Embed Size (px)
Citation preview

Clinical Neurology and Neurosurgery 124 (2014) 85–89
Cryopreservation versus subcutaneous preservation of autologousbone flaps for Cranioplasty: Comparison of the surgical site infectionand bone resorption rates
Cheng-Hsin Cheng a,b,c, Han-Chung Lee a,c, Chun-Chung Chen c, Der-Yang Cho c,Hung-Lin Lin a,c,*aGraduate Institute of Clinical Medical Science, China Medical University, Taichung, TaiwanbDepartment of Neurosurgery, Tainan Municipal An-Nan Hospital, Tainan, TaiwancDepartment of Neurosurgery, China Medical University Hospital, Taichung, Taiwan
A R T I C L E I N F O
Article history:Received 30 December 2013Received in revised form 18 June 2014Accepted 22 June 2014Available online 1 July 2014
Keywords:Autologous cranioplastySurgical site infectionCryopreservationSubcutaneous pocketDecompressive craniectomy
A B S T R A C T
Objective: Decompressive craniectomy is performed to treat malignant brain hypertension. Surgical siteinfection (SSI) and bone resorption are common complications following cranioplasty, and the storagemethod that minimizes such complication has yet to be identified.Methods: Over a 10-year period, the details of 290 decompressive craniectomy procedures performed atour trauma and stroke center were recorded. Bone flaps from 110 patients were preserved insubcutaneous pockets (SPs), and 180 were preserved via cryopreservation (CP).Results: SSIs occurred in 20 cases (18.2%) in the SP group and 20 cases (11.1%) in the CP group (P = 0.129).After dividing each group according to the traumatic brain injury (TBI) etiologies, we found that in the SPgroup, the SSI rates in the TBI and non-TBI patients were 17.3% and. 20.7% (P = 0.899), respectively, and inthe TBI- and non-TBI CP-group patients, the SSI rates were 11.9% and. 9.7% (P = 0.864), respectively. Theaverage decrease in bone flap thicknesses were 1.14 mm in the SP group (n = 34) and 1.89 mm in the CPgroup (n = 57), and this difference was significant (P = 0.039).Conclusions: In this series, the SSI rates were similar in the SP and CP groups. There was no significantdifference when the patients were grouped by TBI etiology. The incidence of bone flap resorption in theCP group was higher than that in the SP group. However, identifying of the method that yields superiorresults might depend on the individual surgeon's preference and the available equipment.
ã 2014 Elsevier B.V. All rights reserved.
Contents lists available at ScienceDirect
Clinical Neurology and Neurosurgery
journal homepage: www.else vie r .com/locate /c l ine uro
1. Introduction
The use of decompressive craniectomy (DC) for the treatment ofsevere intracranial hypertension following trauma, tumor surgery,or cerebrovascular accident reemerged in the mid-1990s [1–3].When the patient survives the illness, cranioplasty with anautologous bone graft or another reconstructive material is oftenperformed to repair the skull defect. Autologous bone flaps remainthe among the of the most commonly used materials for delayedcranioplasty, and their use was first reported in the 1950s [4].
* Corresponding author at: Department of Neurosurgery, China MedicalUniversity Hospital, 2, Yuh-Der Road, Taichung, Taiwan, Taiwan.Tel.: +886 4 22052121 ext. 5034; fax: +886 4 22344055.
E-mail addresses: [email protected] (C.-H. Cheng),[email protected] (H.-L. Lin).
http://dx.doi.org/10.1016/j.clineuro.2014.06.0290303-8467/ã 2014 Elsevier B.V. All rights reserved.
Autologous bone flaps need to be sterilely preserved for severalweeks or months until the cranioplasty can be performed. Severalstorage methods are available for this purpose, and two popularmethods are currently in use. The first method is preservation in asubcutaneous pocket (SP). Nakajima et al. reported the method ofthe subcutaneous preservation of bone flaps in the thigh [5], andAcikgoz et al. preserved bone flaps between the abdominal fat andthe muscle layers [6]. This method requires additional surgicalprocedures. The second favored method is cryopreservation (CP) ofthe bone flap, typically in a deep freezer. The choice of method isusually based on the surgeon's preference, and only a fewpreviously published papers have discussed whether one methodis superior to the other.
To clarify whether differences in the methods used to storebone flaps influence the incidences of surgical site infection (SSI)and bone flap resorption following cranioplasty, we retrospectivelyreviewed the clinical results obtained from our patients whounderwent DC and delayed cranioplasty within a 10-year period.
