Embed Size (px)
Citation preview

Cadem
artiri •M
ollet •H
offmann
CT CORONARYANGIOGRAPHY
Filippo Cademartiri • Nico R Mollet • Udo Hoffmann
CLINICAL PUBLISHING
An Atlas of Investigation and Diagnosis
CL
INIC
AL
PU
BL
ISHIN
G
An Atlas of Investigation and Diagnosis
CT CORONARYANGIOGRAPHYThis volume presents the reader with a thorough groundingin the basics of cardiac CT, with particular reference tocoronary artery disease. Primarily a practical guide, itincludes a review of basic techniques, optimization, datahandling and reporting.
This atlas is based firmly in a clinical context,comprehensively illustrated throughout and uses detailedcase studies to demonstrate the role of cardiac CT in a widevariety of clinical settings. An essential reference for thehospital radiology department, and for trainees in radiologyand cardiology.
Related titles:
Angina: an Atlas of Investigation and ManagementIJ SarembockISBN 978 1 904392 59 0
MDCT in Neuroimaging: an Atlas and Practical GuideE Teasdale, S AitkenISBN 978 1 904392 68 2
Problem Solving in CardiologyHS Lim, GYH LipISBN 978 1 84692 046 2
Website: www.clinicalpublishing.co.uk
ISBN: 978 1 84692 010 3
CT
CO
RO
NA
RY
AN
GIO
GR
AP
HY
CTCA COVER final non-Bracco.qxd:cub.QXD 18/11/10 17:16 Page 1

Dedications
I dedicate this book to my special CardioTeam (Dr Erica Maffei and Dr ChiaraMartini) who are the engine of my daily work. I also dedicate the book to all the
fellows who helped us during the years in achieving great results in this field. (FC)
I dedicate this book to Duco and Justus. (NRM)
I dedicate this book to my parents who have paved the way for me to enter thisexciting field of work. (UH)
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page ii

CLINICAL PUBLISHINGOXFORD
An Atlas of Investigation and Diagnosis
CT CORONARYANGIOGRAPHY
Filippo Cademartiri, MD, PhDDepartment of Radiology and Cardiology,
Azienda Ospedaliero-Universitaria di Parma, Italy
Departments of Radiology and Cardiology, Erasmus Medical Centre, Rotterdam, The Netherlands
Nico R Mollet, MD, PhDDepartments of Radiology and Cardiology,
Erasmus Medical Centre, Rotterdam, The Netherlands
Udo Hoffmann, MDDepartment of Radiology, Harvard-MGH, Boston, USA
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page iii

Clinical Publishingan imprint of Atlas Medical Publishing LtdOxford Centre for InnovationMill Street, Oxford OX2 0JX, UK
Tel: +44 1865 811116Fax: +44 1865 251550Email: [email protected]: www.clinicalpublishing.co.uk
Distributed in USA and Canada by:Clinical Publishing30 Amberwood ParkwayAshland, OH 44805, USA
Tel: 800-247-6553 (toll free within US and Canada)Fax: 419-281-6883Email: [email protected]
Distributed in UK and Rest of World by:Marston Book Services LtdPO Box 269AbingdonOxon OX14 4YN, UK
Tel: +44 1235 465500Fax: +44 1235 465555Email: [email protected]
© Atlas Medical Publishing Ltd 2011
First published 2011
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted,in any form or by any means, without the prior permission in writing of Clinical Publishing or Atlas MedicalPublishing Ltd.
Although every effort has been made to ensure that all owners of copyright material have been acknowledgedin this publication, we would be glad to acknowledge in subsequent reprints or editions any omissions broughtto our attention.
Clinical Publishing and Atlas Medical Publishing Ltd bear no responsibility for the persistence or accuracy ofURLs for external or third-party internet websites referred to in this publication, and do not guarantee that anycontent on such websites is, or will remain, accurate or appropriate.
A catalogue record of this book is available from the British Library
ISBN 978 1 84692 010 3e-ISBN 978 1 84692 626 6
The publisher makes no representation, express or implied, that the dosages in this book are correct.Readers must therefore always check the product information and clinical procedures with the mostup-to-date published product information and data sheets provided by the manufacturers and the mostrecent codes of conduct and safety regulations. The authors and the publisher do not accept anyliability for any errors in the text or for the misuse or misapplication of material in this work.
Printed by Henry Ling, Dorchester Press, Dorset, UK
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page iv

Contents
Editors and contributors vi
Abbreviations viii
Part 1: Introduction to Cardiac CT 11 Introduction 12 Fundamentals of CT 53 Basics of cardiac CT 104 Contrast material administration 175 How to optimize cardiac CT images 236 How to interrogate cardiac CT datasets 277 How to report cardiac CT angiography 32
Part 2: Spectrum of Diseases 378 Coronary anomalies 379 Coronary calcium and atherosclerotic plaques: prognostic value 46
10 Coronary stenosis 5011 Coronary stent imaging 5512 Coronary artery bypass grafts 6013 Collateral findings 64
Part 3: Clinical Applications of Cardiac CT – Case Studies 7214 Overview of clinical applications 7215 Case studies: primary prevention 7816 Case studies: atypical chest pain 9017 Case studies: stable angina pectoris 10218 Case studies: acute coronary syndrome 11319 Case studies: secondary prevention 12420 Case studies: triple rule-out and other collateral findings 13521 Clinical indications of CT coronary angiography 13922 New horizons in cardiac CT technology 146
Index 149
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page v

vi
Editors and contributors
Editors
Filippo Cademartiri, MD, PhDDepartment of Radiology and Cardiology, Azienda Ospedaliero-Universitaria di Parma, Italy
Departments of Radiology and Cardiology, Erasmus Medical Centre, Rotterdam, The Netherlands
Nico R Mollet, MD, PhDDepartments of Radiology and Cardiology, Erasmus Medical Centre, Rotterdam, The Netherlands
Udo Hoffmann, MDDepartment of Radiology, Harvard-MGH, Boston, USA
Contributors
Ricardo J Benenstein, MDDepartment of Radiology, Harvard-MGH, Boston, USA
Andrew R Blum, MDDepartment of Radiology, Harvard-MGH, Boston, USA
Ermanno Capuano, MDDepartment of Radiology and Cardiology, Azienda Ospedaliero-Universitaria di Parma, Italy
Department of Radiology, Erasmus Medical Center,Rotterdam, The Netherlands
Marcel R Dijkshoorn, RTDepartment of Radiology, Erasmus Medical Center,Rotterdam, The Netherlands
Ludovico La Grutta, MDDepartment of Radiology, University of Palermo, Italy
Erica Maffei, MDDepartment of Radiology and Cardiology, Azienda Ospedaliero-Universitaria di Parma, Italy
Roberto Malagò, MDDepartment of Radiology, University Of Verona, Italy
Chiara Martini, RTDepartment of Radiology and Cardiology, Azienda Ospedaliero-Universitaria di Parma, Italy
Department of Radiology, Erasmus Medical Center,Rotterdam, The Netherlands
W Bob Meijboom, MD, PhDDepartments of Radiology and Cardiology, Erasmus Medical Center, Rotterdam, The Netherlands
Lisan Neefjes-Vermunt, MDDepartments of Radiology and Cardiology, Erasmus Medical Center, Rotterdam, The Netherlands
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page vi

