Embed Size (px)
Citation preview
![Page 1: CT Study Req V3 - ERDocs.ca€¦ · CCTH Rule above if ordered Temporary McMaster-NHS CT Head Rule Study SCS Only Proceed to exclusion NO YES [ ] YES (CT head recommend) [ ] NO (CT](https://reader033.pdfslide.us/reader033/viewer/2022052001/6013a5d7b031de733a304ef6/html5/thumbnails/1.jpg)
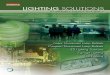
s NI AGAR A H EALTH SYSTEMENext available appointment at any NHS CT SitePLEASE FAX TO LOCATION NEAREST PATIENT'S RESIDENCE
Or Choose: trcNc 905-378-4647 Fax 905-358-7438trSCG 905-378-4647 Fax905-684-6990dWHS 905-378-4647 Fax905-732-9537
INCOMPLETE FEOI,JISITIONS WILL BE RETURNED
CT ConsultationPlease PFIINT patient infomation below.
RequisitionPlease do not imprint.
il
T
Sufiame First Name E ouDaiient
E lnpalient site
-
FllRm
-EEn sit"-E Relerral siie
-
FllRm
D.O_8. Sex H.C.N.
Relerring Physician Physicians to receive copies of report
City Seterring PhysicianPhone (home) Name
sIB
Claim # Dale of Accident dd/mm/yy Address
Employer when accident happened s.t.N. city Postaloode
Employer's Address
AllergyHislory
Head Chest Abdomen / Pelvis RetroDeritoneum OtherE Routine E Routine E Liver E Adrenals E Extremity lsrerlly a'e:;
E Sinus E High Resolution E Pancreas E Kidneys ESpine -.r';' t
E Orbits E Pulmonary Embolus E Spleen tr E Bony Pelvis
tr tr EAorta tr E Neck
tr tr DRenal Colic tr n
BELEVANT PBEVIOIIS IMAGING STUDIES MUST
Historv and Findinqs - include previous imaqinq and laboratory studies Renal History
Physician's Signature:
Urgent Result Contact Number:
Does your patient have any history of renalimpairment or dialysis treatment? EYes ENoDoes your patient have any history of hypenension,or vascular disease? trYes trNo
Does your patient have diabetes? trYes trNo
lf yes are they on Metformin? trYes trNoDoes your patient have anyfamily history of renal disease? trYes trNo
Yqur patient may require contrast media duringthis study, it ihe answer is "Yes" to any ol theabove, or your patient is older than 70 yrs.,please provide a creatinine level performedwithin the last 2 months.
Creatinine- pmol/L or GFB
-WTIS Clinical lndicalion tor Scan Radioloqist Protocol Date Requisition Received
tr Cancer Staging / Diagnosistr Other
2 3 4 D E (office use only)
l N.:
Date Notilied
r.l
Appointment: DayI I Month[ ] Year[ ] Time: HRS WHS tr GNG D SCG tr86 Bev. 1212011
Canadian CT Head Rule Has to be completed for all non contrast Head CT
[ ] Not a trauma
[ ] GCS <13
[ ] Age <16
[ ] Anticoagulants or Bleeding D/O [ ] Open Skull #
[ ] GCS <15 2hrs post injury [ ] Suspected Open or Depressed Skull # [ ] Any sign of Basal Skull # [ ] Age 65yr or older [ ] Vomiting 2 or more times [ ] Amnesia 30min before impact [ ] Dangerous Mechanism (Pedestrian vs car, MVA with ejection, Fall 3ft or more)1.
CCT
HR E
xclu
sion
Crit
eria
2. A
ny E
xclu
sion
s M
et?
3. W
as C
CTHR
Met
?
Allergy History
Must Complete CCTH Rule above if ordered
Temporary McMaster-NHS CT Head Rule Study SCS Only
Proceed to exclusion
NOYE
S
[ ] YES (CT head recommend)
[ ] NO (CT head not recommend)
Important Note: This req is part of a NHS & McMaster NRC Study. The CT head will be performed if ordered regardless of the CT Head Rule. Clinical judgment is paramount.
[ ] Excluded from Rule






![Olcott...Multiple Sclerosis Mumps Osteoporosis Pacemaker Yes Cl Yes [2 Yes Yes Yes [2 Yes Parkinson's Disease [2 Yes ... Yes [2 Yes D Yes Yes C] Yes Yes Rheumatoid Arthritis Yes HABITS](https://img.pdfslide.us/doc/110x75/5f437d8dde860906673fc43a/olcott-multiple-sclerosis-mumps-osteoporosis-pacemaker-yes-cl-yes-2-yes-yes.jpg)
















![AProfileofCasesofGestationalTrophoblasticNeoplasiaat ...downloads.hindawi.com/journals/isrn/2011/453190.pdfYes/No Reg/Irreg Yes/No Cured/need CT and Gynaecologists) guidelines [2]](https://img.pdfslide.us/doc/110x75/5f0f79d97e708231d44459e4/aproileofcasesofgestationaltrophoblasticneoplasiaat-yesno-regirreg-yesno.jpg)