Embed Size (px)
Citation preview

Crystalloids and Colloids in Trauma Resuscitation: A BriefOverview of the Current DebateSandro B. Rizoli, MD, PhD, FRCSC
Background: Controversy regardingcrystalloids or colloids for resuscitationhas existed for over five decades, andlarge numbers of clinical trials have failedto resolve the controversy. In fact, the lim-itations of these studies have intensifiedthe debate. This overview aims to revisitthe debate of fluid resuscitation in traumapatients by critically appraising the meta-analyses on the subject.
Methods: This study was a criticalanalysis of six meta-analyses found byMEDLINE search.
Results: Overall, the choice of fluidmay have a small or no effect on mortality.In trauma, the use of colloids is associatedwith a trend toward increased mortality.
Conclusion: There is an urgent needfor well-designed clinical trials. Because ofmany limitations, meta-analysis should be
interpreted with caution, possibly as hy-pothesis generating. However, even con-sidering all weaknesses and nuances of in-terpretation, the meta-analyses reviewedsuggest that trauma patients should con-tinue to be resuscitated with crystalloids.
Key Words: Fluid resuscitation,Crystalloid, Colloid, Meta-analysis, Evi-dence-based medicine.
J Trauma. 2003;54:S82–S88.
The controversy over choosing crystalloids or colloids forfluid resuscitation has existed for over five decades.Despite the fact that most physicians today prefer to
make their therapeutic decisions on solid scientific evidence,it is indeed the vulnerability of the present evidence thatintensifies the debate. A quick literature search on the subjectresults in a massive number of studies. In fact, there areenough studies to sustain 11 systematic reviews or meta-analyses or quantitative data synthesis (for this study, theseterms are used interchangeably).1–11 However, the poor qual-ity of the majority of the primary studies, which is subse-quently imparted to the systematic reviews, does nothing tosettle the matter. In practice, the use of colloid or crystalloidfluids varies widely across the globe depending on personalchoices, clinical experience, availability, and cost.12
There are, however, other reasons behind this debate.Fluid administration is one of the most basic concepts inresuscitation and is also part of the daily routine of medicallymanaging most hospitalized patients. Fluid resuscitation isalso a very active area of both clinical and experimentalinvestigation, with a continuous accumulation of new insightsand data.13 Furthermore, topics that never completely vanishmay prove to have merit, as demonstrated with the recent
reemergence of the use of steroids in septic shock or evenhypertonic saline in fluid resuscitation.14–16
The goal of this article is to revisit the “current” debateregarding the choice between crystalloids and colloids for theresuscitation of trauma patients. This was done by exploringthe evidence on this topic in meta-analyses, and by appraisingtheir results and recommendations. The conclusion of thiscritical appraisal is that these systematic reviews should beinterpreted with caution and that there is an urgent need forwell-designed clinical trials in fluid resuscitation. When re-suscitation of all critically ill patients is considered, the com-bined results of the meta-analyses suggest that the choice offluid used for resuscitation has a small or no effect on mor-tality. In contrast, when only resuscitation of trauma patientsis considered, the results are very similar and suggest thatresuscitation with colloids carries an increased mortality.Crystalloids therefore should remain the fluid of choice forthe resuscitation of trauma patients in hemorrhagic shock.
WHY CHOOSE COLLOIDS?Most physicians in the developed world today begin
resuscitating trauma patients according to the AdvancedTrauma Life Support (ATLS) guidelines of the AmericanCollege of Surgeons.17 The current ATLS guidelines call foran aggressive fluid resuscitation regimen that starts with a2-L bolus of crystalloids in adults, preferably lactated Ring-er’s (LR) solution. Resuscitation continues with repeatedboluses of LR solution, blood, and a systematic search andrepair of surgically correctable sources of hemorrhage.17
Crystalloids primarily fill the interstitial space; conse-quently, edema is an expected outcome of resuscitation ac-cording to the ATLS guidelines. To expand plasma volume,the classical axiom is that three times more volume of crys-talloid is required than the volume of blood that was lost.17
Today, this ratio is questioned, and should probably be 7:1 or
Submitted for publication April 13, 2002.Accepted for publication May 21, 2002.Copyright © 2003 by Lippincott Williams & Wilkins, Inc.From the Department of Surgery, Sunnybrook and Women’s College
Health Science Centre, University of Toronto, Toronto, Ontario, Canada.Presented at the Fluid Resuscitation in Combat Symposium, Defence
and Civil Institute of Environmental Medicine, October 25–26, 2001, To-ronto, Ontario, Canada.
