Embed Size (px)
Citation preview
1
Cuesta College Athletic Training PO Box 8106 (HWY 1), San Luis Obispo, CA 93403-8106
(805) 546-3225 ph. • (805) 546-3158 Fax
Dear Cuesta Student Athletes and Parents, Cuesta Athletics abides by the medical policies set forth by the California Community College Athletic Association Constitution and Bylaws (CCCAA). Cuesta participates in the Student and Intercollegiate Athletic Accident Insurance program. This program provides secondary (or excess) coverage for injuries sustained while participating in practice or play of intercollegiate athletics. This means that the student-athlete’s primary insurance will be billed first in all cases and the remaining amount, if any, must be submitted to the department’s secondary insurance for payment consideration. The department’s policy has a 52 week period of benefits from the date of the original injury.
In an effort to manage insurance and medical expenses, the Department of Athletics requires that all student-athletes provide evidence of primary medical insurance before commencing intercollegiate practice or play. Failure to provide evidence of insurance coverage may prevent a student-athlete from participating in intercollegiate athletics’ activities. Please ensure that the information on the attached questionnaire is completed accurately.
In the event that the individual is a member of a health maintenance organization, such as Kaiser or Blue Shield HMO, we are required to send the athlete to their primary care physician for treatment. We encourage student athletes to change their primary care physician to the San Luis Obispo area in order to expedite the process should they become injured. This is also beneficial for those athletes who have illnesses that the Student Health Center is not equipped to handle. We hope you can understand that with ever-increasing medical costs we must utilize all possible coverage for proper financial management and at the same time provide good health care.
Listed below are the procedures each student athlete must follow should they become injured during sport participation:
1. All injury evaluation and follow-up care must be done through the Athletic
Training Room (ATR).
2. When the athlete is seen inside the ATR the athletic trainer will write out an injury report form. The athlete will then be given instructions for care of the injury. This may include going to the Health Center or signing up to see one of the team physicians during the clinic hours in the ATR.
3. If it has been determined that the student athlete will require treatment off campus, a
Student Insurance claim form must be filled out. This form must be completed by the athlete and by a Cuesta Athletic Trainer. Any athlete who seeks medical care off campus for an athletically related injury without first consulting with the ATR will not be covered by the Cuesta insurance.
4. If the athlete requires an off campus visit to a medical provider it must be
coordinated through the athlete’s primary insurance. This may mean calling for authorization or visiting the primary care physician.
2
5. If the athlete or the athlete’s parents receive bills or explanation of benefits in the mail, they must be forwarded to:
Student Insurance 10801 National Blvd., Suite 603 Los Angeles, CA 90064
If you do not have the itemized bills and explanation of benefits you cannot proceed with payment from the Student Insurance Group.
6. Each injured athlete’s medical status will be reviewed with the respective head
coach on a regular basis to determine ability to participate. I have enclosed a Medical History Questionnaire along with the Insurance Information sheet. Please return these to the Athletic Training Room or Athletic Director. Remember that the training room must have this information prior to any participation with your Cuesta Team.
I greatly appreciate your time and consideration in this matter. If you have any questions, please call the athletic training room at (805) 546-3225.
Sincerely, Cuesta Athletic Training Staff

3
CUESTA ATHLETIC TRAINING FACILITY GUIDELINES
1. You MUST take a shower before any type of treatment, evaluation, or use of the whirlpools.
2. Sign in if you are receiving treatment (including ice, meds and equipment). 3. DO NOT remove any equipment or supplies from the Athletic Training Facility without
authorization and without signing out. 4. This is a co-ed Athletic Training Facility, proper attire is required. 5. Whirlpool
a. Attire for all: clean swim suit. NO SPANDEX. b. No open wounds or blisters in whirlpool. c. Bring your own towel. d. Whirlpool temp should not be lower than 55°F. e. Dry off before leaving whirlpool area.
6. Absolutely no eating or tobacco use in the Athletic Training Facility unless given permission.
7. Keep cell phone use to a minimum and NEVER when talking to an athletic trainer or physician. Use head phones for your music.
8. Athletic injuries must be evaluated by an Athletic Trainer prior to seeing a physician in the Athletic Training Facility.
9. You must notify the Athletic Training Staff if you plan to seek medical attention for an athletic injury outside of the Athletic Training Facility.
10. Please remember this is a medical facility and we ask that you treat it as such. 11. Refrain from any improper language, horseplay, or behavior that is unbecoming of a
Cuesta Student-Athlete.
Thank You,
Athletic Training Staff

