CRPS/RSD COMPLEX REGIONAL PAIN SYNDROMEComplex Regional Pain
Syndrome (CRPS), or Reflex Sympathetic Dystrophy (RSD), asit was
previously known, is an excruciating chronic and complex disorder
of theautonomic nervous system (dysautonomia), leading to constant
pain that is recorded asbeing as severe as finger amputation
without anesthetic.It is devastating for patients as is
oftendiagnosed too late for full remission,though it is vital to
never give uphope, people can and do go intoremissions but sadly
[at the moment] itis only a small percentage. However,with more
research being done into thiscomplex condition, our knowledge
ofCRPS is evolving and hopefully, wetoo as patients may benefit
from thatresearch.Currently, CRPS is considered to be acondition
that includes interactions between the immune system, the ANS and
theCentral Nervous System (CNS). There are a huge number of
coexisting symptoms,many of which are incredibly hard to deal with
simply as they are so contrary to bothhow we appear (often looking
healthy) and how at odds they are to normal healthyhuman behaviour.
Pain being caused by sound is one example.Stating that someone
needs to step back, because the allodynic pain of themstanding too
close is making your nerves go crazy, or asking someone to
speakmore quietly or stop rustling a plastic bag all sound very
strange yet these thingscan cause our already excruciating pain to
crescendo and magnifies our symptomsand discomfort.CRPS is a
severely disabling condition characterised by burning pain,
increasedsensitivity to all stimuli, and sensations of pain in
response to normally non-painful stimuli including: light touch, a
breeze, sound, vibration, bright lights andmore. (Birklein et al.,
2000; Wasner et al., 2003).In addition, CRPS is characterized by
motor disturbances such as weakness, tremorand muscle spasms
(Veldman et al., 1993), and sympathetic dysfunction, such aschanges
in vascular tone, temperature changes and increased sweating
(Birkleinet al., 1998; Wasner et al., 2001).Neurological effects of
CRPS, including long term cognitive and moodchanges (Marinus, J. et
al, (2011) in Clinical Features and Pathophysiology ofComplex
Regional Pain Syndrome, The Lancet Neurology, Vol 10, Issue 7,
pp637-648)may be incorrectly treated as existing seaparetly from
the condition, howevernew research will hopefully help raise
awareness. It has been shown thatneuropsychological deficits are
present in 65% of CRPS patients, including deficits inthe executive
functions, for example planning, organising, self-awareness,
self-regulation and initiation of action, word recall lexical
memory and consciousmemory of events declarative memory.Sleep is
massively affected, though this is unsurprising given the CNS and
ANSchanges and of course, constant severe pain (Schwartzman, R.J.,
et al. (2009) in TheNatural History of Complex Regional Pain
Syndrome, Clinical Journal of Pain, Vol. 25,Issue 4, pp.
273-280).Another paper by Schwartzman, R.J. (2012) Systemic
complications of complexregional pain syndrome explains full body
involvement and is a good one to print outif you are faced with
what appears to be extensive spreading of our CRPS or
manyadditional symptoms that cannot be otherwise explained. Robert
Schwartzman is one ofthe leading experts in CRPS so this is
definitely worth a read for both you and yourdoctor.CRPS is
currently viewed as involving interactions between the immune
system,the ANS and the Central Nervous System (Rooij, A.M., (2010)
in Genetic andEpidemiological Aspects of Complex Regional Pain
Syndrome, Doctoral Thesis, LeidenUniversity (ignore chapter 4 as
its now been shown that their are no psychologicaldifferences
between control groups & CRPS groups.In most cases an upper or
lower limbis affected but spreading can anddoes occur to other body
parts, ormany different body parts at thesame time (as with full
body orsystemic CRPS) can be involved(Stanton-Hicks et al., 1995)
includinginternal organs.According to Bruehl and Chung(2006), CRPS
may be understood asa biopsychosocial disorder,
wherebypsychological, behavioral andpathophysiological factors
interact in ahighly complex manner. Most studiesof CRPS have
focused on theperipheral and spinal mechanismsresponsible for the
origin anddevelopment of the syndrome.However, the emerging view is
thatthe peripheral (autonomic andsomatosensory) changes in CRPSmust
be viewed as a manifestation ofchanges in the brain (Jnig
andBaron,2002).To prevent getting CRPS ALWAYS TAKE 1000mg/day
VITAMIN C AFTER ANYSPRAIN OR STRAIN research shows that it can help
to prevent CRPS fromoccurring.Complex Regional Pain Syndrome is a
multifactorial disorder with clinical featuresof neurogenic
inflammation, nociceptive sensitisation (which causes extreme
sensitivityor allodynia), vasomotor dysfunction, and maladaptive
neuroplasticity, generated by anaberrant response to tissue injury.
