Embed Size (px)
Citation preview

CT enterography for Crohn’s disease: optimaltechnique and imaging issues
Mark E. Baker,1 Amy K. Hara,2 Joel F. Platt,3 Dean D. T. Maglinte,4 Joel G. Fletcher5
1Imaging Institute/L10, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland Clinic,
9500 Euclid Ave, Cleveland, OH 44195, USA2Mayo Clinic School of Medicine, Mayo Clinic, Scottsdale, AZ, USA3University of Michigan School of Medicine University of Michigan Health System, Ann Arbor, MI, USA4Indiana University School of Medicine Indiana University Health, Indianapolis, IN, USA5Mayo Clinic School of Medicine, Rochester, MN, USA
Abstract
CT enterography (CTE) is a common examination forpatients with Crohn’s disease. In order to achieve highquality, diagnostic images, proper technique is required.The purpose of this treatise is to review the processes andtechniques that can optimize CTE for patients withsuspected or known Crohn’s disease. We will review thefollowing: (1) how to start a CT enterography program;(2) workflow issues, including patient and orderingphysician education and preparation; (3) oral contrastmedia options and administration regimens; (4) intrave-nous contrast media injection for uniphasic and multi-phasic studies; (5) CTE radiation dose reductionstrategies and the use of iterative reconstruction in lowerdose examinations; (6) image reconstruction and inter-pretation; (7) imaging Crohn’s patients in the acute oremergency department setting; (8) limitations of CTE aswell as alternatives such as MRE or barium fluoroscopicexaminations; and (9) dictation templates and a commonnomenclature for reporting findings of CTE in Crohn’sdisease. Many of the issues discussed are summarized inthe Abdominal Radiology Society Consensus MDCTEnterography Acquisition Protocol for Crohn’s Disease
Key words: CT Enterography—Technique and issues
In 1987, both Raptopoulous et al and Thoeni and Filsondescribed the use of neutral enteric oral contrast media inabdominal CT (whole milk and polyethylene glycol,respectively) in abdominal and pelvic CT [1, 2]. Later,Raptopoulos and co-workers introduced the term CT
enterography when describing a technique utilizing largevolumes (1–1.5 L) of a 2% barium-based or 2%–2.5%water soluble iodine-based oral contrast media [3, 4]. Asubsequent investigation describe the use of an isotonicoral agent [5]. With the evolution of multidetector CT(MDCT) and volume scanning and reconstruction aswell as commercially available neutral oral contrastagents, CT enterography (CTE) was subsequently refinedand developed worldwide. In the last decade, CTE hasbecome one of, if not the most common imaging exam-ination in patients with suspected or known Crohn’sdisease, especially in the United States.
In order to achieve a high level of efficacy, optimaltechnique is critical, especially in evaluating patients withobscure gastrointestinal bleeding [6–22]. Further, be-cause CT is now the greatest, single source of non-background ionizing radiation in the United States [23](exposure from medical sources of ionizing radiation in2006 accounted for 48% of the total exposure as opposedto 50% from background; CT contributes 49% of themedical exposure), dose reduction techniques should beutilized, especially in Crohn’s patients, given the chro-nicity of their disease and the likelihood that they willhave repeated examinations in their lifetime.
The purpose of this treatise is to review the processesand techniques that can optimize CTE for patients withsuspected or known Crohn’s disease. We will review thefollowing: (1) how to start a CT enterography program;(2) workflow issues, including patient and orderingphysician education and preparation; (3) oral contrastmedia options and administration regimens; (4) intrave-nous contrast media injection for uniphasic and multi-phasic studies; (5) CTE radiation dose reductionstrategies and the use of iterative reconstruction in lowerdose examinations; (6) image reconstruction and inter-
Correspondence to: Mark E. Baker; email: [email protected]
ª Springer Science+Business Media New York 2015
Published online: 31 January 2015AbdominalImaging
Abdom Imaging (2015) 40:938–952
DOI: 10.1007/s00261-015-0357-4

pretation; (7) imaging Crohn’s patients in the acute oremergency department setting; (8) limitations of CTE aswell as alternatives such as MRE or barium fluoroscopicexaminations; and (9) dictation templates and a commonnomenclature for reporting findings of CTE in Crohn’sdisease. Many of the issues discussed are summarized inthe Abdominal Radiology Society Consensus MDCTEnterography Acquisition Protocol for Crohn’s Disease(Table 1).
How to start a CT enterographyprogram
For an effective CTE program to function, severalimportant key elements must be in place. First, on theimaging side, there must be a champion radiologist,technologist, and nurse that will drive the process andfocus on patients, process, and interpretation of theexamination. The radiologist must be well versed in smallbowel disease, especially in the findings and treatment ofCrohn’s disease, and have a good reputation with refer-ring gastroenterologists, colorectal, and general sur-geons. This individual should have spent time reading theCTE and Crohn’s disease literature as well as attendmeetings and seminars, learning the techniques of inter-preting CTE (for several years, the Society of AbdominalRadiology has provided a one-day course focusing onCTE interpretation). A 16-row MDCT scanner is theminimum requirement for producing 2–3 mm recon-structed slices in multiple planes. It is best to start theprogram in one scanner location, focusing on the peopleand process of CTE. Either a nurse or technologist mustbe assigned the task of instructing and then supervisingthe patient, while ingesting the oral contrast agent. Thisindividual must understand the importance of continu-ous oral contrast ingestion and can often serve as acheerleader, positively encouraging the patient toappropriately ingest the oral agent. A physical areashould be reserved for patients to drink the contrast; anarea easily monitored by the responsible technologist ornurse.
Once the imaging elements are in place, marketing asmall, focused individual or individuals in the gastroen-terology or surgical side of medicine is the next step.Many of these physicians will have already heard aboutCTE at national meetings such as the Digestive DiseaseWeek and the Advances in Inflammatory Bowel Diseasesheld by the Crohn’s and Colitis Foundation. In fact,many gastroenterologists and surgeons cannot get CTEperformed in their community and want this examina-tion for their patients. Starting with a small, interestedgroup will enhance the success of the examination asthese individuals are already fully invested in making theprocess happen. Further, success on a small scale willbreed success on a large scale. When discussing theexamination with this small group, it is important to
stress the patient requirements for a successful exami-nation (see below vis-a-vis oral contrast media ingestion).
Once the ‘‘kinks’’ have been worked out of the sys-tem, and well performed, interpretable exams are beingproduced, the market can be widened by advertising theexamination to a larger number of ordering physicians.The imaging group will likely find that by focusing firston a small number of interested users and providingthem an excellent service and product that when satisfiedthese users will then become their own marketers of theservice. Lastly, once a core group of images has masteredthe process, they should consider expanding the exami-nation location to several sites. However, this core groupshould train the off-site personnel. Further, careful, andongoing assessment of the quality and interpretation ofthese examinations should be performed. As the exami-nation becomes geographically disseminated, it is easy toallow the quality of the exam and its interpretation todeteriorate.
Patient/ordering physician educationand preparation
Over the last 15–20 years, given marked improvements inCT image quality and speed, distinguishing bowel fromother structures without oral contrast opacification inadults is much easier than in the early days of CT. As aresult, many radiologists have become complacent aboutbowel opacification and distension with oral contrastmedia. With CTE, however, this is not the case whereopacifying and distending the small bowel is critical. It istherefore important to first educate the ordering clinicianthat a CTE is distinctly different than a routine abdomenand pelvis CT using positive oral contrast, requiring thatthe patient ingest at least 900–1500 cc of oral agent inapproximately one hour. It is also imperative that theordering clinician, CT nurse and/or technologist stress tothe patient that such an effort is essential for a well-performed study. If the patient arrives without thisknowledge, encouraging them to ingest the oral agent ismuch more difficult. If patients have difficulty ingestingthe required volume of oral contrast, they should be gi-ven the option of having a small feeding tube placed intheir stomach to administer the oral contrast. Surpris-ingly, many patients prefer this method of oral agentadministration.
In practices where enteroclysis expertise is available,some patients have preferred this method with conscioussedation over CTE that requires ingesting a large volumeof oral agent either per mouth or via feeding tube [24].
Workflow set-up and patientsupervision
Ideally, a separate waiting area should be designated forpatients who are about to have a CTE. This area should
M. E. Baker et al.: CT enterography for Crohn’s disease 939

