Embed Size (px)
Citation preview

CS 2015
Pressures, Flows and Volumes during the Cardiac Cycle.
Christian StrickerAssociate Professor for Systems Physiology
ANUMS/JCSMR - ANU
[email protected] http://stricker.jcsmr.anu.edu.au/Cardiac_cycle.pptx
THE AUSTRALIAN NATIONAL UNIVERSITY

CS 2015

CS 2015
AimsAt the end of this lecture students should be able to
• outline the events are used to time the CC;
• describe what delimits systole and diastole; i.e. heart
sounds (S1 and S2);
• draw the important features of pressure, volume and flow
changes during cardiac cycle in ventricles, atria and aorta;
• outline when and how atria and ventricles are filled;
• explain how stroke volume is determined by both, systolic
and diastolic pressures; and
• recognise the relative timing between left and right atria
and ventricles.

CS 2015
Contents
• Linking elements within the CC
• ECG for objective timing
• Cardiac sounds (phonocardiography)
• Heart as two serially connected pumps
• Left ventricle, aorta and left atrium
• Blood pressure change and stroke volume
• Right ventricle and central venous pressure
• Relative timing between two ventricles

CS 2015
Events within Cardiac Cycle• Electrical events (“Pump control”)
– Ionic current flow and action potentials: ECG• EC-coupling
• Mechanical events (“Pump action”)– Muscle contraction: Auscultation
• Pressure generation– Movement of valves (directionality of flow)
» Sounds, clicks and murmurs
– Flow of blood out of ventricle
– Volume changes
– Pressure and volume waves (pulse; see later)

CS 2015
Clinical Relevance• Why are these concepts important?
• Interpretation of clinical signs/findings
to get insight into cardiac function:– Auscultation and phonocardiography
– ECG
– Pulse pressure curves
– Echocardiography (ultrasound)
– Cardiac catheter
– …
• Used daily many times…
Complexity

CS 2015
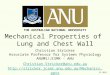
Electrical Events
• From action potentials to ECG.
• ECG provides precise way to determine timing/phase– P wave: Atrial depolarisation.
– QRS complex: Ventricular depolarisation - start of systole.
– T wave: Ventricular repolarisation - end of systole.
Mod
ified
from
Ber
ne e
t al.,
200
4

CS 2015
Mechanical Properties of Heart
• Two serially connected
pumps with a high (left)
followed by a low (right)
pressure vascular bed.
• Directionality enforced by a
pair of valves at in- and out-
flow of each chamber.
• Failing of one part
dramatically imposes load
on preceding element(s).

CS 2015
Systole - Diastole
• Clinical term.
• Systole = period between
S1 → S2 = contraction and ejection
period.
• Diastole = period between S2 →
S1 = relaxation and filling period.
• Duration of systole is quite
constant, however, diastole varies
with heart rate.
• To identify systole and diastole, no
fancy tool required… just ears and
stethoscope: you hear it…

CS 2015
Heart Sounds
S1: Closure of the mitral/tricuspid valves.
S2: Closure (”slamming shut”) of the aortic/pulmonary valves.
Typically split during respiration; during inspiration, venous
return to RA↑ but LA↓ (pooling in pulmonary bed; see later).
S3: Faint rumble; opening of mitral/tricuspid valve with flow
murmur into ventricles (typically heard in young people).
S4: Faint rumble; flow murmur caused by atrial contraction.

CS 2015
Left Ventricle
• Contraction after electrical pacing
• Pressure range:
0 - 120 torr
• Systole duration:
~ 0.3 s @ 75 bpm
• Diastole duration:
variable (~0.5 s)
• Peak diastolic volume:
120 mL
• End-systolic volume:
40 mL
• Stroke volume (SV):
80 mL

CS 2015
Role of Valves
• The role of valves is to
– separate pressures when closed; i.e. Pbefore ≤ Pafter;
– and direct flow when open; i.e. Pbefore > Pafter.
• Valve abnormalities cause murmurs.– Valvular stenosis: narrowing of open valve diameter; requires increased
ventricular pressure to maintain flow through narrowed valve.
– Valvular regurgitation: failure of valve to seal properly: no pressure
separation → flow in both directions; may involve large volumes.

