Embed Size (px)
Citation preview

Blood
Crystalloids, colloids, blood, blood products and blood substitutesdaniel low
Michael Milne
AbstractThe choice of fluid in a given clinical scenario relies on knowledge of the
physiology and pharmacology of the fluid. A broad range of fluids are
discussed in this article, with particular emphasis on problems associ-
ated with excess administration of 0.9% saline. Colloids, blood, blood
products and blood substitutes are also discussed. Balancing the risks
of allogenic blood transfusion for a patient and transfusion thresholds
are considered. The potential of haemoglobin substitutes are still yet
to be realized; however PolyHeme is currently in a phase 3 pre-hospital
trauma trial.
Keywords artificial haemoglobins; blood products; colloids; crystalloids;
perflurocarbons
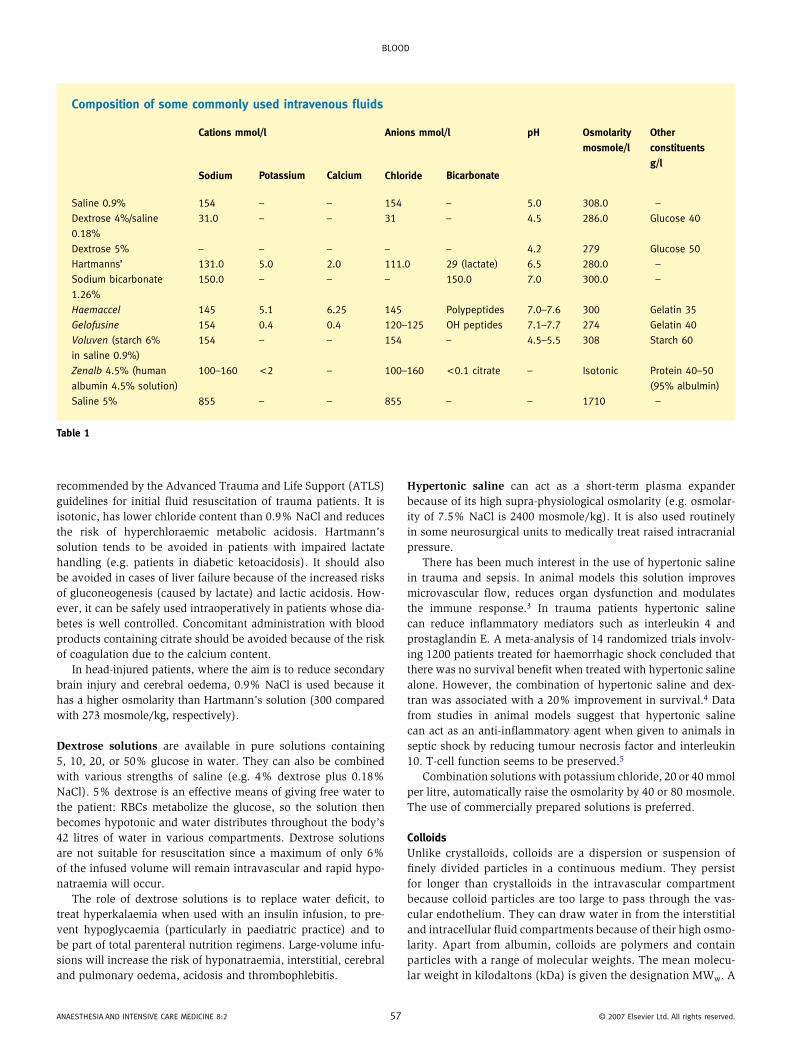
There are many fluids available for intravenous administration. They are normally categorized as crystalloids or colloids. A full understanding of the clinical scenario, the pharmacology of the solution and fluid distribution in the body in both normal and abnormal physiology are essential for choosing the most appro-priate fluid. The physiology of fluid replacement is discussed in Anaesthesia and intensive care medicine 2:2: 67–9. All fluids cause an initial expansion of the intravascular compartment. The duration of this effect depends on how freely the fluid can move across the vascular endothelium. The composition of some commonly used intravenous fluids is shown in Table 1.