86 C.-H. Cheng et al. / Clinical Neurology and Neurosurgery 124 (2014) 85–89
2. Materials and methods
Between May 2001 and May 2010, 430 patients underwentcranioplasty in our trauma and stroke center. Patients withcranioplasties that utilized bone cement, primary cranioplastiesdue to traumatic skull fractures or skull bone tumors, andcraniectomies performed in other hospitals were excluded.Consequently, 290 patients who underwent DC for malignantbrain hypertension and subsequent cranioplasty with autologousbone flaps were enrolled in this study. The standard procedure forDC is to create a large frontotemporoparietal hemicraniectomy(>8 � 8 cm) and dural opening. This technique was performed forTBI, malignant infarction and hypoxic encephalopathy. DCs foraneurysmal subarachnoid hemorrhage were performed withpterional bone flaps that were typically removed for intraoperativebrain swelling. The DCs for intracerebral hemorrhages (ICHs) andtumors depended on the surgical procedures. Some basic patientinformation is presented in Table 1.
For the majority of the study period, the bone flaps wereroutinely stored in our bone bank at a temperature of �70 �C. Of thestudy participants, 180 patients were included in this CP group. Inour standard CP procedure, the soft tissue attached to the bone flapis removed completely, bacterial cultures are performed, the boneflaps are then are immersed in a Betadine solution for at least30 min and a vancomycin solution (500 mg in 500 ml normalsaline) for another 30 min, wrapped in one layer of sterile glove andone layer of a sterile plastic bag, and finally covered with two morelayers of sterile cloth. This package is placed into a deep freezerwithin 30 min. On the day of the cranioplasty, the bone flap isremoved from the bone bank at the beginning of the operation. Theflap is again soaked in a Betadine solution for 30 min and avancomycin solution for 30 min prior to implantation.
From August 2003 to October 2006, our freezer in the bone bankwas not functioning. Therefore, we had to use the SP method topreserve the bone flaps. During this period, 110 bone flaps werestored in SPs. The standard procedure in our institution is to createan SP in the anterolateral thigh. Soft tissue attached to the boneflap is removed completely, and a bacterial culture is performedthen. The SP is created in the subcutaneous layer above themuscular fascia. After carefully ensuring hemostasis, the bone flapis inserted, and one 10 mm drainage tube is left in place. The thighwound was reopened, and the bone flaps were retrieved at thetime of the cranioplasty.
SSI was defined as a surgical wound site that exhibited focalerythema, pus-like discharge or wound rupture. Cases of infectionrequired an additional surgery for bone graft removal.
The microbiologic results are reported in Tables 4 and 5.
Table 1Basic patient data and infection rates.
SP group CP group
(n = 110) (n = 180) P value
Sex (M:F) 79:31 118:62 0.328Age (yr) 48.97 � 17.87 50.45 � 18.80 0.509Initial diagnosis 0.112
TBI 81 (73.6%) 118 (65.6%)Malignant infarction 18 (16.4%) 33 (18.3%)Spontaneous ICH 5 (4.5%) 11 (6.1%)Subarachnoid hemorrhage 4 (3.6%) 13 (7.2%)Tumor edema 0 (0.0%) 5 (2.8%)Hypoxic encephalopathy 2 (1.8%) 0 (0.0%)
Surgical site infection 20 (18.2%) 20 (11.1%) 0.129Duration of bony preservation (days) 61.24 � 60.95 59.82 � 47.71 0.829
x2 test, Yates’ correction x2 test, student’s t-test.CP, cryopreservation; ICH, intracerebral hemorrhage; SP, subcutaneous pocket;TBI, traumatic brain injury.