4

5
Cuesta Intercollegiate Athletic Insurance Questionnaire
For Office Use Only Ent Comp
Accident/Injury benefits for athletes are provided on an “excess” basis. This means ATHLETE’S OWN GROUP INSURANCE OR THAT OF THE ATHLETE’S SPOUSE AND/OR PARENT MUST BE BILLED FIRST. Benefits are available from our program only when the Athlete’s coverage is exhausted or does not apply. The following information is essential to assure that expenses are adequately and completely covered by the proper insurance. Inadequate or incomplete answers will delay payment of medical bills and may jeopardize the athlete’s credit rating. No medical expenses will be paid out of institutional funds without a signed, accurate questionnaire on file. It is the athlete’s sole responsibility to keep the information contained in this document current.
ATHLETES INFORMATION ***WRITE CLEARLY; IF WE CAN’T READ IT, WE WON’T ACCEPT IT***
First Name MI Last Name SS# D.O.B. S por t
Local Address Ci t y S t a t e Z i p Phone Cell Phone Student ID #: Year in School: FR SO DO YOU HAVE INSURANCE: YES NO
Please list the Medical Insurance Policies You Have Below
Primary Insurance Secondary Insurance
Subscriber’s Name Subscriber’s SS# Subscriber’s Name Subscriber’s SS#
Employer
Insurance
Employer Insurance
Insurance Billing Address Insurance Billing Address
Insurance Group #
Claims Phone #
ID/Policy # Authorization Phone #
Insurance Group # Claims Phone#
ID/Policy # Authorization Phone #
Dental Insurance Coverage Vision Insurance Coverage
Dental Insurance Dental Subscriber Vision Insurance Vision Subscriber
Dental Policy # Dental Phone # Vision Policy # Vision Phone #
I/We hereby certify that the foregoing answers are true, complete and correct to the best of my/our knowledge. I/we also hereby authorize any Insurance Company, Organization, Employer, Hospital, Physician, Surgeon, Pharmacy, or other health care provider to release any information with respect to injury, treatment, or insurance. A photo static copy of this authorization shall be considered as effective and valid as the original.
Signature of Parent or Guardian Date Signature of Athlete Date
6
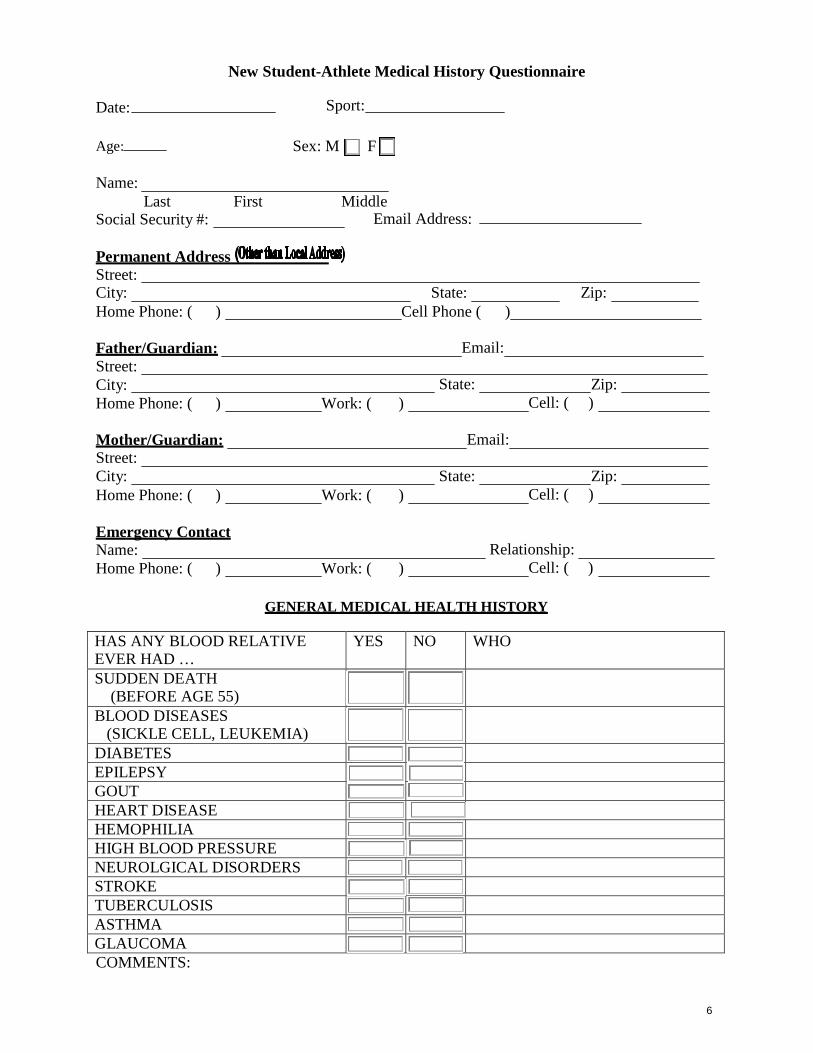
New Student-Athlete Medical History Questionnaire
Date: Age:
Sport: Sex: M F
Name:
Last First Middle
Social Security #: Email Address:
Permanent Address Street: City: Home Phone: ( )
State: Cell Phone ( )
Zip:
Father/Guardian: Street: City: Home Phone: ( )
Work: ( )
Email:
State:
Zip: Cell: ( )
Mother/Guardian: Street: City: Home Phone: ( )
Work: ( )
Email:
State:
Zip: Cell: ( )
Emergency Contact Name: Home Phone: ( )
Work: ( )
Relationship:
Cell: ( ) GENERAL MEDICAL HEALTH HISTORY
HAS ANY BLOOD RELATIVE EVER HAD …
YES NO WHO
SUDDEN DEATH (BEFORE AGE 55)
BLOOD DISEASES (SICKLE CELL, LEUKEMIA)
DIABETES EPILEPSY GOUT HEART DISEASE HEMOPHILIA HIGH BLOOD PRESSURE NEUROLGICAL DISORDERS STROKE TUBERCULOSIS ASTHMA GLAUCOMA COMMENTS:

7
GENERAL MEDICAL HEALTH HISTORY
Do you have or have you EVER had any of the following medical conditions?
YES NO YES NO HIGH BLOOD PRESSURE ASTHMA RHEUMATIC HEART DISEASE
EXERCISE INDUCED ASTHMA
RHEUMATIC FEVER SINUS INFECTION PERICARDITIS NASAL POLYPS ANY HEART DISEASE? NOSE FRACTURE TUMOR, GROWTH, CYST, CANCER
SEIZURE DISORDER/ EPILEPSY
ANY RUPTURED ORGANS? MENINGITIS HEPATITIS MIGRAINE HEADACHES JAUNDICE AMNESIA SICKLE CELL ANEMIA / CARRIER
GOITER, THYROID DISEASE
PLEURISY SKIN DISEASE PNEUMONIA DIABETES POLIO ANEMIA BRONCHITIS ABNORMAL BRUISING TUBERCULOSIS ABNORMAL BLEEDING FREQUENT RESPIRATORY INFECTIONS
GASTROINTESTINAL BLEEDING
MALARIA BLOOD DISEASE MUMPS BLOOD CLOTS MONONUCLEOSIS KIDNEY DISEASE RUBELLA KIDNEY INJURY RED MEASLES / RUBEOLA KIDNEY STONES CHICKEN POX URINARY INFECTIONS ARTHRITIS BLOOD IN URINE EAR INFECTION JOINT INFLAMMATION HEARING DEFECT / LOSS HERPES (ORAL) MUSCULAR DISEASE HERPES (GENITAL) STOMACH ULCER (PEPTIC) SEXUALLY TRANS.
DISEASES
BIRTH DEFECTS EATING DISORDER APPENDICITIS CAR OR AIR SICKNESS GOUT NERVOUS BREAKDOWN CONSTIPATION MENTAL DISORDER HEMORRHOIDS DRUG DEPENDENCY HERNIA COMMENTS:

8
Do you CURRENTLY HAVE any of the following SYMPTOMS or PROBLEMS?
YES NO YES NO FREQUENT HEADACHES ABDOMINAL PAIN VISUAL CHANGES MUSCLE CRAMPS EAR PAIN /HEARING CHANGES
NAUSEA, VOMITING, DIARRHEA
SORE THROAT PENILE DISCHARGE SINUS CONGESTION VAGINAL DISCHARGE BREATHING DIFFICULTY RECTAL BLEEDING RECURRING COUGHING UNUSUAL FATIGUE CHEST PAIN BLOOD IN URINE COMMENTS:
INTERNAL
To your knowledge, were you born with a complete and functioning set of paired organs (eyes, ears, kidneys, ovaries/testicles, lungs)?
YES NO If not, which organs are involved?
Have you ever had surgery to repair or remove any organ (hernia, testicles, appendix, spleen, kidney)?
YES NO If yes, which organ?
Repaired _ Removed Date
Physician: Address:
CARDIAC
YES NO Have you ever felt dizzy, light headed or passed out during or after exercise? Have you ever had chest pain while exercising? Have you ever had irregular heartbeats or heart palpitations? Have you ever been told you have a heart murmur? Have you ever been seen by a heart specialist (cardiologist)?
If Yes? Who: Date: Have you ever had an echocardiogram? Have you ever had a stress (heart) test? COMMENTS:
9
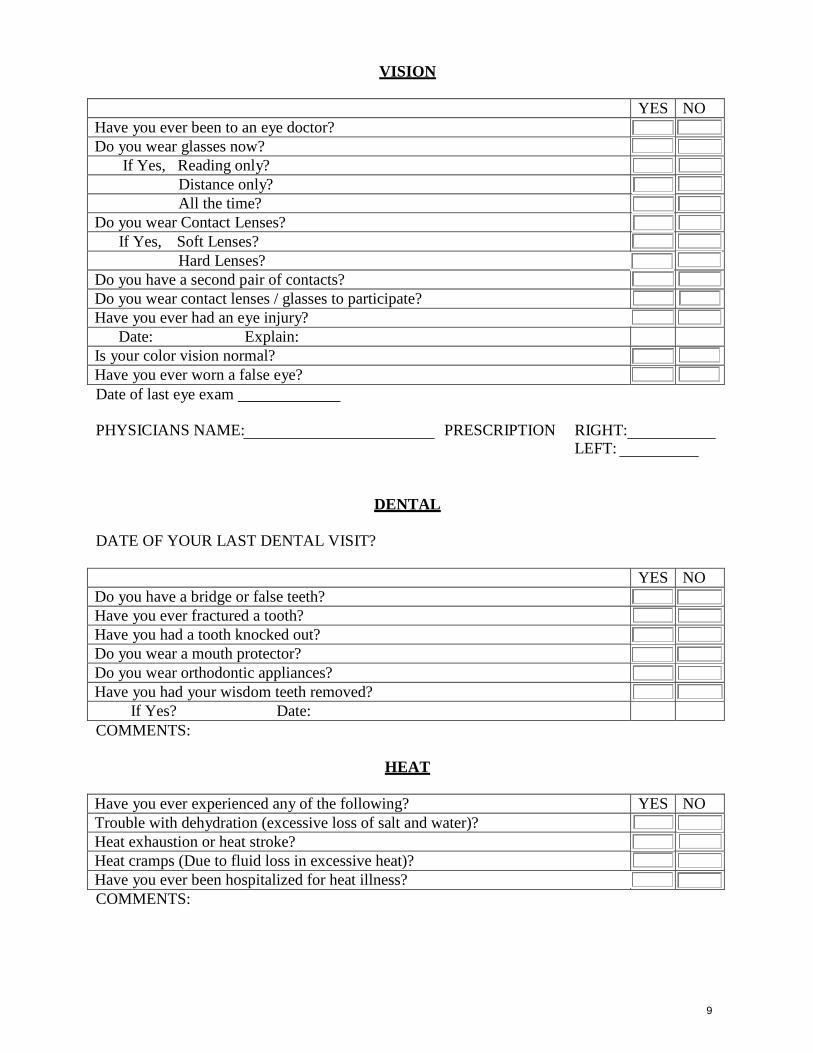
VISION
YES NO Have you ever been to an eye doctor? Do you wear glasses now?
If Yes, Reading only? Distance only? All the time?
Do you wear Contact Lenses? If Yes, Soft Lenses?
Hard Lenses? Do you have a second pair of contacts? Do you wear contact lenses / glasses to participate? Have you ever had an eye injury?
Date: Explain: Is your color vision normal? Have you ever worn a false eye? Date of last eye exam
PHYSICIANS NAME: PRESCRIPTION RIGHT:
LEFT:
DENTAL
DATE OF YOUR LAST DENTAL VISIT?
YES NO Do you have a bridge or false teeth? Have you ever fractured a tooth? Have you had a tooth knocked out? Do you wear a mouth protector? Do you wear orthodontic appliances? Have you had your wisdom teeth removed?
If Yes? Date: COMMENTS:
HEAT
Have you ever experienced any of the following? YES NO Trouble with dehydration (excessive loss of salt and water)? Heat exhaustion or heat stroke? Heat cramps (Due to fluid loss in excessive heat)? Have you ever been hospitalized for heat illness? COMMENTS:
10
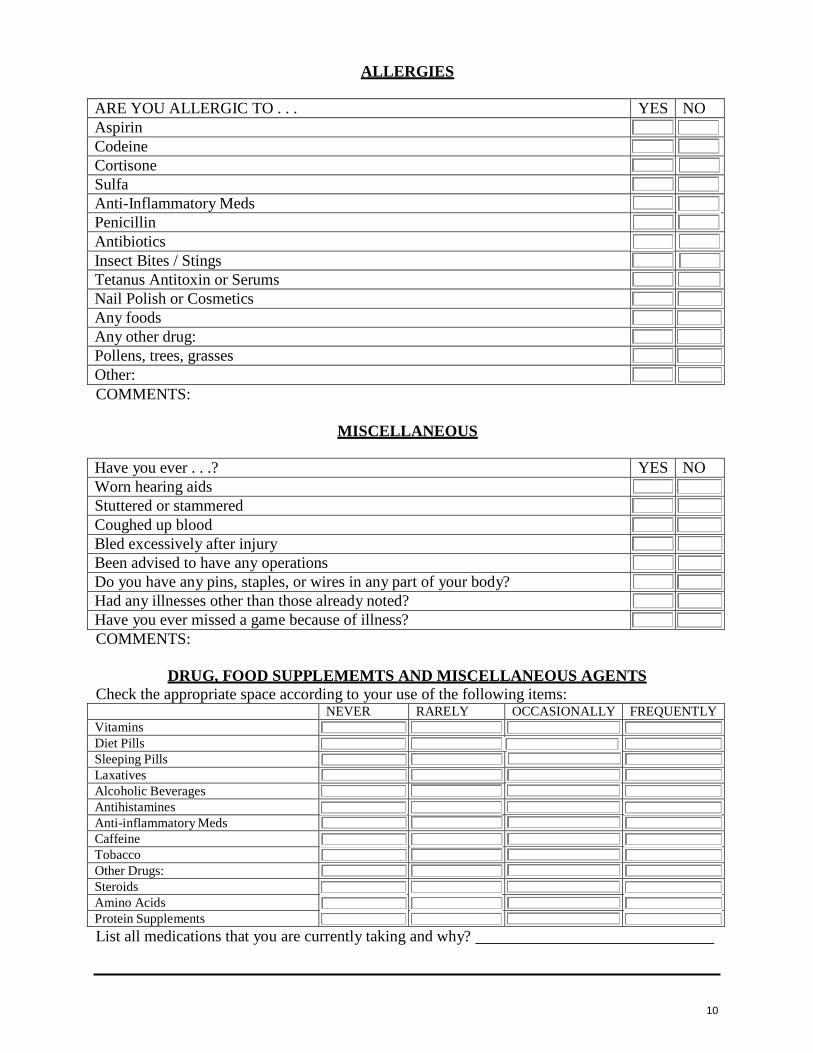
ALLERGIES
ARE YOU ALLERGIC TO . . . YES NO Aspirin Codeine Cortisone Sulfa Anti-Inflammatory Meds Penicillin Antibiotics Insect Bites / Stings Tetanus Antitoxin or Serums Nail Polish or Cosmetics Any foods Any other drug: Pollens, trees, grasses Other: COMMENTS:
MISCELLANEOUS
Have you ever . . .? YES NO Worn hearing aids Stuttered or stammered Coughed up blood Bled excessively after injury Been advised to have any operations Do you have any pins, staples, or wires in any part of your body? Had any illnesses other than those already noted? Have you ever missed a game because of illness? COMMENTS:
DRUG, FOOD SUPPLEMEMTS AND MISCELLANEOUS AGENTS
Check the appropriate space according to your use of the following items:
NEVER RARELY OCCASIONALLY FREQUENTLY Vitamins Diet Pills Sleeping Pills Laxatives Alcoholic Beverages Antihistamines Anti-inflammatory Meds Caffeine Tobacco Other Drugs: Steroids Amino Acids Protein Supplements List all medications that you are currently taking and why?
11
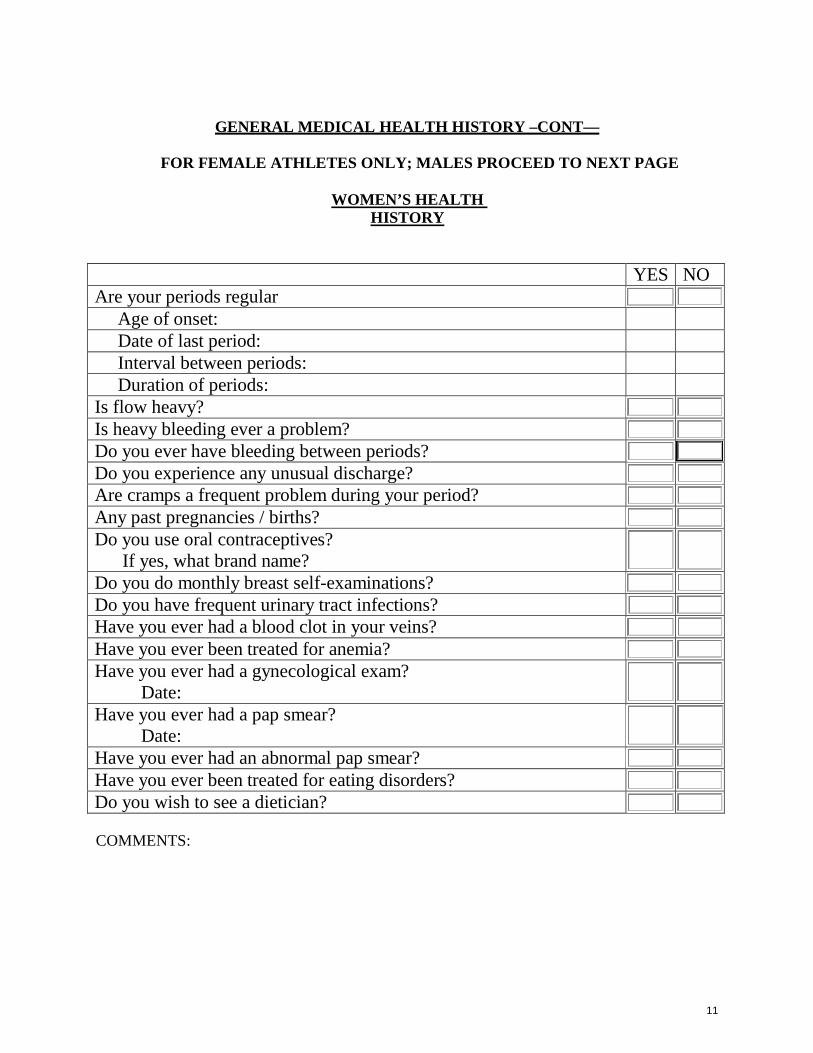
GENERAL MEDICAL HEALTH HISTORY –CONT—
FOR FEMALE ATHLETES ONLY; MALES PROCEED TO NEXT PAGE
WOMEN’S HEALTH
HISTORY
YES NO Are your periods regular
Age of onset:
Date of last period:
Interval between periods:
Duration of periods:
Is flow heavy?
Is heavy bleeding ever a problem?
Do you ever have bleeding between periods?
Do you experience any unusual discharge?
Are cramps a frequent problem during your period?
Any past pregnancies / births?
Do you use oral contraceptives? If yes, what brand name?
Do you do monthly breast self-examinations?
Do you have frequent urinary tract infections?
Have you ever had a blood clot in your veins?
Have you ever been treated for anemia?
Have you ever had a gynecological exam? Date:
Have you ever had a pap smear? Date:
Have you ever had an abnormal pap smear?
Have you ever been treated for eating disorders?
Do you wish to see a dietician?
COMMENTS:

12
ORTHOPEDIC HISTORY QUESTIONAIRE (All Athletes)
PLEASE PLACE A CHECK IN EITHER THE “YES” OR “NO” BOX.
Have you ever injured or consulted a doctor about any injury to . . .
HEAD YES NO DATE Unconscious Dazed / Dizzy Knocked out Concussion Headaches Injections Pains Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practices: # Missed Games: # Other COMMENTS:
NECK YES NO DATE R L Strained Muscle Sprained Ligament Stretches Pinches Disk Injury Dislocations Burners / Stingers Injections Pains Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practices: # Missed Games: # Other
COMMENTS:
13
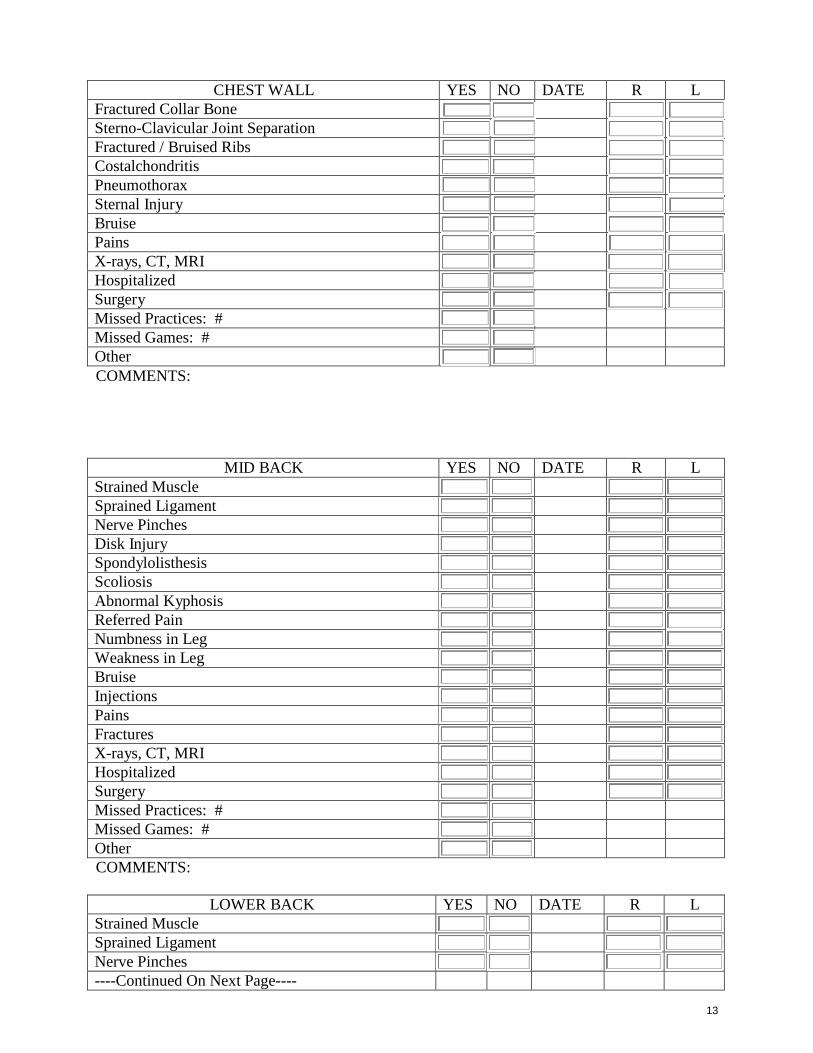
CHEST WALL YES NO DATE R L Fractured Collar Bone Sterno-Clavicular Joint Separation Fractured / Bruised Ribs Costalchondritis Pneumothorax Sternal Injury Bruise Pains X-rays, CT, MRI Hospitalized Surgery Missed Practices: # Missed Games: # Other COMMENTS:
MID BACK YES NO DATE R L Strained Muscle Sprained Ligament Nerve Pinches Disk Injury Spondylolisthesis Scoliosis Abnormal Kyphosis Referred Pain Numbness in Leg Weakness in Leg Bruise Injections Pains Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practices: # Missed Games: # Other COMMENTS:
LOWER BACK YES NO DATE R L
Strained Muscle Sprained Ligament Nerve Pinches ----Continued On Next Page----