Address for reprints: Sandro B. Rizoli, MD, PhD, FRCSC, 2075 Bay-view Avenue, Toronto, Ontario M4N 3M5, Canada; email: [email protected].
DOI: 10.1097/01.TA.0000064525.03761.0C
The Journal of TRAUMA� Injury, Infection, and Critical Care
S82 May Supplement 2003

even 10:1, because of the decreased colloid osmotic pressuresecondary to decreased serum protein concentration fromhemorrhage, capillary leaks, and crystalloid replacement.18
Table 1 provides a good approximation of how much of thetotal volume of crystalloids infused leaks into the extravas-cular compartments (Table 1).
Tissue edema might become an important consideration,especially when dealing with head injury patients where di-lutional hypo-osmolarity may worsen brain edema and im-pact on mortality.19 The dilutional decrease in colloid os-motic pressure by crystalloids may also worsen pulmonaryedema, thus impairing gas exchange.18 It also causes endo-thelial and red blood cell edema, impairing microcirculationand decreasing surface area for tissue oxygen exchange. Suchcirculatory dysfunction might participate in the multiple or-gan dysfunction that follows shock states.20 With normalsaline administration, there is the added concern about hy-perchloremic metabolic acidosis.18
Let us consider the not infrequent situation where atrauma patient is aggressively resuscitated with large volumesof crystalloids. After a while, despite being massively edem-atous with enough tissue edema to compromise organ func-tion, such as pulmonary edema, the patient still has someevidence of being intravascularly depleted.
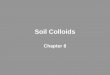
In such a scenario, many physicians, especially in Eu-rope or in an intensive care unit environment, would considerusing colloid fluids for further resuscitation. Colloid fluidshave many attractions and advantages over crystalloid resus-citation. They are more efficient than crystalloids in expand-ing plasma volume and achieve similar resuscitation end-points faster and with much smaller volumes (Table 1).21
Regardless of the evidence that colloids also cause significantbrain and lung edema,22,23 advocates of colloid use argue thatby using smaller volumes and increasing the colloid-osmoticpressure, colloids reduce tissue edema compared with crys-talloids. Colloids such as albumin also increase oxygen de-livery significantly more than LR solution and improve organmicrocirculation.24–26 The expansion in plasma volume andimprovement in organ perfusion by albumin administrationhas been proposed as the explanation for the fact that albuminreduces renal failure and death in cirrhotic patients withspontaneous bacterial peritonitis.27 Even though the highercosts of colloids are frequently mentioned as a concern, thesefigures do not take into account the costs incurred as the
result of resuscitation-associated morbidity and mortality andlength of hospital stay. Furthermore, the low cost of resusci-tation fluids compared with other routine pharmacologic in-terventions exerts no major impact in the surgeon’s choice offluid, and colloids are used in the United States more oftenthan recommended by the Consensus of the University Hos-pital Consortium.28,29
WHICH COLLOID SHOULD BE CHOSEN?Once the physician considers using colloid fluids, the
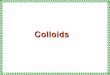
next step is choosing between the different types. There arefour basic types of colloids: albumin and the synthetic dex-trans, gelatins, and starches. An overview of some of theirmost relevant characteristics is presented in Table 2.
The prototypical colloid is albumin, which is synthesizedin the liver and is responsible for 80% of the oncotic pressureof the plasma. Albumin is commercially available in heat-treated preparations, dissolved in isotonic saline. Its colloidosmotic pressure is similar to the oncotic pressure of theplasma, and infusion of the 25% solution expands plasmavolume four to five times the volume infused. Frequentlymentioned disadvantages of albumin include its critical shortsupply, the fact that it is a blood product, the theoretical riskof transmitting unknown infectious particles (such as prions)and, like all other colloids, its cost.