CRPS is ranked as the highest form of chronic painthat exists in
medical science todayReading 42 on the McGill Pain Scale (RSD/CRPS
is referred to as Causalgia, which isLatin for burning pain). CRPS
is a debilitating disease if not treated promptly andproperly. The
onset of CRPS usually follows a trauma, injury or surgery and
increasingevidence suggests that psychological trauma can cause
CRPS or increase the chanceof its development after an injury by an
estimated eight times.See this post for ways manage and treat CRPS,
while this is an open letter to thosewithout CRPS. Without going
into a full-blown description of the disease let us
initiallyconcentrate on the four main symptoms:Constant chronic
burning pain also throbbing, aching stabbing, sharp,
tingling,and/or crushing in the affected area or areas. Allodynia
is a huge problem withRSD/CRPS (extreme pain response from
innocuous stimuli); even a light breeze cancause pain, let alone
the noise, lights, crowds and vibrations, all having a
debilitatingand life-limiting effect. In CRPS normal inputs such as
touch, stroking and movementare misinterpreted as painful. This
ongoing painful interpretation is a big part of
theproblem.Inflammation is not always present. It can take various
forms, the skin may appearmottled, become easily bruised, have a
shiny, dry, red, and tight look to it. An increasein sweating
usually occurs as well.Spasms in blood vessels and muscles of the
extremities this results in a feeling ofcoldness in the affected
extremity, which feels like ice between the bones or fire
burningthe affected areas. Because of an inability to regulate our
inner thermostats, touchingsomething cool can be excruciating or
cause freezing or burning pains. It depends onhow long the CRPS has
been present, and whether it is typically hot CRPS or coldCRPS.This
is as well as body fatigue, skin rashes, occasional low-grade fever
and sorethroats; swelling (edema), sores, dystonia, and tremors.
The spasms can be confined toone area or be rolling in nature,
moving up and down the leg, arm, or back.Insomnia/Emotional
Disturbance CRPS affects the limbic system of the brain. Thiscauses
many problems that might not initially be linked to a disease like
CRPS, amongthem are depression, insomnia, extreme difficulty
concentrating, and short-term memoryproblems. Cognitive
difficulties similar to fibro-fog are prevalent, simply due to
thesensory overload of constant severe pain.CRPS involves a
malfunction of the nervous system that causes pain (often
diffuse,intense and unrelenting) and related sensory
abnormalities). Dysautonomia meansdysregulation of the autonomic
nervous system (ANS). The ANS controls involuntarybodily synergies
between the sympathetic and parasympathetic nervous
symptoms.Necessary involuntary functions include things like
heartbeat, breathing, digestion, andbody temperature regulation.
Studies have also linked the nervous system tothe immune system,
suggesting a possible correlation between ANS and
autoimmunedisorders.In dysautonomia, the ANS does not respond to
stimuli appropriately, either theparasympathetic or sympathetic
nervous system can be hyporesponsive orhyperresponsive, often
heightened by physiologic and psychologic stress. In those
withmitochondrial dysautonomia, mitochondrial dysfunction is
believed to cause thedysautonomia.Since mitochondria provides a
source of energy for cells, fatigue related diseases arecommon
among mitochondrial myopathies. Nerve cells in the brain and
muscles requiresignificant energy and are depleted with
mitochondrial malfunction.Abnormal regulation of body temperature
in mitochondrial disease patients iscommon, resulting in either a
lower or higher baseline body temperature or a distinctintolerance
to heat or cold. There may also be abnormal blood flow and sweating
inthe affected areas, problems with movement of the muscles and
changes in thestructure of the tissues (trophic changes).Complex
Regional Pain Syndrome involves the skin, nerves, blood vessels,
and bones.The sympathetic nervous system reacts to a stimulus, for
example, an injury, although itcould be as little as a spiders
bite. Blood flow may be affected in reaction to a burn, cut,or
severe temperature changes. To stop you from using an injured limb,
the limb swells.Sometimes inexplicably an abnormal or prolonged
sympathetic reflex begins in a limbas reaction to a trauma.The
sympathetic nerves become overactive and can cause extensive
symptoms that inturn cause debilitating consequences. There can be