CS 2015
Aortic Trunk
• SV (homeostatic requirement):
80 mL
• If PLV > PAO : Aortic valve opens.
– AV does not close at Ppeak → due to highest flow
and elasticity of AO.
• Notches indicate valve movements.
• Pressure difference (ΔP):
40 torr
• Duration of blood ejection:
~200 ms
• Ejected volume = SV =
80 mL
• ΔP determines SV: longer ejection → SV↑.

CS 2015
Left Atrium
• SV (homeostatic requirement): 80 mL
• If PLA < PLV: Mitral valve closes.
• Atrium fills towards end of systole.
• If PLA > PLV: Mitral opening (early diastole).
• Under resting conditions, atrial contraction
represents only a “last little push” to fill
ventricle (15%).

CS 2015
Valvular Plane Displacement
• Systole: Movement of valvular
plane towards cardiac apex
(~16 mm) causes mechanical
“suction” on central veins:– Increased atrial filling during
late systole.
– Mechanism: “horror vacui”
imposed by pericardial space.
• Diastole: Movement back
(early filling phase) rises atrial
pressure slightly, aiding
ventricular filling.Modified from Schmidt & Thews, 1977

CS 2015
7 phases of the cycle• Systole
– Contraction phase (isovolumetric)
– Ejection phase• Fast
• Slow
• Diastole– Relaxation phase (isovolumetric)
“elastic recoil”
– Filling phase• Passive ventricular filling
– Rapid ventricular filling
– Slow ventricular filling
• Atrial contraction
Synopsis

CS 2015
• SV (homeostatic requirement):
80 mL
• Largely analogous to phases in left
ventricle, except for slightly changed
valve timings.
• Pressure difference (ΔP):
20 torr
• Ohm’s law: I = ΔP / R; to maintain flow,
Rpulm. must be no more than half Rsyst..
Right Ventricle

CS 2015
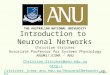
Timing of Right and Left Ventricle
• Cycle starts right atrium (pacing in SAN) and
ends in right ventricle (delayed contraction).
• S1 and S2 are “composed” of contributions
from both respective valves in both ventricles.
Bor
on/B
oulp
aep
2003

CS 2015
Right Atrium & Central Veins
• SV (homeostatic requirement):
80 mL
• Can be seen on jugular vein.
• Measured via a pulse transducer.
• Pulse wave in central veins results from
volume and pressure changes in RA.
• Timing and amplitudes depend on
location (delay and attenuation).

CS 2015
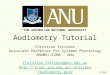
Systole and Diastole Timing
• Pulse rate can be altered over a 3 - 4 fold range.
• At heart rates (HR) >100 bpm, tdiastole < tsystole: Filling ↓.
– Systole at 150 bpm is shorter than that at 50 bpm.
• At high HR, atrial contractions become important.
Mod
ified
from
Kol
ler,
1979

CS 2015
Take-Home Message• Systole: S1 → S2
• Diastole: S2 → S1
• The 7 phases of the cardiac cycle are: isovolumetric
contraction, fast and slow ejection, isovolumetric rela-
xation, fast and slow ventricular filling, atrial contraction.
• Whilst diastole is variable, systole is ± constant.
• SV is dependent on difference between systolic and
diastolic pressure: difference ↑ → SV ↑.
• Most of atrial filling occurs during systole.
• “Insignificance” of atrial contraction at rest.
• “Pump failure” causes load on preceding element(s).

CS 2015
MCQJoe Ackermanis, a 26 year-old male, was diagnosed with an aortic valve
stenosis (narrowing of valve opening). Compared to a normal heart, which
of the following descriptions best describes the pressures in the heart of
this person?Peak atrial pressure
Peak ventricular pressure
Peak aortic pressure
a) ↑ ↑ ↑
b) ↓ ↓ ↓
c) ↓ ↓ ↑
d) ↓ ↑ ↑
e) ↑ ↑ ↓

CS 2015
That’s it folks…

CS 2015
MCQJoe Ackermanis, a 26 year-old male, was diagnosed with an aortic valve
stenosis (narrowing of valve opening). Compared to a normal heart, which
of the following descriptions best describes the pressures in the heart of
this person?Peak atrial pressure
Peak ventricular pressure
Peak aortic pressure
a) ↑ ↑ ↑
b) ↓ ↓ ↓
c) ↓ ↓ ↑
d) ↓ ↑ ↑
e) ↑ ↑ ↓