Alessandro Palumbo, MDDepartment of Radiology and Cardiology, Azienda Ospedaliero-Universitaria di Parma, Italy
Department of Radiology, Erasmus Medical Center,Rotterdam, The Netherlands
Roberto Pozzi Mucelli, MDDepartment of Radiology, University Of Verona, Italy
Francesca Pugliese, MD, PhDCentre for Advanced Cardiovascular Imaging,Barts and The London NIHR Biomedical Research Unit,Queen Mary University of London, The London ChestHospital, London
Marco Rengo, MDDepartment of Radiology and Cardiology, Azienda Ospedaliero-Universitaria di Parma, Italy
Departments of Radiology and Cardiology, Erasmus Medical Center, Rotterdam, The Netherlands
Alexia Rossi, MDDepartments of Radiology and Cardiology, Erasmus Medical Center, Rotterdam, The Netherlands
Annick C Weustink, MDDepartments of Radiology and Cardiology, Erasmus Medical Center, Rotterdam, The Netherlands
Editors and contributors vii
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page vii

Abbreviations
viii
3VD 3-vessel diseaseACS acute coronary syndromeAHA American Heart AssociationAo aortaAV atrioventricularBMS bare-metal stentCABG coronary artery bypass graftCAD coronary artery diseaseCAG coronary angiographyCCA conventional coronary angiographyCHD coronary heart diseaseCM contrast materialCNR contrast to noise ratioCOPD chronic obstructive pulmonary diseaseCT computed tomographyCTCA computed tomography coronary angiographyCX circumflex arteryD1 1st diagonal branchD2 2nd diagonal branchDES drug-eluting stentDSCT dual source computed tomographyEBCT electron beam computed tomographyECG electrocardiogramEDV end-diastolic volumeEF ejection fractionESW effective slice widthFFR fractional flow reserveFOV field of viewFU follow-upHOCM hypertrophic obstructive cardiomyopathyHR heart rateIDR iodine delivery rateISR in-stent restenosisLAD left anterior descending
LCA left coronary arteryLIMA left internal mammary arteryLM left main (artery)LV left ventricular/left ventricleLVOT left ventricular outflow tractMDCT multidetector computed tomographyMIP maximum intensity projectionMO marginal obtuse branchMPR multiplanar reconstructionMRI magnetic resonance imagingMRA magnetic resonance angiographyMSCT-CA multislice computed tomography coronary
angiographyPA pulmonary arteryPACS picture archiving and communication systemPCI percutaneous coronary interventionPDA posterior descending coronary arteryPME peak of maximum enhancementPV pulmonary veinQCA quantitative coronary angiographyRCA right coronary arteryRF risk factorRI reconstruction incrementRV right ventricleSA stable anginaSAS step-and-shootSDCT single detector computed tomographySPECT single photon emission computed tomographySSP slice sensitivity profileSVC superior vena cavaSVG saphenous vein grafttPME time to peak of maximum enhancementVRT volume rendering technique
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page viii

Part 1
Background
Cardiac computed tomography (cardiac CT) has developedin the past 10 years from an investigational tool to clinicalreality. At first it seemed to be one of the ‘pretending’imaging modalities for the noninvasive assessment of thecoronary arteries (with magnetic resonance imaging [MRI]and electron beam CT [EBCT]). Then, in a few years,several generations of scanners provided a dramaticimprovement in image quality and robustness. Operatorsbecame more skilled and more experienced in managing theissues (e.g. heart rate control, X-ray dose, and so on).
The rapid development and the never ceasing validationprocess did not allow a real clinical assessment withendpoints such as prognosis, better care, and cost-effectiveness. Recently, this information has started toappear in the literature, and the excitement around thisimaging modality is growing. However, criticism isincreasing, as many people are worried about the potentialmisuse of cardiac CT for screening. These concerns can beapplied to any other imaging modality characterized by highcosts and a certain biological risk (e.g. stress single photonemission computed tomography [SPECT]).
As has been the case for conventional catheter coronaryangiography, echocardiography, EBCT, SPECT, and MRI,the period in which the international community asks whatis the clinical role and impact of this modality has juststarted. The presence in clinical practice of several othermodalities able to provide similar/complementary/surrogateinformation for the diagnosis of coronary artery disease(CAD) makes the task very difficult. Also the operators areusually very experienced in few or just one of the modalitiesinvolved.
Any diagnostic modality at its best can be used to provideproper and useful clinical information. The main question,therefore, should be, ‘Which one plays the major role in thefirst line or in the ruling out of CAD?’ In our view, cardiacCT is definitely the best candidate for this task. The amountof information that cardiac CT can provide nowadays isextremely large and increasing each year with new scannergenerations and new software applications. The availabilityof CT technology with cardiac features is also increasing at avery fast pace. For these and many other reasons, cardiac CTcould become the modality of choice for suspected CAD.
1
INTRODUCTION TOCARDIAC CT
Chapter 1
IntroductionFilippo Cademartiri, MD, PhD, Nico R Mollet, MD, PhD,and Udo Hoffmann, MD
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 1

