-
8/8/2019 CT SelfEsteem
1/9
Advanc es in P sy ch ia tr ic T re atm ent ( 998 ),o l. 4 , p p.
2 96 -304
Cognitive therapy in the treatment oflow self-esteemMelanie J. V
. Fennell
B eck 's cognitive therapy o riginally dev eloped as asho rt -t
erm t re atmen t f or dep re ss ion (Beck e t a l, 1979) .It has
been shown to be effective with a range ofoth er disorders
including panic d isorder, generali sed anx ie ty d isor de r, soc
ia l phobi a, e at ing d isor de rsand sexual dysfunction (Roth et
al, 1996). It isprom ising in the treatm ent of yet m ore
disorders,many of which have traditionally been thoughtr el at
ively impe rv ious to psychothe rapy , f or example,bipolar
disorder, chronic fatigue and psychosis(C lark & Fairbu rn, 19
97). H ow ever, not ev eryoneresponds w ell to short-term cognitive
therapy. Inparticular, it has been proposed that people withm
ultiple, chronic problem s that are apparentlyex pre ssio ns o f p
erso nality , rath er th an tempo raryresp on ses to a dv erse life
ex perien ces, req uire moreex ten ded th erap y (B eck ef al, 1 99
0).L ow self-esteem (o ften a majo r fo cu s o f in teres t ino
ther p sychothe rapi es ) has been r el at ively neg le ct edin
cognitive therapy. This is perhaps because it isneither a specific
psychiatric disorder nor ap ers on alit y d is ord er. Rath er, it
eme rg es a s a n a sp ec to f, co nseq uen ce o f o r v uln erab
ility facto r fo r m an ypresenting problem s. For exam ple, a neg
ative self-image i s c ent ra l t o dep re ss ion ( aspe ct ), but
cha ra ct eri st ic al ly evapo ra te s a s mood l if ts .A l te
rnat ively, s el f-d en ig ra tio n may o cc ur o nly onc e a s pe
cific d is ord er,su ch as g en eralised an xiety d iso rd er, h as
p ersistedo ver tim e (co nseq uen ce) an d may impro ve o n its
ownas the presenting problem is addressed. Low self-e ste em may p
re dis po se to a ra ng e o f o th er d iffic ul tie
s(vulnerability factor), such as depression ands uic id alit y, e
atin g d is ord ers a nd s oc ia l a nx ie ty . Hereit m ay hinder
pro gress in treatm ent and p ersist evenafter presentin g problem
s have been successfullyresolved.I aim : (a) to introduce
practitioners u nfam iliarw ith the approach to the concepts and m
ethods of
co gn itiv e th erap y; (b ) t o s how read ers more fam iliarw
ith cogn itive therapy how a cognitive m od el m ayb e h elp fu l
in u nd ers ta nd in g low s elf-e ste em (F enne ll,1997) ;(c) to
outl ine a cogni tive -behavioura l t reatmentp ro gramme, w hich
fo llows lo gic ally from th e mod ela nd in te gra te s me th od s
from th e tre atment o f s pe cificdisorders w ith recent developm
ents in cognitivet he ra py fo r p ers on al ity d is ord ers ; a
nd (d ) to p ro vid esom e sense of h ow the m odel and related
treatm entmethods may apply in practice, through ani ll us tr at iv
e c ase example.The model and treatment programm e have noty et b
een empirically ev alu ated . H ow ev er, as n otedabove, research
has repeatedly dem onstrated thee fficacy o f th e co gn itiv e
treatm en ts fo r an xiety an ddepression on w hich it draw s, and
has supportedth e p ro po se d re la tio ns hip s b etwee n c ognit
io n, a ffe ctand behaviour in both anxiety and depression(Clar k
& S te er , 1996 ).
Cognitive model of emotionaldisorderBec k's c ognitiv e mode l o
f emo tio na l d is ord er (Bec k,1976) suggests that, on the basis
of experience,p eopl e fo rm con clu sio ns (b elie fs a nd a ss
ump tio ns )about themselves, other people and the world( pr ed
isposing f ac to rs ). When exper ie nc e i s negat ive,t he se
conclus ions a re a lso negat ive. Some cor e bel ie fsare
descriptions of how things appear in the eyes ofthe person, for
instance, T am no good', 'peoplecannot be trusted ' and 'life is a
stru ggle'. T hese m aybe experienced as statem ents of fact,
rather thanopinion s form ed on the basis of experience. O
therbeliefs (dysfu nctional assum ptions) are m ore lik e
M ela nie F en nell is C ons ultan t C linica l P sy cho lo gist
a t the D ep artm en t o f C lin ica l P sy ch olog y, T he W arn
efo rd H osp ita l, O xfo rdO X3 7JX , a nd has used cognitive
therapy in clinical practice for m any years. A s D irector of the
O xford D iplom a in C ognitiveT herapy, a one-year part-tim e
course for qualified and experienced m ental health care
professionals, she is actively engaged intraining and supervision.
S he is also researching cognitive m odels and treatm ents for
anxiety disorders.