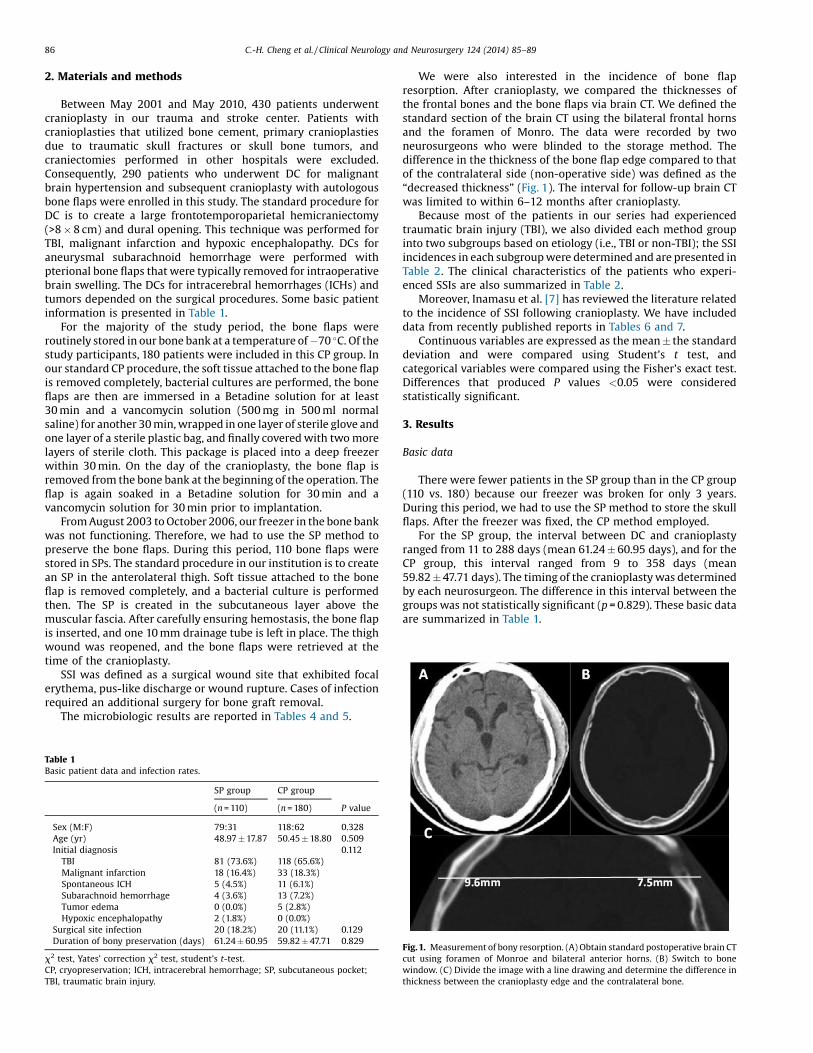
We were also interested in the incidence of bone flapresorption. After cranioplasty, we compared the thicknesses ofthe frontal bones and the bone flaps via brain CT. We defined thestandard section of the brain CT using the bilateral frontal hornsand the foramen of Monro. The data were recorded by twoneurosurgeons who were blinded to the storage method. Thedifference in the thickness of the bone flap edge compared to thatof the contralateral side (non-operative side) was defined as the“decreased thickness” (Fig. 1). The interval for follow-up brain CTwas limited to within 6–12 months after cranioplasty.
Because most of the patients in our series had experiencedtraumatic brain injury (TBI), we also divided each method groupinto two subgroups based on etiology (i.e., TBI or non-TBI); the SSIincidences in each subgroup were determined and are presented inTable 2. The clinical characteristics of the patients who experi-enced SSIs are also summarized in Table 2.
Moreover, Inamasu et al. [7] has reviewed the literature relatedto the incidence of SSI following cranioplasty. We have includeddata from recently published reports in Tables 6 and 7.
Continuous variables are expressed as the mean � the standarddeviation and were compared using Student’s t test, andcategorical variables were compared using the Fisher’s exact test.Differences that produced P values <0.05 were consideredstatistically significant.
3. Results
Basic data
There were fewer patients in the SP group than in the CP group(110 vs. 180) because our freezer was broken for only 3 years.During this period, we had to use the SP method to store the skullflaps. After the freezer was fixed, the CP method employed.
For the SP group, the interval between DC and cranioplastyranged from 11 to 288 days (mean 61.24 � 60.95 days), and for theCP group, this interval ranged from 9 to 358 days (mean59.82 � 47.71 days). The timing of the cranioplasty was determinedby each neurosurgeon. The difference in this interval between thegroups was not statistically significant (p = 0.829). These basic dataare summarized in Table 1.
Fig. 1. Measurement of bony resorption. (A) Obtain standard postoperative brain CTcut using foramen of Monroe and bilateral anterior horns. (B) Switch to bonewindow. (C) Divide the image with a line drawing and determine the difference inthickness between the cranioplasty edge and the contralateral bone.

Table 3Comparison of bony resorption in two groups.
SP group (n = 34) CP group (n = 57) P value
Decreased thickness (mm) 1.14 � 1.20 1.89 � 2.20 0.039*
By student’s t-test.SP, subcutaneous pocket; CP, cryopreservation.
Table 4Summary of 20 SP SSIs.
Thigh infection Cranioplasty infection(n = 8) (n = 12)
Sex (M:F) 8:0 11:1Age (yr) 48.00 � 21.93 46.67 � 15.35Etiology
Traumatic brain injury 6 (75%) 9 (75.0%)Malignant infarction 2 (25%) 2 (16.7%)Subarachnoid hemorrhage 0 (0%) 1 (8.3%)
Infection typeLocal abscess 3 (37.5%) 0 (0%)Ruptured wound 5 (62.5%) 2 (16.7%)EDA 0 (0%) 10 (83.3%)
PathogenNegative culture 5 (62.5%) 0 (0%)Staphylococcus aureus 2 (25.0%) 5 (41.7%)MRSA 0 (0%) 7 (58.3%)Escherichia coli 1 (12.5%) 0 (0%)
Mean (SD) interval (days)DC to SSI 23.75 � 14.93DC to CPL 35.58 � 19.74CPL to SSI
59.83 � 76.81
CPL, cranioplasty; DC, decompressed craniectomy; EDA, epidural abscess; SSI,surgical site infection; SP, subcutaneous pocket; SD, standard deviation; MRSA,methicillin-resistant S. aureus.