Introduction2
The change of paradigm
The main paradigm of diagnostic cardiology is that inpatients with suspected CAD, we have to demonstrate thepresence of ischaemia/inducible ischaemia. This paradigm issupported by decades of studies with several differentimaging modalities. However, we know that there are twomain entities in atherosclerotic coronary disease: stableangina/chronic chest pain (SA) and acute coronarysyndrome (ACS). The underlying disease is the same, butthe clinical manifestation, therapeutic options, andprognosis are quite different (1.1). Stable CAD withsignificantly obstructive stenosis can be managed medicallyor interventionally/surgically based on clinical conditions,symptoms, location, and extension of disease. The spectrumof the management is constantly developing depending onnew drugs and new devices. For ACS, we can only rely forprediction on rule-based traditional risk factor stratificationand/or modalities able to show the presence of inducibleischaemia, an already advanced stage of atherosclerosis.
Extensive studies and trials on calcium score havedemonstrated that the absolute and weighted (i.e. adjustedfor age and gender) burden of calcium within the coronaryarteries provides incremental information over thetraditional strategies for risk stratification (i.e. Framinghamrisk score). Calculating a population risk based on risk
factors is one thing, but it is another to demonstrate thepresence of atherosclerosis. This is a step towards theindividualization of risk stratification. Providing informationon the noncalcific plaque burden may play a further role inthis individualization. As an example, treating a patient withthree risk factors and no evidence of CAD with intensive‘statins’ makes less sense than treating a patient with onerisk factor and demonstrated atherosclerosis of the coronaryarteries.
The presence, degree, and location of stenosis areimportant predictors of events and survival. However, theimpact of stress techniques (i.e. stress electrocardiogram[ECG], stress echocardiography, stress SPECT) can belimited by several factors. In these cases and especially whenthe pretest likelihood of disease remains intermediate, apowerful tool to exclude CAD is mandatory. On the otherhand, the implementation of a tool able to rule out thepresence of significant stenosis early in the diagnosticalgorithm may definitely reduce time and cost.
Pivotal position of cardiac CT
Cardiac CT can play the pivotal role in cardiovascularimaging (1.2). The flexibility, availability, and robustness ofthe modality allows a comprehensive assessment that can bechallenged only by the reference standards (i.e. invasiveangiography). This concept applies to coronary arteries andto all other vascular regions of the human body.
For coronary artery disease it is expected that CT willbecome the primary tool for risk stratification and diagnosisof obstructive CAD (1.2). Previously, as described above,the key issue was ischaemia. This will remain true, sinceischaemia is the most important determinant for thedecision to revascularize. However, the diagnostic potentialof CT is broader than ischaemia (and actually CT does notshow ischaemia, yet). CT can show atherosclerosis in termsof presence, location, extent, type, and ultimately degree ofobstruction. This unique clinical information is still underinvestigation but it is likely to become a very important partof risk stratification and pharmacological strategy decisionmaking.
In the near future CT will become the reference standardfor the assessment of patients with suspicion of CAD in anyclinical condition (e.g. stable, unstable, acute). The onlylimitation is likely to remain at the level of operators’ skilland operator numbers. It is not easy to train an operator for
1.1 The burden of coronary artery disease in the generalpopulation is very large and it develops in most cases inrelation to cardiovascular risk factors. Stableangina/chronic chest pain (SA) and acute coronarysyndrome (ACS) are two different clinical entities with thesame underlying chronic disease. Sometimes theyoverlap; however, most of the time they have a differentclinical presentation and different clinical history.
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 2

Introduction 3
Patients with suspected CAD
Functional test (e.g. stress ECG)
Normal/negative PositiveDoubt/inconclusive/unfeasible
Functional imaging
Discharge
No ischaemia Ischaemia
Medical therapy and aggressive risk factors
modification
Location
CAG + PCI/CABG if needed
Patients with suspected CAD
Functional imaging (e.g. stress SPECT)
Normal/negative PositiveDoubt/inconclusive/unfeasible
Discharge
Functional imaging (e.g. stress ECG/MRI)
Ischaemia
Medical therapy and aggressive RF
modification
CAG + PCI/CABG if needed
No ischaemia Doubt/inconclusive/unfeasible
No obstructive CAD
No CAD
A
B
1.2 Simplified current algorithms for CAD detection (A, B). The entire flow is based on the demonstration ofischaemia. CT introduces a totally new concept (C, overleaf). With a high sensitivity and negative predictivevalue, it enables exclusion and inclusion of patients and the beginning of the algorithm. Then, functional tests willbe used for better delineation of the functional importance of CAD detected by CT. CABG, coronary artery bypassgraft; CAD, coronary artery disease; CAG, coronary angiography; ECG, electrocardiogram; MRI, magneticresonance imaging; PCI, percutaneous coronary intervention; RF, risk factors.
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 3

Introduction4
proper cardiovascular imaging with CT, and it may takemore than 1 year. However, this level of training is the onlyone that can guarantee the expected performance in dailyroutine.
New CT technologies allow robust imaging in difficult
conditions (e.g. high heart rate) with low X-ray exposure(1–4 mSv). A new paradigm should be applied because ofthese improvements. If radiation is a manageable problem,the issues are when cardiac CT is useful and whether itchanges the diagnosis/treatment/prognosis of our patients.
Patients with suspected CAD
Pretest likelihood of CAD
Intermediate
Noninvasive anatomical imaging – CTCA
Borderline 50%atherosclerosis
Severe/obstructiveCAD (LM, 3VD)
Nonobstructive CAD
NormalNo CAD
Functional imaging
No ischaemia Ischaemia
CAG + PCI/CABGMedical therapy and aggressive RF modification
Discharge/RFmodification
HighLow
C
1.2 (Continued) 3VD, three-vessel disease; CABG, coronary artery bypass graft; CAD, coronary artery disease; CAG,coronary angiography; CTCA, computed tomography coronary angiography; LM, left main; PCI, percutaneous coronaryintervention; RF, risk factors.
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 4

Fundamentals of CTErica Maffei, MD, Alessandro Palumbo, MD, Chiara Martini, RT,Marcel R Dijkshoorn, RT, Annick C Weustink, MD,Nico R Mollet, MD, PhD, and Filippo Cademartiri, MD, PhD
Chapter 2
Introduction
Computed tomography (CT) technology has improvedtremendously in the last 10 years, evolving from singledetector to 64-slice multidetector CT (MDCT) and beyond.Sixty-four-slice MDCT allows new applications such asnoninvasive coronary artery imaging and brain perfusionimaging. Although basics are shared between single detectorCT (SDCT) and MDCT, concepts of spiral imaging arebeing applied in an increasingly sophisticated way. Inaddition, the scanning approach differs between differentgenerations of MDCT technologies. As a consequence,being aware of scan principles is mandatory to understandimage features and to optimize examination protocol.
The aim of this chapter is to describe fundamentals ofspiral MDCT and to provide the keys for optimizing scanningparameters in order to obtain adequate postprocessing.
Image reconstruction
Image reconstruction generates cross-sections of a volumefrom multiple views. This is the core concept of CT andimplementations have been developed accordingly.
As digital pictures are formed by two-dimensional digitalelements (pixels), a volume can be represented by three-dimensional digital elements (voxels) (2.1). In CT, theattenuation values of the voxels that form the slice areassigned to the pixels that form the cross-sectional image,which may be thought of as the ‘surface’ of the slice. Imagereconstruction supplies the values of the voxels that form theslice from the multiple projections that are obtained fromdifferent angles by rotating the X-ray tube-detector systemof the gantry around the volume (2.2). The moreprojections are obtained, the better defined is the resultingimage.
5
2.1 Contrast-enhanced CT of the mediastinum in a patientwith aortic dissection. The magnification of a region ofinterest shows the elements that form the picture (pixels)as small squares.
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 5