CrystalloidsCrystalloids are solutions of small ionic or non-ionic particles that can pass through a semi-permeable membrane when in solu-tion. These solutions have different concentrations of sodium chloride and other salts, and some solutions contain a form of bicarbonate precursor, such as lactate. Dextrose solution does not contain sodium chloride or other salts, and its administration is a convenient way of giving a patient free water to allow the
Daniel Low, MRCPCH, FRCA, is Specialist Registrar in Anaesthesia in
Bristol. He qualified from the University of Nottingham in 1997 and
trained in paediatrics. His research interests include medical education
and medical simulation.
Michael Milne, BA, MB, BChir, MRCP, FRCA, is Consultant in Anaesthesia and
Intensive Care at North Bristol NHS Trust. He qualified from Cambridge
in 1983 and trained in Southampton and Bristol. His interests include
vascular and neurovascular anaesthetic care.
ANAESTHESIA ANd INTENSIVE CARE MEdICINE 8:2 5
excretion of a sodium load or to slowly rehydrate a hypernatrae-mic state.
0.9% Sodium chloride (saline) is indicated in sodium depletion, which may arise from conditions such as diabetic ketoacidosis, ileus, ascites or gastroenteritis. It has a calculated osmolarity of 308 mosmole/kg; the measured osmolarity is slightly lower because ions do not completely dissociate. 1 litre of 0.9% saline given to a 70 kg individual will distribute into an extracellular fluid (ECF) compartment of 14 litres, leaving a maximum of 35% of the administered saline in the intravascular space. Thus 3 litres of 0.9% NaCl are required to replace each litre of blood loss.
0.9% NaCl is commonly, although incorrectly, called normal saline. The term ‘normal’ does not imply physiological appropri-ateness. A ‘normal’ solution means a molar solution (i.e. 1 litre of solution contains 1 mole of the solute). For NaCl a 1 molar solution would contain 58.5g NaCl per litre (molecular weight Na, 23; Cl, 35.5). The following calculation demonstrates the actual content of 0.9% NaCl solution:• 0.9% NaCl = 0.9 g NaCl in 100 ml water or 9 g NaCl in 1000 ml water.• Since 58.5 g = 1 mole; 9/58.5 = 0.154 moles of NaCl in 1 litre solution = 154 mmol solution in 0.9% saline.
0.9% NaCl is often inappropriately used. A few litres cause a hypercoagulable state and a hyperchloraemic metabolic acidosis. In the postoperative setting, where the stress response encour-ages the body to retain sodium and hence water, excessive use of 0.9% NaCl can raise serum osmolarity and cause fluid overload. Pulmonary oedema can occur if there is a breakdown in capillary permeability or impaired left ventricular function. Several pro-spective randomized studies have compared the effects of 0.9% NaCl and balanced salt-based fluids such as Hartmann’s solution, and have found greater urinary output in patients treated with balanced salt-based solutions. In a prospective, randomized and blinded study of 200 cardiac surgical patients who received nor-mal saline-based hydroxyethyl starch (HES), balanced salt HES, Hartmann’s or normal saline-based 5% albumin solution as their intraoperative fluid therapy, those patients treated with normal saline-based fluids had significantly worse renal function with a higher requirement for postoperative dialysis than those treated with balanced salt-based solutions.
Post-saline acidosis has been recognized since 1923. Whether acidosis is caused by hyperchloraemia (hence the term hyper-chloraemic acidosis) or whether it is simply a metabolic acido-sis associated with hyperchloraemia is under continued debate. Recent work has extended Van Slyke’s hypothesis from 1917.1,2 Electroneutrality is a relatively new concept in acid–base theory: anions, particularly chloride, are considered as acids; and cations, particularly sodium, as bases. In this biochemical model, the size of the difference in charge between strongly charged cations and strongly charged anions is thought to influence acid–base status. Regardless of the outcome of this debate, hyperchloraemia can cause renal vasoconstriction and a decrease in glomerular filtra-tion rate.
