Embed Size (px)
Citation preview

1
Anthony PowellGillian Lieberman, MD
CT Imaging of the Kidney
Anthony Powell, HMS IVBeth Israel Deaconess Medical Center
Gillian Lieberman, MD
Images: BIDMC, Dept of Radiology, 2001.
September 2001
Images: Netter, FH: Atlas of Human Anatomy, 2nd ed. Novartis, 1997

2
Anthony PowellGillian Lieberman, MD
Renal Anatomy: Axial View
Gerota’s FasciaPerinephric fat
Pararenal fat
Peritoneum Right Kidney
Renal Capsule
Renal Artery
Renal Vein
Images: Netter, FH: Atlas of Human Anatomy, 2nd ed. Novartis, 1997
3
Anthony PowellGillian Lieberman, MD
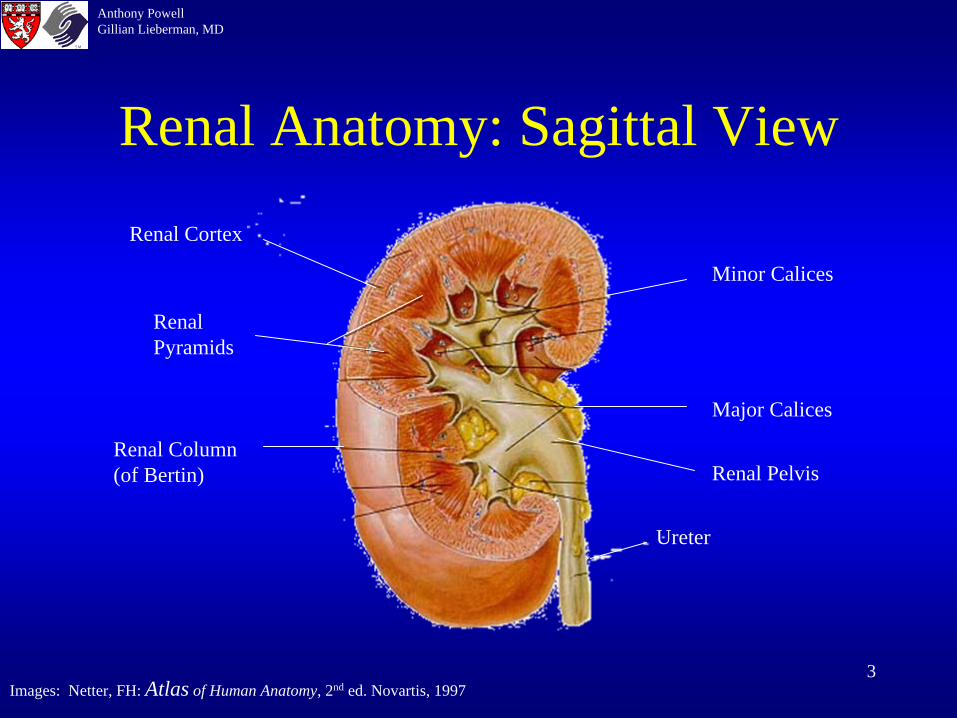
Renal Anatomy: Sagittal View
Minor Calices
Renal Pelvis
Major Calices
Renal Column (of Bertin)
Renal Pyramids
Renal Cortex
Ureter
Images: Netter, FH: Atlas of Human Anatomy, 2nd ed. Novartis, 1997

4
Anthony PowellGillian Lieberman, MD
Standard CT Technique for Renal Imaging
• 5mm-10mm collimation usually adequate to demonstrate kidneys
• IV contrast allows differentiation of pathologic processes from nl parenchyma– Corticomedullary differentiation max at 30 sec– Nephrographic phase best seen at 70-100 sec
• Non-contrast Helical CT for uro/nephrolithiasis
5
Anthony PowellGillian Lieberman, MD
Congenital Abnormalities
• Duplicated collecting system/partial duplication bifid renal pelvis
• Horseshoe Kidney– Connecting isthmus across midline, usu between lower poles
• Crossed Ectopia– The ureter of the ectopic kidney inserts into the bladder
orthotopically (I.e. on opposite side)
• Pelvic or Intrathoracic Kidney• Renal hypoplasia• Renal agenesis

6
Anthony PowellGillian Lieberman, MD
Crossed Ectopia
• Lower kidney is usually the ectopic one
• In 90% there is fusion of both kidneys (crossed- fused ectopia)
• Incidence 1:1000 births
• Slightly increased incidence of calculi, however, incidence of other assoc anomalies is low