Fundamentals of CT6
There are two methods of performing imagereconstruction from these views. The first method isiterative reconstruction, in which subsequent projections areused to correct the values of the voxels composing the slice1.This method is accurate but computationally expensive andis no longer used.
The second method is backprojection, in which the overallX-ray attenuation of a projection is assigned to each voxelalong the ray1. The value of each voxel is then obtained fromthe sum of every value of the projection along the rayscoming through this voxel. Put simply, it is like ‘flattening’on a surface the value of every projection along its direction(2.3). A drawback is that this is a summation operation onlyand the image is blurred. To overcome this, a convolutionkernel can be applied before backprojection (2.3). Aconvolution kernel is a filter that modifies the value of a voxelaccording to the values of the surrounding voxels. Thisapproximated method is called filtered backprojection1.
Scanning parameters
Image quality, scanner performance, and the effect ofscanning parameters can be assessed by considering thefollowing elements:
2.2 Simplified representation of a CT scanner. The gantryincludes the X-ray tube and the detector arrays, whichrotate around the table. The X-ray beam is collimated tohit the detector array. Parallel projections are obtainedthrough the rotation of the X-ray tube–detector system.
Image noise, which depends on the statistical fluctuation ofthe signal during sampling and on interpolation in CTimage reconstruction2, 3. Image noise is inversely propor -tional to the number of detected photons, tube current, anddetector collimation4.
Slice sensitivity profile (SSP), which represents thecontribution of each position along the z-axis (i.e.longitudinal axis, perpendicular to the scan plane) withinthe slice to the signal5. The SSP broadens proportionally totable feed and depends on the interpolation algorithm3.Image noise and SSP determine spatial and contrastresolution6, 7.
2.3 In this example, a hyper-attenuating cylinder isscanned in the transverse plane. With backprojection, thevalue of each voxel of the slice is obtained from thevalues of the projections passing through it. However, thisis an additive operation and the margins of the cylinderare blurred. With filtered backprojection, a convolutionkernel is applied to the signal before backprojection. Aconvolution kernel acts as a filter, which modifies thevalue of a point according to the surrounding points andthe features of the function that is used. In this case theconvolution kernel is set to enhance the differencesbetween the values of each voxel by modifying the shapeof the signal at its margins. Filtered backprojectionovercomes image blurring, although with strong kernels,image noise is also increased.
Backprojection Filtered backprojection
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 6

Fundamentals of CT 7
Spatial resolution represents the minimum distance at whichtwo signals can be discriminated as separate. Generally,spatial resolution in the z-axis is much inferior to resolutionon the scan plane and depends on object position relative tothe scanner isocentre8.
Contrast resolution can be described by the contrast to noiseratio (CNR), and represents the capability to discern twodensities with a given background noise.
Temporal resolution is the shortest interval at which twosignals can be discriminated as separate.
Aliasing is a signal-dependent process due to an insufficientsampling frequency with respect to the frequency of thesampled signal. The Nyquist criterion states that a signalmust be sampled at a rate greater than twice that of itshighest frequency component in order to avoid aliasing. Inother words, an insufficient sampling frequency allows morethan a single representation of a signal. Aliasing is also afunction of the objects being imaged, their relationships,and the distance from the scanner isocentre8, 9. Aliasing maymanifest with stair-step artefacts or as spurious information,which can be treated as additive noise8–10.
Interpolation geometry in CT reconstruction associated withhigh-contrast interfaces, which are oriented in an obliqueplane, generate rotational artefacts and objectdeformation9–13. These artefacts are particularly evidentwith higher pitch (2.4).
Patient dose will not be explored in this chapter. The dosedepends on scanning parameters, but also on the patient’scharacteristics and the examination type, and relates to theinformation required (e.g. screening, diagnosis, follow-up).
Among parameters that can be set by the operator,collimation, table feed, and reconstruction increment areparticularly important.
Collimation
Collimation is the width of the X-ray beam at the scannerisocentre that hits the array of detectors. In SDCT thedetector row collimation equals the X-ray beam collimation.In MDCT the detector width is a fraction of the total X-raycollimation14. In MDCT, the slice thickness depends on thenumber of detectors that are used. The detector geometrydetermines how detectors are combined to form the slice.
Table feed – pitch
Table feed is the speed of translation of the patient into thescanner. The pitch is defined as a ratio of the table feed persingle gantry rotation to collimation, which in MDCTcorresponds to the total active detector width12, 14, 15. Thepitch reflects the width of the helix and the distance of theprojections (2.5). Low pitch improves SSP, thus increasingspatial and contrast resolution and sampling frequencyalong the z-axis and vice versa2, 3, 6, 9, 16–21. High pitchentails object distortion along the z-axis, aliasing, and arotation artefact8, 11, 13, 14. High pitch also reduces imagequality in MDCT, although the SSP is more complex inMDCT than in SDCT18. In MDCT a ‘preferred pitch’ canbe set in order to avoid artefacts and redundancy of data14.In 16-row MDCT, pitch is negligible in routine applicationswith the exception of cardiac imaging, in which dataoversampling (e.g. very low pitch) is needed for cardiac-gated reconstruction.
2.4 Aliasing. Three-dimensional reconstruction withvolume rendering algorithm of a table-tennis ball. A stair-step artefact is visible on the left image (A) where thesurface of the object is obliquely oriented with respect tothe scan plane. This artefact occurs because of theinterpolation geometry. The right image (B) has beenobtained from a scan with higher pitch, keeping constantall other parameters. The helical appearance of the stair-step artefacts increases with helical pitch.
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 7