be easily visible to a supervising technologist or nurse.The supervising health care provider should take own-ership in the process and is responsible for determining ifthe patients are complying with the schedule of drinkingthe oral contrast agent. If the patient is not or cannotcomply with the schedule, and does not respond to gentleencouragement, the supervising technologist or nurseshould inform the radiologist. At that time, a determi-nation should be made as to whether a small nasogastricor feeding tube be placed in the stomach, by which theagent can be administered. There are some patients whoeither cannot or will not ingest the minimum amount oforal agent and refuse any sort of oral or nasogastric tube.Some of these patients are too sick to ingest the largevolume of agent. In these cases, we will then perform theexamination after the patient has ingested 500–800 cc oforal agent. Surprisingly, we often find that there isalready a sufficient amount of intrinsic succus entericusfor a diagnostic examination.
Before starting the oral contrast ingestion, we havefound that the IV cannula should be placed first. If dif-ficulties arise from placing an IV, and the patient hasalready started to ingest the oral agent, there will be adelay in initiating the scan. Delay in placing the IV canresult in diarrhea (most oral agents other than water arecathartics) and poor opacification of the small bowel.
Various regimens/schedules exist for the administra-tion of oral contrast (Table 1). In general, most centersrequire the patient ingest at least 900 cc of oral contrastagent. Most require the patient to continuously sip theoral agent. It is better for the patient to sip rather thangulp down the agent in large aliquots. Most regimensrequire that the patient must ingest approximately 450 ccof liquid every 15 min, over 45 min. This results in thepatient ingesting 1350 cc of liquid. In a study fromEssen, investigators found that a volume of 1350 cc waspreferable for optimal small bowel distension; ingestion
of 1800 cc led to a significantly higher rate of crampingand diarrhea; 900 cc yielded sufficient duodenal disten-sion, if imaged soon after ingestion, but led to less jejunaland ileal distension [25]. In this investigation, the subjectswere timed with a stopwatch and ingested the oral agentsat a rate of 40 mL/min, an extremely regimented proto-col and likely not clinically achievable! After one hour,some sites scan their patients; while at other sites, anadditional 250–500 cc of water is administered. In theselater sites, the patient is scanned at 70 min after the startof oral contrast ingestion.
Special considerations should be given to patientswith end ileostomies, ileal-anal pouches, and patientswith ileal-sigmoid or ileal-rectal anastomoses. First, thesepatients do not have or have a short segment of colon.Thus, the neutral contrast will reach the conduit endmuch faster than in patients with a normal length colon.For ileostomy patients, we scan the patients when con-trast reaches the ileostomy bag. Often these patients willingest less than the 900–1350 cc of oral agent. Forpatients with either ileal pouches or a short segment ofremaining colon, we scan the patients when they havetheir first watery bowel movement.
Oral contrast agent choice
Investigations in the late 1980’s and 90’s were the first toexplore the use of low attenuation (<25–30 H.U.), non-barium, or iodine-containing oral agents in abdominalCT [7, 25–35]. Strongly influenced by Alec Megibow, thedevelopment of CTE was further motivated by the for-mulation of VoLumen� by E–Z–EM (now owned byBracco) [7]. Over the last 10 years, a variety of oralagents have been used for CTE. These include water,methylcellulose mixtures with water, VoLumen� (Brac-co), polyethylene glycol, lactulose, and milk. Water is avery acceptable agent for the very proximal bowel
Table 1. 2014 Society of Abdominal Radiology consensus statement on CT enterography acquisition protocol for children and adults with Crohn’sdisease
MDCT scanner with a minimum of 16-detector rowsOral contrast: >900 cc neutral enteric contrast administered in regularly divided doses 45–60 min prior to scanning
For children, 20 cc/kg of oral agentIntravenous contrast: 300 mg/mL iodine; injection rate 3–4 cc/s
For children, 2 cc/kg for children up to 120 ccTiming of image acquisition: enteric to portal phase imaging (50–70 s after beginning of injection)Radiation dose Level: CTDIvol <15 mGy for most patients (<220 pounds)
Protocol adapted for individual patient sizeEncouraged to adapt to patient size using kV selection, automated exposure control, mAs selection, and noise reduction methods (image-based orraw data-based iterative reconstruction)
Planes of reconstruction: axial, coronal, & sagittal (optional based upon purpose of examination and subsequent findings)Slice thickness: axial (2–3 mm); coronal (2–3 mm) and sagittal (2–3 mm)Alternatives if iodinated intravenous contrast cannot or should not be used
Contrast-enhanced MRENon-contrast-enhanced MRE if severe CKDAddition of diffusion weighted imaging (see SAR Consensus MR Enterography Acquisition Protocol)
If CT is used, large volumes of positive enteric contrast should be administered (this method is considered inferior to a non-contrast-enhancedMRE)Dedicated small bowel examination utilizing barium and regular, dedicated fluoroscopic techniques by an experienced imager (rotation andpalpation)
940 M. E. Baker et al.: CT enterography for Crohn’s disease

