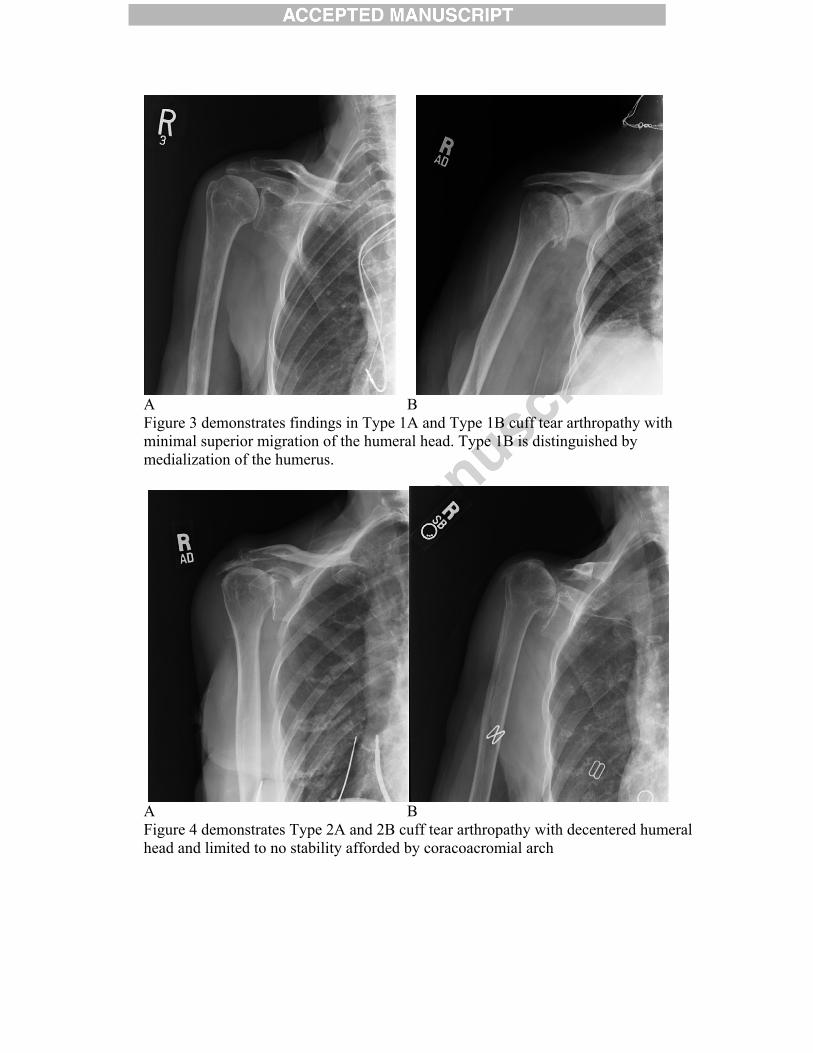
A B Figure 3 demonstrates findings in Type 1A and Type 1B cuff tear arthropathy with minimal superior migration of the humeral head. Type 1B is distinguished by medialization of the humerus.
A B Figure 4 demonstrates Type 2A and 2B cuff tear arthropathy with decentered humeral head and limited to no stability afforded by coracoacromial arch

A B
C Figure 5 shows radiographs of a patient previously treated with hemiarthroplasty for cuff tear arthropathy that developed continued superior migration of the humeral head and glenoid erosion. Image C shows post-op radiographs after conversion to a reverse prosthesis. Notice the superior augmented glenoid baseplate required in order to achieve proper glenoid component positioning.
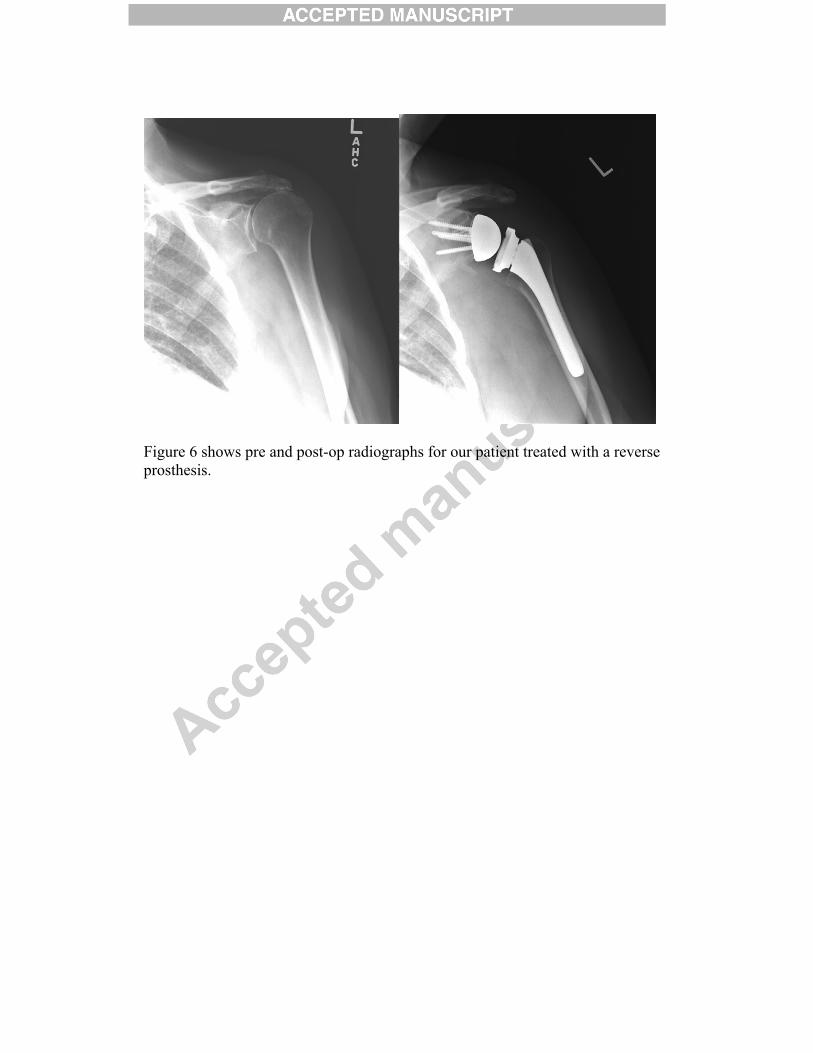
Figure 6 shows pre and post-op radiographs for our patient treated with a reverse prosthesis.



![Shoulder Arthroplasty Americas 2014 [Read-Only]memorialhermann.org/uploadedfiles/_library_files/ironman/management...Irreparable rotator cuff tear is a contraindication to glenoid](https://img.pdfslide.us/doc/110x75/5afc1a527f8b9a32348fdecb/shoulder-arthroplasty-americas-2014-read-only-rotator-cuff-tear-is-a-contraindication.jpg)