Fundamentals of CT8
Reconstruction increment
The reconstruction increment (RI) is the distance betweenreconstructed images. The RI affects spatial and contrastresolution along the z-axis. Consider an object that isimaged with a collimation width that is equal to the object’slength in the z-axis. In the best case the object is centred tothe reconstructed slice; in the worst case the object isbetween two adjacent slices.
Effective slice width
In MDCT, images can be reconstructed with a thicknessthat differs from the thickness of the detector. Basically,thicker slices are obtained by combining several slices (2.6).This effective slice width (ESW) can be thicker than thedetector width but can never be thinner. ESW is useful forcontrolling image noise and artefacts14. Given an ESW,thinner collimations provide higher image quality butenhance artefacts9.
2.5 Representation of the helical pitch. The higher thetable feed, the wider the helix. The pitch is defined as theratio between the table feed and the collimation, which inmultidetector scanners is the sum of the detectors’ width.
Convolution kernel
A convolution kernel is a filter that modifies the value of avoxel according to the values of the surrounding voxels.Convolution kernels are applied before backprojection ofraw data for image reconstruction. Alternatively, filters canbe applied to two-dimensional images22. Sharp kernels andfilters are used to enhance the edges of high-contraststructures (lung parenchyma or bone). Yet, in this instance,image noise is increased. Smooth kernels or filters enhanceCNR, reducing image noise.
2.6 Effective slice width. The data from severaldetectors along the longitudinal axis can be combinedto obtain images that include information from slices ofdifferent thickness.
Pitch 0.5 1 1.5 2
d d d d
c c c c
Effectiveslices
a
b
c
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 8

Fundamentals of CT 9
References
1. Brooks RA, Di Chiro G. (1975) Theory of imagereconstruction in computed tomography. Radiology117:561–572.
2. Kalender WA, Polacin A. (1991) Physical performancecharacteristics of spiral CT scanning. Med Phys18:910–915.
3. Polacin A, Kalender WA, Marchal G. (1992) Evaluationof section sensitivity profiles and image noise in spiralCT. Radiology 185:29–35.
4. Wang G, Vannier MW. (1996) Maximum volumecoverage in spiral computed tomography scanning. AcadRadiol 3:423–428.
5. Kalender WA. (1994) Technical foundations of spiralCT. Semin Ultrasound CT MR 15:81–89.
6. Kalender WA, Polacin A, Suss C. (1994) A comparisonof conventional and spiral CT: an experimental study onthe detection of spherical lesions. J Comput Assist Tomogr18:167–176.
7. Brink JA, Heiken JP, Balfe DM, et al. (1992) Spiral CT:decreased spatial resolution in vivo due to broadening ofsection-sensitivity profile. Radiology 185:469–474.
8. Yen SY, Rubin GD, Napel S. (1999) Spatially varyinglongitudinal aliasing and resolution in spiral computedtomography. Med Phys 26:2617–2625.
9. Fleischmann D, Rubin GD, Paik DS, et al. (2000) Stair-step artifacts with single versus multiple detector-rowhelical CT. Radiology 216:185–196.
10. Hopper KD, Pierantozzi D, Potok PS, et al. (1996) Thequality of 3D reconstructions from 1.0 and 1.5 pitchhelical and conventional CT. J Comput Assist Tomogr20:841–847.
11. Wang G, Vannier MW. (1994) Stair-step artifacts inthree-dimensional helical CT: an experimental study.Radiology 191:79–83.
12. Brink JA. (1995) Technical aspects of helical (spiral)CT. Radiol Clin North Am 33:825–841.
13. Wilting JE, Timmer J. (1999) Artefacts in spiral-CTimages and their relation to pitch and subjectmorphology. Eur Radiol 9:316–322.
14. Hu H. (1999) Multi-slice helical CT: scan andreconstruction. Med Phys 26:5–18.
15. McCollough CH, Zink FE. (1999) Performanceevaluation of a multi-slice CT system. Med Phys26:2223–2230.
16. Wang G, Vannier MW. (1994) Longitudinal resolutionin volumetric x-ray computerized tomography – analyticalcomparison between conventional and helicalcomputerized tomography. Med Phys 21:429–433.
17. Wang G, Vannier MW. (1994) Spatial variation ofsection sensitivity profile in spiral computed tomography.Med Phys 21:1491–1497.
18. Wang G, Vannier MW. (1999) The effect of pitch inmultislice spiral/helical CT. Med Phys 26:2648–2653.
19. Hu H, Fox SH. (1996) The effect of helical pitch andbeam collimation on the lesion contrast and slice profilein helical CT imaging. Med Phys 23:1943–1954.
20. Kalender WA, Seissler W, Klotz E, et al. (1990) Spiralvolumetric CT with single-breath-hold technique,continuous transport, and continuous scanner rotation.Radiology 176:181–183.
21. Verdun FR, Meuli RA, Bochud FO, et al. (1996) Imagequality and dose in spiral computed tomography. EurRadiol 6:485–488.
22. Wildberger JM, Mahnken AM, Flohr T, et al. (2003)Spatial domain image filtering in computed tomography:feasibility study in pulmonary embolism. Eur Radiol13:717–723.
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 9

Chapter 310
Basics of cardiac CTErica Maffei, MD, Alessandro Palumbo, MD, Chiara Martini, RT, Marcel R Dijkshoorn, RT, Ermanno Capuano, MD, Annick C Weustink, MD,Nico R Mollet, MD, PhD, and Filippo Cademartiri, MD, PhD
Basic cardiac technique
The most important components of a CT system are the X-ray tube and the system of detectors (3.1). The combinationof a fast rotation time and multislice acquisition isparticularly important for cardiac applications1–3. The latestgeneration of 64-MDCT scanners meets theserequirements. They are able to acquire 64 sub-millimetreslices per rotation and routinely achieve excellent imagequality and the visualization of small-diameter vessels of thecoronary circulation, combining isotropic spatial resolution
Introduction
For several years now multidetector computed tomography(MDCT) scanners have been available which enable thesimultaneous acquisition of 64 slices per rotation. Theadditional improvement in spatial and temporal resolutionof these new devices has already provided excellent results inthe field of cardiac imaging. In the future the optimizationof protocols will enable MDCT coronary angiography toreach levels of diagnostic accuracy similar to those ofinvasive techniques.
3.1 Geometry of a CT scanner. A CT scanner is designed with an X-ray tube and a detector that rotate around the table(A). During the rotation the table moves in order to generate the volume dataset (B).
A B
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 10