(stomach, duodenum and proximal jejunum). However,because water is normally absorbed in the more distalsmall bowel, it is ineffective in luminal opacification anddistention [32]. Thus, higher osmolality agents or agentsthat retain fluid, such as those containing methylcellu-lose, polyethylene glycol, or sugars such as sorbitol andlactulose, and even milk, are more effective in main-taining small bowel opacification and distension.
In a comparison of 2 L of water, methylcellulose,polyethylene glycol, or 1.35 L of low concentrationbarium (LCB, i.e., VoLumen�) followed by 0.5 L ofwater, PEG, and LCB distended the small bowel loopsmore than water or methylcellulose [33]. Optimal ter-minal ileal distention time after start of ingestion was51–72 min. Water and methylcellulose had fewer sideeffects; water was the most preferred agent and PEGthe least. Gas and/or diarrhea are the most commonside effects.
In the previously mentioned study from Essen, water,locust bean gum with 5% mannitol, and VoLumen with1.4% sorbitol and 2% sorbitol were ingested [25].Regardless of the agent, volumes of up to 1350 mL wereassociated with no or only mild side effects or objections.However, 1800 mL of contrast agent led to a signifi-cantly higher rate of diarrhea and cramps, higher for thesorbitol containing agents. All agents but water yieldedequivalent levels of small bowel distension.
Consistent bowel opacification
Regardless of techniques utilized, most if not all radiol-ogists encounter examinations with inconsistent bowellumen opacification and distention (Figs. 1, 2). Thejejunum is the most difficult segment of bowel to opacify.In the standard small bowel series, overhead films areroutinely obtained to determine the level of stomachopacification and the location of the barium column inthe small bowel. If the stomach is collapsed, it is easy tohave the patient ingest more barium, as keeping thestomach full, promotes continued small bowel peristalsis.Unfortunately, we do not have the ability to periodicallyassess the level of gastric distention with oral contrastagents nor determine the location of the contrast in thesmall bowel. This is why the consistent and almostcontinuous sipping of contrast is helpful in maintaininguniform small bowel opacification and distention.
Prone imaging, employed by many centers in MRE,may promote jejunal opacification and distention. Somecenters utilize anti-spasmolytics, such as glucagon andLevsin, in order to promote small bowel opacification.
Lastly, it is important to recognize that at least withCrohn’s disease, most active disease will be detected evenwhen the bowel opacification and distention is inconsis-tent. Because of depressed peristalsis, virtually all seg-ments of affected bowel will have some fluid present
upstream to the disease site. Further, virtually all seg-ments of disease, small bowel will have important otherfindings of wall thickening (>3 mm) and hyperen-hancement (either mural stratification or homogeneoushyperenhancement) [5, 8]. Extra-mural findings such asdistended vasa recta, fibrofatty proliferation, sinus tractor fistulae, and abscess may also be present. In otherwords, luminal narrowing is not the only sign ofabnormal bowel. These additional signs are all importantmethods of distinguishing a segment of small bowel withCrohn’s disease from a segment that is collapsed orcontracting.
Intravenous contrast enhancement
Iodinated contrast media enhancement is essential indetecting active inflammatory small bowel Crohn’s dis-ease as well as penetrating disease. In Crohn’s disease, ifthe patient cannot receive iodinated contrast mediabecause of a severe contrast allergy or CKD, one shouldconsider an MRE. In cases of severe CKD, when gado-linium cannot or should not be administered due to thepossibility of systemic nephrogenic fibrosis, the alterna-tives include a fluoroscopic small bowel barium study oran unenhanced MRE, relying on the heavily weightedT2-weighted and diffusion weighted pulse sequences. Inpractices where expertise is available, in instances wheregadolinium cannot be administered, an alternative is CTenteroclysis with positive enteral contrast.
In routine, uniphasic scanning, most institutions usecontrast media that contain 300 mg/mL of organic io-dine. In most cases, at least 120–150 cc of contrast mediais injected, with dose adjustment based on patient’sweight when patients weigh <100–125 pounds.
For multiphasic scanning, many institutions usecontrast media that contains more organic iodine, from350–370 mg/mL. For more concentrated iodine-con-taining contrast media, the volume of contrast media isadjusted downward so that the patient does not receivemore than a total of 60–70 g of organic iodine. The rate
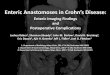
Fig. 1. Normal CTE with suboptimal small bowel distension.A shows collapsed jejunum (long arrow) on the axial image inthe upper abdomen. B shows relatively collapsed jejunum(long arrow) and ileum (short arrow) on the axial image in themid abdomen. C shows a small amount of contrast in theterminal ileum (long arrow) on the axial image in the pelvis. Dshows contrast-filled ileum (note no folds) (short arrow) on thecoronal view in the anterior abdomen. E shows collapsedjejunum (long arrow) in the left upper quadrant and contrast ina relatively non-distended loop of ileum (short arrow) in theright mid abdomen on the coronal view in the mid abdomen. Fshows relatively collapsed jejunum (long arrow) and smallamount of contrast in the terminal ileum (short arrow) on thecoronal view in the posterior abdomen.
c
M. E. Baker et al.: CT enterography for Crohn’s disease 941

of contrast media injection depends upon the size of thecatheter used, the viscosity of the contrast media, and thelocation of the vein used. In general, for uniphasicscanning, most institutions inject the contrast media at a
rate of 3 cc/s, with some institutions attempting to injectat a rate of 4 cc/s. For multiphasic scanning, the arterialphase is best achieved by injecting the contrast media at arate of 4–6 cc/s.
942 M. E. Baker et al.: CT enterography for Crohn’s disease

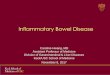
Fig. 2. Normal CTE with optimally distended mid to distaljejunum, with proximal jejunum still not distended. This is avery common result as it is very difficult, if not impossible toscan when the proximal jejunum is distended with the neutraloral contrast agent. A shows collapsed loops of jejunum (longarrow) on the axial image in the upper abdomen. B showsmore contrast-filled jejunal loops (note folds) (long arrow) on
the axial image in the upper abdomen. C shows contrast-filledileal loops (short arrow) on the axial image in the lowerabdomen. D shows fluid-filled distal jejunum or proximal ileum(fewer folds present) (short arrow) on the coronal view in themid abdomen. E shows collapsed jejunal folds (long arrow)and more contrast-filled ileum (short arrow) on the coronalview in the mid to posterior abdomen.
M. E. Baker et al.: CT enterography for Crohn’s disease 943

Scanner timing vis-a-vis contrastmedian injection (uniphasic andmultiphasic)
Uniphasic examinations: primary use for knownor suspected Crohn’s disease
For Crohn’s disease, CTE employs MDCT with narrowsection thickness and reconstruction interval, intrave-nous contrast material, and large volumes of neutralcontrast agent to distend the lumen in an effort to im-prove the detection of small bowel inflammation andextracolonic complications. CTE can be performed dur-ing the enteric phase (45–50 s after injection) [36] and theportal venous phase (70 s after injection). Maximumpeak small bowel wall enhancement occurs during theenteric phase (50 s post-contrast media injection) [36]. Asa result, many centers scan at 50 s. However, thisinvestigation did not take into account the location ofsmall bowel. Subsequent work has shown that jejunalattenuation is greater than ileal attenuation, and col-lapsed bowel loops demonstrate greater attenuation thandistended bowel loops [13]. Another investigationshowed that there is no significant difference in detectingCrohn’s disease when the enteric phase is compared tothe portal venous phase [37]. Lastly, there is also someMR data that suggest more delayed imaging, up to 5–7 min, may detect more disease [38]. At the ClevelandClinic, using the 128 MDCT scanners, because thescanners are very fast and scanning often occurs duringthe later arterial phase, our portal venous phases havebeen adjusted to start at 90 s rather than 70 s.
Multiphasic examinations for suspectedmesenteric ischemia or obscure gastrointestinalbleeding
Multiphasic examinations after the administration ofintravenous contrast media are rarely used in patientswith known or suspected Crohn’s disease. These exam-inations are reserved for patients with obscure or acutegastrointestinal tract bleeding and Soto et al describe thetechnique in the article in this issue.
Dose reduction strategies and iterativereconstruction
Every effort should be made to limit the radiationexposure from CT in all patients, especially, in patientswith Crohn’s disease. Several studies have shown thatsome Crohn’s patients can receive large cumulative doses(over 100 mSv) over the course of their disease, and oftenare examined with CT two to three times a year [39–45].In one series, encompassing a 15-year period of time, themean ionizing radiation dose was 36.1 mSv [41]. Over theentire study period, there was an increasing use of CT,
and while CT accounted for only 16.2% of all imagingstudies, it accounted for 77.2% of the radiation dose.Further in that study, the total ionizing radiationexceeded 75 mSv in 15.5% of the patients. Patients whoreceived higher doses had disease onset before 17 yearsof age, upper gastrointestinal tract or penetrating dis-ease, required intravenous steroids or infliximab or hadmultiple surgeries. There is recent evidence that radiationexposure from CT scans in children results in anincreased risk of brain tumors and leukemia [46, 47].Most pediatric centers almost exclusively use MR orultrasound as a means of evaluating younger patients.
Efforts to reduce the dose from CT are ongoing andinclude alterations in kVp and mAs vis-a-vis body hab-itus, lateral body width, weight, and BMI, altering thescan pitch as well as applying new reconstruction tech-niques to lower dose examinations, generally termediterative reconstruction. Dose reductions from CTDIvolof 15–20 to <10 mGy and even below 5 mGy have beenachieved [48–56]. However, the most substantial reduc-tions in dose have been in smaller patients who weigh lessthan 160–180 pounds (Fig. 3).
A growing concern among radiologists is what dataare lost with lower dose examinations. All the knowniterative reconstruction techniques lower the noise levelon these lower dose exams; often below ‘‘full’’ dose noiselevel examinations reconstructed with standard filteredback projection techniques. However, there is growingevidence that these iterative reconstruction techniquescannot overcome low-contrast object detection loss dueto noise [57–65]. Small, low-contrast objects (a lowerattenuation mass in an enhanced liver for instance) aremuch more difficult to detect by the human eye whencompared to higher contrast objects [59]. Further, todate, low-contrast object detection (an object of lowerattenuation vis-a-vis background) is lost with lower doseMDCT, even with any of the known iterative recon-struction techniques, including model-based iterativereconstruction, which processes only raw data ratherthan the faster, hybrid forms of IR. To summarize, un-like weighted filtered back projection, spatial resolutionis contrast-dependent for IR (i.e., no loss of spatial res-olution for high-contrast objects). However, using IR,there is often loss of low-contrast resolution.
Crohn’s disease identification is a high-contrast issuewith CT (i.e., identifying a process with a higher atten-uation vis-a-vis background). Studies using lower dosetechniques have shown that reducing exposure does notresult in a reduction in diagnostic efficacy of small bowelCrohn’s disease. However, we do not know how muchwe can reduce the dose without losing this efficacy. Iflower dose CTE is utilized in a patient with Crohn’sdisease, radiologists may have to accept a lower sensi-tivity in detecting low attenuation lesions in the liver, thelow-contrast objects that are most readily present in a
944 M. E. Baker et al.: CT enterography for Crohn’s disease