14
LOWER BACK --cont YES NO DATE R L Disk Injury Sacroiliac Joint Disorder Referred Pain Pain Down Leg Numbness in Leg Weakness in Leg Bruise Injections Pains Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practice: # Missed Games: # Other COMMENTS:
SHOULDERS YES NO DATE R L Strained Muscle Sprained Ligament A-C Separations Dislocations Partial Dislocations Shoulder Slips out of Place Rotator Cuff Injury Impingement Tendinitis Bursitis Bruise Injections Pain with Overhead Activity Arm Goes “Dead” After Trauma Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practice: # Missed Games: # Other COMMENTS:
15
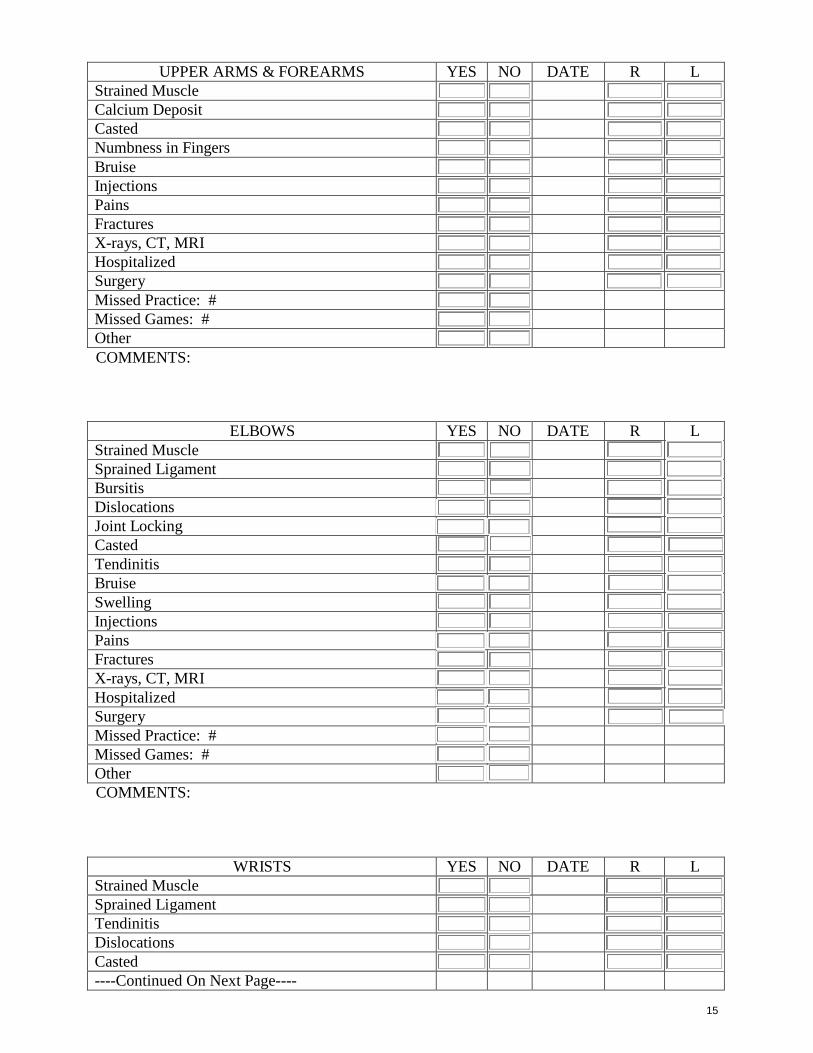
UPPER ARMS & FOREARMS YES NO DATE R L Strained Muscle Calcium Deposit Casted Numbness in Fingers Bruise Injections Pains Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practice: # Missed Games: # Other COMMENTS:
ELBOWS YES NO DATE R L Strained Muscle Sprained Ligament Bursitis Dislocations Joint Locking Casted Tendinitis Bruise Swelling Injections Pains Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practice: # Missed Games: # Other COMMENTS:
WRISTS YES NO DATE R L Strained Muscle Sprained Ligament Tendinitis Dislocations Casted ----Continued On Next Page----