Of the synthetic colloids, dextran and gelatins are rarelyconsidered for the resuscitation of trauma patients, especiallyin North America. Besides its plasma-expanding properties,dextrans have a powerful anticoagulant effect and have beenused for the prevention of postoperative venous thrombosisand pulmonary embolism.30 The anticoagulant properties ofdextrans have limited their indication for the resuscitation oftrauma patients; however, small amounts have been success-fully used to prolong the effect of hypertonic salineinfusion.15 Gelatins are mostly unavailable in North America,and their modest and short-lived effectiveness in expandingplasma volume has decreased the enthusiasm for this type ofcolloid worldwide.30
The remaining option in colloids is hydroxyethyl starch(HES). Although in Europe there are several commerciallyavailable formulations, in North America the options arealmost exclusively restricted to the high-molecular-weighthetastarch and pentastarch.31,32 Different from other colloids,the pharmacokinetics of each HES formulation is determinedby its structure, which includes not only molecular weight butalso degree of substitution (number of hydroxyethyl groupspresent divided by the quantity of glucose molecules) andC2/C6 hydroxylation rate.
This group of HES synthetic colloids, especially pen-tastarch, is very attractive. The colloid osmotic pressure of10% pentastarch is two times that of the oncotic pressure ofthe plasma and expands plasma volume 1.5 times the volumeinfused. Besides their effectiveness in expanding plasma vol-ume, they are readily available, have an unlimited supply,carry no risk of transmitting infectious disease, have minimal
Table 1 Effect of Different Solutions on PlasmaVolume Expansion
Volume infused(mL) Type of Fluid Infused Plasma Volume
Expansion (mL)
1,000 D5W 1001,000 lactated Ringer’s 250
250 7.5% hypertonic saline 1,000500 5% albumin 375100 25% albumin 450500 Pentastarch 500
Crystalloids and Colloids in Trauma Resuscitation
Volume 54 • Number 5 S83

side effects, have a long shelf life, and are less expensive thanalbumin.
With so many favorable characteristics, the next questionis why colloids are not used more often. The answer is the“evidence” suggesting that the use of colloids may be asso-ciated with increased mortality. The next section of thisreview focuses on reviewing the meta-analyses on the con-troversy of choosing between colloids and crystalloids forresuscitation.
WHAT IS THE EVIDENCE?Meta-analyses or systematic reviews were created to
bring together information from randomized controlled trialsof the same intervention. Meta-analyses have become a majorsource of information for clinicians and often provide themost accurate and authoritative guidelines to therapy.
In reviewing the current literature on colloid versuscrystalloid fluid resuscitation in critically ill patients,including trauma, the author encountered nine originalmeta-analyses1–8,11 and two updates of previous meta-analyses.9,10 Of the original meta-analyses, two studies byWade et al. and another by Bunn et al. focused primarily onthe effect of hypertonic saline resuscitation rather than on thedebate between crystalloids and colloids.3,4,11 The two up-dates and the three meta-analyses on hypertonic saline werenot included in this review, which focused on the remainingsix reviews, as follows.
Velanovich (1989) and Bisonni et al. (1991)Velanovich1 and Bisonni et al.2 were the first two meta-
analyses ever performed on fluid resuscitation. These studiesshare many similarities. Meta-analysis had been describedjust a few years earlier, and Velanovich spent most of theMaterial and Methods section explaining the mathematicalbasis of the new methodology. Bisonni et al. criticized Vela-novich for including one study with 472 patients whereas theremaining studies combined included only 354 patients,clearly impacting on the final analysis. Thus, Bisonni et al.simply repeated the earlier analysis, this time excluding thelarge study.
In both analyses, the authors do not report how theprimary randomized controlled trials (RCT) were collected orassessed for validity. Only trials with random allocation andthat reported mortality rates were included. There are briefcomments about nine RCTs that were excluded from Vela-novich’s analysis but not much elaboration about how datawere extracted. There is no information about the differenttypes of colloid or crystalloid fluids used, the different pro-tocols, surgical interventions, age groups, or other patientcharacteristics.