patient population. Fortunately, identifying smaller, low-contrast hepatic lesions are much less important inpatients with Crohn’s disease than in patients with aprimary malignancy.
At the Cleveland Clinic, we routinely employ anattenuation-based automated tube voltage selection toolfor all of our CTE examinations (CARE kV, SiemensHealthcare). In patients less than 200–200 pounds, thetool almost always utilizes 100 kVp, and, thus, lowers thedose (it is vitally important to ensure that the patient iscentered in the CT gantry in order for this tool to be
effective). If the patient is not centered, inappropriateassumptions will be made by the software, often resultingin the use of either 120 or 140 kVp, markedly increasingthe patient’s dose). We also use a weight-based approachto setting the quality reference tube current–exposuretime product (mAs) (qmAs = 1 mAs* patient weight(lbs) (up to 220 pounds) [66, 67]. In the near future, wewill likely reduce the qmAs to ½ mAs*patient weight(lbs) and apply iterative reconstruction. In a recentlypresented, multi-reader, objective, and subjective inves-tigation at Cleveland Clinic using CARE kV and a
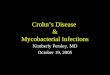
Fig. 3. Patient with Crohn’s colitis s/p colectomy withrectal remnant scanned in 2006 before any changes in CTenterography protocol and in 2014 with new protocol. A, Bare axial and coronal images, respectively, from the 2006exam showing the diseased rectosigmoid remnant (arrow).In 2006, the patient weighed 114 pounds. The techniqueused was 120 kVp with a quality reference mAs of 200.The resulting CTDIvol was 9.59 mGy. C, D are axial and
coronal images, respectively, from the 2014 exam showingthe diseased rectosigmoid (arrow). In 2014, the patientweighed 113 pounds. In 2014, CARE kV was used with aquality reference mAs of 113 (the tube voltage selectedwas 100 kVp). The resulting CTDIvol was 5.12 mGy. Onall sets of images, the stratified enhancement patternof active colonic Crohn’s disease is easily identifiable(arrows).
M. E. Baker et al.: CT enterography for Crohn’s disease 945

weight-based mAs, half-dose imaging was statisticallynon-inferior to full dose imaging in detecting activeinflammatory terminal ileal Crohn’s disease, using bothfiltered back projection and iterative reconstruction(sonogram-affirmed iterative reconstruction) (CTDIvol ½dose mean = 6.55 mGy, median = 3.68 mGy, range-181–22.25 mGy; population mean weight = 165 pounds(range = 94–315 pounds) (median weight = 143 pounds;population mean BMI = 25.68 (range = 16.6–54)(median = 22.33) (mean ROC curve areas = 0.908–0.935 for all doses & reconstructions) (Figs. 4, 5) [68].Interestingly, more of the half-dose images, regardlessof reconstruction were subjectively deemed suboptimalor non-diagnostic than those at full dose reconstructedwith filtered back projection. However, regardless ofthis subjective assessment by the readers, their accuracyin distinguishing active inflammatory Crohn’s disease
from normal was not affected. Given these findings, it isvery likely we can reduce the dose to a third of ouroriginal, already lower dose scans in patients with sus-pected or known Crohn’s disease.
Reconstruction strategies
Using a modern PACS and workstation, theoretically, aradiologist does not need to reconstruct the scan data inmultiple planes. However, the referring clinicians, oftengastroenterologists and surgeons, want and need toreview the examination themselves. We have found thatmulti-planar reconstructions in orthogonal planes areessential in the evaluation of Crohn’s disease and inpatients with obscure gastrointestinal bleeding. In Cro-hn’s disease, a fistula or sinus tract may not be visualizedin one plane and obvious in another. The most common
Fig. 4. Patient weighing 108 pounds with mixed stenotic andactive inflammatory small bowel Crohn’s disease of the ileumscanned usingCAREkVat full and half-dose, and reconstructedwith filtered back projection (FBP) and iterative reconstruction(sonogram-affirmed iterative reconstructionorSAFIRE). Imagesat full dose (A), half-dose reconstructed with FBP (B), half-dosereconstructed with SAFIRE, strength 3 (C), and half-dosereconstructed with SAFIRE strength 4 (D). Tube voltageselected was 100 kVp; quality reference mAs was 108. The
CTDIvol at full dose was 4.86 mGy (half-dose = 2.43 mGy)(SSDE = 7.4 mGy full dose; half-dose = 3.7 mGy). The ilealdisease (arrow) is easily identified on all the scans, including thehalf-dose images reconstructedwith filteredbackprojection.Thedisease is mixed stenotic and active inflammatory for the fol-lowing reasons: stratified enhancement pattern, luminal nar-rowing, and upstream dilation. The half-dose images wereobtained by extracting the scan data from one tube, operating at50% output, from a dual-source CT scanner.
946 M. E. Baker et al.: CT enterography for Crohn’s disease