many symptoms but the mostcommon one issevere, burning pain. Some
of the other symptoms due to ANSdysfunction include swelling,
temperature change, skin colour change, diminishedmotor function,
and severe sweating. These symptoms usually happen in a limb butcan
occur anywhere in the body, trunkel CRPS in the face or organs are
some extremeexamples. Symptoms may vary with each individual who
has Complex Regional PainSyndrome or CRPS/RSD.Reflex Sympathetic
Dystrophy/RSD is the former name for Complex Regional PainSyndrome
(CRPS). The name of Reflex Sympathetic Dystrophy (RSD) was changed
toComplex Regional Pain Syndrome (CRPS) in 1993 by the
International Association forthe Study of Pain.It has been known by
many names such as algodystrophy or Causalgia or RSD, but isnow
most commonly known as CRPS. The are 2 forms of Complex Regional
PainSyndrome. The only difference between type 1 and type 2 is type
two is easier todiagnose. CRPS type one is formerly known as RSD
and CRPS type two wascausalgia. Complex Regional Pain Syndrome and
Reflex Sympathetic Dystrophy areused synonymously today.Early
TreatmentThe main goal of treatment for CRPS is reversal of the
course, amelioration of suffering,return to work if at all
possible, avoiding surgical procedures such as amputation,
andimprovement in/some quality of life. The key to success is early
diagnosis and earlyassertive treatment. Devastatingly, lack of
proper understanding and proper diagnosisleads to improper
treatment with poor outcome.Read this post on: How to Manage and
Treat Complex Regional Pain Syndrome forCRPS Awareness MonthThere
is a desperate need for future research in thetreatment of
CRPSDelay in diagnosis is a factor in therapeutic failure.
According to Poplawski, et al,treatment, and its results, are
hampered by delay in diagnosis. Early diagnosis (up to 2years) is
essential for achieving the goal of successful treatment results.
Simplemonotherapy with only nerve block, only Gabapentin, or
otherwise, is not sufficient formanagement of CRPS.Treatment should
be multidisciplinary and simultaneous: effective analgesia,
properantidepressants to reduce pain and insomnia; physiotherapy,
nerve blocks, properdiet, when indicated channel blockers, and
anticonvulsant therapy should be appliedearly and simultaneously.
Administration of minimal treatments is apt to fail leading
tolifelong disability and such severe pain that work is often
seldom ever returned to.RSD/CRPS Causes Trauma (physical trauma;
there has also been evidence of psychologicaltrauma causing a surge
of activity in the amygdala and sympathetic nervoussystem, CRPS can
occur in this instance when a secondary physical traumahappens
simultaneously or while this activity is occurring) Soft-tissue
injuries fractures heart disease (caused by inadequate blood
supply) Spinal cord disorders Cerebral lesions Infections Surgery
Repetitive motion disorder recent research suggests that severe
emotional trauma prior to a physicaltrauma, massively increases the
likelihood of CRPS developingIt is not known why these factors
cause CRPS but there are many hypotheses that arethe subject of
research. Severe emotional trauma such as rape or abuse has been
thesuggested to increase the chances of CRPS developing, with so
many patients beingtrauma survivors. Another interesting link made
by a doctor at Bath Hospital wasthe correlation of eating disorders
in the patient histories of those who have developedCRPS.However,
just as each human is unique, each case is unique. CRPS type
two(causalgia) is defined by burning pain, allodynia (innocuous
stimuli causing severepain/an increase in symptoms), and onset
usually occurs after nerve injury but it may bedelayed.The burning
pain is constant and exacerbated by: light touch vibration stress
sounds temperature movement of the limb (though remaining still is
also painful, it can be a strangeart and balance) emotional
disturbance someone standing to close or being very animated
barometric changesAbnormalities in skin temperature and blood flow
mayoccur as well as sudomotor dysfunction. Dystrophicchanges may
occur in the skin, hair or nails. CRPSvertigo and a whole host of
ANS-disfunction symptomsmay be experienced.PainThe pain of CRPS is
constant and characterized, atleast initially by burning. Not in a
descriptive sense butas if your limb or limbs are actually in a
fire. This unrelenting pain is enhanced withevery movement or
stimuls. Allodynia is involved (innocuous stimuli causing
severepain), making socialising even more complicated and painful.