Eight RCTs were included in Velanovich’s study, with826 patients. With the exclusion of one study, Bisonni et al.analyzed 354 patients. Five studies included trauma patients.In Velanovich’s meta-analysis, the use of colloids was asso-
Table 2 Main Characteristics of the Four Types of Colloid Fluids
Source CommercialIncreasePlasmaVolume
Anticoagulation Half-Life Anaphylaxis(%) Disadvantages
Albumin Human 5% 0.7–1.3 None 16 h 0.5–1.5 Human productRisk infection
25% 4.0–5.0 Short supplyDecrease serum
calcium
Dextran Glucose polymersproduced by bacteria
40-kDa 10% solution70-kDa 6% solution
1.0–1.50.8
Von Willebrand-like syndromeIncrease bleeding timeIncrease fibrinolysisDVT/PE prophylaxis
6–12 h 1.5–3 Implicate in ARFAccumulate SRE
Maximum dose20 mL/kg
Interfere with serumglucose measure
Gelatin Polydisperse peptidesfrom bovine collagen
Broad range 1.0 Minimal (?) �3 h 0.05–10 Modest effectiveness
ModifiedPolygelins
Hetastarch Polymers of glucose(starch) derivedfrom amylopectin
Varies with:Molecular weightDegree substitutionC2/C6 ratio
6% hetastarch10% pentastarch
Small effect 10 h–days 0.1 Adverse effect on renaltransplant
Increase amylaseAffect white cell
chemotaxisMaximum dose 1.5 L/
day1.51.0–1.3
DVT, deep vein thrombosis; PE, pulmonary emboli; ARF, acute renal failure.
The Journal of TRAUMA� Injury, Infection, and Critical Care
S84 May Supplement 2003

ciated with an overall increase in mortality of 5.7% (95%confidence interval [CI], 9.4–20.8%). When trauma trialswere analyzed separately, there was an increase in mortalityof 12.3% (95% CI, 4.6–29.2%) associated with the use ofcolloid fluids. Using a much smaller group of patients,Bisonni et al. reported no statistically significant difference inoverall mortality between colloids and crystalloids. Theyfound, however, a clear trend toward increased mortality inhypovolemic patients (mostly trauma patients), where themortality rate associated with colloids was 17.8% versus7.3% for crystalloids.
The results of these two studies are mostly of historicalinterest because of the limitations of the methodology used.For instance, in the 1989 analysis, the author was the only oneresponsible for searching for the studies, collecting the data,and performing the statistical analysis. To avoid bias, it isstrongly recommended that more than one investigator carryout these tasks independently and then stipulate a manner forresolving the differences in interpretation. This and othermethodologic flaws make the results of these early studiesunreliable.
The subsequent two meta-analyses were published in1998, just months apart from each other.6,33 Both studieswere performed in England, were published in the BritishMedical Journal, and reported very similar results. These twosystematic reviews made front page in many newspapers andhad a major impact on British physicians’ practice, with theuse of albumin solutions in the United Kingdom decreasingby at least 40% by the end of that same year.34
Schierhout and Roberts (1998)The study by Schierhout and Roberts33 was designed to
measure the impact of resuscitation with any colloid (naturaland synthetic) versus crystalloids in critically ill patients. Themethodology used is clearly superior to that of the earlierstudies. Inclusion criteria required random or quasi-randomallocation and excluded neonates. Studies with hypertonicsaline were included. Trial identification was comprehensiveand included some manual searching in addition to directcontact with authors. Two reviewers independently collecteddata and determined eligibility. The studies were categorizedinto trauma, surgery, burns, and others and analyzed sepa-rately. The statistical methods included the funnel plot asym-metry analysis to identify publication or other selection bias.The mathematical analysis is clearly stated and isreproducible.
Of the 48 RCTs identified, 37 were included. The con-clusions, however, were based solely on the 19 studies (in-cluding 1,315 patients) that reported mortality rates. Thepooled relative risk (RR) of death in all categories combinedwas 1.19 (95% CI, 0.98–1.45). For the trauma studies, the RRwas 1.30 (95% CI, 0.95–1.77). These numbers did not reachstatistical significance. However, taking into account that therisk of death in patients given colloids was 24% versus 20%with crystalloids, resuscitation with colloids resulted in an
increase in the absolute risk of dying of 4% (0–8%). Theauthors’ recommendation is that colloids should not be usedoutside RCTs.