would be an entero-vesicular fistula, often not visualizedaxially, but easily identified in the coronal or sagittalplane. In general, only the axial and coronal planes arereconstructed, with sagittal reconstruction reserved forcases of suspected mesenteric ischemia or where the planeadds information to the axial and coronal images.
Interpretation techniques
Using a workstation, radiologists should page throughthe examination specifically assessing the bowel in a
continuous fashion. This is the surrogate for rotationand palpation used in the fluoroscopic examination ofthe small bowel. In the axial plane, this paging results ina cephalad, caudad, etc., approach. In the coronal plane,this paging results in an anterior, posterior, anterior, etc.,approach. Altering the window and level as the inter-pretation process continues is essential. Some of us assessthe bowel using narrow windows, much like liver win-dows, in order to detect the high attenuation, hyperen-hancing patterns of Crohn’s disease and hyperenhancingsmall bowel tumors such as carcinoids. However, it is
Fig. 5. Patient weighing 255 pounds with subtle, activeinflammatory neo-terminal ileal disease without luminal nar-rowing using CARE kV at full and half-dose, and recon-structed with filtered back projection (FBP) and iterativereconstruction (sonogram-affirmed iterative reconstruction orSAFIRE). Images at full dose (A), half-dose reconstructedwith FBP (B), half-dose reconstructed with sonogram-affirmedSAFIRE, strength 3 (C), and half-dose reconstructed withSAFIRE, strength 4 (D). Tube voltage selected was 120 kVp;quality reference mAs was 220. The CTDIvol at full dosewas 38.27 mGy (half-dose = 19.13 mGy) (SSDE full dose =
34.2 mGy; half-dose = 17.1 mGy). The ileal disease is iden-tifiable on all the scans (arrow), but more difficult on the half-dose image reconstructed with FBP (B) where there is morenoise. In obese patients, more subtle disease could beobscured with doses lower than used here, unless the data isreconstructed with some form of iterative reconstruction.Using the dictation format, the impression on this patientshould be active inflammatory small bowel Crohn’s diseasewithout luminal narrowing. The half-dose images wereobtained by extracting the scan data from one tube, operatingat 50% output, from a dual-source CT scanner.
M. E. Baker et al.: CT enterography for Crohn’s disease 947

also important to view the image dataset using soft tissueand even wider windows, as some tumors are not hype-renhancing and may be subtly similar to the water tonear water attenuation oral contrast.
Even though the findings on a static CTE are notidentical to the findings of a fluoroscopic study, there aresurrogates on CTE than can assist the radiologist inidentifying disease. The small bowel is attached to amesentery that extends diagonally from the left upperquadrant to the right lower quadrant, assuming norotational variation. In a virgin belly, the bowel undulatesand moves with peristalsis in a curving, rotating manner.Thus, the border of the small bowel is curved or rounded,not angulated or ‘‘fixed’’. The bowel loops should notlook tethered or drawn toward other loops or structures.There should not be any linear strands between the smallbowel loops. Further, given the amount of mesenteric fat,the space between the small bowel loops is generallyconsistent, without asymmetric deposition of fat aroundsome loops and not others. The radiologist must be at-tuned to alterations in the small bowel border to deter-mine if the bowel is ‘‘fixed,’’ angulated, and ‘‘tethered.’’Additionally, as previously stated, in Crohn’s disease,affected segments almost always have other findingsaccompanying the mural findings, such as mural stratifi-cation and/or hyperenhancement.
For patients with ileal pouches, the radiologist shouldremember that without a colon, the distal small bowelproximal to the pouch always dilates. Thus, in thesepatients, a small bowel obstruction should not be diag-nosed unless there is an unequivocal transition point. If apossible small bowel obstruction is suspected in a patientwith an ileal pouch, a contrast enema is often a bettermethod of evaluation.
Imaging acutely ill Crohn’s patients
Anacutely ill patientwithCrohn’s diseasemay have a smallbowel obstruction, an acute exacerbation of the disease,new or unsuspected penetrating disease, and/or an abscessor infectious phlegmon. Studies have shown that CTEsubstantially changes clinical management and improvesphysician confidence level in a largenumberof patientswithCrohn’s disease [69–74]. The postoperative patient (within2–3 weeks), most often presents with signs of infection.
We approach the acutely ill and postoperative Cro-hn’s patient almost always with a CT rather than anMRE or fluoroscopic study as the examination can beperformed almost immediately and rapidly. However, weseparate the acutely ill, non-surgical patients from thepatients in the perioperative period. Patients who are notpost-surgical receive neutral oral contrast media; patientsin the perioperative period receive positive oral andrectal (if there is a colonic anastomosis) contrast media.In the non-surgical patient, we have not found that theuse of neutral oral contrast media limits the ability to
detect an abscess even though abscesses have similarattenuation as neutral contrast-filled bowel [73]. Carefulscrutiny of the images should allow the observer to dis-tinguish the two. However, in post-surgical patients, thepossibility of an anastomotic leak is relatively high. Theuse of neutral contrast media will not detect anastomoticdehiscence. Thus, we use positive oral and/or rectalcontrast media in these patients.
Performing a CTE on a hospitalized patient is partic-ularly challenging. Many of these patients have some levelof a bowel obstruction. These patients may not be able toingest any oral contrast media. However, most alreadyhave bowel filled if not dilated with neutral succusentericus and do not need to ingest any oral agent. Manyof hospitalized patients have nausea, even without a bowelobstruction or are unable to ingest large amounts ofcontrast media. The use of a naso- or orogastric tube orfeeding tube facilitates the process of bowel opacification.In all instances, however, no hospitalized patient shouldbe allowed to ingest the oral agent on the floor. We re-quire that all inpatients come to the department, whereradiology personnel can monitor oral contrast mediaingestion. Clinical information is critical in deciding howmore oral agent should be ingested before scanning.
Imaging Crohn’s patients in theemergency department
Institutions should have a specific Emergency Departmentapproach in dealing with acute ill Crohn’s patients. First,MRE is generally not a practical imaging alternative foremergency department patients. Recent investigations haveshown that CT imaging in the emergency setting is veryefficacious in identifying important complications of Cro-hn’s disease [71, 72, 74]. However, before contemplating aCT, risk stratification should be performed by the orderingphysician. This should be based on history and physicalfindings. In one analysis, a prior history of intestinalobstruction or intraabdominal abscess, current hemato-chezia, and leukocytosis (WBC count >12,000 lL) wereindependent predictors of urgent findings on a subsequentCT (abscess, perforation, obstruction, or new or worseningnon-Crohn’s disease findings) [74]. If the patient presenta-tion warrants immediate imaging, then a CT should beperformed. As previously stated, if the patient is not post-operative, then neutral oral contrast media should beadministered. If the patient is postoperative, then positiveoral contrast media should be administered. Additionally,as in allMDCTE, lowdose techniques should be employed.
Limitations of CTE- when to imagewith MRE and/or dedicated smallbowel series or enteroclysis
There are clinical scenarios where CTE may not or is notan appropriate examination. First, there is no evidence
948 M. E. Baker et al.: CT enterography for Crohn’s disease