Even a light breeze isenough to make the pain rocket so having
hectic people around massively increasesthe
pain.InflammationSwelling is sometimes localized, but often
relentless and progressive. Swellingintensifies the pain and
promotes stiffness, which can be the beginning of atrophy
anddeformity. Keeping the movement going is crucial! When tissue is
injured or inflamed,excess fluid enters the tissues from damaged
blood vessels within these injuredtissues. If the veins cannot
remove all of this fluid, the part swells (edema). Howeverthis
swelling is usually only temporary, because the tissues heal and
the blood vesselsno longer leak excessively. Swelling is one of the
symptoms of CRPS. Early in thecourse of the disease, this
inflammatory process causes edema. The swelling in CRPSmay exist
far longer than it would take normal tissue to heal because CRPS:
Prevents healing Causes constant inflammation May cause dilation of
the arteries which will cause more fluid to leak, and maycause the
veins to contract, which also prevent the normal removal of
non-protein fluid from tissues. The edema of RSD may last for long
periods of time STIFFNESS, like swelling, is progressive resulting
in less motion of the joints,which again, results in increased
swelling and pain This in turn, can producefurther deformity and
joint changes. DISCOLOURATION indicates circulatory changes that
diminish the nutrition ofthe tissues of the skin, ligaments, bones
and tendons. The result is thin, shinyskin, pencil-like fingers and
changes in ligaments. This further contributes tostiffness and
pain. CRPS in the upper extremities had been classified in
thefollowing five ways, based on the location and intensity of
symptoms.Traditionally, complex regional pain syndrome was seen as
a three-stage disease;however, these stages are increasingly being
seen as theoretical as all the featuresmay not be present and the
speed of progression varies hugely between patients. Somepatients
never actually progress to stage III, while others get to stage III
and lose someof the symptoms of the earlier stages.Early
recognition of the disease, correct diagnosis, and proper
treatment, are allessential in keeping RSD from becoming a chronic,
life-long condition. Treatment mustbegin within months of onset,
ideally within three months.The following excerpt is taken from the
America RSD Hope website:1) The CONSTANT PAIN can be described as a
burning pain. It feels as if a red hotpoker were inserted into the
affected area. it is also described as throbbing, achingstabbing,
sharp, tingling, and/or crushing in the effected area; this is not
always the siteof the trauma. The effected area is usually hot or
cold to the touch. The pain will bemore severe than anticipated for
the type of injury sustained. This is a hallmark of thedisease.
Allodynia is typically present as well. Allodynia is an extreme
sensitivity totouch, sound, vibration, barometric pressure changes,
loud noises, wind/breeze,temperature, clothing, and even the gentle
touch of a loved one. This makes itincreasingly difficult on the
spouses, children, and other family members; as their softesttouch
can now cause pain instead of comfort. If the patient has not been
properlydiagnosed yet and these sensations not properly explained,
these symptoms can causeextreme duress and confusion to all
involved. For more on What Does CRPS FeelLike click here.2)
INFLAMMATION is not always present in the same form but it can take
variousforms; the skin may appear mottled, become easily bruised,
bleeding in the skin, smallred dots, have a shiny, dry, red, and
tight look to it. In addition; increase in sweatingusually occurs
as well as swelling in and around the joints (shoulders, knees,
wrists). Insome patients a lack of sweating may occur, and some
even go back and forth betweenthe two.3) The SPASMS result in a
feeling of coldness in the effected extremity as well as
bodyfatigue, skin rashes, low-grade fever, swelling (edema), sores,
dystonia, and tremors.The spasms can be confined to one area or be
rolling in nature; moving up and downthe leg, arm, or back. They
can involve not only muscles but also blood vessels.4) The fourth
part of this square is INSOMNIA and EMOTIONAL DISTURBANCE.CRPS
affects the limbic system of the brain. Doctor Hooshang Hooshmand
described itwell: The fact that the sympathetic sensory nerve
fibers carrying the sympathetic painand impulse up to the brain
terminate in the part of the brain called limbic system. Thislimbic
(marginal) system which is positioned between the old brain
(brainstem) and thenew brain (cerebral hemispheres) is mainly
located over the temporal and frontal lobesof the brain. This
causes many problems that might not initially be linked to a
diseaselike CRPS; chief among them are depression, insomnia and
short-term memoryproblems but also includes agitation,
irritability, and possibly even poor judgement.CRPS can cause
Depression, NOT the other way around. Read more here: RSD Hope What
is CRPS?Here are some of the many symptoms of CRPS/RSD: Skin
temperature, skin colour changes Pain caused by innocuous stimuli,
for instance sound, vibration, light touch, evensomeone in the room
can increase pain. Allodynia is pain from thing that youwould never
expect to cause pain, while hyperalgesia is an exaggerated
painresponse, so far more pain than should result from a stimulus.