Table 2Comparison of surgical site infection incidence by etiology and storage method.
TBI Non-TBI P value
SP groupThigh infection 6/81 (7.4%) 2/29 (6.9%) 1.000Epidural abscess 8/76 (10.5%) 4/27 (14.8%) 0.508Total SSI 14/81 (17.3%) 6/29 (20.7%) 0.899
CP groupInfection 14/118 (11.9%) 6/62 (9.7%) 0.846
YSP, subcutaneous pocket; CP, cryopreservation; TBI, traumatic brain injury.Yates’ correction x2 test.
C.-H. Cheng et al. / Clinical Neurology and Neurosurgery 124 (2014) 85–89 87
Incidence of SSI
The total SSI incidence of all 290 patients was 13.8%. Twentycases of infection occurred in the SP (18.2%). In the CP group,infection occurred in 20 patients (11.1%). The difference betweenthese groups was not statistically significant (p = 0.129). Detaileddata for each infection case are summarized in Tables 4 and 5.
In the SP group, there were two infection sources i.e., the thighwound and the cranioplasty site. Therefore, we separated thepatients into two subgroups for discussion purposes (Table 4).Among these patients, 5 cultures were negative. Of the 8 patientswho developed an SSI in the thigh wound, 2 were infected withStaphylococcus aureus (S. aureus) and one with Escherichia coli (E.coli). In contrast, there were 12 SSIs in the cranioplasty wounds.The most common pathogen (7 cases) was methicillin-resistantStaphylococcus aureus (MRSA), and SA was isolated from the other5 patients. Moreover, there were 5 cases in which the removal ofthe skull bone from the thigh was required due to wound rupture,and 3 cases developed purulent discharges from the thigh wounds.In all but 1 patient, the skull flap was removed from the infectedthigh. In that 1 case, we debrided the wound, and the retrievedskull flap was preserved in the other thigh. Cranioplasty wasperformed two months later without infection in this case. In thecranioplasty wound infection group, 10 epidural abscesses (EDA),and 2 ruptured wounds occurred. The mean interval from the DCto the thigh SSI was 23.75 days. Among the 12 infectedcranioplasties, the mean interval from the DC to the cranioplastywas 35.58 days, and the mean duration from cranioplasty to SSIwas 59.83 days.
In the CP group, 20 cases of infection were recorded (Table 5).The most common pathogen (8 cases) was MRSA. There were 15patients who developed EDA. The other 5 cases were infected dueto ruptured wounds. The mean duration from DC to cranioplasty inthis group was 59.05 days, and the mean interval from cranioplastyto SSI was 38.40 days.
Subgroup analyses
Detailed comparisons of the various subgroups (by TBI etiology,SSI, SP and CP) are presented in Table 2.
The incidence of bone resorption
We also calculated the incidence of bone flap resorption. Forthis calculation, we excluded the infected cases, and limited thefollow-up interval to between six and twelve months. Thus, 91cases were included in this study of bone resorption. There were34 patients in the SP group. The mean follow-up interval to brainCT was 228 days (range from 6 to 12 months). The CP groupincluded 57 patients. The mean follow-up interval was 250 days.The bony resorption data are shown in Table 3.
Literature review
Inamasu et al. [7] reviewed several articles documenting theincidences of SSIs following autologous cranioplasties. All of thesearticles were reports of retrospective studies, and only oneinvolved a comparison of the incidence of SSI between SP andCP groups [7]. A list of the previously published data is shown inTables 6 and 7.
4. Discussion
SP and CP are the two methods that are most commonly usedto store autologous bone flaps [8]. However, the SP method isforbidden by law in some countries. It remains unclear whetherone method is superior to the other because, to our knowledge,prospective randomized trials evaluating the efficacies andsafeties of the two methods have not been conducted. The mostcommon complication of cranioplasty is infection of the bone flapand surrounding tissues, and the incidence of this complicationhas been reported to be as high as 33% [1,9–13]. Thus, storagemethods with lower SSI incidences might be favored by surgeonsTables 4 and 5.