7
Anthony PowellGillian Lieberman, MD
Crossed Ectopia
Images: BIDMC, Dept of Radiology, 2001.
Axial abdominal CT, contrast enhanced, nehrogram phase
Right orthotopic kidney
Left crossed ectopic kidney

8
Anthony PowellGillian Lieberman, MD
NephrocalcinosisCauses:• Renal Artery Atherosclerosis• Nephrolithiasis= stones in the collecting system
• Medullary Nephrocalcinosis (95%)= calcium deposition in medulla– Renal Tubular Acidosis, Medullary Sponge Kidney, HyperCa2+
states (hyperPTH, Paraneoplastic), Papillary necrosis (Diabetes Mellitus, sickle cell), TB
• Cortical Nephrocalcinosis (5%)= calcium deposition in cortex– Chronic poststrep glomerulonephritis, Oxalosis, Alport synd,
Acute cortical necrosis
• Infection, Cyst, Tumor, Hematoma

9
Anthony PowellGillian Lieberman, MD
Nephrolithiasis
• Epidemiology– Up to 10% by age 70, usu in 3rd to 4th decade– 4:1 M to F ratio– More prevalent in the South
• Risk Factors– Hypercalcemic states, Crohn’s, stents, RTA, infection,
gout, hypercalciuria, hyperuricosuria, cystinuria
• Symptoms– Asymptomatic, flank pain, hematuria
10
Anthony PowellGillian Lieberman, MD
CompositionOPAQUE contains calcium +/ phosphate• Calcium calculi
– Ca oxalate, Ca phosphate
• Struvite calculi– Magnesium ammonium phosphate= triple phosphate
SEMI OPAQUE contains sulphur• Cystine calculiLUCENT• Uric acid stones;Xanthine• Matrix (coagulated mucoid material)