Tremors, shakes, spasms and muscle contractions that can cause
unusualmovements and postures (dystonia) Temperature changes and
inability to regulate temperature Changes in hair/nails/skin
Sweating changes, sometimes sweating varies from one side of the
body to theother Fluid build-up causing swelling (edema) Lower bone
density as they become more porous (osteoporosis) Avoiding using
the part of the body which hurts, which then causes
additionalproblems like the muscles starting to waste away through
lack of use (atrophy) Central Nervous System (CNS) dysfunction and
hyperactivity.The CNS is made up of the brain and spinal cord which
use the information from thewider spread ANS to control and
co-ordinate what we do. The CNS can do strangethings when its
dependent on a faulty ANS for its information. As the
conditiondevelops the pain becomes continuous, it is truly
relentless. There are brief periodswhere it may not be as severe,
but considering that the pain experienced is off the scaleof
previous personal experience for most patients, the lesser pain
moments are stillexcruciating by normal standards. No wonder the
natural response is to stop usingwhichever part of our body is
affected.Read more at: What is CRPS? | Elle and the Auto
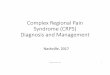
Gnome.Complex regional pain syndrome in adultsIntegrative
conceptual model of CRPS. In the affected limb after trauma,
enhanced anti-dromic secretion of neuropeptides from sensory nerve
endings [77], enhanced releaseof immune mediators from various
cells [22] and surface binding autoantibodies [54]may contribute
both to change regional sensory nerve function, and elicit
sensoryaxonal degeneration; resulting functional and structural
changes may then elicit furtherchanges creating a vicious cycle
[70]. Some of these changes may be enhanced bytissue ischaemia
([59], data not shown). The long-lasting response of patients with
long-standing CRPS to thelikely centrally actingNMDA-receptor
antagonist ketamine [47,48] also suggests that, at least in chronic
cases these regional factors do not sufficientlyactivate
nociceptors (otherwise pain intensity would return as the ketamine
plasma leveldeclines); these factor may rather create a low-level
activation of sensory nervessustaining central sensitization in the
dorsal horn (see main text). Certain methods ofbrain training, and
spinal cord stimulator treatment can, through yet unknownmechanisms
alter regional factors in the affected limb, as evidenced by their
reportedefficacy to reduce limb swelling [13, 66, 92]. The model
does not account for thepresumed role of sympathetic dysfunction in
some patients.CRPS is a sympathetically mediated disorderSweating
and colour/temperature differences between CRPS-affected and
unaffectedlimbs are in part mediated by a complex sympathetic
dysregulation. There is a low,rather than high, centrally mediated
sympathetic outflow to cutaneous vasoconstrictorsin the
CRPS-affected extremity, which likely contributes to produce red
and warmextremities [35]; other vasomotor signs such as cold
temperature and bluishdyscolouration may be caused by reactive
adrenoceptor up-regulation and/orsupersensitivity, rather than by a
dysregulation of the sympathetic outflow [36, 37].Vaso- and
sudomotor signs often diminish with time. The permanent cold
temperaturein some cases of late CRPS may be due to endothelial
rather than sympatheticdysfunction [38]. Evans [39] had introduced
the, now superseded term RSD to indicatethat regional autonomic
dysregulation actually causes the patients pain. Hannington-Kiff
[40] later suggested that agents that deplete the limb autonomic
nerve endings ofnoradrenaline, such as regional guanethidine
should, therefore, be effective.Unfortunately, all four RCTs
conducted to assess this treatment have been negative[19]. Given
the experience shared by many clinicians that this method, termed
i.v.regional sympathetic block (IVRSB), actually does reduce pain
in some patients, onewonders whether it is perhaps the application
of tourniquet that conveys that effect.Indeed, IVRSB with saline
may be more effective than IVRSB with guanethidine [41].Local
anaesthetic application to the sympathetic ganglia (i.e. stellate
or lumbarsympathetic blocks) can relieve pain for the short term in
selected patients [42], butrepeat application does not prolong that
effect [43]. Sympathetically maintained pain(SMP), that is pain
that can be reduced by sympathetic blockade, although common
inearly CRPS, is rare in long-standing CRPS [44]. While there
clearly is autonomicdysregulation [45], both the discussed rarity
of SMP in those clinically particularlyproblematic long-standing
cases, and the emergence of novel aetiological conceptshave
contributed to prompting CRPS experts to de-emphasize the
importance of theconcept of sympathetic dysfunction for advancing
patient treatment.Central sensitization is the driving factor for
CRPSCentral sensitization is the molecular process that corresponds
to the clinicalobservation that after a period of intense or
repeated noxious stimulation (a noxiousstimulus actually or
potentially causes tissue damage), innocuous (non-noxious)
stimulibecome painful and remain painful (for a while at least)
even if the initial noxiousstimulation has subsided. This mechanism
is important in most chronic pain [46]. SinceN-methyl D-aspartate
(NMDA) receptors play a critical role in central sensitization,
therecent observation in two RCTs that low-dose i.v. ketamine (an
NMDA antagonist) candramatically reduce CRPS pain, indicates an
important role for such centralsensitization [47, 48]. There is
currently no RCT evidence for high-dose ketamine comaunder
intensive care conditions, which has sometimes been discussed in
the media[49]. In the two published low-dose RCTs, ketamine
strongly reduced average painintensity for several weeks
independently of the CRPS disease duration, but withoutimproving
function. It is uncertain how these research findings will
translate into clinicalpractice. Side effects from repeated
ketamine infusions are poorly understood, andsome experts have
expressed concern about potential neurotoxicity [50].