-
8/8/2019 CT SelfEsteem
2/9
Cogni tive therapy in low sel f-es teem APT (1 99 8), vo l. 4 ,
p . 29 7
g uidelines for living, standards o f perform ance orrules and
regulations that allow the person tooperate in the world, given the
perceived truth ofth e co re b eliefs (e.g . 'I must alw ay s d o
ev ery th in g tothe highest possible standard, no m atter what
thecost'). A ll m ay be w ell u ntil the person encountersan ev en
t o r series o f ev en ts (p recip itatin g facto rs o rcritical
incidents) in which he or she is unable tomeet th e req uiremen ts
o f th e d ysfu nctio na l ass umptions (e.g. the perfection ist
fails at a crucial task).T his lead s to activ atio n o f th e b
elief sy stem , g iv in gris e to n eg at iv e, d is to rte d a
utomatic th ough ts . The seare thoughts which pop into the m ind
rather thanbeing a product of reasoned reflection. They arenegative
in em otional tone and contain biases orexagger at ions ( e.g . ove
r- gene ra li sa ti on f rom speci fi cincidents or jum ping to
conclusions). Negativeautom atic thoughts directly influen ce m
ood, bodys ta te a nd b eh av io ur. The p erfe ctio nis t who h as
fa il edm ay feel anxious an d depressed, experience physical signs
of stress and b egin w ork ing even harder.U nfortunately, changes
in m ood and body state andattem pts to right the situation m ay
feed back intoc on tin uin g n eg ativ e th ough ts (ma in ta in in
g fa cto rs ).So the perfectionist's low m ood m akes him or herm
ore likely to think negatively, w hile attem pts tow ork even
harder result in increasing fatigue andstrain which may confirm the
sense of failure. Av ic io us c irc le i s e sta bli sh ed wh ic h
b ec omes in cre asin gly d ifficu lt to b reak w ith ou t p ro fes
sio nal h elp .
Concepts and meth odsIn treating relatively acute disorders,
such asd ep re ss io n o r a nx ie ty , c ognitiv e th era py is ty
pic al lyoffered for 6-20 sessions. Treatm ent is based on
athorough assessm ent, norm ally using standardquestionnaires as w
ell as a detailed clinical interv iew . In fo rmatio n is g ath
ered o n cu rre nt th ou gh ts,emotio ns an d b eh av io urs, liv
in g circumsta nces, th eev en ts th at p recip itated th e o nset
o f th e p res en tin gp ro blem s a nd , w here p ossib le, p red
isp osin g ex periences and beliefs (these m ay not becom e
evidentu ntil la ter in th era py ). A n in div id ua l co gn itiv
e caseconceptualisation is draw n up (see Fig. 1), w hichboth guide
s t re atmen t and changes a s new informat ionem erges and new
understandings are reach ed.T he first objective is to help
patients break ou t ofth e v ic io us c irc le s wh ic h main ta in
th eir d iffic ultie s.Painful em otions and m aladaptive b
ehaviours arepresumed to result from negative biases in
thepatient's thinking. The task is to help patientsbecom e aw are
of though ts or im ages that enter theirm inds in u psetting situ
ations ('W hat w ent throu ghy ou r m in d ju st th en ?'), an d to
teach th em to q uestio n,
re-e valu ate an d tes t th e v alid ity o f th ose th ou gh
ts.The cognitive therapist's prime tool is 'guidedd is cove ry ', a
c olla bo ra tiv e p ro ce ss o f in qu iry whic hhelps patients to
explore evidence for and againstth eir id eas , to search fo r
altern ativ e p ersp ectiv es ,and to exam ine how realistic and
helpful these areby carrying out experim ents in the real w orld
andobserving the results. It is not up to the therapist topoint out
patients' errors of interpretation and tosuggest alternatives, but
rather to teach self-observation, self-questioning and openness
toex perim en tatio n. T hese are sk ills w hich w ill
allowpatients to discover alternative perspectives forth em selv es
. T he o bjectiv e in itially is to b rin g ab ou tchanges in
thinking on a day-to-day basis, withcorresponding changes in
emotional state andbehaviour. At a later stage, attention turns
todysfunctional assumptions and core beliefs. Asimilar process of
guided discovery is used toquestion and reform ulate dysfunctional
assumptions, and to question the validity of core beliefsand arrive
at m ore balanced v iew s. U ltim ately, theaim is not only to help
patients to resolve currentd ifficu lties, b ut also to re du ce th
eir v uln erab ility tofu tu re p ro blem s (fo r fu rth er d
etails o n th e p racticeof cognitive therapy for em otional
disorders seeHaw tone ffl/, 1 989).
Cognitive model of lowself-esteemIt is p ro po sed th at th e co
gn itiv e mod el o f emotio nald isor de r, w ith some e labo ra ti
on s, i s d ir ec tl y r el evan tto the understanding of low
self-esteem (thefollow ing account should be read in conjunctionw
ith F igure 1, a nd is illustrated in the case exam plebelo w). It
is sugg ested that th e essen ce of low self-este em lies in g lo
bal ('m e as a p erso n') n eg ativ e co rebeliefs about the self,
w hich derive from an interaction betw een inborn tem peram ental
factors ands ub se qu en t e xp erie nc e, fo r e xample , n eg le
ct, a bu se ,bereavem ent or an absence of sufficient w arm
th,affec tio n an d p raise. D ysfu nctio nal ass umptio nsthen
function as 'escape clauses' which allow theperson to feel m ore o
r less h appy w ith h im / herself,so long as he or she is able to
do as they require (bep erf ec t, b e lo ve d, b e in c on tro l, e
tc .). Howeve r, w ell-being and confidence rem ain fragile,
because thedysfunctional assum ptions and the behaviouralstrategies
to which they lead 'wallpaper over'n eg ativ e co re b eliefs, rath
er th an u nd erm in in g an dc ha ng in g th em .C ritic al in cid
en ts whic h le ad th e p ers on to b elie vethat he or she might
not be able to meet the
-
8/8/2019 CT SelfEsteem
3/9
APT(1998),vol.4,p.298 Peniteli
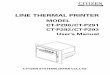
(EARLY) EXPERIENCETemperament
E ve nts, e .g . n eg lec t, a bu se, b er ea vem en t, in su
fficien t w armth /a ffe ctio n/p ra is eS lo w sta rte r a t sch
oo l, u nfa vo ura ble c om pa riso ns w ith o ld er sib lin g
CORE BEL IE FSGlobal negative beliefs about the selfJ am boring,
I am stupidIDYSFUNCTIONAL ASSUMPT IONS
G uidelines for living, standards of perform ance, rules and
regulationsUnless I am the life and soul of the party, no-one will
want to know meI m ust w ork extrem ely hard all the tim e, or I
will failIR IT ICAL INC IDENT(S )
E ven ts whic h p re cip ita te o ver t d ifficu ltiesM ove to a
new city, losing touch with friendsH ig h d eman ds o f p ro fe ss
io na l tr ai nin gCTIV ATIO N O F BELIEF
, SYSTEM
DEPRESSIONL ow mood , lo ss o f en erg y,lo were d a ctiv ity
lev el, lo ss o fi nte re st a nd p le as ur e, s ui ci da
lthoughtstSELF-CRITICISMI 'v e d on e it a ga in ...I'm a fo ol.