11
Anthony PowellGillian Lieberman, MD
CT Imaging of Stones
• Essentially all renal and ureteral calculi have high attenuation on non-contrast CT (all but matrix stones have atten of > 100HU)
• CT has sensitivity of 97% and specificity of 96%• Can also see hydronephrosis, hydroureter, renal
enlargement, or perirenal stranding• Must differentiate from phlebolith which is a
calcified blood clot in a pelvic vein.(appearance: round/ovoid, smooth, central lucency, in true pelvis)
12
Anthony PowellGillian Lieberman, MD
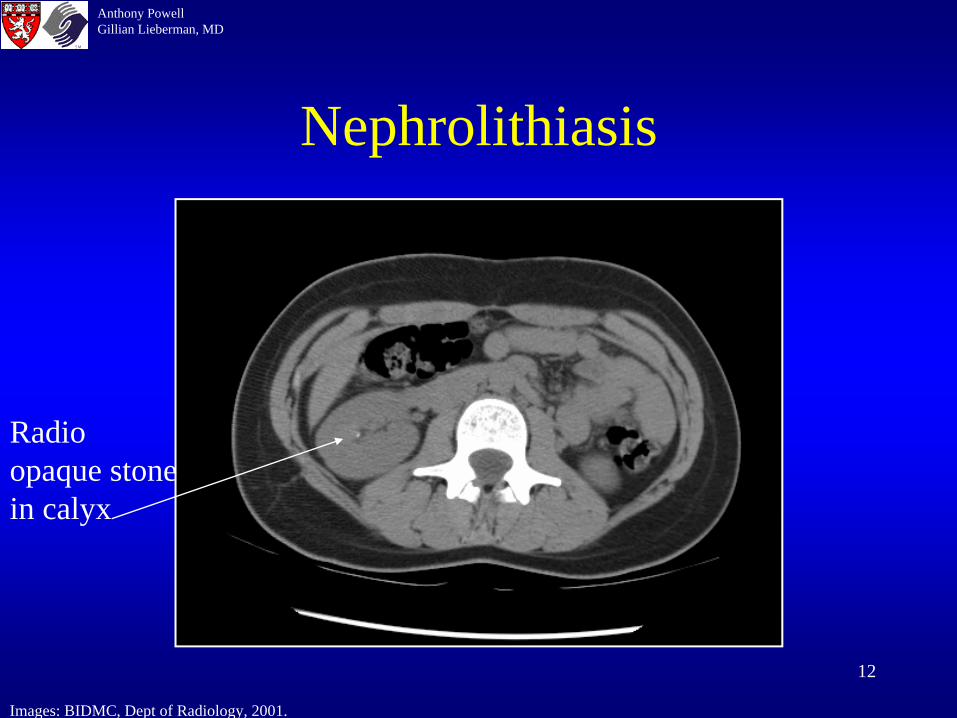
Nephrolithiasis
Images: BIDMC, Dept of Radiology, 2001.
Radio opaque stone in calyx
13
Anthony PowellGillian Lieberman, MD
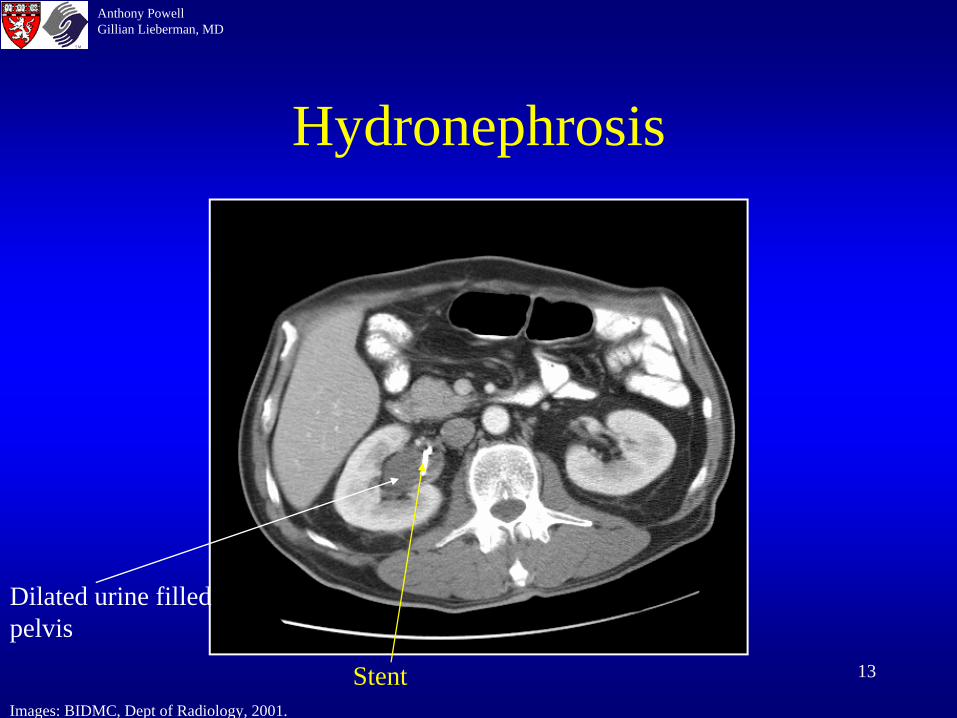
Hydronephrosis
Images: BIDMC, Dept of Radiology, 2001.
Dilated urine filled pelvis
Stent
14
Anthony PowellGillian Lieberman, MD
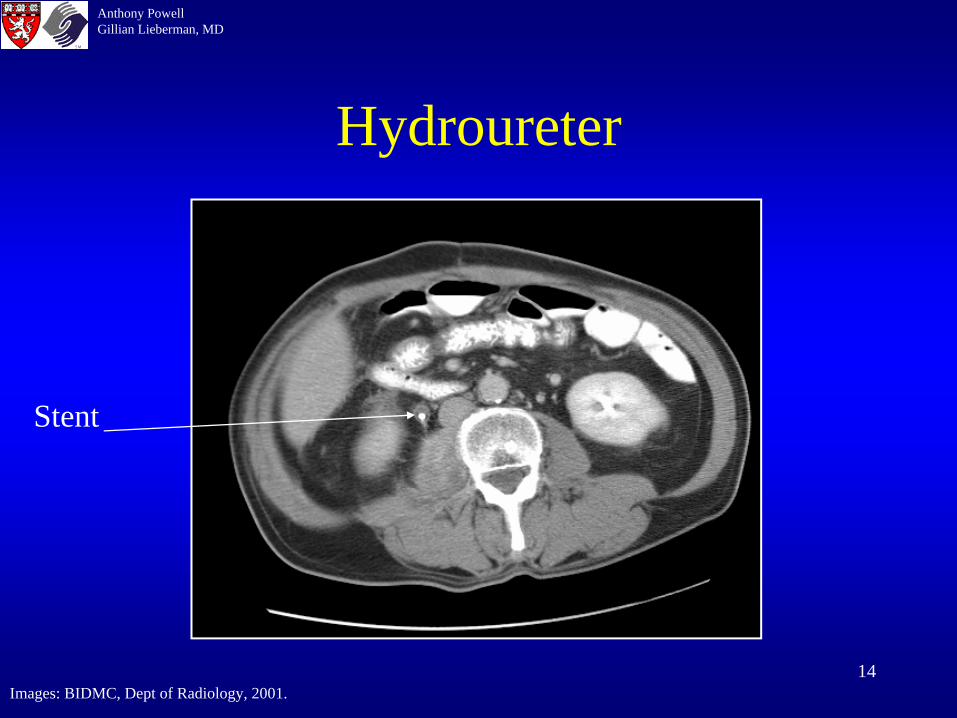