Basics of cardiac CT 11
(0.4 mm3) with gantry rotation times of 330 ms. They alsoredefine the MDCT methodology of analysing coronaryplaque and evaluating stent lumens.
The technical characteristics of each scanner varyaccording to the model, and development is ongoing andrapid. The precise temporal resolution of the imagesobtained by MDCT scanners depends on many factors:gantry rotation speed, size and position of the field of viewin the scan volume, and the image reconstruction andpostprocessing algorithms. In reality, the data acquired athalf a rotation of the gantry are enough to reconstruct asingle tomographic image with retrospective or prospectiveelectrocardiogram (ECG) control (3.2, 3.3). The temporalresolution of the latest MDCT scanners thereforeapproximate 165 ms4–6. This can be enough to obtain
images of the heart during the diastolic phase (when cardiacmotion is at a minimum) free of obvious motion artefacts ifthe heart rate (HR) is <70 beats per minute.
3.2 Retrospective ECG gating vs. prospective ECGtriggering. The two main techniques for cardiac CT ECGsynchronization are displayed. Upper panel: retrospectiveECG gating, based on spiral continuous X-ray delivery atlow pitch while recording the ECG track. Afterwards theoperator is able to decide arbitrarily which phase of thecardiac cycle is worth reconstructing. Lower panel:prospective ECG triggering, based on sequential scanning(also called ‘step and shoot’ mode). Radiation is deliveredonly within the phase of the cardiac cycle that has beendecided prior to the initiation of the scan. It requires verylow heart rate and/or very high temporal resolution toguarantee adequate image quality.
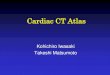
3.3 Baseline ECG in MDCT coronary angiography. Thecardiac cycle is composed of a systole and a diastole.Systole involves contraction of the atria, followed bycontraction of the ventricles. The synchronized contractionis guided by a conducting system which arises from thesinoatrial node in the right atrium. The impulse thenpropagates to the atrio-ventricular node via the walls ofthe atria. From the atrio-ventricular node the impulse istransmitted via the conducting system across the septumand the ventricular walls. This phenomenon is depicted bythe ECG trace, which shows the typical sequence ofwaves (A) P-wave (atrial contraction), QRS complex(ventricular contraction), T-wave (ventricularrepolarization). Normally the P–R interval is <200 ms, the QRS complex is <120 ms, and the Q–T interval is ~420 ms.Therefore, the duration of a complete systoliccontraction with repolarization wave is ~550 ms. Thediastolic period is ~450 ms. This means that for a heartrate of 60 bpm systole and diastole account for 55% and45% of the cardiac cycle, respectively (B). The ~200 mswindow for the ECG retrospectively gated reconstructionobtainable with MDCT coronary angiography is generallyplaced in the diastolic phase (A). The most generallyfavourable position extends from mid- to end-diastole justprior to the P-wave.
50% 50%
ECG
50%
X-ray
ECG
X-ray
Retrospective ECG gating
Prospective ECG gating
R–R interval
A
B
Temporal window
~200 ms
P
R
T
QS
Q–T~420 ms
<200 msP–R
<120 msQRS
R–R1000 ms
~450 msdiastole
~550 mssystole
HR 60 bpm
ECG
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 11

Basics of cardiac CT12
Sensation 64 Definition AS+ Definition DS Definition flashScanTubes 1 1 2 2Slices/rot (detectors) 64 (32) 128 (64) 64 (32) 128 (64)Slice collimation 0.6 mm 0.6 mm 0.6 mm 0.6 mmTube voltage 120 kV 120 kV 120 kV 120 kVTotal tube load (maximum) 180 mA/rot 212 mA/rot 413 mA/rot 528 mA/rotRotation time 330 ms 300 ms 330 ms 285 msEffective temporal resolution 165 ms 150 ms 83 ms 75 msEffective spatial resolution 0.3×0.3×0.4 mm 0.3×0.3×0.4 mm 0.3×0.3×0.4 mm 0.3×0.3×0.4 mmFeed/rotation (standard spiral mode) 3.84 mm 8.45 mm 4.99 mm 8.45 mm
at 60 bpmFeed/second (standard spiral mode) 11.6 mm 28.2 mm 15.1 mm 29.6 mm
at 60 bpmPitch (standard spiral mode) at 60 bpm 0.20 0.22 0.26 0.23Scan time (standard spiral mode, scan 10 s 4 s 8 s 4 s
length 12 cm)Scan time (high-pitch spiral, scan – – – 300 ms
length 12 cm)
X-ray dose*Spiral (full dose) (mSv) 12 6 12 12Spiral (ECG modulation) (mSv) 7 2 5 3Prospective (minimum) (mSv) 2 1.5 4 2High-pitch spiral (mSv) – – – 1
ReconstructionEffective slice width 0.6–0.75 mm 0.6–0.75 mm 0.6–0.75 mm 0.6–0.75 mmReconstruction increment 0.3–0.4 mm 0.3–0.4 mm 0.3–0.4 mm 0.3–0.4 mmTemporal windows (‘hot spots’) End-diastole End-diastole End-diastole End-diastole
End-systole End-systole End-systole End-systoleFOV 140–180 mm 140–180 mm 140–180 mm 140–180 mmConvolution kernel Medium Medium Medium Medium
Contrast materialSynchronization TB/BT TB/BT TB/BT TB/BTROI AAo AAo AAo AAoThreshold in the ROI +100 HU +100 HU +100 HU +100 HUPredelay 10 s 10 s 10 s 10 sCM volume 80–120 ml 80 ml 80 ml 60 mlCM rate 4–6 ml/s 4–6 ml/s 5–6 ml/s 5–6 ml/sIodine concentration 350–400 mgI/ml 350–400 mgI/ml 350–400 mgI/ml 350–400 mgI/mlBolus chaser 40 ml @ 4–6 ml/s 40 ml @ 5–6 ml/s 40 ml @ 4–6 ml/s 40 ml @ 5–6 ml/sVenous access Antecubital Antecubital Antecubital Antecubital
*Radiation dose is calculated at 120 kV (X-ray beam energy)TB, test bolus; BT, bolus tracking; AAo, ascending aorta; FOV, field of view; HU, Hounsfield unit; ECG, electrocardiogram; ROI, region of interest; CM, contrast material; bpm beats per minute
Table 3.1 Scan and reconstruction parameters
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 12