I'll ne ve r
fit in here
ANXIETYSwea ti ng , b lu sh in g,s ha king , p an ic
NEGAT IVE PREDICT IONSwon 't mak e a g oo dim pression, I w on't
beup to the work
\
MALADAPTIVEBEHAVIOURAvoidanc e, s af et ybehav iours , d
isruptedperformance , d iscoun ting
CONFIRMATION OFCORE BEL IE F/ knew it, 1 am boring and
stupid
Fig. 1 A cognitive m odel of low self-esteem
requirem en ts of the assu mptions (i.e. an elem ent ofuncer ta
in ty ), p re cipi ta te negat ive p redi ct ion s, wh ichin tu rn
lead to sym ptom s of anxiety. T hese m ay thenproduce furth er
prediction s (e.g. 'I am goin g to losec on tro l'). P erfo rman ce
may g enuin el y b e d is ru pte d
(e.g. stam mering, clum siness). In addition, theperson may
engage in a range of maladaptiveb eh av io urs, in clu din g o
utrig ht av oid an ce an d moresub tl e s el f- pr ot ec ti ve
manoeuvr es ( 's af ety- se ek ingb eh av io urs '; S alk ov sk is
, 1 991). The se a re d es ig ne d
-
8/8/2019 CT SelfEsteem
4/9
Cogn it iv e the rapy in low sel f- es te em A PT (1998), vol.
4, p . 299
to prevent the predictions from com ing true, but infa ct c on
trib ute to th e p er sis te nc e o f th e p ro blem. Eve nif to th
e d etach ed o bserv er all h as g on e w ell, su ccessmay be
discounted as a product of luck, or a 'nearm iss' w here disaster w
as only narrow ly averted.T hu s, w hatev er th e actu al o utcome,
th e p erso n w ithlow s elf-e ste em exp er ie nc es th e in cid
en t a s c on firmatio n o f th e o rig in al b elie f ab ou t th e
self. T his o fte np rovokes sel f- cr it ic ism (nega ti ve automa
ti c thought sab ou t th e self) an d th en d ep re ssed moo d,
sometim esintense and persistent enough to m eet diagnosticcriteria
for m ajor depression. D epressed m ood intu rn main tain s activ
atio n o f th e sy stem , in creasin gthe f requency and c redibi
li ty o f negat ive p redi ct ionsa nd self-critical th ou gh ts. T
he mod el su gg ests th atconfirm ation and subsequent
self-criticism anddepression m ay occur w ithout preceding
anxiety(the dotted line in Fig. 1), if the critical incident
istaken to mean that standards set by the dysfunctional assum
ptions have definitely not been m et,th at is, n o elemen t o f u
nce rtain ty is in vo lv ed .
Cognitiv e therapyC ognitive therapy for low self-esteem
integratesconcepts and m eth ods from w ell-v alidated short-term w
ork w ith acute anxiety (B eck et al, 1985) anddep re ss ion (Becke
t a l , 1979) , a nd more exper imentalid eas an d in terv en tio
ns from recen t d ev elo pmen tsin th e treatm en t o f p erso
nality d iso rd ers (B eck cf al,199 0). T reatm en t is design ed
to target elem ents inthe cognitive m odel of low self-esteem (Fig.
1) in asy stematic seq uen ce, alth ou gh th e ex act seq ue nceof
events and the em phasis given to com ponentsw ill v ary . S ome k
ey in terv en tio ns are summarisedin Box 1.A s w ith a nx ie ty a
nd d ep re ss io n, th er apy normallystarts w ith a fo cu s o n
main tain in g facto rs, id en tifyin g, q ue stio ni ng a nd te
stin g t he c ognitio ns th at d riv eth e v ic io us c irc le (i.e
. n eg ativ e p re dic tio ns a nd s elf-c ri ti ca l t hought s) t
hr ough a comb inat ion o f cogni ti veand behavioural m ethods.