Hartmann’s solution (Ringer’s lactate) is a balanced salt solution that has a composition similar to ECF. Formulated by Sydney Ringer for use in paediatric metabolic acidosis, it is the crystalloid of choice for ECF replacement. This solution is also
6 © 2007 Elsevier ltd. All rights reserved.
Blood
Composition of some commonly used intravenous fluids
Cations mmol/l Anions mmol/l pH Osmolarity
mosmole/l
Other
constituents
g/lSodium Potassium Calcium Chloride Bicarbonate
Saline 0.9% 154 – – 154 – 5.0 308.0 –
dextrose 4%/saline
0.18%
31.0 – – 31 – 4.5 286.0 Glucose 40
dextrose 5% – – – – – 4.2 279 Glucose 50
Hartmanns’ 131.0 5.0 2.0 111.0 29 (lactate) 6.5 280.0 –
Sodium bicarbonate
1.26%
150.0 – – – 150.0 7.0 300.0 –
Haemaccel 145 5.1 6.25 145 Polypeptides 7.0–7.6 300 Gelatin 35
Gelofusine 154 0.4 0.4 120–125 oH peptides 7.1–7.7 274 Gelatin 40
Voluven (starch 6%
in saline 0.9%)
154 – – 154 – 4.5–5.5 308 Starch 60
Zenalb 4.5% (human
albumin 4.5% solution)
100–160 <2 – 100–160 <0.1 citrate – Isotonic Protein 40–50
(95% albulmin)
Saline 5% 855 – – 855 – – 1710 –
Table 1
recommended by the Advanced Trauma and Life Support (ATLS) guidelines for initial fluid resuscitation of trauma patients. It is isotonic, has lower chloride content than 0.9% NaCl and reduces the risk of hyperchloraemic metabolic acidosis. Hartmann’s solution tends to be avoided in patients with impaired lactate handling (e.g. patients in diabetic ketoacidosis). It should also be avoided in cases of liver failure because of the increased risks of gluconeogenesis (caused by lactate) and lactic acidosis. How-ever, it can be safely used intraoperatively in patients whose dia-betes is well controlled. Concomitant administration with blood products containing citrate should be avoided because of the risk of coagulation due to the calcium content.
In head-injured patients, where the aim is to reduce secondary brain injury and cerebral oedema, 0.9% NaCl is used because it has a higher osmolarity than Hartmann’s solution (300 compared with 273 mosmole/kg, respectively).
Dextrose solutions are available in pure solutions containing 5, 10, 20, or 50% glucose in water. They can also be combined with various strengths of saline (e.g. 4% dextrose plus 0.18% NaCl). 5% dextrose is an effective means of giving free water to the patient: RBCs metabolize the glucose, so the solution then becomes hypotonic and water distributes throughout the body’s 42 litres of water in various compartments. Dextrose solutions are not suitable for resuscitation since a maximum of only 6% of the infused volume will remain intravascular and rapid hypo-natraemia will occur.
The role of dextrose solutions is to replace water deficit, to treat hyperkalaemia when used with an insulin infusion, to pre-vent hypoglycaemia (particularly in paediatric practice) and to be part of total parenteral nutrition regimens. Large-volume infu-sions will increase the risk of hyponatraemia, interstitial, cerebral and pulmonary oedema, acidosis and thrombophlebitis.
ANAESTHESIA ANd INTENSIVE CARE MEdICINE 8:2 5
Hypertonic saline can act as a short-term plasma expander because of its high supra-physiological osmolarity (e.g. osmolar-ity of 7.5% NaCl is 2400 mosmole/kg). It is also used routinely in some neurosurgical units to medically treat raised intracranial pressure.