Basics of cardiac CT 13
Scan parameters
The ideal protocol enables high spatial resolution (thincollimation), high temporal resolution (fast gantry rotation)and low radiation dose (prospective modulation of the tubecurrent synchronized to the ECG11) compatible with a goodsignal-to-noise ratio. The main scan parameters for 64-sliceCT of the heart are presented in Table 3.1.
Retrospective gating
The acquisition of image data in the MDCT coronaryangiography scan is continuous during the cardiac cycle,such that the data corresponding to the phase when cardiacmotion is at a minimum need to be extracted retrospectivelyto minimize blurring and motion artefacts (3.4, 3.5)5, 6.This process is called cardiac gating (3.2). Once the datahave been acquired they can be reconstructed withretrospective gating in any phase of the cardiac cycle byshifting the initial point of the image reconstruction windowrelative to the R-wave. Therefore, the combination of z-interpolation and cardiac gating enables a stack of paralleltomographic images to be generated which represent theheart in the same phase of the cardiac cycle5, 6. A realoptimization of retrospective gating is yet to be achieved.
Patient selection
Inclusion criteriaNormally inclusion criteria for the scan are HR <65 bpm(spontaneous or induced by drugs) and ability to maintainbreath-hold for a period compatible with the scan time2, 3, 7.Both these criteria are aimed at avoiding motion artefacts.Even though MDCT coronary angiography can bediagnostic with a higher HR, motion artefacts progressivelyreduce the number of segments that can be visualizedcorrectly8. The second criterion aims at avoiding artefactsassociated with respiratory motion.
Exclusion criteriaPatients with a HR ≥70 bpm, known allergies to iodinatedcontrast agent, renal insufficiency (serum creatinine >120mmol/l), pregnancy, respiratory failure, unstable clinicalconditions, and severe heart failure are excluded from theMDCT coronary angiography study. In cases of mild renalfailure, the administration of contrast agent may betolerated better if an iso-osmolar agent is used and/or if thepatient is adequately hydrated prior to contrast agentinjection9. However, some low-osmolar agents that can offerimproved attenuation, e.g. iomeprol (Iomeron-400), havealso been shown to be suitable for renally impaired subjectsin a recent study10.
3.4 Positioning the reconstruction time window. Severalprinciples need to be borne in mind regarding thepositioning of the time window when performing imagereconstruction in MDCT coronary angiography. Theoperator should concentrate on three main areas of theECG trace. The first (a) is the end-diastolic phase. In thisphase the ventricle has completed filling, just prior to atrialsystole and motion is at a minimum. The second phase(b) is the early mid-diastolic phase. In this phase the heartis filling and there is generally residual motion which doesnot allow adequate coronary artery imaging. The thirdphase (c) is end-systole. In this phase the heart is inisovolumetric contraction and motion is at a minimum. Theimages obtained in this phase can be just as valid asthose obtained at end-diastole and in a number of caseseven better.
R Rc b a
ECG
From 25 to 35%+200 to +300 ms
From 55 to 70%-450 to -300 ms
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 13

To obtain images in the diastolic phase, some operatorsreconstruct the images in relation to the phase (i.e. apercentage) of the cardiac cycle (typically 50–60% of theR–R interval), whereas others use the time window of the
absolute interval prior to the peak of the next R-wave(typically 300–400 ms; 3.5)12, 13. Multiple reconstructionsare usually performed in different time windows, and thephysician/operator successively selects the dataset wheremotion artefacts are minimal, paying particular attention tothe visualization of the right coronary artery14. In MDCTcoronary angiography different time windows can beoptimized and used in the same patient for the visualizationof the left and right coronary arteries4, 13, 14. Improving thetemporal resolution of the MDCT coronary angiographyscan by increasing gantry rotation speed is subject toobvious limitations. To overcome these difficulties new datapostprocessing strategies have been proposed to furtherincrease temporal resolution. With the simultaneousacquisition of multiple slices using an MDCT coronaryangiography scanner and the relative overlapping of thevolume acquired, multisegment reconstructions can becreated.
In a multisegment reconstruction data acquired in thesame cardiac phase but from different cardiac cycles arecombined in a single image. In this case the temporalresolution will depend on the number and size of thesegments used for the creation of a single image, but it willbe higher than that derived from a single segment5. Thistechnique is sensitive to variations in beat-per-beat HR andthe current implementation of these algorithms does notalways improve image quality15–19.
Prospective triggering
The first geometry for ECG synchronization applied totomographic equipment was prospective ECG triggering. Inparticular this technique was applied to an older technology(i.e. electron beam computed tomography) that could relyon a very high temporal resolution in the range of50–100 ms. This technique suffered from low spatialresolution and the field of application was mainly calciumscore. In the last 2 years CT technology has producedscanners with newer software and/or very high temporalresolution (i.e. dual-source CT with 83 ms temporalresolution). New software applications allow prospectivescanning using a ‘pad’ (a temporal window that can bemodified according to the operator’s experience and thepatient’s HR). Combining these newer technologies withaggressive HR control it is possible to obtain diagnosticimage quality with prospective ECG triggering (3.2)
Basics of cardiac CT14
3.5 End-diastolic positioning of temporal windows. A: Thetemporal windows are positioned in the end-diastolicphase consecutively prior to the next R wave at 50 msdistance each. B: The temporal windows are positioned inthe end-diastolic phase at 5% R–R interval distance.
R
A
B
-450 ms
R
-400 ms-350 ms
100%
60%
R
65%70%
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 14