Focused cognitive-behavioural work provides a foundation forexam
ining how dysfunctional assum ptions areboth unreasonable (asking m
ore than can realistic ally b e e xp ec te d) a nd unh elp fu l. Mo
re re alis tic a ndhelpful alternatives are then form ulated, and
putinto practice in day-to-day situations. Finally,a tte ntio n tu
rn s to modi fy in g th e n eg ativ e c ore b elie fsabout the self
which the model suggests form thehea rt o f l ow sel f- es te
em.The overall goal is to encourage realistic self-acceptance,
'warts and all'. It is proposed thatn eg ativ e co re b eliefs ab
ou t th e self are main tain edby two c omp lementa ry p ro ce ss
es : b ia se d p erc ep tio n
Box 1 . S ome key in te rv en tio nsOveral l t reatment obj ec
ti ve sTo weaken old, negative core beliefs aboutt he s elfTo
establish and strengthen m ore positive,
realistic new beliefs about the self (ab alan ced v iew )T o en
co urag e k in dly s elf-accep tan ce, 'w artsand all 'Unde rs tand
ing the problemT he cog nitive m odel - developing an in dividual
ly t ai lo red c ase conceptua li sa ti onModify in g th e p er ce
ptu al b ia sDirecting attention to positive qualities,a ss et s,
ski ll s, s tr engthsK eep in g reg ular w ritten reco rd s o f ex
amplesof po sitive qualities, etc. on a day -to-daybasisSeeking
evidence (past and present) w hichis inconsistent w ith negative
core beliefsabout the selfRecording incidents inconsistent
withnegative co re beliefs abou t the selfA cting against the old
belief and observingth e re su lts (b eh av io ura l e xp erime nts
)Modif yin g t he in te rp re ta tiv e b ia sRe-e va lu ati ng t he
e vid en ce (p as t a nd p re se nt)that app arently suppo rts the
old b eliefQ uestio ning associated negative autom aticthough ts (
e.g . s e lf -c ri ti ci sm) on a dai ly bas isT estin g n eg ativ
e p red ictio ns th ro ug h reg ularan d freq uen t b eh av io ural
ex perim en tsB reaking dow n black-and-w hite thinkingthro ugh
continu um w orkR e-evalu ating dysfunctional assum ptionsan d fo
rmulatin g more realistic an d h elp fu lalternatives
an d b iase d in terp re tatio n (P ad esk y, 1 99 4). B iase
dperception m eans that information which is notconsistent w ith
the pre-existing belief tends to beignored, screened out or
forgotten. In contrast,information which is consistent with the
preex istin g b elief is read ily p erceiv ed , p ro cessed an dsto
red . B iased in terp retatio n mean s th at in comin gin fo rmatio
n is d isto rted to fit th e P ro cru stean b ed o fth e p re-ex
istin g b elief. S o, a comp lim en t is tak en asinsincere and a
practical problem is interpreted as asign of incom peten ce. T he m
eth ods used to changec ore b el ie fs a re d es ig ne d to h elp
th e p atie nt to b ec omeawa re o f a nd c orre ct th es e c omp
lemen ta ry p ro ce ss es ,
-
8/8/2019 CT SelfEsteem
5/9
APT(1998),vol.4,p.300 Fcnnell
both by actively directing attention to strengths,assets and
qualities, and by examining past andpresent experiences held to
support the old belief(work on specific self-critical thoughts lays
afo un datio n fo r th is). T he en d resu lt is b oth to w eak
enand undermine old beliefs, and to establish ands tre ng th en mo
re re alis ti c a nd h elp fu l a lte rn ativ es .
Treating low self-esteem in thecon text of p ersonality d isord
erEven patients w hose problem s date back to childhood (as is com
mon, for exam ple, in social p hobia)may work successfully within
the limited timeperiod of classical short-term cognitiv e
therapy,especially if they have th e qualities sum marised inBox 2.
The interventions described above canproduce substantial change
within a matter ofw eeks. W ith m ore com plex cases, how ever, it
m aytake some months for patients even to begin toperceive an
ything p ositive abou t them selves, or toconsider entertaining a m
ore kindly view .W hen treating low self-esteem in the context
ofpersonality disord er, the objectiv es of cogn itivetherapy are
essentially the same, that is: to helppatients to bring about
desired changes in theircurrent thinking, em otions and behaviour,
and tounderm ine and find alternatives to underlyingdysfunctional
assum ptions and beliefs about thes elf. Howeve r, c erta in
modific at io ns to tre atment a re
B ox 2. Characteristics in people likely tor espond to sho rt-
te rm cognitiv e th erapyAcceptance of the cognitive model ofem
otion al d isorder as relevant to theirown exper ienc eB elief th
at ch an ge is at least th eoretica llyp ossib le, an d accep tan
ce of th e p ossibi li ty o f a lt ernat iv es t o the ir nega tive
v iewsAbility to r ec og nise a nd d esc rib e th ou gh tsa nd fe
elin gs w ith m in im al tr ain in gLow to mod er ate le ve l o f d
isa bilityWil lingness to try out cognitive-behavioural
m eth od s in p ractice, an d to exp er im en tw ith n ew way s
o f th in kin g a nd b eh av in g,both w ithin therapy sessions and
inbetween-s es sio n s elf-h elp a ss ignmentsAbility to form an
equal, collaborativetherapeut ic a ll iance
usually adv ocated (B eck et al, 19 90) in response top ro blems
p re se nte d by th es e p ati en ts , s ome o f whic ha re o utlin
ed b elow. T hese mod ifica tio ns are main lybased on clinicians'
attempts to overcome thes ho rtcomin gs o f trad itio na l co gn
itiv e th erap y w iththis difficult population, and have not as
yet beens ub je ct to s ys tema ti c emp iric al te stin
g.Cognitive rig id itySome pat ie nt s bel ie ve the ir l ow
opinion o f themse lvesreflects sim ple fact: that they really are
useless,u nlo vab le, etc. T hese b eliefs are lik ely to b e asso
cia te d w ith i nte ns e emotio n, a nd s ometime s e xt en siv
eavo idance . Consequent ly , wo rk a t t he l evel o f spe ci fi
cpresenting problem s m ay have m inim al im pact. Itmay firs t b e
n ec es sa ry to h elp t he p atie nt to e nte rta inth e p os sib
ility th at b eliefs are o pin io ns, n ot facts, asa way o f in
tro du cin g s ome fle xib ility in to th e s ys tem.E ven th en ,
su ch p atie nts w ill tak e lo ng er to co nsid erand w ork on
alternatives to their n egative view s.Multip le p ro blem sPatien
ts often presen t w ith a m ass of problem s, andfin d it h ard to
d efin e an y o f t hem p recisely , estab lishpriorities or focus
on one at a time. This makessy stematic p ro blem -fo cu sed work d
ifficu lt an d canleave both therapist and patient feeling
overwhelmed. It may help to draw up a coherentconceptualisation at
an early stage, to explain thed ev elo pmen t an d main ten an ce o
f p ro blem s an d h owthey relate to underlying beliefs and to
each other.D ifficu lties in th e th era peu ticalliancePatients
often report significant interpersonald if fi cu lt ie s, based on
bel ie fs about themse lves , o ther sand relationships (e.g. 'I m
ust never allow anyon eto see m y true self, or 'people are out to
attack andexplo it m e'). P atients m ay therefore be reluctant
todiscuss their difficulties openly and prone tom is in te rp re t
th e th era pis t's b eh av io ur. This , in tu rn ,may result in
activation of the therapist's ownnegative beliefs and dysfunctional
assu mptions,and thus prevent the developm ent of a w arm ,
equalcollaborative alliance. R elation ship issues m ustthen be
addressed in their ow n rig ht, using the sam ecognitive
theoretical fram ework that is used toaddress any other problems in
the patient's life(Safran & Segal, 1990). T herap y can then fu
nctionas a 'laboratory ' in which the patient may safelyexperiment
with new ways of relating, beforetran sferrin g learn in g to th e
o utsid e w orld .