that a CTE will adequately evaluate patients who haverecurrent small bowel obstructions, presumably due toadhesive disease. In these patients, an enteroclysis likelywith CT rather than fluoroscopic remains the best testavailable [75]. Second, as previously stated, patients withCrohn’s disease, who are not postoperative and notthought to have an abscess, and in whom a previous CTEhas been performed, are best followed with an MRE
rather than a CTE. The liberal use of MRE shouldreduce the cumulative dose from CT that they mayreceive. Lastly, there are some patients who cannotreceive either intravenous iodinated contrast media orgadolinium due to chronic kidney disease. In these cases,an unenhanced MRE or a dedicated fluoroscopic smallbowel series are the best alternatives. While to ourknowledge there are no data, an unenhanced MRE,relying on the heavily weighted T2 sequences and diffu-sion weighted imaging should detect active inflammatorydisease and penetrating disease. A reasonable alternativeis a barium-based, fluoroscopic examination. However,only a radiologist trained in the fluoroscopic techniquesof rotation and palpation should perform this examina-tion. Unfortunately, these skills are not taught in resi-dency programs, due to the lack of patients (onedownside of the proliferation of CT and MR enterog-raphy). Some highly specialized centers use ultrasound,especially in pediatric and thin adult patients. In isolatedcenters, an enteroclysis is considered a better examina-tion. However, unless conscious sedation is used, thepatient generally willrefuse to tolerate more than one of these examinations.Further, conscious sedation requires nursing supportfor administration and monitoring, increasing the costsof care.
Reporting CTE
As health care is evolving, radiologists must recognizethat proper reporting and nomenclature will play anincreasing role in measuring outcomes. Imaging in Cro-hn’s disease is increasingly used to determine therapy andmeasure its affect (e.g., Lemann score) [76–78]. Endos-copy is limited in that it is invasive, cannot assess theentire bowel, or the extraluminal structures. CTE andMRE are increasingly used to determine the therapy,both medical and surgical as well as follow therapy. Byreporting appropriately and consistently, radiologistswill demonstrate ‘‘meaningful use,’’ a process nowmandated by the federal government.
Many if not most departments now have voice rec-ognition dictation systems. The user can modify thesesystems to contain report templates. These templates canbe modified to prompt the user to include importantinformation both for billing and communication.
From the perspective of the ordering physician, it isimportant to title the examination as a uniphasic or mul-tiphasic CT enterography. Without this title, the clinicianmay not know that an enterography was performed.Adjacent to this title, one can for billing purposes state thatthe examination is an abdomen and pelvis CT with intra-venous contrast enhancement. This alerts the referringphysician that an enterography was performed.
Next, information related to quality and safety,sometimes mandated by CMS and/or state regulations,
Table 2. CTE report template (preliminary Society of AbdominalRadiology consensus statement on nomenclature and reporting ofCTE/MRE; a similar reporting template is also discussed by Al-Hawaryet al. [79]
Title: CTE (abdomen and pelvis CT with intravenous contrast)History:Technique: standard, single-phase (multi-phase) CT enterographyContrast:
Oral: type and volume consumedIV: type and volume of iodinated contrast media injected
Other medications: if applicable (i.e., glucagon, Levsin, etc.)Radiation dose: DLP (mGy/cm), CTDIvol (mGy) or SSDE (mGy)Comparison:Result or findings:
Disease locationStomachSmall bowelDuodenum, jejunal, and/or ilealColon
Enhancement patternStratified or homogeneous
Bowel wall thickeningSite, location, and length of disease
StrictureSmall bowel luminal narrowingWithout upstream dilationWith upstream dilation
Penetrating diseaseSinus tractFistulaSimpleComplex
Mesenteric findings (perienteric findings)StrandingFibrofatty proliferationVasa recta distensionFluid collectionNot amenable to drainage (<3 cm; generally, catheter deployment
in a cavity <3 cm difficult or impossible)Amenable to drainage (>3 cm and accessible to intervention)
Extra-intestinal findingsCholelithiasis, nephrolithiasis, PSC, sacroiliitis, perianal disease, andAVN of femoral heads
Abdomen: other findings not otherwise mentionedPelvis: other findings not otherwise mentionedImpressions:
Active inflammatory small bowel Crohn’s diseaseWithout luminal narrowingWith luminal narrowing
Mixed stenotic and active inflammatory small bowel Crohn’s disease(the term fibrostenosis is controversial to some physicians caringfor Crohn’s disease patients; they believe that some degree offibrosis can be effectively treated medically) (this term should onlybe used when both luminal narrowing and upstream bowel dila-tion >3 cm are present)
Penetrating Crohn’s disease (added to either active inflammatory ormixed disease) (almost always only present with mixed stenotic andactive inflammatory small bowel Crohn’s disease)
Quiescent or inactive small bowel Crohn’s diseaseFibrostenotic small bowel Crohn’s disease
M. E. Baker et al.: CT enterography for Crohn’s disease 949