Hydroureter
Images: BIDMC, Dept of Radiology, 2001.
Stent
15
Anthony PowellGillian Lieberman, MD
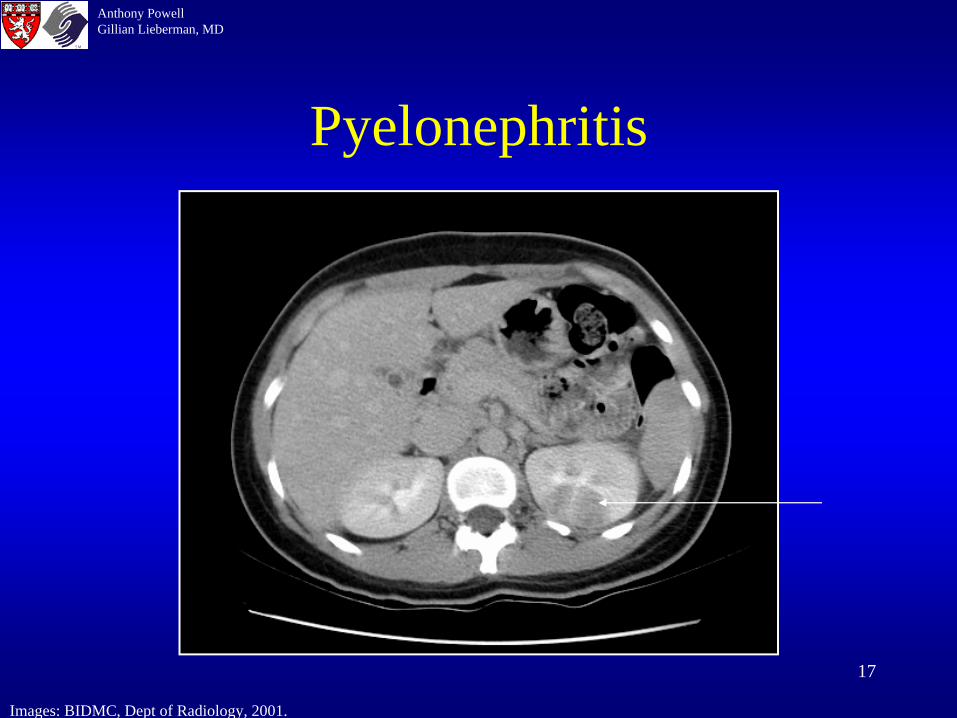
Pyelonephritis
• Bacterial infection of portions of renal parenchyma
• Usually via ascending infection from the bladder• Risk Factors include vesicoureteral reflux, DM,
pregnancy, immunocompromised states, prolonged catheterization, neurogenic bladder
• Sx’s include flank pain, fever, pyuria, leukocytosis• Usual suspects E. coli, proteus, klebsiella
16
Anthony PowellGillian Lieberman, MD
CT Imaging of Pyelonephritis
• Focal or diffuse renal enlargement• Parenchyma may be low in attenuation on non-
contrast (C-) images• Usually wedge-shaped regions of decreased
enhancement on C+ images• Perinephric stranding or fluid collections, often w/
thickening of Gerota’s fascia
17
Anthony PowellGillian Lieberman, MD
Pyelonephritis
Images: BIDMC, Dept of Radiology, 2001.