The study suffers from the same limitations as mostmeta-analyses included in this review, including low mortal-ity rate (4.7%), inclusion of studies with insufficient infor-mation on interventions and patient characteristics, and amultitude of different resuscitation regimens. The inclusionof hypertonic saline is also a confounding factor. Hypertonicsaline is often administered in conjunction with a colloid(most often with dextrans), making it difficult to classify ascrystalloid or colloid. Still, their results cannot be ignored.
Cochrane Injuries Group Albumin Reviewers (1998)The stated goal of the study by the Cochrane Injuries
Group Albumin Reviewers6 was to quantify the effect onmortality of administering human albumin or plasma proteinfraction for the resuscitation of critically ill patients. Like theprevious study, methodology is clearly described and meetshigh standards. RCTs were identified by meticulous searchincluding manual searching, reviewing meeting proceedings,and directly contacting authors. There was neither languagerestriction nor exclusion of unpublished studies. Allocationconcealment was the main measurement of trial quality, andtwo reviewers independently extracted the data. Studies wereseparated into three categories: hypovolemia (caused by sur-gery or trauma), burns, and hypoalbuminemia. Data analysisand statistical methods are clearly described and included thefunnel plot asymmetry test for published bias.
Thirty studies met the inclusion criteria, comprising1,419 patients and 156 deaths. The pooled RR of death withalbumin or plasma protein fraction administration was 1.68(95% CI, 1.26–2.23). For hypovolemic patients (surgery ortrauma), the RR of death was 1.46 (95% CI, 0.97–2.22). Thepooled difference in the risk of death with albumin was 6%,or 6 additional deaths for 100 patients resuscitated withalbumin.
The major criticisms of this study related not to theanalysis itself but to the limitations of the primary studies,including the fact that it reviews 30 relatively small RCTs.However, in this analysis, the overall risk of death reachedstatistical significance and its results are consistent with theprevious three meta-analyses.
Choi et al. (1999)The objective of the study by Choi et al.7 was to sys-
tematically review the effects of isotonic crystalloids com-pared with colloids in fluid resuscitation of adult critically illpatients. Search criteria and study selection were very similarto the two meta-analyses published 1 year earlier. Choi et al.differed from those studies in that they excluded the studieswith hypertonic saline, and instead of using allocation con-cealment as the main measurement of trial quality, theyevaluated the rigor of several methodologic features such asrandomization, consecutive patient selection, blinding, and
Crystalloids and Colloids in Trauma Resuscitation
Volume 54 • Number 5 S85

documentation of co-interventions. They also explored therelation between study quality and study results and measuredthe effects on mortality and endpoints such as pulmonaryedema. Most importantly, they planned a priori a separateanalysis of trauma patients.
Their results showed no overall difference in mortality,pulmonary edema, or length of stay between crystalloid andcolloid fluid resuscitation, but simply showed a trend towardlower mortality in favor of crystalloids. The authors them-selves point to the limitations of such a study and commentthat small but still clinically important differences may existthat were not detected.
When the trauma subgroup was analyzed, however, theresults demonstrated a statistically significant increase inmortality associated with the use of colloids. In reflectingover these findings, Choi et al. suggested that the results ofthis meta-analysis are best viewed as hypothesis generatingrather than as a justification to ban the use of colloids.
Wilkes and Navickis (2001)The study by Wilkes and Navickis8 is the most recent
and comprehensive of the meta-analyses performed on thissubject. Wilkes and Navickis’ meta-analysis focuses on theuse of albumin versus crystalloids in critically ill patients.Their stated goal is to test the hypothesis that albumin ad-ministration is not associated with increased mortality. Tothis end, they use rigorous and commendable methodology.They used a very comprehensive search strategy to minimizechance of publication and English-language bias. Article se-lection was explicit, with no restriction on clinical indica-tions. Both authors extracted data independently, and therewas a deliberate effort to avoid the inclusion of repeated dataresulting from multiple reporting of the same studies. Theyassessed the quality of the primary studies according to blind-ing, allocation concealment, mortality as an endpoint, andcrossover. A table disclosing the attributes of each study isalso presented.