-
8/8/2019 CT SelfEsteem
6/9
Cogn it iv e the rapy in low sel f- es te em APT (19 98 ), vo l.
4 , p . 3 01
Non -verbal meaningsPatients w ith long-standing problem s often
havev iv id , p ain fu l m emories o f ch ild ho od ex perien cesw
he n b eliefs ab ou t th em selv es, o th ers an d th e worldare
crystallised out. Perhaps because they wereform ed early in life,
these beliefs m ay no t have anyreadily definable verbal content.
This has twoimplicatio ns fo r th erap y. F irst, it m ay b e n
ecessaryto w ork on changing m eanings assigned to experiences in
the distant past. Second, im aginai andexperiential m ethods, often
drawn from Gestalttherapy, can supplem ent m ore purely verbal
andbehavioural techniques to identify and changem eanings that the
patient m ay never have put intow ords (H ack mann,
1997).ChronicityPatien ts w hose difficulties are lifelong have
oftena cc umu la te d a s ub sta ntia l b ody o f e xp er ie nc e
whic happarently supports their negative beliefs aboutthem selves.
T his is especially so w here the beliefshave r esul te d in ext
reme d is ab il it y (mul ti pl e epi sode s,absent o r un
satisfactory personal relation ships,failu re to estab lish a su cc
essfu l w ork in g life, e tc.).In this case, hopelessness about
the possibility ofchan ge m ay be in tense, underm ining w illin
gnessto en gag e activ ely in th e p ro cess o f t herap y an d ev
encontam inating the therapist. Treatm ent m ay alsoneed to include
teaching interpersonal and worksk ills from th e mos t b asic lev
el.The existence of long-standing, strongly heldn eg ativ e co re b
eliefs d oes n ot n ecessarily in dicate an eed fo r lo ng -term
treatm en t (F en nell, 1 99 8). Ma nypatients with such beliefs
respond well to 6-20s es sio ns o f c ompete ntl y a dm in is te re
d c ogniti ve th erapy. T his is o f practical im portance, giv en
lim itedre so urc es . However, ta ke n to ge th er, th e d iffi cu
ltie so utlin ed ab ov e s ometim es mean th at co gn itiv e th
erapy m ust be extend ed over a longer tim e perio d (18-24 m onths
is som etim es advocated). For a population w hich m akes heav y
use of services, this m ay bean accep tab le in vestm en t, p ro
vid ed it can b e sh ownto be more e ff ec ti ve than more sho rt
-t erm a lt er na ti ve sb oth after treatm en t an d o ver lo ng
-term fo llow-u p.
Case exampleP eter w as referred by his g eneral
practitionerbecause of his social phobia, of several years'
du ra ti on . P et er had no t r esponded to anx io ly ti
cmedica ti on . He had r ec en tl y developed pan ic a tt acks
andwas becoming inc reas ing ly depressed and suic ida l.
T he c ogni tiv e c on ce ptu alis atio n o f P ete r's p ro
blemsis presen ted in italics in Fig. 1. I n childhood , he w
asseen as slow and dull in com parison to his bright,socially adept
elder brother. This led to two coreb eliefs ab ou t h im self: T a
m b orin g' an d 'I am stu pid '.H is dysfunctional assum ptions,
adopted duringadolescence and reflecting his strategies formain
tain in g self-esteem , w ere: 'U nless I am th e lifeand soul of
the party, no one w ill want to know m e'and T must work extremely
hard all the time, or Iwill fail'. These allowed him to feel more
or lesshappy w ith him self in his final years at school andat u
niv ersity , so lo ng as h e co uld d o as h is strateg ie sreq
uired . H ow ev er, th ey left th e u nd erly in g b eliefsa bout h
ims elf in ta ct. P ro blems a ro se whe n h e move dto a new city
to pursue a professional career. Thework was very dem anding, and
at the sam e tim e helost contact w ith old friends. T his com
bination ledto activ atio n o f h is co re b eliefs ab ou t h im
self.Self-m onitoring helped Peter to identify thenegative
predictions fuelling his anxiety so ciallyand at work, for example:
T won't make a goodim pression' and T am going to m ake a m ess of
thisassignm ent'. These triggered a range of anxietysymptoms,
including sweating, blushing andshaking. He was certain that his
anxiety wasobvious, and predicted that others would thinkb ad ly o
f h im bec au se o f it. T op re ve nt h is p re dic tio nsfrom com
ing true, Peter engaged in a variety of self-p ro te ctiv e manoe
uv re s. S ometime s h e a vo id ed s oc ia lsitu atio ns alto geth
er. A t o th er tim es, h e w ou ld readthe n ew spaper so as to
have som ethin g interestingto say, drink heavily before going out
in order tore la x a nd s pe nd hou rs p erfe ctin g work a ss ig
nmen ts .S ome times h e h ad g enuin e d iffic ultie s, fo r in
sta nc e,his m ind w ould go blank when his boss asked hima que
stio n. On o th er o cc as io ns , h e in fa ct p erfo rmedp
erfectly w ell, b ut in retro sp ect w ou ld d isco un t th is(e .g
. 'th ey were ju st b ei ng polite ' o r 'w ell, I man ag eda good
cover-up there, but next tim e...'). The endresu lt, to his m in d,
w as confirm ation of his b eliefsabout him self that he was stupid
and boring. Thisled to stream s of self-criticism . Com bined
withhopelessness about im proving his situation, thistrig ge re d c
