Embed Size (px)
Citation preview

CTE AND MRE:CTE AND MRE:WHO, HOW, WHAT, WHYWHO, HOW, WHAT, WHY
Joel F. Platt, M.D.University of Michigan

OBJECTIVESOBJECTIVES
Review basics of performing CTE and MRE
Identify key imaging findings with CTE and MRE
Discuss factors that may influence choice of CTE vs MRE

IMAGING OF SMALL BOWELIMAGING OF SMALL BOWEL
NeoplasmObstructionIBDIschemiaTrauma

CTECTEWHAT IS IT?WHAT IS IT?
MDCTSingle or dual phase scanningLow attenuation oral contrastIV contrastAxial and 3DFocus on bowel

CTECTE
CT exam focused on small bowel
CT exam optimized for small bowel

CTE ORAL CONTRASTCTE ORAL CONTRASTIMPORTANT CHOICEIMPORTANT CHOICE
IntrinsicWaterLAOCMilk and others

CTE TECHNIQUE: CTE TECHNIQUE: ORAL CONTRASTORAL CONTRAST
VoLumen administration:– 6 hours fasting prior to scan– 1350 ml 3 bottles of 450 ml over 90 min
• 450 ml 90 min• 450 ml 45 min• 225 ml 20 min• 225 ml 5 min
Young B et al; JCAT 2008Kuehle CA et al; AJR 2006
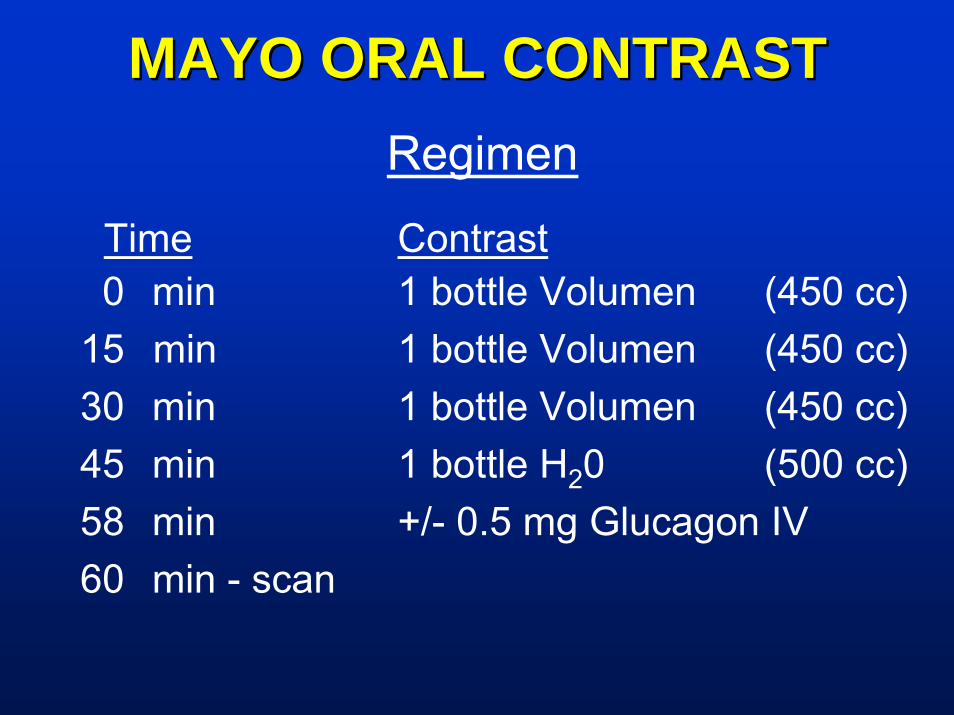
MAYO ORAL CONTRASTMAYO ORAL CONTRASTRegimen
Time Contrast0 min 1 bottle Volumen (450 cc)
15 min 1 bottle Volumen (450 cc)30 min 1 bottle Volumen (450 cc)45 min 1 bottle H20 (500 cc)58 min +/- 0.5 mg Glucagon IV60 min - scan
““SELFSELF”” PREPPED PATIENTPREPPED PATIENT
A new observation with VoLumen not seen with bright oral agentsSeen with active bowel disease Crohns, infections, malabsorption, obstructionGives appearance of good VoLumen prep