Of the 415 studies on this subject, 55 met the studyrequirements, including 3,504 randomly assigned patientswith 525 deaths, making it the analysis with the largestnumber of studies and patients to date. Twenty-seven RCTswere performed on surgical or trauma resuscitation, involving1,504 patients. Other RCTs focused on burns, hypoalbumin-emia, high-risk neonates, ascites, acute respiratory distresssyndrome, hyperbilirubinemia, septic and hypovolemicshock, ischemic stroke, vascular leaky syndrome, and ovarianhyperstimulation syndrome. Their pooled relative risk ofdeath was 1.11 (95% CI, 0.95–1.28) for all patients and 1.12(95% CI, 0.85–1.46) for surgery and trauma patients. Theconclusion of the authors is that there is no evidence thatalbumin significantly affects mortality across all trials and forthe subgroup of surgery and trauma patients. Furthermore, thehigher the methodologic quality of the studies included(blinding, mortality as an endpoint, no crossover, and 100 ormore patients), the lower the estimated relative risk, thus
favoring albumin. Their conclusion is that the results of thisstudy “should allay concerns about the safety of albumin.”
Although data extraction and synthesis were excellentlyperformed, the conclusions are intriguing, especially whencompared with previous meta-analyses.6,33 As pointed out inthe accompanying editorial comment by Cook and Guyatt,35
the results of this study are similar to the other meta-analysesbut the interpretations clearly dissimilar. The editorial recog-nizes that the results of the meta-analysis by Wilkes andNavickis show no statistically significant increase in mortal-ity; however, the point estimate indicates an increase inrelative risk of death of more than 10% for surgical andtrauma patients and a confidence interval consistent with arelative overall increase in mortality up to 46%. The editori-al’s conclusion is that “point estimates that suggest harm andconfidence intervals that include important increases in mor-tality cannot allay concerns about the potentially harmfuleffects of albumin.”35 The best evaluation of the results fromthis meta-analysis is that there is a trend toward increasedmortality when albumin is used to resuscitate surgical andtrauma patients, a trend that does not reach statisticalsignificance.
DISCUSSION AND CONCLUSIONSIt is interesting that Wilkes and Navickis reported in their
study that they found 415 potentially relevant RCTs on al-bumin versus crystalloid resuscitation.8 This enormousamount of data on one specific topic explains the fact thatmeta-analyses are being used more frequently to set guide-lines for medical practice.35 However, as is clear in thepresent review, meta-analyses need to be interpreted withcaution and may not always provide the definitive, soundrationale for changing current practices.36
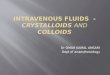
The first limitation of a meta-analysis is that it can onlybe as good as the quality of the individual RCTs it includes.Table 3 summarizes some of the weaknesses of the primaryclinical trials on fluid resuscitation. The observation that
Table 3 Most Frequently Mentioned Limitations of thePrimary RCTs Included in the Meta-analyses Reviewed
Few studies were blindedNo specific criteria for the diagnosis of different conditionsHeterogenous:
Indications for fluid resuscitationInterventions or resuscitation protocolsTypes of fluids usedSubsets of patients (trauma and surgical hypovolemia analyzed
together)Co-interventionsComorbidity
Outdated protocols (�50% studies performed before 1990)End point was not mortalitySmall number of patients includedSmall number of deathsPublication bias (preference for “positive” studies)Crossover
The Journal of TRAUMA� Injury, Infection, and Critical Care
S86 May Supplement 2003

approximately half of the studies were performed more thana decade ago might explain many of the methodologic short-comings. Another important limitation of the primary RCTsis the lack of information on co-interventions such as bloodtransfusion and even surgery. Therefore, the first conclusionof the present review is that there is an urgent need forwell-designed clinical trials on fluid resuscitation.