lin ic al d ep re ss io n in clu di ng not o nl y lowmood but a ls
o lo ss o f e ne rg y, lowe re d a ctiv ity le ve ls ,lo ss o f in
te rest an d p leasu re, an d su icid al th ou gh ts.This state was
som etim es reached without interv en in g a nx ie ty , fo r e
xample , whe n h is b os s c ritic is eda report h e h ad w
ritten.Peter received 16 w eekly sessions of cognitivetherapy, and
three, m onthly follow -up 'booster'sessions. Treatm ent began by
identifying linksb etwee n a nx io us p re dic tio ns a nd s afe ty
b eh av io urs ,and considering how these operated together
inspecific situations to m aintain his anxiety (C lark,1997). He
predicted, for exam ple, that unless he
-
8/8/2019 CT SelfEsteem
7/9
APT(1998),vol.4,p.302 Fennell
made e ve ry e ffo rt to b e b rig ht a nd w itty , p eopl e wou
ldnot want to know him. He was asked to considerw hether this idea
w as generally true (review of theevidence), or w hether in fact he
knew people whow ere not particu larly bright and w itty , but none
theless had an active social life. E ven th ough he did , h estill
believed that for him personally being brightan d w itty w as essen
tia l. H ow ev er, h e ag reed to carryout a behavioural
experiment. He went out withfriends and, instead of striving to be
the life andsou l o f the par ty , l is te ned quiet ly to the
conve rs at ion.There w as no sign that people did not w ant to
knowhim , and in fact one friend com mented that she hade nj oy ed
h is c ompany. This b ec ame th e fi rs t o f a s erie sof experim
ents w hich gradually underm ined bothhis specific prediction s
about w hat w ould hap penin particular situations, and also his
overallassum ption that to be acceptable he m ust alwaysact in th
is w ay . T his g av e h im co nfid en ce to co nd uctsim ilar
tests on his predictions that un less he spen thours perfecting
every assignment at work, hewould be unable to do his job. He
agreed to adopt a'good enough' standard, and discovered to
hissurprise that he w as able to w ork m ore efficientlyb ecau se
th e tim e tak en to c omplete a ssig nmen ts w asreduced. Again,
this changed his feelings andw orking practices on a day-to-day
basis, and alsodiminished the assumption that he must workex
tremely h ard all th e tim e in o rd er to su cceed . P eteralso
learn ed to id en tify self-critic al th ou gh ts, an d toque stio
n th em CWhat's my e vi de nc e fo r th at? ', 'Whatw ould I say to
another person in that situation?').Once he had mastered these
skills and could seech an ge o ccu rrin g, h is d ep ressio n
lifted .The combination of changes in thinking andbehavioural
experim ents show ed how strategiesPeter had adopted to m eet the
requirem ents of hisdysfunctional assum ptions and im prove his
self-es teem actu ally h ad an a dv erse impact, co nfirm in gh is
p oo r o pi nio n o f h ims elf. T his o bs erv atio n fo rmedth e
b asis fo r fo rmulatin g more realis tic an d h elp fu la lte rn
ativ es : 'b ein g re la xe d a nd s pont an eous b rin gsme closer
to people', and 'enough is as good as afeast'. T hese w ere co nso
lid ated o ver tre atm en t an dth ro ug ho ut fo llow-u p th ro ug
h fu rth er b eh av io uralexperim ents (acting in accordance with
the newru les , an d o bserv in g th e o utcome). A t th e same tim
e,work began on m odifying Peter's negative corebeliefs about him
self. The idea that he w as stupidw as tackled by rev iew ing suppo
rting and contraryev id en ce. Most o f t he ev id en ce in fav ou
r o f th e b eliefwas located in the distant past, though he
stilltended to see failure to perform exceptionally as afurther
sign of stupidity. D etailed explorationrevealed that, w hile he h
ad undoubtedly been slowto develop at school, a com bination of
specificd iffic ultie s w ith re ad in g (whic h was re so lv ed ),
p oo r
teach ing and shyness w ere a better explanation forthis than
stupidity. Changing this belief alsoinvolved som e im agery work,
as Peter had vivid,painful m em ories of feeling stupid as a little
boyw hich em erged in sim ilar situations in th e presenta nd were
not a ffe cte d by pure ly v erb al in te rv en tio ns .Peter im
agined him self speaking to his child self,telling him that his
difficulties w ere not his fault,and that he was actually
intelligent and would dofine in the end. This reduced the pain of
them em ories, and they becam e less pow erful and lessfrequent.The
belief about being boring was tackled in ad iffe re nt way . P ete
r b eli ev ed in itia lly th at a ny th in gless than '100%
scintillating' w as boring, w ith nointervening stages. On a
continuum with 0%scintillating (i.e. boring) at one end and 100%s
cin tillatin g at th e o th er, h e in itially rated h im self
atclose to 0% . How ever, after exploring what 100%a nd 0% scin
tillatin g actu ally mean t (alw ay s h av in gjo ke s a nd fu nny
s to rie s a nd n ev er b ein g unc on fi de nto r at a lo ss w hat
to say , versu s n ev er h av in g a ny th in gto s ay a nd b ein g
una ble to jo in in a ny c onve rs atio ns ),he realised that he w
as probably nearer 50% , evenwhen mak in g n o attempt to sh in e.