Basics of cardiac CT 15
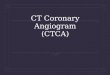
3.6 Prospective tube current modulation. Whilereconstruction can be reliably performed in the end-diastolic phase (especially at low and regular heart rates),tube current can be modulated and reduced to 4–20% ofthe peak during the systolic phase.
Dose
Radiation dose has been one, if not the main, issue ofcardiac CT since the first reports. The increase in spatialresolution brought an inevitable increase in dose. With 64-slice CT and no special means for reduction, the range ofdose was from 10 to 25 mSv. The first means of reducingradiation dose was applied to retrospective ECG gating andrelied on ECG-controlled prospective tube currentmodulation (3.6). Using this technique it is possible toreduce radiation dose by up to 50% depending on thepatient’s HR (the lower the HR, the lower the dose). Therecent implementation of prospective ECG triggering hasled to a dramatic reduction in radiation dose due to thecapability of exposing the patient to radiation only in thedesired phase without significant deterioration of imagequality (range 1–4 mSv).
Limitations in MDCT coronaryangiography
Patients with an HR higher than 70 bpm should notundergo MDCT coronary angiography. Only patients withslightly irregular cardiac rhythms can be included (e.g. earlybeat, atrial fibrillation, left bundle-branch block, prolongedQRS complex, HR less than 40 bpm). In this case the scanshould not be performed with ECG-controlled tube currentmodulation11. In the presence of an abnormal HR thelocation of the period with lowest dose will be variable andcan be included within diastole. In addition, the presence ofrhythm irregularities, with the exclusion of low HR (<40bpm), does not allow the application of multisegmentreconstruction algorithms20, 21. This is due to the variabilityin diastolic filling, which hampers the combination of dataoriginating from contiguous cardiac cycles.
Future developments and outlook
The newer technical developments are all aiming to: (1)reduce radiation dose; (2) increase image quality; and (3)extend the spectrum of applications.
The reduction in radiation exposure is already a realitysince the latest solutions (dual-source CT) allow an averagedose of 1–2 mSv. The implementation of dual-energy willallow further reductions in dose to sub-mSv cardiac CT.
Image quality will increase due to the improvement ofdetector technology (more sensitivity and speed). The finalobjective would be flat panel technology with 0.2 mm3
resolution. The spectrum of applications will be enhancedagain with the implementation of dual-energy. Thepossibility of obtaining multiparametric imaging of the heartwith CT will enhance plaque characterization, delayedenhancement, and perfusion capabilities without significantimpact on radiation dose.
Conclusions
The recent developments and technological research incardiac imaging with MDCT are integrating with, andprofoundly changing, the diagnostic protocol of the patientwith suspected coronary artery disease, for whompercutaneous coronary angiography has for long been theimaging modality of absolute diagnostic value. It shouldnonetheless be borne in mind that although MDCTcoronary angiography is a promising technique, it is the soledomain of highly skilled operators. The clinical outcome ofthe technique is in fact closely associated with theoptimization of each step of the procedure.
Dose
Time
Max
Min
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 15

Basics of cardiac CT16
References
1. Flohr TG, Schoepf UJ, Kuettner A, et al. (2003)Advances in cardiac imaging with 16-section CT systems.Acad Radiol 10:386–401.
2. Nieman K, Cademartiri F, Lemos PA, et al. (2002)Reliable noninvasive coronary angiography with fastsubmillimeter multislice spiral computed tomography.Circulation 106:2051–2054.
3. Ropers D, Baum U, Pohle K, et al. (2003) Detection ofcoronary artery stenoses with thin-slice multidetector rowspiral computed tomography and multiplanarreconstruction. Circulation 107:664–666.
4. Achenbach S, Ulzheimer S, Baum U, et al. (2000)Noninvasive coronary angiography by retrospectivelyECG-gated multislice spiral CT. Circulation102:2823–2828.
5. Ohnesorge B, Flohr T, Becker C, et al. (2000) Cardiacimaging by means of electrocardiographically gatedmultisection spiral CT: initial experience. Radiology217:564–571.
6. Kachelriess M, Kalender WA. (1998) Electrocardiogram-correlated image reconstruction from subsecond spiralcomputed tomography scans of the heart. Med Phys25:2417–2431.
7. Mollet NR, Cademartiri F, Nieman K, et al. (2004)Multislice spiral computed tomography coronaryangiography in patients with stable angina pectoris. J AmColl Cardiol 43:2265–2270.
8. Nieman K, Rensing BJ, van Geuns RJ, et al. (2002) Non-invasive coronary angiography with multislice spiralcomputed tomography: impact of heart rate. Heart88:470–474.
9. Aspelin P, Aubry P, Fransson SG, et al. (2003)Nephrotoxic effects in high-risk patients undergoingangiography. N Engl J Med 348:491–499.
10. Thomsen HS, Morcos SK, Erley CM, et al.;Investigators in the Abdominal Computed Tomography:IOMERON 400 Versus VISIPAQUE 320 Enhancement(ACTIVE) Study (2008) The ACTIVE Trial:comparison of the effects on renal function of iomeprol-400 and iodixanol-320 in patients with chronic kidneydisease undergoing abdominal computed tomography.Invest Radiol 43(3):170–178.
11. Jakobs TF, Becker CR, Ohnesorge B, et al. (2002)Multislice helical CT of the heart with retrospective ECGgating: reduction of radiation exposure by ECG-
controlled tube current modulation. Eur Radiol12:1081–1086.
12. Nieman K, Oudkerk M, Rensing BJ, et al. (2001)Coronary angiography with multi-slice computedtomography. Lancet 357:599–603.
13. Georg C, Kopp A, Schroder S, et al. (2001) [Optimizingimage reconstruction timing for the RR interval inimaging coronary arteries with multi-slice computerizedtomography]. Rofo Fortschr Geb Rontgenstr Neuen BildgebVerfahr 173:536–541.
14. Hong C, Becker CR, Huber A, et al. (2001) ECG-gatedreconstructed multi-detector row CT coronaryangiography: effect of varying trigger delay on imagequality. Radiology 220:712–717.
15. Flohr T, Ohnesorge B. (2001) Heart rate adaptiveoptimization of spatial and temporal resolution forelectrocardiogram-gated multislice spiral CT of the heart.J Comput Assist Tomogr 25:907–923.
16. Cademartiri F, Luccichenti G, Marano R, et al. (2003)Non-invasive angiography of the coronary arteries withmultislice computed tomography: state of the art andfuture prospects. Radiol Med (Torino) 106:284–296.
17. Sato Y, Matsumoto N, Kato M, et al. (2003)Noninvasive assessment of coronary artery disease bymultislice spiral computed tomography using a newretrospectively ECG-gated image reconstructiontechnique. Circ J 67:401–405.
18. Cademartiri F, Mollet NR, Lemos PA, et al. (2004)Standard vs. user-interactive assessment of significantcoronary stenoses with multislice computed tomographycoronary angiography. Am J Cardiol 94:1590–1593.
19. Austen WG, Edwards JE, Frye RL, et al. (1975) Areporting system on patients evaluated for coronary arterydisease. Report of the Ad Hoc Committee for Grading ofCoronary Artery Disease, Council on CardiovascularSurgery, American Heart Association. Circulation51(Suppl 4):5–40.
20. Dewey M, Laule M, Krug L, et al. (2004) Multisegmentand halfscan reconstruction of 16-slice computedtomography for detection of coronary artery stenoses.Invest Radiol 39:223–229.
21. Halliburton SS, Stillman AE, Flohr T, et al. (2003) Dosegmented reconstruction algorithms for cardiac multi-slice computed tomography improve image quality? Herz28:20–31.
CTCA Bracco final_hl corr.qxd:Dementia final.qxd 15/11/10 08:11 Page 16