CTE DELAY TIME CTE DELAY TIME
40 sec vs 70 secNo advantage for CTE1 Phase is sufficient70 sec preferred
Vandenbroucke et al, Acta Radiology 2007

CTECTEOPTIMAL SCAN DELAYOPTIMAL SCAN DELAY
50 sec delay 14 sec after aortic peakEnteric phase better than arterial5 ml/sec injection rate
Schindera et al, Radiology 2007

RADIATION DOSE IN CTERADIATION DOSE IN CTE
Often young patients
Often need repeat imaging
Low dose CTE vs MRE

MRE PROTOCOL (1.5 T)MRE PROTOCOL (1.5 T)3-plane localizerAxial and coronal T2W single-shot fast spin-echo SSFSE (HASTE)axial & coronal steady-state free precession FIESTA (B-TFE)Coronal pre and post contrast 3D SPGR-LAVA (THRIVE) with fat-saturationAxial delayed postcontrast 2D SPGR-LAVA (THRIVE) with fat-saturation

MR PULSE SEQUENCESMR PULSE SEQUENCEST2-weighted (single –shot techniques)– HASTE, SSFSE, SSTSE– Fat suppression? Improves conspicuity of ↑ SI
bowel wall and mesenteric fat, but diminished discrimination of bowel wall
Contrast enhanced 3D gradient echo sequence– FAME, VIBE, THRIVE– Fat suppression: yes
May use balanced GRE– FIESTA, TruFISP, Balanced FFE
Employ parallel imaging

MRE MRE PedsPeds Protocol Protocol –– PrescanPrescanNPO – only if sedated examPt arrives 90 minutes before exam start timeOral prep:– 2-3 bottles of VoLumen “CT” oral contrast material over 60-90
minutes– 8 oz water immediately prior to scan
• VoLumen & water are both biphasic (T1W hypo- intense & T2W hyperintense)
Glucagon administered as split dose (smooth muscle relaxant) – 0.25-0.5 mg IV immediately prior to localization– 0.25-0.5 mg IV immediately prior to postcontrast imaging
MRE MRE PedsPeds Protocol Protocol –– SequencesSequencesC.S. Mott Children’s Hospital (1.5T)– 3-plane localizer & parallel imaging reference scans– T2W single-shot fast spin-echo (SSFSE)
• axial & coronal– Balanced steady-state free precession (SSFP)
• axial & coronal– Diffusion-weighted echo-planar (EPI)
• axial– T2W fast spin-echo (FSE) with fat-saturation
• axial– Dynamic postcontrast 3D SPGR (THRIVE) with fat-saturation
• coronal– Delayed postcontrast 3D SPGR (THRIVE) with fat-saturation
• axial & coronal

MDCT OF IBDMDCT OF IBD
DiagnosisDifferentialActivityComplications
CTE FOR IBD WHY NOW?CTE FOR IBD WHY NOW?
16 slice or beyond MDCT
Water/Volumen for oral contrast
Volume visualization/workstation
Aggressive medical therapy for IBD

CTECTEGOOD QUESTIONSGOOD QUESTIONS
Known IBD, ? disease activityKnown stricture,? medical vs surgical treatment
Complications from IBD

CROHNCROHN’’S STRICTURES STRICTUREMANAGEMENTMANAGEMENT
Inflammatory– Medical therapy – steroids, anti-TNFA
agents---- side effects
Fibrotic– Surgical treatment

CTECTEQUESTIONABLE INDICATIONQUESTIONABLE INDICATION
R/O IBDShort term F/U after treatmentDifferentiate types of bowel disease

MDCT FOR IBDMDCT FOR IBD
Mucosal/wall enhancement
Local vascularity
Extraluminal complications
Anastomotic disease

CTE OF CROHNS ACTIVECTE OF CROHNS ACTIVE
Mural enhancementMural stratificationThick bowelSTSEngorged vasa rectaObstruction
Paulsen et al, Radiographics 2006

CTE FEATURES OF ACTIVE CTE FEATURES OF ACTIVE CROHNS DISEASE CROHNS DISEASE
Mural thickening: – > 3 mm in distended bowel
Mural hyperenhancement: – Visual assessment in comparison with adjacent loops
Mural stratification: – Enhancing mucosa and serosa with hypodense
submucosa due to edemaWall thickening associated with hyper-enhancement is the most sensitive sign of active disease*
*Booya F et al; Radiology 2006