18
Anthony PowellGillian Lieberman, MD
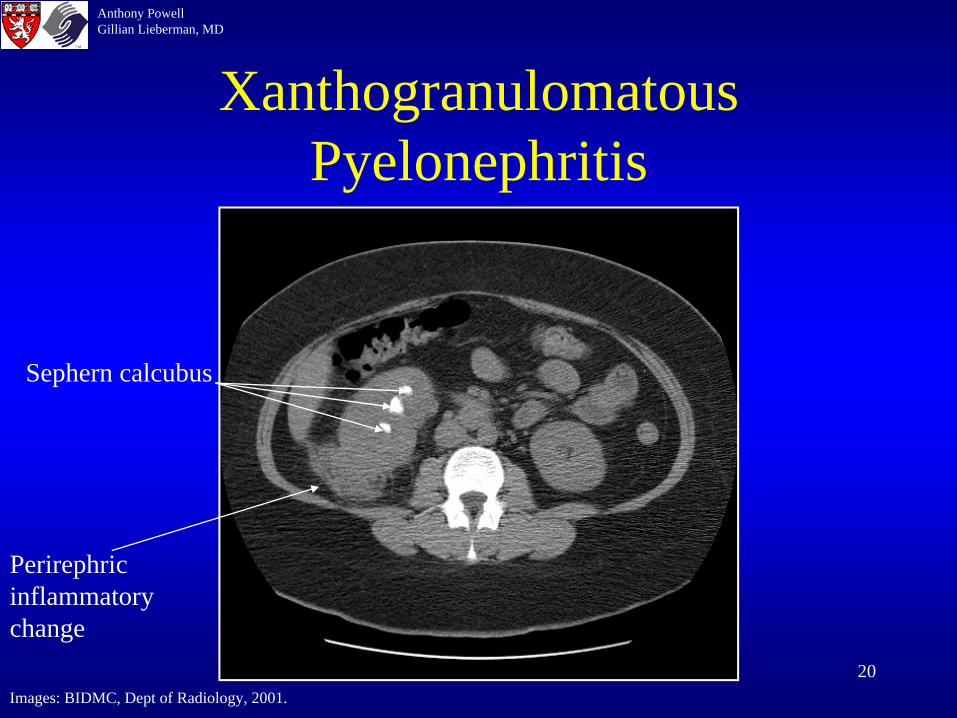
Xanthogranulomatous Pyelonephritis (XGP)
• Bacterial renal infection with an unusual/characteristic immune response
• Parenchyma infiltrated with lipid-laden macrophages
• Proteus mirabilis is usual causative organism• Associated with staghorn calculus• Often chronic, non-spec sx’s fever, malaise,
pain, leukocytosis
19
Anthony PowellGillian Lieberman, MD
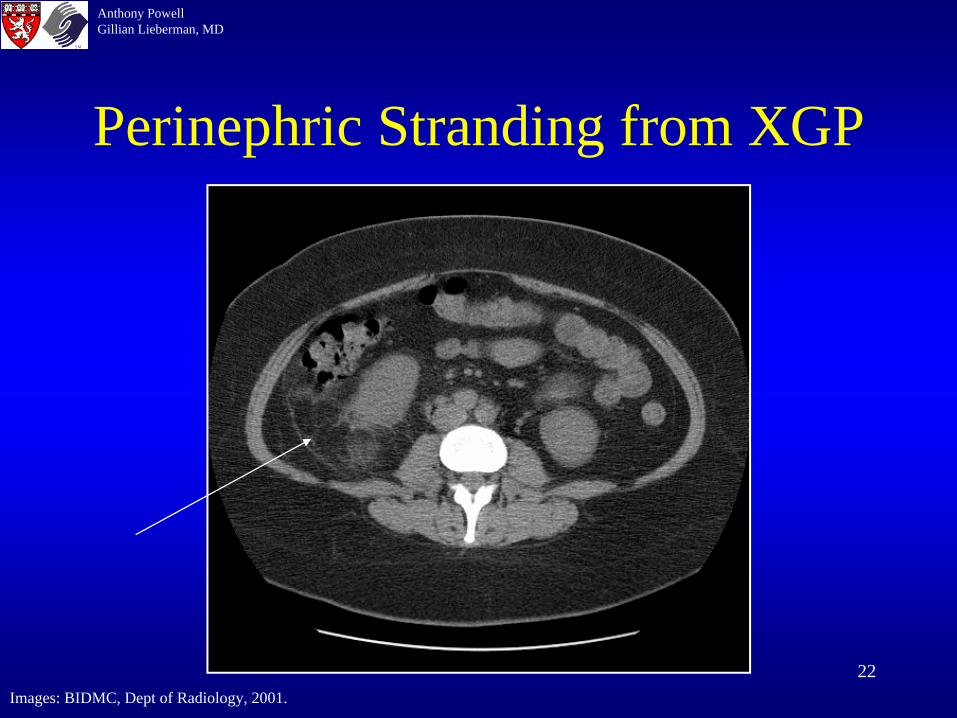
CT Characteristics of XGP
• May demonstrate classic finding of staghorn calculus
• Low-attenuation renal mass; decreased excretion of contrast
• Enlarged kidney• Perinephric inflammatory changes• 85% of cases have diffuse renal involvement
20
Anthony PowellGillian Lieberman, MD
Xanthogranulomatous Pyelonephritis
Images: BIDMC, Dept of Radiology, 2001.
Perirephric inflammatory change
Sephern calcubus