There has been much interest in the use of hypertonic saline in trauma and sepsis. In animal models this solution improves microvascular flow, reduces organ dysfunction and modulates the immune response.3 In trauma patients hypertonic saline can reduce inflammatory mediators such as interleukin 4 and prostaglandin E. A meta-analysis of 14 randomized trials involv-ing 1200 patients treated for haemorrhagic shock concluded that there was no survival benefit when treated with hypertonic saline alone. However, the combination of hypertonic saline and dex-tran was associated with a 20% improvement in survival.4 Data from studies in animal models suggest that hypertonic saline can act as an anti-inflammatory agent when given to animals in septic shock by reducing tumour necrosis factor and interleukin 10. T-cell function seems to be preserved.5
Combination solutions with potassium chloride, 20 or 40 mmol per litre, automatically raise the osmolarity by 40 or 80 mosmole. The use of commercially prepared solutions is preferred.
ColloidsUnlike crystalloids, colloids are a dispersion or suspension of finely divided particles in a continuous medium. They persist for longer than crystalloids in the intravascular compartment because colloid particles are too large to pass through the vas-cular endothelium. They can draw water in from the interstitial and intracellular fluid compartments because of their high osmo-larity. Apart from albumin, colloids are polymers and contain particles with a range of molecular weights. The mean molecu-lar weight in kilodaltons (kDa) is given the designation MWw. A
7 © 2007 Elsevier ltd. All rights reserved.

Blood
better indicator of performance is the number average molecular weight, given the designation MWn, which can account for the distribution of weights and not just an average. In addition to the MWn, the ionic charge of the particles and the permeability of the vascular endothelium to the colloid influences longevity of the solution in the intravascular compartment.
Gelatins (Gelofusine and Haemaccel) contain modified gelatins between 30 and 35 kDa MWn. They have no oxygen-carrying ability, a half-life of 3 hours in the circulation and a small (0.4%) risk of allergic reactions. They have no clinical effect on coagula-tion, except that caused by haemodilution.
Hydroxyethyl starch (HES) solution comprises hydroxyethyl etherified amylopectin molecules. Their properties vary accord-ing to their concentration, molecular weight and extent of hydrox-ylation or substitution. They have an intravascular half-life of 24 hours, and are hydrolysed by amylase into smaller molecules. Those with a MW of less than 50 kDa are renally excreted. Amy-lase action is suppressed by higher levels of substitution and with greater etherification at the C2 rather than the C6 position. HES can plug capillary leaks induced by sepsis and trauma, and restore macrophage function after haemorrhagic shock.
HES can cause a coagulopathy, which is thought to be due to depressed platelet function secondary to diminished von Willebrand factor (vWF) antigen. Another explanation for this coagulopathy is that saline-based HES preparations do not con-tain the calcium required for platelet activation and the function of the platelet GPIIb/IIIa receptor, which binds fibrinogen and causes aggregation.
Other side effects of HES include intractable pruritis and extravasation injuries. HES does not interfere with blood cross- matching.
Dextrans are derived from the action of the bacterium Leuconostoc mesenteroides on a sucrose medium via the enzyme dextran sucrase. The product is a group of branched polysaccharides of 200,000 glucose units. These undergo partial hydrolysis to produce molecules of mean MW 40, 60, 70 and 110 kDa.
Dextran 40 is hyperoncotic and initially acts as a plasma expander before its rapid elimination by the kidneys. Its main use is for promoting peripheral blood flow (in prophylaxis for deep vein thrombosis and in maintaining graft patency in flap surgery). Improvement of blood flow occurs because of a reduc-tion in plasma viscosity and possibly by reducing the interaction between the vascular endothelium and the cellular components of blood. Dextrans reduce platelet adhesiveness, enhance fib-rinolysis and may reduce factor VIII activity. Doses above 1.5 g/kg produce a coagulopathy. Modern dextrans do not interfere with blood cross-matching. Renal tubular obstruction may occur because of dextran casts. Anaphylaxis can occur (1/4500) from previous cross-immunization against bacterial antigens forming dextran-reactive antibodies.
Blood and blood productsBlood is obtained from volunteer donation within the UK. The administration of this process rests with the National Blood Service, a special health authority of the NHS. Currently fresh-frozen plasma (FFP) treated with methylene blue for viral
ANAESTHESIA ANd INTENSIVE CARE MEdICINE 8:2 58
inactivation is sourced from the USA. This is because of the risk of transmitting prion-related new variant Creutzfeld-Jakob disease via transfusion.