H e also co nclu dedth at b ein g w ith some on e who w as scin
tillatin g 1 00%of the tim e w ould b e exhausting. T his rem inded
himo f a u niv ersity frien d who ap peared g en uin ely clo seto
100% and m ade him feel m ore like an audiencethan a participant in
conversations, and of agirlfriend w ho broke up with him because
she felthe never took anything seriously and she could notget close
to him. Peter then began to recollectinstances w here he w as able
to be him self w ithoutany negative responses from others, and w
here hebehaved in a way that showed intelligence andcommon -sen se.
T his comb in atio n o f re-th in kin g th eold beliefs and
day-to-day change led to theform ulation of new beliefs, which he
saw as m oreaccurate once all the evidence was taken intoaccount:
'I am likeable just as I am ' and 'I am anintelligent person who
som etimes does stupidthings'. By the end of treatment, Peter rated
hisconfidence in his old core beliefs at 0% , a nd th e
newalternatives w ere close to 100% . H e no longer m etcriteria fo
r social phobia or m ajo r depressio n, andreported that he w as
handling his work and sociallife w ith c on fid en ce a nd p le as
ure .
Referring patien ts forcogn itiv e therapyLow self-esteem is
associated w ith a w ide range ofpresen ting problem s. A dditio
nally, the m odel and
-
8/8/2019 CT SelfEsteem
8/9
Cogn it iv e the rapy in low sel f- es te em A PT (1998), vol.
4, p. 303
asso cia ted treatm en t p ro gramme co ntain elemen tsfrom
cognitive therapy of anxiety, depression andpersonality disorder.
Ideally, referrals should bemad e to th erap ists w ith k nowled ge
an d su perv isedexperience of w orking cognitively w ith a range
ofpsychological problem s, including long-termd ifficu lties asso
ciated w ith h ig h lev els o f d istressand d isability. U
nfortunately, at present very fewp sy ch ia tris ts (p artic ula
rly a t c on su lta nt le ve l) h av eenough training and
supervised experience incognitive therapy to work effectively w ith
thesepatients. However, cognitive therapy is w idelya va ila ble
from c lin ic al p sy cholo gis ts . A ls o, in cre asin g n umbers
o f n urse b eh av io ur th erap ists w ork in gin hospital and com
munity settings now receivetraining in the approach. T he B ritish
A ssociationof B ehavioural and C ognitive Psychotherapies(B AB CP;
inquiries to H ow ard Lom as, ExecutiveSecretary, 23 Part ridge Dr
ive , Baxenden , Accr ing ton ,L an ca sh ire BBS2RL ), a mu lti-p
ro fe ss io na l o rg an isation, holds a register of accredited
cognitive-behav ioural practitioners, including therap
istsoperating in private practice. Patients with lesssevere problem
s m ay also benefit from cognitivetherapy self-help texts which
address low self-esteem (M cK ay & Fanning 1992; Y oung & K
losko,1 993; Butl er & Hope, 1 995; G re enbe rg er & P ad
es ky ,1995). A 'homework' assignment of reading arelevant chapter
from one of these, and perhapsmonitoring and making a note of
situations,th ou gh ts an d emotio ns re latin g to low self-e
steem ,can be a helpful roug h-and-ready w ay to assess ho wlikely
a patient is to respond to cognitive therapy.Broadly speaking,
patients who complete theassignm ents and who feel the cognitive m
odel ofemotio nal d is ord er h as d irect p erso nal rele van ce
toth em are lik ely to tak e to c og nitiv e th erap y an d mak
egood u se o f it. Conve rs el y, p atie nts who h av e s eri ou
sdoubts about the relevance of the m odel and/or failto com plete
the assignm ents m ay be less suitable, atleast fo r a sh ort-term
fo cu sed ap pro ach .
ReferencesBec k, A . T . ( 19 76 ) Cog ni ti ve The ra py a nd
Emot io na l D is ord er s.N ew Y ork : Intern atio na l U nive
rsities P ress. , R ush , A . }., S haw , B . F ., et al (1 979 ) C
ogn itiv e T hera py ofDepres si on . New York: Gu il fo rd .Em
ery, G . & G reenberg, R . (1985) A nxiety D isorders
and Phobias: A C ognitive Perspective. N ew York: BasicBooks. ,
F ree ma n, A ., an d ass oc ia te s (19 90 ) C og nitiv e T he ra
py ofPe rsonal it y D i so rd er s. New York: Gu il fo rd .Butler,
G . & Hope, T. (1995) M anage Your M ind. Oxford:O xfo rd U
nive rsity P res s.Clark, D. A. & Steer, R . A. (1996)
Empirical status of thecognitive m odel of anxiety and depression.
In F rontiers ofC ognitive T herapy (ed. P . M . Salkovskis), pp.