must be reported. In our institutions this includes historyor reason for the examination; technique used; contrastmedia administered and/or ingested (type and volumespecified); amount and type of anti-peristaltic agentadministered; and, in many cases, documenting the‘‘dose’’ received by the patient [dose length product(DLP) and/or CTDIvol]. As with any radiology report,comparison examinations should be mentioned. Theresults or findings then must be documented. Lastly, animpression should synthesize the findings into anunderstandable and clinically relevant fashion.
The Society of Abdominal Radiology Crohn’s Dis-ease Focus Group has made initial attempts to definethe necessary elements of a CTE report and thenomenclature that should be utilized including how tosynthesize the findings into an appropriate impression(Table 2). This is an ongoing, international process thatincludes collaboration with gastrointestinal and colo-rectal societies.
Acknowledgments. We would like to thank the many other members ofthe Crohn’s Disease Focus Group of the Society of Abdominal Radi-ology who contributed thoughts and ideas that are incorporated in thisdocument: Mahmoud Al-Hawary, Suhda Anupindi, David Bruining,Kassa Darge, Jonathan Dillman, David Einstein, Jeff Fidler, MichaelGee, Flavius Gugliemo, Tracy Jaffe, Seong Ho Park, Daniel Podbere-sky, Jordi Rimola, Dushyant Sahani, Jorge Soto, Stuart Taylor, andlast but not least Alec Megibow, whose foresight and leadership helpedpropel small bowel imaging into the 21st Century.
Conflict of interest. Dr. Baker receives support from Siemens Health-care in the form of salary support, software, and hardware to investi-gate radiation dose reduction in CT and has informal consultationswith Bracco. Dr. Fletcher receives support from Siemens Healthcare inthe form of grant support. Dr. Maglinte is a consultant for Cook Inc.Drs. Hara and Platt has no conflicts of interest.
References
1. Raptopoulos V, Davis MA, Davidoff A, et al. (1987) Fat-densityoral contrast agent for abdominal CT. Radiology 164:653–656
2. Thoeni RF, Filson RG (1988) Abdominal and pelvic CT: use ofmetoclopramide to enhance bowel opacification. Radiology169:391–393
3. Raptopoulos V, Schwartz RK, McNicholas MM, et al. (1997)Multiplanar helical CT enterography in patients with Crohn’s dis-ease. AJR 169:1545–1550
4. Rosen MP, Siewart B, Sands DZ, et al. (2003) Value of abdominalCT in emergency department for patients with abdominal pain. EurRadiol 13:418–424
5. Mazzeo S, Caramella D, Battola L, et al. (2001) Crohn disease ofthe small bowel: spiral CT evaluation after oral hyperhydrationwith isotonic solution. J Comput Assist Tomogr 25:612–616
6. Wold PB, Fletcher JG, Johnson CD, Sandborn WJ (2003)Assessment of small bowel Crohn disease: noninvasive peroral CTenterography compared with other imaging methods and endos-copy-feasibility study. Radiology 229:275–281
7. Megibow AJ, Babb JS, Hecht EM, et al. (2006) Evaluation ofbowel distention and bowel wall appearance by using neutral oralcontrast agent for multi-detector row CT. Radiology 238:87–95
8. Hara AK, Leighton JA, Heigh RI, et al. (2006) Crohn disease of thesmall bowel: preliminary comparison among CT enterography,capsule endoscopy, small-bowel follow-through and ileoscopy.Radiology 238:128–134
9. Bodily KD, Fletcher JG, Solem CA, et al. (2006) Crohn disease:mural attenuation and thickness at contrast-enhanced CT enter-
ography- correlation with endoscopic and histologic findings ofinflammation. Radiology 238:505–516
10. Booya F, Fletcher JG, Huprich JE, et al. (2006) Active Crohndisease: CT findings and interobserver agreement for enteric phaseCT enterography. Radiology 241:787–795
11. Paulsen SR, Huprich JE, Fletcher JG, et al. (2006) CT enterogra-phy as a diagnostic tool in evaluating small bowel disorders: reviewof clinical experience in over 700 cases. Radiographics 26:641–662
12. Hara AK, Alam S, Heigh RI, et al. (2008) Using CT enterographyto monitor Crohn’s disease activity: a preliminary study. AJR190:1512–1516
13. Baker ME, Walter J, Obuchowski NA, et al. (2009) Mural atten-uation in normal small bowel and active inflammatory Crohn’sdisease on CT enterography: location, absolute attenuation, rela-tive attenuation and the effect of wall thickness. AJR 192:417–423
14. Hara AK, Walker FB, Silva AC, Leighton JA (2009) Preliminaryestimate of triphasic CT enterography performance in hemody-namically stable patients with suspected gastrointestinal bleeding.AJR 193:1252–1260
15. Huprich JE, Fletcher JG, Fidler J, et al. (2011) Prospective blindedcomparison of wireless capsule endoscopy and multiphase CTenterography in obscure gastrointestinal bleeding. Radiology2011(260):744–751
16. Lee SS, Oh TS, Kim HJ, et al. (2011) Obscure gastrointestinalbleeding: diagnostic performance of multidetector CT enterogra-phy. Radiology 259:739–748
17. Huprich JE, Barlow JM, Hansel SL, Alexander JA, Fidler JL(2013) Multiphase CT enterography evaluation of small-bowelvascular lesions. AJR 2013:65–72
18. Wang Z, Chen JG, Liu JL, Qin XG, Huang Y (2013) CT enter-ography in obscure gastrointestinal bleeding: a systematic reviewand meta-analysis. J Med Imaging Rad Oncol 57:263–273
19. Elsayes KM, Al-Hawary MM, Jagdish J, Ganesh HS, Platt JF(2010) CT enterography: principles, trends and interpretation offindings. Radiographics 30:1955–1974
20. Gourtsoyianni S, Zamboni GA, Romero JY, Raptopoulos VD(2009) Routine use of modified CT enterography in patients withacute abdominal pain. Eur J Radiol 69:388–392
21. Panes J, Bouhnik Y, Reinisch W, et al. (2013) Imaging techniquesfor assessment of inflammatory bowel disease: joint ECCO andESGAR evidence-based consensus guidelines. J Crohn’s Colitis7:556–585. doi:10.1016/j.corhns.2013.02.020
22. Bruining DH (2010) CT enterography: is it the current state-of-the-art for small bowel diagnostics? Dig Dis 28:429–432
23. National Council on Radiation Protection and Measurements(2009) Ionizing radiation exposure of the population of the UnitedStates. Report 160. Bethesda, MD: National Council on RadiationProtection and Measurements.
24. Maglinte DDT, Applegate KE, Rajesh A, et al. (2009) Conscioussedation for patients undergoing enteroclysis: comparing the safetyand patient-reported effectiveness of two protocols. Eur J Radiol70:512–516
25. Kuehle CA, Ajaj W, Ladd SC, et al. (2006) Hydro-MRI of thesmall bowel: effect of contrast volume, timing of contrast admin-istration and data acquisition on bowel distension. AJR 187:W375–W385
26. Rollandi GA, Curone PF, Biscaldi E, et al. (1999) Spiral CT of theabdomen after distention of small bowel loops with transparentenema in patients with Crohn’s disease. Abdom Imaging 24:544–549
27. Fletcher JG (2008) CT enterography technique: theme and varia-tions. Abdom Imaging 34:283–288
28. Huprich JE, Fletcher JG (2009) CT enterography: principles,technique and utility in Crohn’s disease. Eur J Radiol 69:393–397
29. Ilangovan R, Burling D, George A, et al. (2012) CT enterography:review of technique and practical tips. Br J Radiol 85:876–886
30. Sood RR, Joubert I, Franklin H, Doyle T, Lomas DJ (2002) Smallbowel MRI: comparison of polyethylene glycol preparation andwater as oral contrast media. J Magn Reson Imaging 15:401–408
31. Arslan H, Etlik O, Kayan M, et al. (2005) Peroral CT enterographywith lactulose solution: preliminary observations. AJR 185:1173–1179
32. Hebert JJ, Taylor AJ, Winter TC, Reichelderfer M, Weichert JP(2006) Low-attenuation oral GI contrast agents in abdominal-pel-vic computed tomography. Abdom Imaging 31:48–53
950 M. E. Baker et al.: CT enterography for Crohn’s disease