In acute blood loss, resuscitation with fresh whole blood is the ideal replacement because it has oxygen-carrying ability and expands the intravascular compartment. The transfusion threshold has been on a gradual decline during the past two decades, which has been prompted by safety concerns regarding HIV in the 1980s. The decision to transfuse a patient needs to balance the risks of varying severities of anaemia and the risks of allogenic transfusion.
Balancing risks of allogenic transfusion: all blood products carry risks of infection with known and unknown agents. Risks are reduced with screening, chemical and heat treatment, but are not eliminated. Blood products also carry the risks of anaphylaxis. The risk of bacterial contamination is highest with the use of platelets because they are stored at room temperature. ABO incompatibility of RBC products and transfusion-related lung injury (TRALI) are the commonest specific risks of transfusion. TRALI is an immune- mediated condition mediated by antibodies in the transfused plasma. Graft-versus-host disease is a delayed transfusion reaction of donor granulocytes against recipient tissues. The risk of this dis-ease has been reduced by routine leucodepletion of donated blood.
In the TRICC trial (Transfusion Requirements In Critical Care)6 838 patients were randomly allocated to a restrictive or liberal transfusion strategy. The restrictive group were transfused at hae-moglobin levels of 7 g/dl, the liberal group were transfused at 10g/dl. The 30-day mortality was slightly lower in the restrictive group (18.7 versus 23.3%). Subgroup analysis of patients with cardiovascular disease did not show any difference in mortality between the two strategies.
Blood is collected from donors into an anticoagulant, commonly CAPD-1 (citrate, adenine, phosphate and dextrose). A unit of whole blood has a volume of 400–450 ml. It is tested for common serious transmissible viruses (including HIV, hepatitis B and C). Most units are centrifuged to separate out the component parts, leaving 250 ml of packed RBCs plus supernatant. SAGM is a saline preservative containing saline, adenine, glucose and mannitol, and 100ml is added to the packed RBCs to increase the volume to 350 ml and to give a haematocrit of 0.6–0.7. No appreciable citrate or clotting factors remain in the packed cells.
Packed RBCs can be given to increase patients’ oxygen-carrying capacity. However, care should be taken when infusing large volumes because hypothermia or low levels of 2, 3 diphospho-glycerate can cause a left shift in the oxygen dissociation curve, which impairs oxygen delivery to tissues. RBCs can be stored for 35 days at 4°C or liquid-nitrogen frozen for longer storage.
Blood products: the supernatant from a unit of whole blood is centrifuged again at 20°C to yield 1 unit of platelets containing 50–70 ml of plasma, which can be stored at 20–24°C for up to 5 days. Alternatively, platelets can be obtained by platelet-pheresis, which yields 6 units from one donor. The remaining plasma is processed and frozen to form FFP. The activity of fac-tors V and VIII are preserved in this process. During the rapid thawing of FFP, a gelatinous precipitate is formed, which is rich in factor VIII and fibrinogen. This is called cryoprecipitate, and can be separated, refrozen and stored for up to 1 year.
© 2007 Elsevier ltd. All rights reserved.

Blood
Platelets are essential for normal coagulation. Counts below 50 × 109/litre are associated with increased blood loss during surgery. Counts below 20 × 109/litre are associated with spon-taneous bleeding. Transfusion of platelets is indicated in a bleed-ing patient with thrombocytopenia, platelet dysfunction and prophylactically before an invasive procedure. 1 unit increases the platelet count by 5 × 109/litre, and ABO compatibility is desirable. Compatible platelets survive for 1–7 days and do not cause rhesus sensitization and haemolytic reactions.
FFP contains all plasma proteins. It is indicated for coagulo-pathies caused by isolated factor deficiencies, warfarin therapy, liver failure and thrombotic thrombocytopenic purpura. The ini-tial dose in adults is 15 ml/kg. 1 unit will increase each clotting factor by 2–3%. ABO compatibility is desirable.