The current retrospective study revealed that the overall SSIincidence in the CP group was lower than that of the SP group(11.11% vs. 18.18%, respectively). However, this difference was notsignificant (P = 0.129). Interestingly, analyses of the SP group dataaccording to the location of the SSI revealed that the incidence ofthigh SSI was 7.27% and that of cranioplasty was 11.65%. Comparedof the cranioplasty SSIs between only the CP and SP groupsrevealed similar rates (11.11% vs. 11.65%, respectively). In ouropinion, the additional surgical wound in the thigh or abdomenand the additional surgical time required for the SP group mighthave been one of the reasons for the higher overall infection rate. A
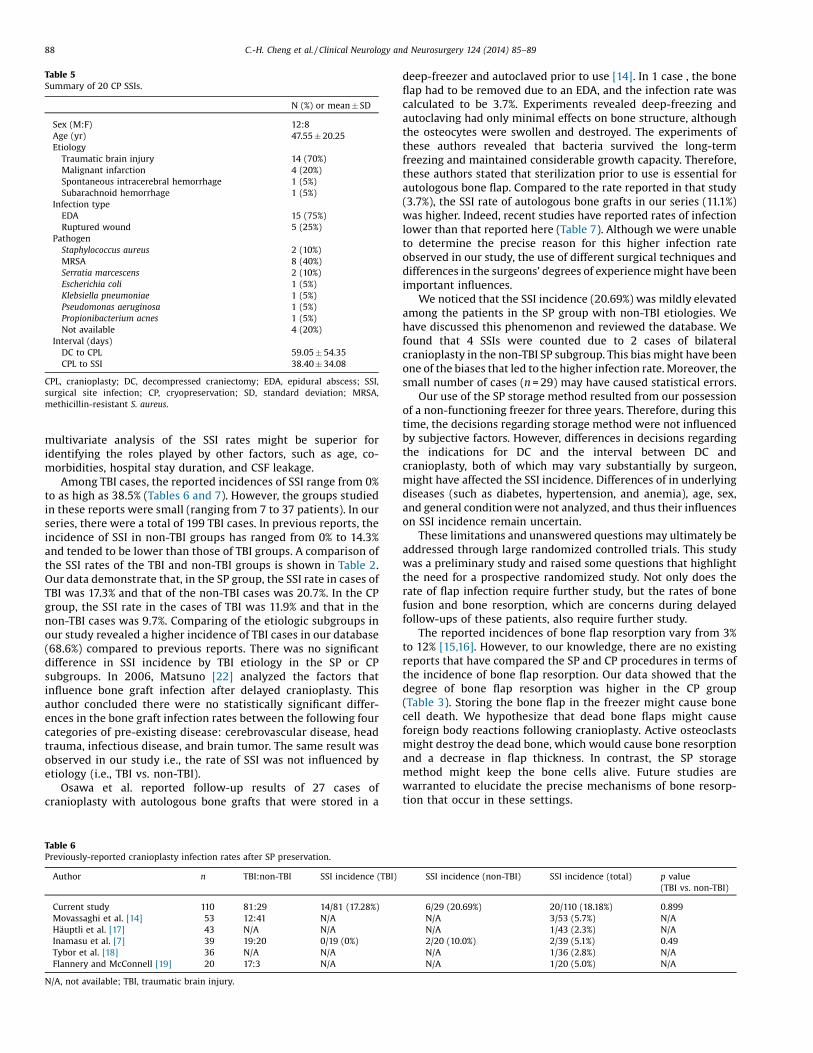
Table 5Summary of 20 CP SSIs.
N (%) or mean � SD
Sex (M:F) 12:8Age (yr) 47.55 � 20.25Etiology
Traumatic brain injury 14 (70%)Malignant infarction 4 (20%)Spontaneous intracerebral hemorrhage 1 (5%)Subarachnoid hemorrhage 1 (5%)
Infection typeEDA 15 (75%)Ruptured wound 5 (25%)
PathogenStaphylococcus aureus 2 (10%)MRSA 8 (40%)Serratia marcescens 2 (10%)Escherichia coli 1 (5%)Klebsiella pneumoniae 1 (5%)Pseudomonas aeruginosa 1 (5%)Propionibacterium acnes 1 (5%)Not available 4 (20%)
Interval (days)DC to CPL 59.05 � 54.35CPL to SSI 38.40 � 34.08
CPL, cranioplasty; DC, decompressed craniectomy; EDA, epidural abscess; SSI,surgical site infection; CP, cryopreservation; SD, standard deviation; MRSA,methicillin-resistant S. aureus.
88 C.-H. Cheng et al. / Clinical Neurology and Neurosurgery 124 (2014) 85–89
multivariate analysis of the SSI rates might be superior foridentifying the roles played by other factors, such as age, co-morbidities, hospital stay duration, and CSF leakage.