21
Anthony PowellGillian Lieberman, MD
XGP with Staghorn Calculus
Images: BIDMC, Dept of Radiology, 2001.
22
Anthony PowellGillian Lieberman, MD
Perinephric Stranding from XGP
Images: BIDMC, Dept of Radiology, 2001.
23
Anthony PowellGillian Lieberman, MD
Renal Cystic Disease
• Very common 50% of pts over age of 50• Assoc w/ many syndromes, etiology unknown,
probably arise from obstructed tubules or ducts• Most commonly asymptomatic• Rarely, may have hematuria, HTN, cyst infection,
or mass effect
24
Anthony PowellGillian Lieberman, MD
CT Characteristics of Simple Cysts
• Smooth, imperceptible cyst wall• Sharp demarcation from surrounding renal
parenchyma• Water attenuation (<15 HU), homogenous
throughout lesion• Non-enhancing• Simple cysts are w/o septations or calcification• May have slight elevation of adjacent renal
parenchyma Beak sign

25
Anthony PowellGillian Lieberman, MD
Complex Cysts: Categorized using the Bosniak Classification• Categories based on imaging features that are
intended to serve as guideline for estimating likelihood of malignancyType I- simple cystType II- mildly complicated cyst mild Ca2+, thin
septations, no enhancementIIF- slightly more complex type II lesions
Type III- complex cysts thick wall; multiple, irreg, thick septations/calcifications, no enhancement
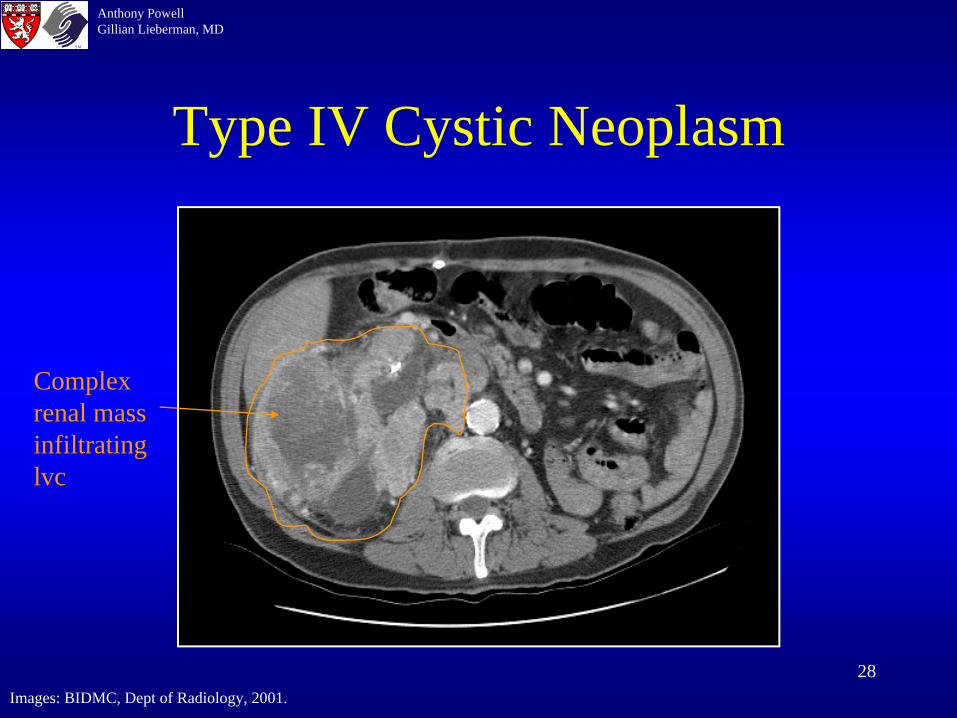
Type IV- cystic neoplasm enhancing wall or solid component
26
Anthony PowellGillian Lieberman, MD
Treatment
• Type I – no f/u required• Type II – no f/u required• Type IIF – f/u CT after 3-6 months• Type III – Excision• Type IV - Excision
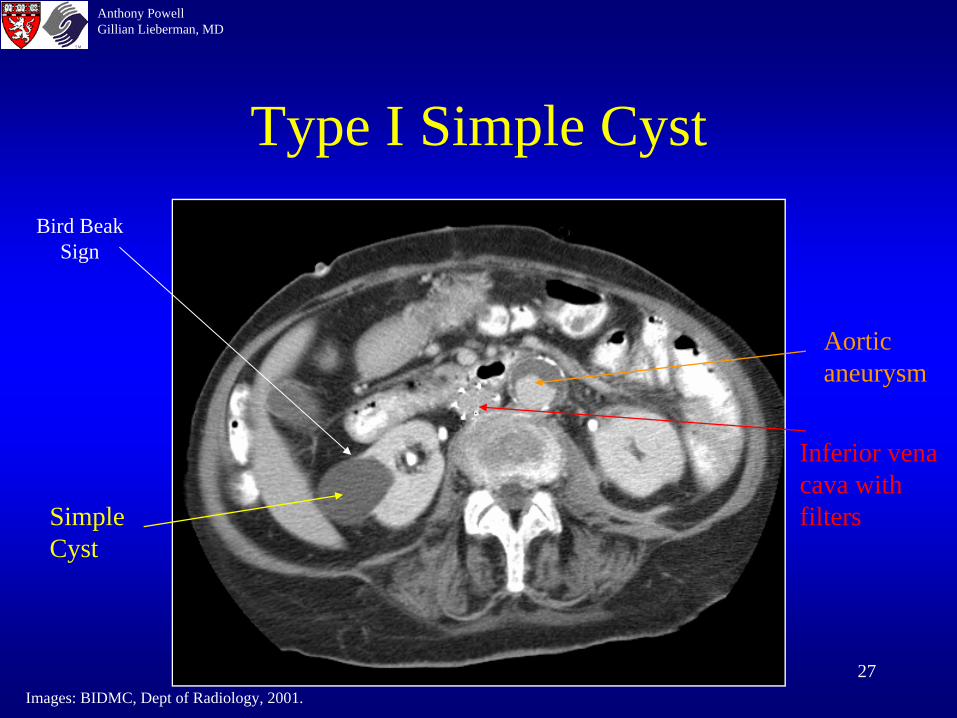
27
Anthony PowellGillian Lieberman, MD
Type I Simple CystBird Beak
Sign
Images: BIDMC, Dept of Radiology, 2001.
Simple Cyst
Aortic aneurysm
Inferior vena cava with filters
28
Anthony PowellGillian Lieberman, MD
Type IV Cystic Neoplasm
Images: BIDMC, Dept of Radiology, 2001.
Complex renal mass infiltrating lvc