Cyroprecipitate is reserved for severe disseminated intravascular coagulation, which results in consumption of all clotting factors especially fibrinogen. This substance is usually indicated when the fibrinogen concentration falls below 1 g/litre.
Albumin is a major plasma protein with a MW of 69 kDa. Albu-min helps to maintain colloid oncotic pressure, preserves micro-vascular integrity, provides binding and transport for molecules and acts as a plasma buffer. Its concentration falls in the critically ill. 4.5% and 20% solutions are available for transfusion and are usually used as plasma expanders rather than as a treatment for hypoalbuminaemia.
Blood substitutesTwo distinct strategies are being developed in the search for an oxygen-carrying blood substitute. One strategy involves the development of haemoglobin-based oxygen carriers (HBOCs) that mimic the role of haemoglobin. The other involves carrying oxygen in a dissolved state using perfluorocarbon emulsions.
Haemoglobin-based oxygen carriers (HBOC): the idea of using purified haemoglobin instead of RBCs has been around since 1916 when a haemoglobin-saline solution was used on humans to treat anaemia. However, this procedure failed because of renal toxicity caused by erythrocyte stromal lipids. Once stroma-free haemoglobins were available it became apparent there were still two main problems: the purified haemoglobin had too high an affinity for oxygen and too short an intravascular half-life. The HBOCs currently in development have been engineered to have a reduced affinity for oxygen (mimicking the effects of 2, 3 diphosphoglycerate) and an extended circulation time.
ANAESTHESIA ANd INTENSIVE CARE MEdICINE 8:2 59
Preventing haemoglobin tetramer breakdown has been achieved by cross-linking tetramers, creating haemoglobin polymers and encapsulating haemoglobin within a lipid vesicle.
PolyHeme is a cross-linked polymer of human haemoglobin, in which two or more tetramers are linked. It uses a pyridoxal molecule bonded to each tetramer, reducing oxygen affinity to a degree that favours tissue oxygen delivery. There is currently a multicentre, phase 3 pre-hospital trauma study that is evaluating the safety of PolyHeme in hypovolaemic trauma patients.
Perfluorocarbon emulsions (PFCEs): originally synthesized dur-ing the development of the atomic bomb, perfluorocarbon emul-sions were given the codename ‘Joe’s stuff’. They are organic compounds in which all the hydrogen molecules are replaced with halogens, principally fluoride. They have the ability to carry large amounts of dissolved oxygen (e.g. perflubron carries 53 ml of oxygen in 100 ml of solution at 25°C). The main side effects of these substances occur in the reticuloendothelial system: flu- like symptoms (cause by macrophage phagocytosis of PFCE molecules), hepatosplenomegaly and thrombocytopenia. Since the molecules cannot be metabolized – because of the strong carbon–fluoride bonds – they take up to 24 months to be elim-inated from the body. ◆
RefeRenCeS
1 van Slyke d, Cullen G. Studies of acidosis I: the bicarbonate
concentration of the blood plasma; its significance, and its
determination as a measure of acidosis. J Biol Chem 1917; 30:
R289–346.
2 Peters JP, Van Slyke dd. Carbonic acid and acid-base balance:
quantitative interpretations clinical chemistry. Philadelphia:
Williams and Wilkins, 1931.
3 del Pilar A, Garrido G. Small volume of hypertonic saline as the
initial fluid replacement in experimental hypodynamic sepsis.
Crit Care 2006; 10: R62.
4 Wade CE, Kramer GC, Grady JJ, et al. Efficacy of hypertonic 7.5%
saline and 6% dextran-70 in treating trauma: a meta-analysis of
controlled clinical studies. Surgery 1997; 122: 609–16.
5 Junger WG, Hoyt dB, Hamreus M, et al. Hypertonic saline activates
protein tyrosine kinases and mitogen-activated protein kinase p38
in T-cells. J Trauma 1997; 42: 437–43 (discussion 443–5).
6 Hebert PC, Wells G, Blajchman MA, et al. A multicenter randomized,
controlled clinical trial of transfusion requirements in critical care.
N Engl J Med 1999; 340: 409–17.
© 2007 Elsevier ltd. All rights reserved.