Among TBI cases, the reported incidences of SSI range from 0%to as high as 38.5% (Tables 6 and 7). However, the groups studiedin these reports were small (ranging from 7 to 37 patients). In ourseries, there were a total of 199 TBI cases. In previous reports, theincidence of SSI in non-TBI groups has ranged from 0% to 14.3%and tended to be lower than those of TBI groups. A comparison ofthe SSI rates of the TBI and non-TBI groups is shown in Table 2.Our data demonstrate that, in the SP group, the SSI rate in cases ofTBI was 17.3% and that of the non-TBI cases was 20.7%. In the CPgroup, the SSI rate in the cases of TBI was 11.9% and that in thenon-TBI cases was 9.7%. Comparing of the etiologic subgroups inour study revealed a higher incidence of TBI cases in our database(68.6%) compared to previous reports. There was no significantdifference in SSI incidence by TBI etiology in the SP or CPsubgroups. In 2006, Matsuno [22] analyzed the factors thatinfluence bone graft infection after delayed cranioplasty. Thisauthor concluded there were no statistically significant differ-ences in the bone graft infection rates between the following fourcategories of pre-existing disease: cerebrovascular disease, headtrauma, infectious disease, and brain tumor. The same result wasobserved in our study i.e., the rate of SSI was not influenced byetiology (i.e., TBI vs. non-TBI).
Osawa et al. reported follow-up results of 27 cases ofcranioplasty with autologous bone grafts that were stored in a
Table 6Previously-reported cranioplasty infection rates after SP preservation.
Author n TBI:non-TBI SSI incidence (TBI)
Current study 110 81:29 14/81 (17.28%)
Movassaghi et al. [14] 53 12:41 N/A
Häuptli et al. [17] 43 N/A N/A
Inamasu et al. [7] 39 19:20 0/19 (0%)
Tybor et al. [18] 36 N/A N/A
Flannery and McConnell [19] 20 17:3 N/A
N/A, not available; TBI, traumatic brain injury.
deep-freezer and autoclaved prior to use [14]. In 1 case , the boneflap had to be removed due to an EDA, and the infection rate wascalculated to be 3.7%. Experiments revealed deep-freezing andautoclaving had only minimal effects on bone structure, althoughthe osteocytes were swollen and destroyed. The experiments ofthese authors revealed that bacteria survived the long-termfreezing and maintained considerable growth capacity. Therefore,these authors stated that sterilization prior to use is essential forautologous bone flap. Compared to the rate reported in that study(3.7%), the SSI rate of autologous bone grafts in our series (11.1%)was higher. Indeed, recent studies have reported rates of infectionlower than that reported here (Table 7). Although we were unableto determine the precise reason for this higher infection rateobserved in our study, the use of different surgical techniques anddifferences in the surgeons’ degrees of experience might have beenimportant influences.
We noticed that the SSI incidence (20.69%) was mildly elevatedamong the patients in the SP group with non-TBI etiologies. Wehave discussed this phenomenon and reviewed the database. Wefound that 4 SSIs were counted due to 2 cases of bilateralcranioplasty in the non-TBI SP subgroup. This bias might have beenone of the biases that led to the higher infection rate. Moreover, thesmall number of cases (n = 29) may have caused statistical errors.
Our use of the SP storage method resulted from our possessionof a non-functioning freezer for three years. Therefore, during thistime, the decisions regarding storage method were not influencedby subjective factors. However, differences in decisions regardingthe indications for DC and the interval between DC andcranioplasty, both of which may vary substantially by surgeon,might have affected the SSI incidence. Differences of in underlyingdiseases (such as diabetes, hypertension, and anemia), age, sex,and general condition were not analyzed, and thus their influenceson SSI incidence remain uncertain.
These limitations and unanswered questions may ultimately beaddressed through large randomized controlled trials. This studywas a preliminary study and raised some questions that highlightthe need for a prospective randomized study. Not only does therate of flap infection require further study, but the rates of bonefusion and bone resorption, which are concerns during delayedfollow-ups of these patients, also require further study.
The reported incidences of bone flap resorption vary from 3%to 12% [15,16]. However, to our knowledge, there are no existingreports that have compared the SP and CP procedures in terms ofthe incidence of bone flap resorption. Our data showed that thedegree of bone flap resorption was higher in the CP group(Table 3). Storing the bone flap in the freezer might cause bonecell death. We hypothesize that dead bone flaps might causeforeign body reactions following cranioplasty. Active osteoclastsmight destroy the dead bone, which would cause bone resorptionand a decrease in flap thickness. In contrast, the SP storagemethod might keep the bone cells alive. Future studies arewarranted to elucidate the precise mechanisms of bone resorp-tion that occur in these settings.