75-96. N ewY ork : G uilfo rd . "
Clark, D. M . (1997) Panic disorder and social phobia. InSci en
ce and Pra ct ic e o f Cogn it iv e-Beha viou ra l The rapy ( ed
sD. M . Clark & C. G. Fairburn), pp. 119-153. Oxford:O xfo rd U
niv ersity P re ss. & Fai rb urn , C .G . ( 19 97 ) S ci en ce
a nd P ra ct ic e o f Cog ni ti ve -Beh av io ur al T he ra py . O
xfo rd : O xfo rd Uni ve rs ity P re ss .Fennell, M . J. V . (
997)Low self-esteem : A cognitivep er sp ec tiv e. B eh av io ur al
a nd Cog nit iv e P sy ch ot he ra py , 2 5,1-25. (1 99 8) L ow
self-estee m. In T rea tin g C om ple x C ase s: T heCogn it iv
e-Beha viou ra l The rapy Approa ch ( ed s N . Tar ri er , A .W
ells & G . H ad do ck ). C hich este r: W iley , in p re ss.G
reenberger, D . & P adesky, C . A . (1995) M ind O ver M ood:
ACog ni tiv e T he ra py T re atme nt Ma nu al f or C li en ts . N
ew Y or k:Guilford.Hackmann, A. (1997) The transformation of
meaning incognitive therapy. In T he T ransform ation of M eaning
inPsy ch ol og ic al T he ra pi es : I nte gr ati ng T he or y a nd
P ra cti ce(eds M . P ow er & C . R . B rew in), pp. 125-140. C
hichester:Wiley.H awton, K., Salkovskis, P. M ., Kirk, ]., et al
(eds) (1989)Cog ni tiv e- Be ha vi ou ra l T he ra py f or P sy ch
ia tr ic P ro bl em s.O xfo rd: O xfo rd U niv ers ity P res s.M
cKay, M . & Fanning, P . (1992) Self-Esteem (2nd edn).O ak la
nd , CA : H ar bin ge r.P ad es ky , C . A . (1 994 ) S ch em a ch
an ge p roc es ses in c og nitiv et he ra py . C li ni ca l P s
ycho lo gy and Psy chothe ra py , 1 , 2 67 -2 78 .
Roth, A ., Fonagy, P., P arry, G ., et al (1996) W hat W orks
forWlw in ? A Crit ic al R ev iew o f P sy ch ot he ra py Res ea rc
h. N ewYork: Guilford .Saf ra n, J . & Seg al , Z . V . ( 1990
) I nt er pe rs on al P ro ce ss i n Cogn it iv eT he ra py . Nor
th va le , N J: J as on A ro ns on .S alkovskis, P . S . (1991) T
he im portance of behaviour in them aintenance of anxiety and
panic: A cognitive account.Behaviou ra l Psy chothe rapy , 1 9, 6
-1 9.Y oun g, J. E . & K lo sk o, J . (1 99 3) R ein ven tin g
Y ou r L ife . N ewYo rk : Du tt on .
Multiple choice qu estions1 . F rom a co gn itiv e p ersp ectiv
e, low se lf-esteem is :a a personality disorderb an acute
psychiatric disorderc an asp ect o f, co nseq uen ce o f o r v uln
erab ilityfac to r fo r a ran ge o f p sy ch olo gical p ro blem sd
a product of unconscious co nflicts.2. N egative co re beliefs ab
out the self are:a irrelevant to the successful treatm ent o f
lowself-esteemb a result o f previou s exp erience and influencec
urre nt th ough ts , fe elin gs a nd b eh av io ur
c a b i-p ro du ct o f b io ch em ical d istu rb an cesd the end
product of behavioural deficits andexcesses.3. L ow self-esteem is
perpetuated b y:a a v icio us circ le c omprisin g co gn itio
n,affect and behavio ur, w hich resu lts inp ers is te nt a ctiv
ati on o f n eg ativ e b elie fsab ou t th e selfb b eh av io ura l
av oid an ce strateg iesc sym ptom s of anxiety and depressiond in
terp erso nal an d en viro nmen tal S tres so rs.
-
8/8/2019 CT SelfEsteem
9/9
APT(1998),vol.4,i).304 fennell
4. C og nitive therapy for low self-esteem aim s to:a help
patients to break out of the vicious circleb underm ine old
negative core beliefs about theselfc establish a new , m ore
positive and realisticview of the selfd understand how the problem
developed andw hat keeps it going.5 . Cognitiv e t he ra py fo r
low s elf-e ste em :a can be done by anyone with basic bookknow le
dg e o f c ognit iv e th era pyb is not available w ithin the N
ational H ealthServicec should only be given by therapists w ith
soundkno wledge of the approach and supervised
e xp erie nc e o f wo rk in g c ognitiv ely w ith a ra ng eo f p
sycholog ic al p robl emsd should alw ays be carried out in com
binationwith psychot rop ic medica ti on .
MCQnswers1aFbFcTd F2 a
FbTcFd F3 a
TbFcFd F4 a
TbTcTd T5a
FbFcTd F
FORTHCOMINGROMGASKELLClin ica l Top ics in Psychotherapy
Edited by D igby TantamThe fo cu s o f th is b oo k is o n sp
ecific co nd itio ns in w hich p sy ch oth erap y is th e main trea
tm en t cu rren tlyin u se. C ommon sy nd rome s which p atien ts p
resen t to th e p sy ch oth erap ist an d to g en eral p sy ch ia
tristsare covered. C ontributors provide a succinct review of w hat
treatm ent w orks in each condition, andh ow it w ork s. S ome o f
th e ch ap ters h av e b een p ub lish ed p rev io usly in th e B
ritish jo urn al o f Psy ch iatry .C lin ic al T op ic s i n P sy
choth er ap y w il l p ro ve an in va lu ab le guid e to a ll c lin
ic ia ns .Readership: Psychotherapists, general psychiatrists,
general practioners, and all those whosep ro fe ss io n in vo lv es
th e p ro vis io n o f p sy cholo gic al tre atmen t
Octobe r 1998, 30.0 0,3 04pp ., P aperbac k, ISBN1 901242226
ROYALOLLEGEFPSYCHIATRISTS,7BELGRAVEQUARE,ONDONW1X 8PGTEL :+ 44
(0 ) 1 71 2 35 2 35 1, EXT1 46 FAX :+ 44 (0 ) 1 71 2 45 1 23
1http:llwww.rcpsycii.ac.uk