16
WRISTS -- Cont YES NO DATE R L Bruise Cyst Injections Pains Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practice: # Missed Games: # Other COMMENTS:
HANDS YES NO DATE R L Strained Muscle Sprained Ligament Dislocations Casted / Splinted Bruise Cyst Injections Pains Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practice: # Missed Games: # Other COMMENTS:
FINGERS / THUMBS YES NO DATE R L Strained Muscle Sprained Ligament Dislocation Casted Cyst Bruise Injections Pains Fractures X-rays, CT, MRI Hospitalized ----Continued On Next Page----
17
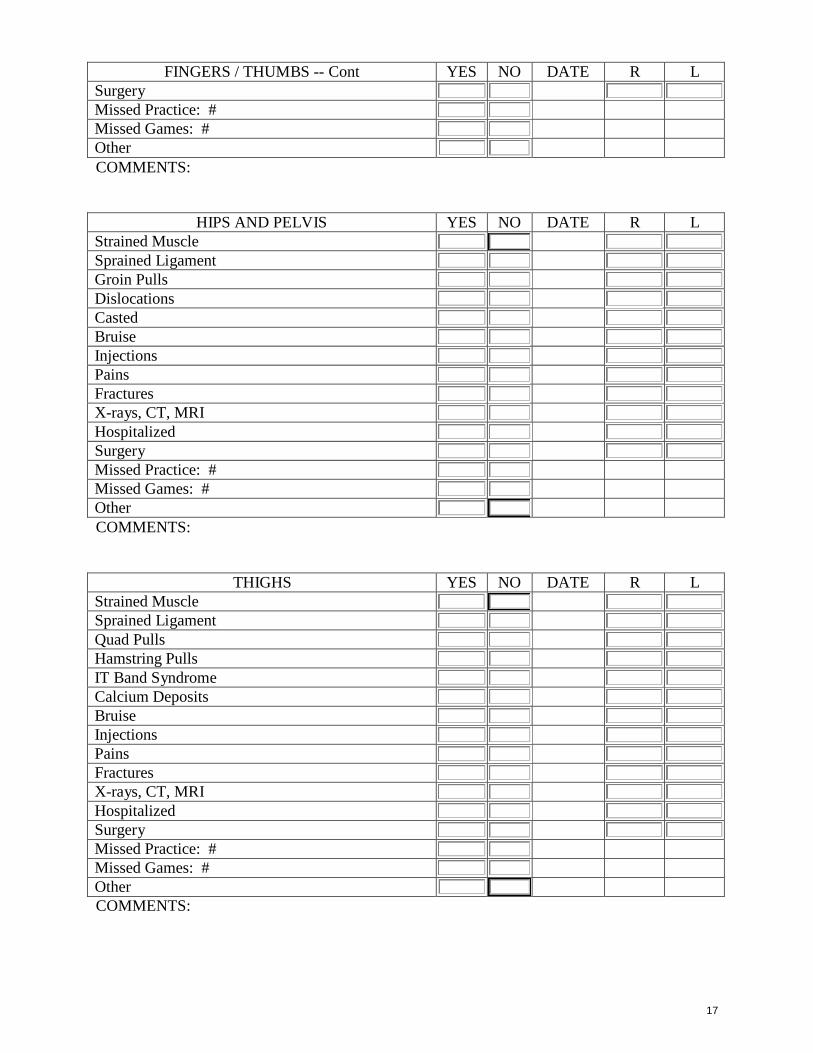
FINGERS / THUMBS -- Cont YES NO DATE R L Surgery Missed Practice: # Missed Games: # Other COMMENTS:
HIPS AND PELVIS YES NO DATE R L Strained Muscle Sprained Ligament Groin Pulls Dislocations Casted Bruise Injections Pains Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practice: # Missed Games: # Other COMMENTS:
THIGHS YES NO DATE R L Strained Muscle Sprained Ligament Quad Pulls Hamstring Pulls IT Band Syndrome Calcium Deposits Bruise Injections Pains Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practice: # Missed Games: # Other COMMENTS:

18
KNEES YES NO DATE R L Strained Muscle Sprained Ligament Torn Ligaments Torn Cartilage Knee Cap Injury Knee Cap Dislocation Osgood Schlatter’s Bursitis Swelling Locking Giving Away Sudden Weakness, Shifting Wear Brace --- Kind? Casted Arthritis Chondromalacia Grinding Tendinitis Jumper’s Knee Bruise Injections Pains Pain with Stairs Pain with Squats Arthrograms Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practice: # Missed Games: # Other COMMENTS:
LOWER LEGS YES NO DATE R L Strained Muscle Sprained Ligament Shin Splints Bursitis Bruise Injections Painful – Tight Calf with Activity Achilles Tendon Injury Stress Fracture Fractures ----Continued On Next Page----

19
LOWER LEGS -- Cont YES NO DATE R L Hospitalized Surgery Missed Practice: # Missed Games: # Other COMMENTS:
ANKLES YES NO DATE R L Strained Muscle Sprained Ligament Dislocations Instability Giving Out Weakness Dislocation Casted / Splinted Bruise Injections Pains Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practice: # Missed Games: # Other COMMENTS:
FEET AND TOES YES NO DATE R L Strained Muscle Sprained Ligament Turf Toe Plantar Fasciitis Bunions Dislocations Casted / Splinted Bruise Injections Fractures X-rays, CT, MRI Hospitalized Surgery Missed Practice: # Missed Games: # Other COMMENTS:

20
YES NO Have you had or do you have any other medical problems or injuries not listed on this form?
Do you have any medical or health problems that you are currently receiving medical treatment for?
Is there any reason that you are not able to participate in athletics? Are there any additional health problems you would prefer to discuss privately with our team physician?
IF ANY OF THE ABOVE QUESTIONS WERE ANSWERED YES, PLEASE COMMENT:
List any special protective equipment you require or would like to have provided:
The undersigned, here within,
A. Understands that he/she must refrain from practice or play during medical treatments until he/she is discharged from treatment or given a written permit by the attending physician to resume participation.
B. Understands and will abide by the Athletic Training Facility Guidelines.
C. Understands that his/her having passed the physical examination does not necessarily
mean that he/she is physically qualified to engage in athletics, but only that the examiner did not find a medical reason to disqualify him/her.
D. Fully realizes the Cuesta College, San Luis Obispo, Department of Athletics cannot
be held responsible for any previous medical condition(s) that he/she might have.
E. Understands permission to participate in intercollegiate athletics will not be granted until all subsequent forms are completed and have successfully passed the physical examination.
F. Certifies that the answers to the health history questionnaire correct and true.
SIGNATURE: DATE:
Upon completion of this Medical History form, it will be reviewed and signed by a certified athletic trainer.
SIGNATURE:
NATA Certified Athletic Trainer
DATE:

21
Cuesta College Athletic Training PO Box 8106 (HWY 1), San Luis Obispo, CA 93403-8106
(805) 546-3225 ph. • (805) 546-3158 Fax
Directions: Medical Consent
I. Please read carefully and sign the following consent forms. If you are under 18 years of age, your parents must also sign.
II. If you choose to refuse to sign any of these consent forms, please write “Refuse to Sign”, the date, and your signature. Notify your athletic trainer.
III. This document will remain in effect for one year of signing and any portion may be revoked at the discretion of the student-athlete by notifying your athletic trainer.
Basic Content: I. Medical Consent: Allows athletic trainers, health center staff and
physicians to provide any medical and personal counseling services needed while a student-athlete at Cuesta College, San Luis Obispo.
II. Release of Medical Information to the Media: Allows those listed to release information concerning your injuries to the media.
III. Release of Information to Professional Sports: Allows those listed to release any and all information concerning you, including medical records and other items listed.
IV. Assumption of Risk: Acknowledges that all athletic activity affords a certain amount of risk of injury and that you are aware of these risks and the rules of your sport intended to minimize these risks.
V. Blood Borne Pathogens: Acknowledges that exposure and transmission of Blood Borne Pathogens is possible through athletics and that you are willing to assume responsibility.
I. Medical Consent
I hereby grant permission to the Cuesta College, San Luis Obispo intercollegiate team physician, student health center and/or their consulting physician(s) to render to my son or daughter or myself any treatment or medical or surgical or personal counseling care that they deem reasonably necessary to the health and well-being of the student-athlete.
22
I also hereby authorize the athletic training staff at Cuesta College, San Luis Obispo who are under the guidance of the team physician, to render to my son or daughter or myself any preventative, first aid, rehabilitative or emergency treatment that they deem reasonably necessary to the health and well-being of the student-athlete.
Also, when necessary for executing such case, I grant permission for hospitalization at an accredited medical facility.
If the student-athlete is under 18 years of age, a parent or guardian signature is required.
Date:
Signature of Student-Athlete
Date:
Signature of Parent or Guardian
II. Authorization for release of Medical Information to the Media
This is to authorize Cuesta College, San Luis Obispo athletic training staff and team physicians to release medical information of my son or daughter or myself to the Cuesta Sports Information Department to provide media outlets for any information concerning illness or injury relative to my past, present, or future participation in intercollegiate athletics at Cuesta.
If the student-athlete is under 18 years of age, a parent or guardian signature is required.
Date:
Signature of Student-Athlete
Date:
Signature of Parent or Guardian
23
III. Authorization for Release of Medical Information for Employment in Professional Sports
I, , hereby authorize and request the Cuesta College San Luis Obispo Athletic Training Department to supply to professional athletic teams, their scouts, representative agents, athletic trainers, physicians, or employees, any and all medical information concerning or having bearing upon my participation in intercollegiate athletics at Cuesta College, San Luis Obispo. This authorization shall include, but not limited, to any and all information within their knowledge, or contained in any medical records under their supervision or control concerning my physical condition, illness, injuries, and any treatment, hospitalization, examinations, x-rays, and to make such reports to such persons or organizations concerning myself that they may request; and I hereby fully discharge all parties to whom this authorization extends from any and all privilege in connection with the disclosure of information included in this authorization.
If the student-athlete is under 18 years of age, a parent or guardian signature is required.
Date: Signature of Student-Athlete
Date: Signature of Parent or Guardian
IV. Assumption of Risk
Participation in sport requires an acceptance of risk of injury. Athletes rightfully assume that those who are responsible for the conduct of sport have taken reasonable precaution to minimize such risk and that peers participating in the sport will not intentionally inflict injury upon them.
Attempts to legislate safety via rule books and equipment standards, while helpful, is seldom entirely effective. Relying on officials to enforce compliance with rules is also insufficient. Compliance with rules implies respect on everyone’s part (student-athlete, coach, athletic trainer, physician, and athletic director) for the intent and purpose of rules and guidelines.

24
I understand that by voluntarily participating in athletics at the collegiate level, I am undertaking a non-controllable risk, which may result in injury, illness or death.
I understand sickness and/or injuries are common in all athletics and that Cuesta College, San Luis Obispo Athletics Department will provide the most reasonable medical coverage in order to reduce the severity of such illness and/or injury. The administration, coaches, and athletic trainers will equally provide to each student-athlete, equipment required to produce the safest possible intercollegiate athletic environment regardless of age, sex, race, or religion.
I acknowledge and understand that the college is not providing transportation and it is my responsibility to arrange for any transportation to and from the activity. If the college is providing transportation but I do not use the transportation, I am responsible to make my own transportation arrangements and the college assumes no responsibility or liability of any kind.
I have read the above assumption of risk statement. I understand that there are certain inherent risks involved while participating in intercollegiate athletics. I acknowledge the fact these risks exist and I am willing to assume responsibility for such risks while participating at Cuesta College, San Luis Obispo.
If the student-athlete is under 18 years of age, a parent or guardian signature is required.
Date: Signature of Student-Athlete
Date:
Signature of Parent or Guardian