SSI incidence (non-TBI) SSI incidence (total) p value(TBI vs. non-TBI)
6/29 (20.69%) 20/110 (18.18%) 0.899N/A 3/53 (5.7%) N/AN/A 1/43 (2.3%) N/A2/20 (10.0%) 2/39 (5.1%) 0.49N/A 1/36 (2.8%) N/AN/A 1/20 (5.0%) N/A
Table 7Previously-reported cranioplasty infection rates after CP.
Author n TBI:non-TBI SSI incidence (TBI) SSI incidence (non-TBI) SSI incidence (total) p value(TBI vs. Non-TBI)
Nagayama et al. [20] 195 28:167 4/28 (14.3%) 4/167 (2.4%) 8/195 (4.1%) 0.02Current study 180 118:62 20/118 (11.86%) 6/62 (9.67%) 20/180 (11.1%) 0.846Asano et al. [21] 110 24:86 2/24 (8.3%) 3/86 (3.5%) 5/110 (4.5%) 0.65Matsuno et al. [22] 54 26:28 10/26 (38.5%) 4/28 (14.3%) 14/54 (25.9%) 0.06Prolo et al. [23] 53 37:16 N/A N/A 2/53 (3.8%) N/ACheng et al. [11] 52 33:19 5/33 (15.2%) 2/19 (10.5%) 7/52 (13.5%) 0.64Iwama et al. [24] 49 15:34 1/15 (6.7%) 0/34 (0%) 1/49 (2.0%) 0.30Shimizu et al. [25] 39 15:24 1/15 (6.7%) 0/24 (0%) 1/39 (2.6%) 0.38Inamasu et al. [7] 31 14:17 4/14 (28.6%) 1/17 (5.9%) 5/31 (16.1%) 0.15Osawa et al. [26] 27 7:20 0/7 (0%) 1/20 (5.0%) 1/27 (3.7%) 0.58Ima et al. [27] 131 61:70 8/61 (13.1%) 6/70 (8.6%) 14/131 (10.7%) N/AKim et al. [28] 85 42:43 4/42 (9.5%) 2/43 (4.7%) 6/85 (7%) N/A
N/A, not available; TBI, traumatic brain injury.
C.-H. Cheng et al. / Clinical Neurology and Neurosurgery 124 (2014) 85–89 89
5. Conclusions
SP and CP might both be effective and safe methods for thestorage of bone flaps for cranioplasty, regardless of whether theetiology is TBI or non-TBI. The results of the current retrospectivereview of the experiences of single institution with two autologouscranioplasty flap storage methods indicate that a large randomizedprospective study is warranted to identify the superior method.Additionally, the rates of flap infection, bone fusion and boneresorption following delayed cranioplasty all require further study.
References
[1] Beauchamp KM, Kashuk J, Moore EE, Bolles G, Rabb C, Seinfeld J, et al.Cranioplasty after postinjury decompressive craniectomy: Is timing of theessence? J Trauma 2010;69(2):270–4.
[2] Koh MS, Goh KY, Tung MY, Chan C. Is decompressive craniectomy for acutecerebral infarction of any benefit? Surg Neurol 2000;53:225.
[3] Schwab S, Steiner T, Aschoff A, Schwarz S, Steiner HH, Jansen O, et al. Earlyhemicraniectomy in patients with complete middle cerebral artery infarction.Stroke 1998;29:1888.
[4] Grossman N, Shemesh-Jan HS, Merkin V, Gideon M, Cohen A. Deep-freezepreservation of cranial bones for future cranioplasty: nine years of experience inSoroka University Medical Center. Cell Tissue Bank 2007;8(3)243–6 Epub 2007.
[5] Nakajima T, Someda K, Yamanouchi Y, Matsumura H. Subcutaneouspreservation of free skull bone flap taken out in decompressive craniectomya follow-up study. No Shinkei Geka 1977;5(3):1329–33.
[6] Acikgoz B, Ozcan OE, Erbengi A, BertanV, Ruacan S, Acikgoz HG, et al.Histopathologic and microdensitometric analysis of craniotomy bone flapspreserved between abdominal fat and muscle. Surg Neurol 1986;26:557–61.
[7] Inamasu J, Kuramae T, Nakatsukasa M. Does difference in the storage methodof bone flaps after decompressive craniectomy affect the incidence of surgicalsite infection after cranioplasty? Comparison between subcutaneous pocketand cryopreservation. J Trauma 2010;68(January 1)183–7 discussion 187, 2010.
[8] Zingale A, Albanese V. Cryopreservation of autogeneous bone flap in cranialsurgical practice: what is the future? A grade B and evidence level 4 meta-analytic study. J Neurosurg Sci 2003;47:137–9.