29
Anthony PowellGillian Lieberman, MD
Conditions Associated with Multiple Cysts
• Autosomal Dominant PCKD• Autosomal Recessive PCKD• Acquired Cystic Disease (hemodialysis pts)• Von-Hippel-Lindau disease• Tuberous Sclerosis• Medullary Sponge Kidney

30
Anthony PowellGillian Lieberman, MD
Benign Masses
• Cysts• Angiomyolipoma• Oncocytoma (via epithelial cells of prox tubule)• Renal Adenoma • Mesoblastic Nephroma (hamartomatous tumor,
usu present at birth)• Hemangioma• Various Renal Pelvic Tumors(papilloma, angioma,
fibroma)• Hematoma
31
Anthony PowellGillian Lieberman, MD
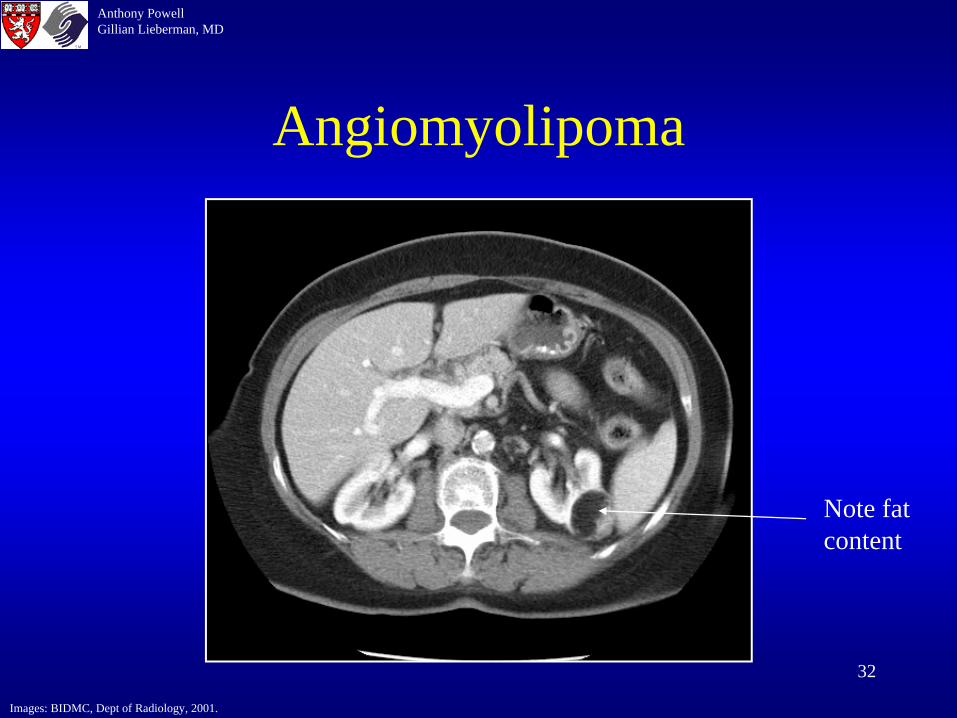
Angiomyolipoma
• Hamartomas containing fat, smooth muscle, and blood vessels
• Usually asymptomatic, but may spontaneously bleed
• Large AMLs resected or embolized• Multiple AMLS usually Associated w/ tuberous
sclerosis• On CT *fat attenuation in mass*, strong
contrast enhancement (RCCs rarely contain fat), no Ca2+
32
Anthony PowellGillian Lieberman, MD
Angiomyolipoma
Images: BIDMC, Dept of Radiology, 2001.
Note fat content