Currentprotocols for ketamine treatment are expensive and
cumbersome. In the publishedprotocols, either a 5day hospital
inpatient stay, or 10 consecutive working-dayoutpatient treatments
are required to achieve pain relief lasting several weeks.Recently,
a small pilot trial suggested efficacy of i.v. magnesium which,
similar toketamine, may work to reduce central sensitization
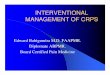
[51].Budapest diagnostic criteria (AD must apply). Note that it is
possible to distinguishbetween CRPS-1 (without damage to major
nerves) and CRPS-2 [associated with (yetnot causing) damage to a
major nerve, a very rare presentation], but there is currentlyno
RCT-derived evidence that this distinction has any consequence for
treatment. a Thereflected understanding of allodynia as painful
sensation to a number of normally non-painful stimuli is under
review by the IASP taxonomy group. Some experts suggest thatthe
term allodynia should be reserved only for brush-stroke evoked pain
(dynamicmechanical allodynia). bHyperalgesia is exaggerated pain to
a painful stimulus such asa pinprick. cFor example, raised systemic
inflammatory markers are not associated withCRPS, even in the
initial inflammatory phase; such a finding of raised markers
wouldlead to a search for an alternative or concomitant cause.
Abnormal nerve conductionstudies do not exclude CRPS, but the
primary cause of the observed abnormality mustbe clarified: CRPS,
by definition is always secondary, its presence cannot explain
majornerve damage. Figure adapted from Ref. [4].via Complex
regional pain syndrome in adults.What Body Parts are Involved?CRPS
is a multi-symptom condition typically affecting one, two, or
sometimes even allfour extremities. It can also be in the face,
shoulders, back, eyes, and other areas of thebody as well. CRPS is
an involvement of nerves, skin, muscles, blood vessels
(causingconstriction, spasms, and pain) as well as bones. This is
from the Orthopod website:Sympathetic nerves are responsible for
conducting sensation signals to the spinal cordfrom the body. They
also regulate blood vessels and sweat glands. Sympathetic
gangliaare collections of these nerves near the spinal cord. They
contain approximately20,000-30,000 nerve cell bodies. CRPS is felt
to occur as the result of stimulation ofsensory nerve fibers. Those
regions of the body rich in nerve endings such as thefingers,
hands, wrist, and ankles are most commonly affected.When a nerve is
excited, its endings release chemicals. These chemicals
causevasodilation (opening of the blood vessels). This allows fluid
to leak from the bloodvessel into the surrounding tissue. The
result is inflammation or swelling leading to morestimulation of
the sensory nerve fibers. This lowers the pain threshold. This
entireprocess is called neurogenic inflammation.This explains the
swelling, redness, and warmth of the skin in the involved area
initially.It also explains the increased sensitivity to pain. As
the symptoms go untreated, theaffected area can become cool, have
hair loss, and have brittle or cracked nails. Muscleatrophy or
shrinkage, loss of bone density (calcium), contracture, swelling,
and limitedrange of motion in joints can also occur in the affected
limb. These are in part caused bydecreased blood supply to the
affected tissues as the condition progresses.(Source: A Patients
Guide to Pain Management: Complex Regional Pain Syndrome)Does
RSD/CRPS Spread?It may spread from one part of the body to another
regardless of where the originalinjury occurred. RSD/CRPS can
spread in up to 70% of the cases. However, in a smallnumber of
cases (8% or less) it can become Systemic or body-wide. CRPS
usuallyspreads up/down the same limb, or to the opposite limb but
in an increasing number ofcases it spreads to other areas of the
body.The pain of CRPS is continuous and it is widely recognised
that it can beheightened by emotional or physical stress. Limbic
system involvement suggests apropensity for trouble with sleeping,
mood, appetite and sexual desire; in a study of 824patients with
CRPS, 92% reported insomnia, 78% irritability, agitation, anxiety,
73%depression and 48% had poor memory and felt they lacked
concentration.Patients are frequently classified into two groups
based upon temperature, whether theyare predominately warm or hot
CRPS, or cold CRPS. The vast majority,approximately 70% of
patients, have the hot type, which is said to be an acute form
ofCRPS. Cold CRPS is said to be indicative of a more chronic and