[9] Doerfler A, Engelhorn T, Forsting M. Decompressive craniectomy for earlytherapy and secondary prevention of cerebral infarction. Stroke 200132(813).
[10] Chang V, Hartzfeld P, Langlois M, Mahmood A, Seyfried D. Outcomes of cranialrepair after craniectomy. J Neurosurg 2010;112(May 5):1120–4.
[11] Cheng YK, Weng HH, Yang JT, Lee MH, Wang TC, Chang CN, et al. Factorsaffecting graft infection after cranioplasty. J Clin Neurosci 2008;15:1115–9.
[12] Nagayama K, Yoshikawa G, Somekawa K, Kohno M, Segawa H, Sano K, et al.Cranioplasty using the patient’s autogenous bone preserved by freezing—anexamination of post-operative infection rates. No Shinkei Geka 2002;30:165–9.
[13] Cheng YK, Weng HH, Yang JT, Lee MH, Wang TC, Chang CN, et al. Factorsaffecting graft infection after cranioplasty. J Clin Neurosci 2008;15(10):1115–9.
[14] Movassaghi K, Ver Halen J, Ganchi P, Amin-Hanjani S, Mesa J, Yaremchuk MJ,et al. Cranioplasty with subcutaneously preserved autologous bone grafts.Plast Reconstr Surg 2006;117:202–6.
[15] Gooch MR, Gin GE, Kenning TJ, German JW. Complications of cranioplastyfollowing decompressive craniectomy: analysis of 62 cases. Neurosurg Focus2009;26(June 6):E9.
[16] Honeybul S. Complications of decompressive craniectomy for head injury. JClin Neurosci 2010;4(April 4):430–5.
[17] Hauptli J, Segantini P. New tissue preservation method for bone flaps followingdecompressive craniotomy. Helv Chir Acta 1980;47:121–4.
[18] Tybor K, Fortuniak J, Komu�nski P, Papiez T, Andrzejak S, Jaskólski D, et al.Supplementation of cranial defects by an autologous bone flap stored in theabdominal wall. Neurol Neurochir Pol 2005;39:220–4 discussion 225.
[19] Flannery T, McConnell RS. Cranioplasty why throw the bone flap out? Br JNeurosurg 2001;15:518–20.
[20] Nagayama K, Yoshikawa G, Somekawa K. Cranioplasty using the patient’sautogenous bone preserved by freezing—an examination of post-operativeinfection rates. No Shinkei Geka 2002;30:165–9.
[21] Asano Y, Ryuke Y, Hasuo M, Simosawa S. Cranioplasty using cryopreservedautogenous bone. No To Shinkei 1993;45:1145–50.
[22] Matsuno A, Tanaka H, Iwamuro H, Takanashi S, Miyawaki S, Nakashima M,et al. Analyses of the factors influencing bone graft infection after delayedcranioplasty. Acta Neurochir (Wien) 2006;148:535–40.
[23] Prolo DJ, Burres KP, McLaughlin WT, Christensen AH. Autogenous skullcranioplasty: fresh and preserved (frozen), with consideration of the cellularresponse. Neurosurgery 1979;4:18–29.
[24] Iwama T, Yamada J, Imai S, Shinoda J, Funakoshi T, Sakai N, et al. The use offrozen autogenous bone flaps in delayed cranioplasty revisited. Neurosurgery2003;52:591–6.
[25] Shimizu S, Morikawa A, Kuga Y, Mouri G, Murata T. Cranioplasty usingautogenous bone cryopreserved with dimethylsulfoxide (DMSO). No ShinkeiGeka 2002;30:479–85.
[26] Osawa M, Hara H, Ichinose Y, Koyama T, Kobayashi S, Sugita Y, et al.Cranioplasty with a frozen and autoclaved bone flap. Acta Neurochir (Wien)1990;102:38–41.
[27] Ima SH, Jang DK, Han YM, Kim JT, Chung DS, Park YS, et al. Long-term incidenceand predicting factors of cranioplasty infection after decompressive craniec-tomy. J Korean Neurosurg Soc 2012;52(October 4):396–403.
[28] Kim H, Sung SO, Kim SJ, Kim SR, Park IS, Jo KW. Analysis of the factors affectinggraft infection after cranioplasty. Acta Neurochir (Wien) 2013;155(November11):2171–6.












![Chapter 8 Ovarian Tissue Cryopreservation and ...oncofertility.northwestern.edu/sites/oncofertility/files/legacy_files/uploadedfile...of bone marrow transplant patients [2]. The clinical](https://img.pdfslide.us/doc/110x75/5eba1c3a9509ce3d9165f516/chapter-8-ovarian-tissue-cryopreservation-and-of-bone-marrow-transplant.jpg)
