33
Anthony PowellGillian Lieberman, MD
Malignant Masses
• Renal Cell Cancer• Transitional Cell Cancer• Wilm’s Tumor • Nephroblastomatosis (multiple rests of
embryologic metanephric blastoma)• Lymphoma• Metastases (lung, breast, colon, melanoma)

34
Anthony PowellGillian Lieberman, MD
Renal Cell Ca
• Most common primary renal malignancy (85% of primary renal tumors)
• Assoc w/ smoking, family hx, age, Von Hippel- Lindau, Acquired Cystic Disease/chronic dialysis, phenacetin abuse
• Presentation: Hematuria, flank pain, wt loss, palp mass, fever, anemia, paraneoplastic syndromes
• liver enzymes w/o mets Stauffer syndrome

35
Anthony PowellGillian Lieberman, MD
CT characteristics
• Variable from complex cyst to large, heterogeneous renal mass
• Generally enhancing• May have calcifications• May have hemorrhage and central necrosis• Usually no fat
36
Anthony PowellGillian Lieberman, MD
Robson Staging
• Stage I – contained w/in renal capsule• Stage II – contained w/in Gerota’s fascia• Stage III
A – venous invasion (renal v, IVC)B – lymphatic invasion C – both
• Stage IV – distant metastasis (lungs, liver, lytic bone, adrenal, contra renal)

37
Anthony PowellGillian Lieberman, MD
Renal Cell Ca
Images: BIDMC, Dept of Radiology, 2001.

38
Anthony PowellGillian Lieberman, MD
RCC
Images: BIDMC, Dept of Radiology, 2001.

39
Anthony PowellGillian Lieberman, MD
References• Netter, FH: Atlas of Human Anatomy, 2nd ed. Novartis, 1997• Slone RM, Fisher AJ, Pickhardt PJ, Gutierrez FR, Balfe DM: Body
CT, A Practical Approach, 1st ed. McGraw-Hill, 2000• Weissleder R, Rieumont MJ, Wittenberg J: Primer of Diagnostic
Imaging, 2nd ed. Mosby, 1997• Beth Israel Deaconess Medical Center, Dept of Radiology, Teaching
Files, 2001• Gay SB, Woodcock RJ: Radiology Recall, 1st ed. Lippincott Williams
and Wilkins, 2000

40
Anthony PowellGillian Lieberman, MD
Acknowledgements
• Pamela Lepkowski• Gillian Lieberman M.D.• Richard Cooper M.D.• Joe Barry M.D.• Mary Keogan M.D.





