33. Young BM, Fletcher JG, Booya F, et al. (2008) Head-to-headcomparison of oral contrast agents for cross-sectional enterogra-phy: small bowel distention, timing, and side-effects. J ComputAssist Tomogr 32:32–38
34. Koo CW, Shah-Patel LR, Baer JW, Frager DH (2008) Cost-effectiveness and patient tolerance of low-attenuation oral contrastmaterial: milk versus VoLumen. AJR 190:1307–1313
35. Minordi LM, Vecchioli A, Mirk P, Bonomo L (2011) CT enter-ography with polyethylene glycol solution vs CT enteroclysis insmall bowel disease. Br J Radiol 84:112–119
36. Schindera ST, Nelson RC, DeLong DM, et al. (2007) Multi-detector row CT of the small bowel: peak enhancement temporalwindow-initial experience. Radiology 243:438–444
37. Vandenbroucke F, Mortele KJ, Tatli S, et al. (2007) Noninvasivemultidetector computed tomography enterography in patients withsmall bowel Crohn’s disease: is a 40-second delay better than 70seconds? Acta Radiol 48(1052–1060):2007
38. Makanyanga J, Punwani S, Taylor SA (2012) Assessment of wallinflammation and fibrosis in Crohn’s disease: value of T1-weighted,gadolinium-enhanced MR imaging. Abdom Imaging 37:933–943
39. Jaffe TA, Am Gaca, Delaney S, et al. (2007) Radiation dose fromsmall-bowel follow-through and abdominopelvic MDCT in Cro-hn’s disease. AJR 189:1015–1022
40. Peloquin JM, Pardi DS, Sandborn WJ, et al. (2008) Diagnosticionizing radiation exposure in a population-based cohort ofpatients with inflammatory bowel disease. Am J Gastroenterol103:2015–2022
41. Desmond AN, O’Regan K, Curran C, et al. (2008) Crohn’s disease:factors associated with exposure to high levels of diagnostic radi-ation. Gut 57:1524–1529
42. Brenner DJ (2008) Should computed tomography be the modalityof choice for imaging Crohn’s disease in children? The radiationrisk perspective. Gut 57:1489–1490
43. Palmer L, Herfarth H, Porter CQ, et al. (2009) Diagnostic ionizingradiation exposure in a population-based sample of children withinflammatory bowel diseases. Am J Gastroenterol 104:2816–2823
44. Kroeker KI, Lam S, Birchall I, Fedorak RN (2011) Patients withIBD are exposed to high levels of ionizing radiation through CTscan diagnostic imaging: a five-year study. J Clin Gastroenterol45:34–39
45. Chatu S, Subramanian V, Pollok RC (2012) Meta-analysis: diag-nostic medical radiation exposure in inflammatory bowel disease.Aliment Pharmacol Ther 35:529–539
46. Pearce MS, Salotti JA, Little MP, et al. (2012) Radiation exposurefrom CT scans in childhood and subsequent risk of leukaemia andbrain tumors: a retrospective cohort study. Lancet 380:499–505
47. Brenner DJ, Hall EJ (2012) Cancer risks from CT scans: now wehave data, what next? Radiology 265:330–331
48. Kambadakone AR, Prakash P, Hahn PF, Sahani DV (2010) Low-dose CT examinations of Crohn’s disease: impact of image quality,diagnostic performance and radiation dose. AJR 195:78–88
49. Allen BC, Baker ME, Einstein DM, et al. (2010) Effect of alteringautomatic exposure control settings and quality reference mAs onradiation dose, image quality, and diagnostic efficacy in MDCTenterographyof active inflammatoryCrohn’s disease.AJR195:89–100
50. Guimaraes LS, Fletcher JG, Yu L, et al. (2010) Feasibility of dosereduction using novel denoising techniques for low kV (80 kV) CTenterography: optimization and validation. Acad Radiol 17:1203–1210
51. Siddiki H, Fletcher JG, Hara AK, et al. (2011) Validation of lowerradiation computed tomography enterography imaging protocol todetect Crohn’s disease in the small bowel. Inflamm Bowel Dis17:778–786
52. Kambadakone AR, Chaudhary NA, Desai GS, et al. (2011) Low-dose MDCT and CT enterography of patients with Crohn disease:feasibility of adaptive statistical iterative reconstruction. AJR196:W743–W752
53. Craig O, O’Neill S, O’Neill F, et al. (2012) Diagnostic accuracy ofcomputed tomography using lower doses of radiation for patientswith Crohn’s disease. Clin Gastroenterol Hepatol 10:886–892
54. Kaza RK, Platt JF, Al-Hawary MM, et al. (2012) CT enterographyat 80 kVp with adaptive statistical iterative reconstruction versus at120 kVp with standard reconstruction: image quality, diagnosticadequacy and dose reduction. AJR 198:1084–1092
55. Gonzalez-Guindalini FD, Botelho MPF, Huseyin GT, et al. (2013)MDCT of chest, abdomen, and pelvis using attenuation- basedautomated tube voltage selection in combination with iterativereconstruction: an intrapatient study of radiation dose and imagequality. AJR 2013(201):1075–1082
56. Hough DM, Fletcher JG, Grant KL, et al. (2012) Lowering kilo-voltage to reduce radiation dose in contrast-enhanced abdominalCT: initial assessment of a prototype automated kilovoltage selec-tion tool. AJR 199:1070–1077
57. Kanal KM, Chung JH, Wang J, et al. (2011) Image noise and liverlesion detection with MDCT: a phantom study. AJR 197:437–441
58. Hernandez-Giron I, Geleijns J, Calzado A, Veldkamp WJH (2011)Automated assessment of low contrast sensitivity for CT systemsusing a model observer. Med Phys 38(S1):S25
59. Baker ME, Dong F, Primak A, et al. (2012) Contrast-to-noise ratioand low-contrast object resolution on full-and low-dose MDCT:SAFIRE versus filtered back projection in a low-contrast objectphantom and in the liver. AJR 199:8–18
60. Pickhardt PJ, Lubner MG, Kim DH, et al. (2012) Abdominal CTwith model-based iterative reconstruction (MBIR): initial results ofa prospective trial comparing ultralow-dose with standard-doseimaging. AJR 199:1266–1274
61. Von Falck C, Bratanova V, Rodt T, et al. (2013) Influence ofsonogram affirmed iterative reconstruction of CT data on imagenoise characteristics and low-contrast detectability: an objective ap-proach. PLos One 8(2):e56875. doi:10.1371/journal.pone.0056875
62. Schindera ST, Odedra D, Raza SA, et al. (2013) Iterative recon-struction algorithm for CT: can radiation dose be decreased whilelow contrast detectability is preserved? Radiology 269:511–518
63. Schindera ST, Odedra D, Mercer D, et al. (2014) Hybrid iterativereconstruction technique for abdominal CT protocols in obesepatients: assessment of image quality, radiation dose, and low-contrast detectability in a phantom. AJR 202:W146–W152
64. Husarik DB, Schindera ST, Morsbach F, et al. (2014) Combiningautomated attenuation-based tube voltage selection and iterativereconstruction: a liver phantom study. Eur Radiol 24:657–667
65. Goenka AH, Herts BR, Dong F, Obuchowski NA, et al. (2014)Effect of reduced radiation exposure and iterative reconstructionon detection of low contrast attenuation lesions in an anthropo-morphic liver phantom: an 18-reader study. Radiology 272:154–163
66. Herts B, Baker ME, Obuchowski N, et al. (2013) Dose reductionfor abdominal and pelvic MDCT following a change to a graduatedweight-based protocol for selecting quality reference mAs, kVp andslice collimation. AJR 200:1298–1303
67. Baker, ME, Karim W, Bullen J, Primak A, Dong F, Herts BR(2014) Estimated radiation exposure using automatic tube voltageselection with both fixed and weight-based quality reference mAs,and with a fixed 120 kVp, weight-based quality reference mAs.Presented at the 2014 American Roentgen Ray Society AnnualMeeting, May, 2014, San Diego, CA.
68. Gandhi N, Baker, ME, Goenka AH, et al (2014) Diagnosticaccuracy of sonogram affirmed iterative reconstruction and filteredback projection in CTE at half-dose for active inflammatory ter-minal ileal Crohn’s disease: a multireader study. Presented at the2014 Radiologic Society of North America Scientific Assembly andAnnual Meeting, December, 2014, Chicago, IL
69. Bruining DH, Loftus EV, Ehman EC, et al. (2011) Computedtomography enterography detects intestinal wall changes and ef-fects of treatment in patients with Crohn’s disease. Clin Gastro-enterol Hepatol 9:679–683
70. Bruining DH, Siddiki HA, Fletcher JG, et al. (2012) Benefit ofcomputed tomography enterography in Crohn’s disease: effects onpatient management and physician level of confidence. InflammBowel Dis 18:219–225
71. Kerner C, Carey K, Mills AM, et al. (2012) Use of computedtomography in emergency departments and rates of urgent diag-noses in Crohn’s disease. Clin Gastroenterol Hepatol 10:52–57
72. Isreali E, Ying S, Henderson B, et al. (2013) The impact ofabdominal computed tomography in a tertiary referral centreemergency department on the management of patients withinflammatory bowel disease. Aliment Pharmacol Ther 38:513–521
73. Vogel J, Moreira A, Baker ME, et al. (2007) CT enterography forCrohn’s disease: accurate preoperative imaging. Dis Colon Rectum50:1761–1769
M. E. Baker et al.: CT enterography for Crohn’s disease 951

74. Kerner C, Carey K, Baillie C, et al. (2013) Clinical predictors ofurgent findings on abdominopelvic CT in emergency departmentpatients with Crohn’s disease. Inflamm Bowel Dis 19:1179–1185
75. Kohli MD, Maglinte DDT (2009) CT enteroclysis in incompletesmall bowel obstruction. Abdom Imaging 34:321–327
76. Pariente B, Cosnes J, Danese S, et al. (2011) Development of theCrohn disease digestive damage score, the Lemann score. InflammBowel dis 17:1415–1422
77. Pariente B, Peyrin-Biroulet L, Cohen L, Zagdanski AM, ColombelJF (2011) Gastroenterology review and perspective: the role of
cross-sectional imaging in evaluating bowel damage in Crohn dis-ease. AJR 197:42–49
78. Rimola J, Ordas I, Rodriguez S, Ricart E, Panes J (2012) Imagingindexes of activity and severity for Crohn’s disease: current statusand future trends. Abdom Imaging 37:956–958
79. Al-Hawary MM, Kaza RK, Platt JF (2013) CT enterography:concepts and advances in Crohn’s disease imaging. Radiol Clin NAm 51:1–16
952 M. E. Baker et al.: CT enterography for Crohn’s disease