25
V. Blood-Borne Pathogens and Intercollegiate Athletics (Copyright, 1997, by the NCAA)
Blood-Borne pathogens are disease-causing microorganisms that can be potentially transmitted through blood contact. The blood-borne pathogens of concern include (but are not limited to) the hepatitis virus (HBV) and the human immunodeficiency virus (HIV). Infection with these viruses has increased throughout the last decade among all portions of the general population. These diseases have potential for catastrophic health consequences. Knowledge and awareness of appropriate preventative strategies are essential for all members of society, including student- athletes.
The particular blood-borne pathogens HBV and HIV are transmitted by practicing risky unprotected sexual contact (heterosexual and homosexual), direct contact with infected blood or blood components, and prenatally from mother to baby. Experts have concurred that the risk of transmission on the athletic field is minimal.
HBV is a blood-borne pathogen that can cause infection of the liver. Many of those infected will range from no symptoms to a mild flu-like illness. One third will have severe hepatitis, which cause the death of one percent of that group. Currently, in the United States there are one million chronic carriers of HBV. Chronic complications of HBV infections include cirrhosis of the liver and liver cancer. The incidence of HBV in student-athletes is presumably low, but those practicing risky behaviors off the athletic field have an increased likelihood of infection (just as in the case of HIV). An effective vaccine to prevent HBV is available and recommended for all college students by the American College Health Association.
The Acquired Immunodeficiency Syndrome (AIDS) is caused by HIV, which infects cells of the immune system and other tissues such as the brain. Some of those infected will remain asymptomatic for many years. Others will more rapidly develop the manifestation of the HIV disease (i.e. AIDS). Some experts believe virtually all persons infected with HIV will eventually develop AIDS, which is fatal. In the United States there are 40,000 to 50,000 newly infected persons each year. There are 1.5 million infected persons in the United States. The risk of infection is
26
increased by having unprotected sexual intercourse and sharing IV needles. Currently, there is no vaccination available to prevent HIV.
HBV is a more “sturdy/durable” virus than HIV and is more highly concentrated in blood. HBV is more likely to be transmitted by exposure to infected blood, particularly with needle-stick exposure, but also exposure to open wounds and mucus membranes. The risk of transmission for either HBV or HIV is considered minimal; however, most experts agree that the specific epidemiological and biologic characteristics of the viruses make them a realistic concern for transmission in sports with sustained close physical contact.
Cuesta College, San Luis Obispo athletic training staff acknowledges the risks and utilizes Universal Precautions as recommended by the Center for Disease Control, OSHA and the NCAA Sports Medicine Handbook to minimize the risk of blood-borne pathogen exposure and transmission on the context of athletic events and treatment guidelines for the health care of student-athletes. I have carefully read and fully understand the risk of blood- borne pathogens exposure and transmission.
If the student-athlete is under 18 years of age, a parent or guardian signature is required.
Date:
Signature of Student-Athlete
Date: Signature of Parent or Guardian


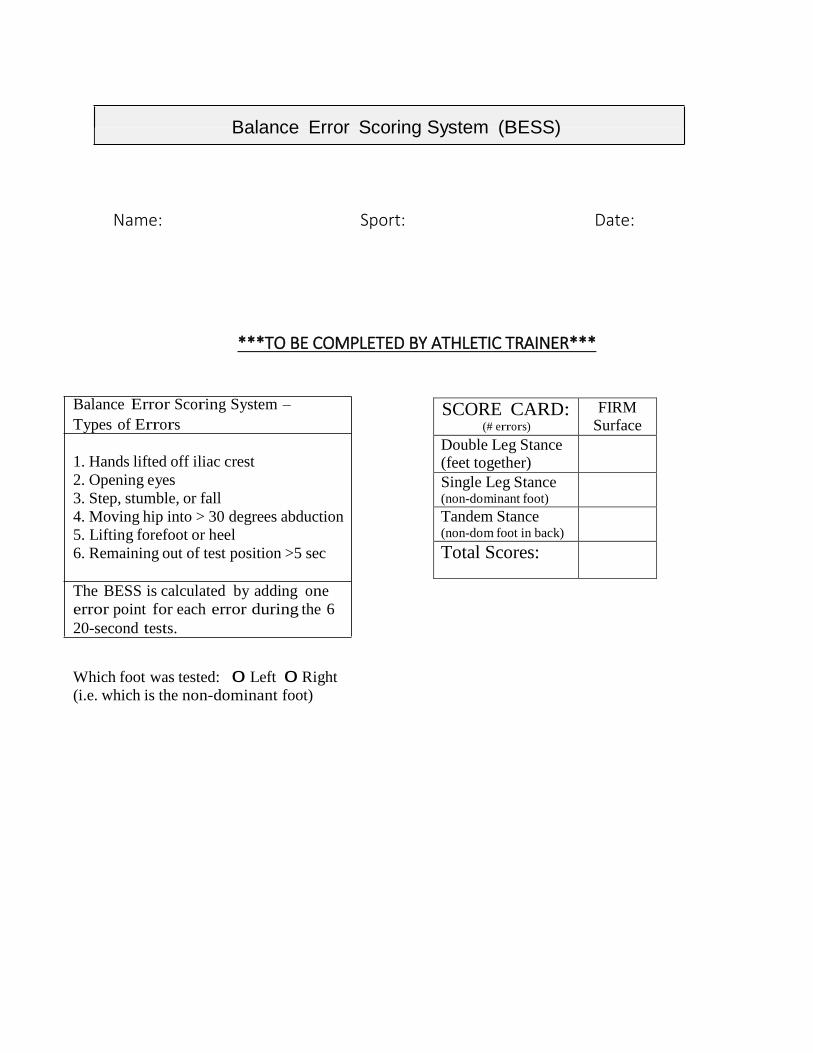
SCORE CARD: (# errors)
FIRM Surface
Double Leg Stance (feet together)
Single Leg Stance (non-dominant foot)
Tandem Stance (non-dom foot in back)
Total Scores:
Balance Error Scoring System (BESS)
Name: Sport: Date:
***TO BE COMPLETED BY ATHLETIC TRAINER***
Balance Error Scoring System –
Types of Errors
1. Hands lifted off iliac crest
2. Opening eyes
3. Step, stumble, or fall
4. Moving hip into > 30 degrees abduction
5. Lifting forefoot or heel
6. Remaining out of test position >5 sec
The BESS is calculated by adding one
error point for each error during the 6
20-second tests. Which foot was tested: 0 Left 0 Right
(i.e. which is the non-dominant foot)