long-term CRPS,affecting 30% of long-term CRPS patients.With poorer
McGill Pain Questionnaire (MPQ) scores, increased central nervous
systeminvolvement and a higher prevalence of dystonia, this new
stage (though the idea ofstages of RSD/CRPS has been abandoned by
pain specialists) of the CRPS can bemanaged but is obviously.If you
have developed Cold CRPS, trying to maintain mobility and keep
movement inthe area is vital. Microcirculation is compromised,
though little is known as with otherCRPS cases how to treat it.
Obviously, heat therapy comes into its own here.Prognosis is not
favourable for cold CRPS patients, longitudinal studies suggest
thesepatients have poorer clinical pain outcomes and show
persistent signs of centralsensitisation correlating with disease
progression.Previously it was considered that CRPS had three
stages; it is now believed thatpatients with CRPS do not progress
through these stages sequentially. These stagesmay not be
time-constrained, and could possibly be event-related, such as
ground-levelfalls or re-injuries in previous areas. It is important
to remember thatoftenthe sympathetic nervous system is involved
with CRPS, and the autonomicnervous system can go haywire and cause
a wide variety of strange symptoms.CRPS FrustrationComplex Regional
Pain Syndrome is frequently dismissed by health professionals
formany reasons including: They dont understand the diagnosis
and/or they are not familiar with thedisorder. They understand the
diagnosis but lack experience in how to treat it properly. Many
think that the client is pretending to be ill or exaggerating their
pain. CRPS is thought to be hopeless and there isno cure (have
hope!). CRPS is purely psychological and that it is nota medical
condition, i.e. Its all in your head,which is clearly a myth. Many
people who work within the health caresystem dread accepting a
client with CRPSbecause they know that effective treatmentrequires
an ongoing, almost daily assessment ofthe condition to develop the
proper regimen. It isfar too time consuming for most clinics
toadequately care for the patient. Generally,doctors like to cure
not manage chronic illness. Due to the nature of RSD/CRPS, the
conditioncan quickly change for better or worse forreasons that are
not fully understood. Therefore it is necessary to scheduleevenly
spaced treatment sessions in order to benefit, which is often not
possiblefor many patients who now are unable to work. The health
care provider must address the plan of care very carefully once
thediagnosis is made and must thoroughly customise therapy for each
ComplexRegional Pain Syndrome patient.Many patients suffer
needlessly through a lack of understanding from their
GP/doctor,resulting in insufficient pain management that causes
additional stress on an alreadyover-taxed body. All individual
characteristics (psychological, social, physiological) mustbe taken
into account during therapy.Communication between the family
members, health professionals, and the patientmust be clear,
on-going and well established. It is common for the patient to have
failedin a previous program if a positive, creative, caring
relationship was not . If either thepatient or the therapist senses
a communication problem, it is far better to acknowledgethat
another clinician may be of greater benefit to the patients
progress.How is Complex Regional Pain Syndrome treated?Everyone
with CRPS needs good medical support and treatment. While this is
notalways possible, especially if you live in a rural or remote
area, this website can helpguide you in things that help improve
your pain and function. Because pain involves thewhole person, to
get the best outcomes treatments and management usually require
acombination of some of the following approaches: Pacing (also see
Pain Management) Relaxation techniques; yoga; breathing; Tai Chi;
Chi Kung etc. Mindfulness based relaxation Gentle movement and
mobilisation techniques Coping and Managing your pain Use of pain
medicines and medical procedures Complimentary medicine (see
Pain-Relief and Coping for Severe Pain)The primary task is to
eliminate or treat all possible causes. If there is no known
cause,or if with the removal of the cause, the symptoms do not
satisfactorily disappear, thenthere are only the symptoms of
RSD/CRPS to be treated. Successful treatment ofRSD/CRPS is
dependent on: Early diagnosis. If diagnosed early, the prognosis is
very good. Begin treatment of the underlying cause, if there is
one. If not, then focus on thetreatment of the RSD/CRPS process.