However, the quality of the primary RCTs is not the onlyfactor limiting the meta-analyses on fluid resuscitation. Themeta-analyses reviewed also have methodologic deficienciesthat have come to the surface in this review. Despite havingsimilar goals, each meta-analysis identified a very differentgroup of RCTs, whereas many large and well-designed RCTswere ignored by most meta-analyses.8 Webb pointed out that20 of 30 RCTs (67%) involving colloid administration wereincluded in one but not in the other colloid meta-analysis.36
The meta-analyses also included very heterogeneous popula-tions for analysis. Even when only trauma was being consid-ered, trauma and elective surgical patients were often pooledand analyzed as one group.8 Another limitation is the strikingfact that similar mathematical results can be interpreted sodifferently. As pointed out by Cook and Guyatt, the results ofthe effect of albumin on mortality were interpreted as alarm-ing in one study, with the author urging to restrict its use,whereas similar results in another study were interpreted asreassuring of the safety of albumin.35 This leads to the secondconclusion of this overview, that meta-analysis should beinterpreted cautiously and, as suggested by Choi et al. inrelation to fluid resuscitation, viewed as hypothesis generat-ing given the limitations in both study design and limitationsof the primary RCTs.7
Finally, all six meta-analyses examined in this overviewdemonstrated a trend toward increased mortality when col-loids were used to resuscitate trauma patients. In fact, themeta-analysis that was designed a priori to investigate theeffect of crystalloids and colloids in trauma resuscitation wasthe only one showing a statistical difference in mortality infavor of crystalloids.7 Therefore, even when all limitationsand nuances of interpretation are considered, one piece ofevidence that comes out is that trauma patients should prob-ably continue to be resuscitated with crystalloids.
REFERENCES1. Velanovich V. Crystalloid versus colloid fluid resuscitation: a meta-
analysis of mortality. Surgery. 1989;105:65–71.2. Bisonni RS, Holtgrave DR, Lawler F, Marley DS. Colloids versus
crystalloids in fluid resuscitation: an analysis of randomizedcontrolled trials. J Fam Pract. 1991;32:387–390.
3. Wade CE, Kramer GC, Grady JJ, Fabian TC, Younes RN. Efficacyof hypertonic 7.5% saline and 6% dextran-70 in treating trauma: ameta-analysis of controlled clinical studies. Surgery. 1997;122:609–616.
4. Wade CE, Grady JJ, Kramer GC, Younes RN, Gehlsen K, HolcroftJW. Individual patient cohort analysis of the efficacy of hypertonicsaline/dextran in patients with traumatic brain injury andhypotension. J Trauma. 1997;42:S61–S65.
5. Schierhout G, Roberts I. Fluid resuscitation with colloid orcrystalloid solutions in critically ill patients: a systematic review ofrandomised trials. BMJ. 1998;316:961–964.
6. Human albumin administration in critically ill patients: systematicreview of randomised controlled trials. Cochrane Injuries GroupAlbumin Reviewers. BMJ. 1998;317:235–240.
7. Choi PT, Yip G, Quinonez LG, Cook DJ. Crystalloids vs. colloids influid resuscitation: a systematic review. Crit Care Med. 1999;27:200–210.
8. Wilkes MM, Navickis RJ. Patient survival after human albuminadministration: a meta-analysis of randomized, controlled trials. AnnIntern Med. 2001;135:149–164.
9. Alderson P, Schierhout G, Roberts I, Bunn F. Colloids versuscrystalloids for fluid resuscitation in critically ill patients. CochraneDatabase Syst Rev. 2000;2:CD000567.
10. Bunn F, Lefebvre C, Li WP, Li L, Roberts I, Schierhout G. Humanalbumin solution for resuscitation and volume expansion in criticallyill patients: the Albumin Reviewers. Cochrane Database Syst Rev.2000;2:CD001208.
11. Bunn F, Roberts I, Tasker R, Akpa E. Hypertonic versus isotoniccrystalloid for fluid resuscitation in critically ill patients. CochraneDatabase Syst Rev. 2000;4:CD002045.
12. Fakhry SM, Alexander J, Smith D, Meyer AA, Peterson HD.Regional and institutional variation in burn care. J Burn CareRehabil. 1995;16:86–90.
13. Needham DM, Detsky AS, Stewart TE. Recent evidence forintravenous fluid choice in patients with severe infection. IntensiveCare Med. 2001;27:609–612.
14. Annane D, Bellissant E. Prognostic value of cortisol response inseptic shock. JAMA. 2000;284:308–309.
15. Rizoli SB, Rotstein OD, Sibbald WJ. The immunological effects ofhypertonic saline. In: Vincent JL, ed. 2002 Yearbook of IntensiveCare and Emergency Medicine. Berlin: Springer-Verlag; 2002:446–453.