CTE OF ACTIVE IBDCTE OF ACTIVE IBD
Mesenteric changes:– Mesenteric fat stranding– Prominence and engorgement of vasa
recta “comb sign”Mesenteric changes are the most specificCT finding for active CD and correlate with levels of C reactive protein*
*Colombel JF et al; Gut 2006

CTE IN CROHNS DISEASECTE IN CROHNS DISEASECTE has reported sensitivity of 80 – 90% for detection of active Crohn disease1
Higher specificity as compared to capsule endoscopy (89% vs 53%)2
CTE can identify intramural inflammation in 24% of patients with normal appearing mucosa on ileoscopy3
CTE changed gastroenterologist’s impression of steroid benefit in 61% of patients4
Booya A et al; Abdominal Imaging 2008 2. Solem CA et al; Gastrointest Endosc 2008 3. Siddiki H et al RSNA 2008 4. Higgins PD et al Inflamm Bowel Dis 2008

CTE CTE MONITOR CROHNMONITOR CROHN’’S STATUSS STATUS
40 exams (20 patients)CTE correlated with symptoms in 80%Symptoms could get worse with stable/improved CTERadiation/MRE
Haara et al, AJR 2008

CTE vs SURGICAL PROOFCTE vs SURGICAL PROOF
36 patientsStricture, Fistula, AbscessCTE highly accurate compared to proofSearch for multiple fistula and strictures
Vogel et al, Dis Colon Rectum 2007

MRE ADVANTAGESMRE ADVANTAGESNo ionizing radiation– Young patients– Life long disease– Life long imaging
Complete evaluation– Bowel– Extraenteric
Superior contrast resolution

MRE DISADVANTAGESMRE DISADVANTAGES
Scanner timeLabor intensiveExpenseWorse spatial resolution than CTMore unpredictable

CTE vs MRECTE vs MRE
26 patients CTE = MRE for more advanced dzMRE better for milder dzComplications seen by both
Low, JMRI 2000

CTE vs MRECTE vs MREIppolito et al. (Abdom Imaging 2009):– Compared MRE vs. CTE agreement in 29 pts
• wall thickening (kappa=1)• mucosal hyperenhancement (kappa=1)• CTE superior to MRE for detection of mesenteric fibrofatty proliferation &
lymphadenopathy (p<0.05)• MRE superior in visualization of fistulae
–– CONCLUSION:CONCLUSION: MRE is accurate in monitoring activity of CD compared to CTE and may be considered an alternative to CTE in assessing degree of CD and evaluating therapeutic effectiveness

CTE vs MRECTE vs MRESiddiki et al. (AJR 2009):– 30 pts with suspected Crohn evaluated with CTE, MRE, and
ileoscopy– MRE & CTE sensitivities for detection of small bowel Crohn disease
similar (90.5% vs 95.2%; p=0.32)– MRE & CTE both identified 8 cases active small bowel inflammation
in which endoscopy was normal
–– CONCLUSIONS:CONCLUSIONS:• MRE & CTE have similar sensitivities for detecting active small bowel
inflammation• Cross-sectional enterography provides added information to endoscopy
CTE vs MRECTE vs MRELee et al. (Radiology 2009):– 31 pts with suspected Crohn evaluated with CTE, MRE, SBFT, and
ileoscopy– No differences in ability to detect active terminal ileitis between
modalities (p>0.017)– Sensitivity for detection of extra-enteric complications were higher for
CTE / MRE (100% for both, p<0.001)
–– CONCLUSION:CONCLUSION: Because MRE has a diagnostic effectiveness comparable to CTE, this technique has potential to be used as a radiation-free alternative for evaluation of patients with CD

CTE vs MRECTE vs MRE
Learning curveTechniqueResolutionCostRadiationAvailability

CTE/MRE SMALL BOWELCTE/MRE SMALL BOWELSUMMARYSUMMARY
With proper technique CTE/MRE can provide comprehensive evaluation of small bowelIncreasing role of imaging for obstruction, ischemia and IBD