16. Rizoli SB, Kapus A, Fan J, Li YH, Marshall JC, Rotstein OD.Immunomodulatory effects of hypertonic resuscitation on thedevelopment of lung inflammation following hemorrhagic shock.J Immunol. 1998;161:6288–6296.
17. American College of Surgeons, Committee on Trauma. In: AdvancedTrauma Life Support Manual. Chicago: American College ofSurgeons; 1997:21–60.
18. Orlinsky M, Shoemaker W, Reis ED, Kerstein MD. Currentcontroversies in shock and resuscitation. Surg Clin North Am. 2001;81:1217–1262.
19. Doyle JA, Davis DP, Hoyt DB. The use of hypertonic saline in thetreatment of traumatic brain injury. J Trauma. 2001;50:367–383.
20. Mazzoni MC, Borgstrom P, Intaglietta M, Arfors KE. Capillarynarrowing in hemorrhagic shock is rectified by hyperosmotic saline-dextran reinfusion. Circ Shock. 1990;31:407–418.
21. Tremblay LN, Rizoli SB, Brenneman FD. Advances in fluidresuscitation of hemorrhagic shock. Can J Surg. 2001;44:172–179.
22. Ernest D, Belzberg AS, Dodek PM. Distribution of normal salineand 5% albumin infusions in septic patients. Crit Care Med. 1999;27:46–50.
23. Lucas CE, Ledgerwood AM, Higgins RF, Weaver DW. Impairedpulmonary function after albumin resuscitation from shock.J Trauma. 1980;20:446–451.
24. Lang K, Boldt J, Suttner S, Haisch G. Colloids versus crystalloidsand tissue oxygen tension in patients undergoing major abdominalsurgery. Anesth Analg. 2001;93:405–409.
25. Groeneveld AB. Albumin and artificial colloids in fluidmanagement: where does the clinical evidence of their utility stand?Crit Care. 2000;4(suppl 2):S16–S20.
26. Vincent JL. Issues in contemporary fluid management. Crit Care.2000;4(suppl 2):S1–S2.
Crystalloids and Colloids in Trauma Resuscitation
Volume 54 • Number 5 S87

27. Sort P, Navasa M, Arroyo V, et al. Effect of intravenous albumin onrenal impairment and mortality in patients with cirrhosis andspontaneous bacterial peritonitis. N Engl J Med. 1999;341:403–409.
28. Vincent JL. Fluid management: the pharmacoeconomic dimension.Crit Care. 2000;4(suppl 2):S33–S35.
29. Yim JM, Vermeulen LC, Erstad BL, Matuszewski KA, Burnett DA,Vlasses PH. Albumin and nonprotein colloid solution use in USacademic health centers. Arch Intern Med. 1995;155:2450–2455.
30. de Jong E, Levi M. Effects of different plasma substitutes on bloodcoagulation: a comparative review. Crit Care Med. 2001;29:1261–1267.
31. Treib J, Baron JF, Grauer MT, Strauss RG. An international view ofhydroxyethyl starches. Intensive Care Med. 1999;25:258–268.
32. Treib J, Haass A, Pindur G, Grauer MT, Wenzel E, Schimrigk K.All medium starches are not the same: influence of the degree of
hydroxyethyl substitution of hydroxyethyl starch on plasma volume,hemorrheologic conditions, and coagulation. Transfusion. 1996;36:450–455.
33. Schierhout G, Roberts I. Fluid resuscitation with colloid orcrystalloid solutions in critically ill patients: a systematic review ofrandomised trials. BMJ. 1998;316:961–964.
34. Roberts I, Edwards P, McLelland B. More on albumin: use ofhuman albumin in UK fell substantially when systematic review waspublished. BMJ. 1999;318:1214–1215.
35. Cook D, Guyatt G. Colloid use for fluid resuscitation: evidence andspin. Ann Intern Med. 2001;135:205–208.
36. Webb AR. The appropriate role of colloids in managing fluidimbalance: a critical review of recent meta-analytic findings. CritCare. 2000;4(suppl 2):S26–S32.
The Journal of TRAUMA� Injury, Infection, and Critical Care
S88 May Supplement 2003