The key approach is to provide adequate pain relief in order to
undertakerehabilitation with the primary aim of restoring function
as early as possible. Also,with the recent research in
neuroscience, it is vital to control pain so that painpathways in
the brain do not become maladaptively rewired, making recoveryeven
more difficult.See How to Manage and Treat Complex Regional Pain
Syndrome.What Does CRPS/RSD Feel Like?CRPS pain can be anywhere in
the body where there are nerves. Most commonly in thefour
extremities but some people have it in other areas such as eyes,
ears, back, face,etc. Here Keith Orsini answers the question: what
does it feel like?Well, if you had it in your hand, imagine your
hand was doused in gasoline, lit on fire,and then kept that way 24
hours a day, 7 days a week, and you knew it was never goingto be
put out. Now imagine it both hands, arms, legs, feet; well, you get
the picture. Isometimes sit there and am amazed that no one else
can see the flames shooting off ofmy body. The second component to
CRPS is what is called Allodynia. Allodynia isan extreme
sensitivity to touch, sound, and/or vibration. Imagine that same
hand nowhas the skin all burned off and is completely raw. Next,
rub some salt on top of it andthen rub some sandpaper on top of
that! THAT is allodynia! Picture getting prettyvivid? Now, because
of the allodynia, any normal touch will cause pain; your
clothing,the gentle touch of a loved one, a sheet, rain, shower,
razor, hairbrush, shoe, someonebrushing by you in a crowded
hallway, etc. In addition, sounds, especially loud or deepsounds
and vibrations, will also cause pain; a school bell, thunder, loud
music, crowds,singing, yelling, sirens, traffic, kids screaming,
loud wind, even the sound in a typicalmovie theatre. This is what
allodynia is all about. Imagine going through your daily lifewhere
everything that you touch, or that touches you, where most every
noise aroundyou from a passing car or plane to children playing,
causes you pain. In addition to theenormous pain you are already
experiencing from the CRPS itself. Imagine living withthat pain and
allodynia 24 hours a day, every day, for months, years, and longer.
Thereare many other symptoms which you can read about in our CRPS
SYMPTOMS sectionbut these are the two main ones that most patients
talk about the most. ~ Keith Orsinivia What Does CRPS Feel Like?
American RSDHope.Fibromyalgia and CRPSAlthough many CRPS patients
are later diagnosed with Fibromyalgia, the two arefrequently
confused but remain vastly different in terms of day-to-day living
and severityof symptoms. Some fibromyalgia patients are completely
debilitated but even they canhave moments of reduced pain. CRPS is
constantly at a severe level and personally, Ifeel the difference
of character between the two pains also confirms the
differencesbetween the two pain conditions. There may be a
continuum, with dysautonomia andcentral sensitization being present
in both but there are clearly distinct symptoms thatare present in
CRPS that are absent in fibromyalgia.What You Can Do For Your
CRPS:Pain educationTo manage pain and gain more control over your
lifeand symptoms in spite of CRPS, you must understandhow pain
behaves. Visit the Pain Management page formore info and watch a
great video with the amazingProf, Lorimer Moseley, who banishes the
jargon andoffers a description of the pain process that even
themost unscientific of pain princesses can understand.How to
Manage and Treat Complex RegionalPain SyndromeMobilisation &
massage techniquesFor pain relief, to reduce stiffness, increase
circulation, ease movement and gain agood sense of your body; all
important in the recovery process but also if you need tospend a
long time in bed or resting due to high pain levels. see
Pain-Relief and Copingfor Severe Pain.Specific exercisesTo mobilise
tight & stiff body regions, to develop normal control of
movement; graduallyprogressing from just a couple of repetitions to
ten (see a physiotherapist for guidanceon how to strengthen disused
muscles).General exerciseTo progressively build up your tolerance
and confidence for daily activity and yourchosen exercises; always
keep within your limitations, increasing your timed activityvery
gradually. Read this blog post on Therapeutic Yoga with a
restorative yogasequence, which can be very healing and gentle
enough to not cause a flare-up ofsymptoms; swimming/aqua physio is
immensely helpful with RSD/CRPS.Graded exposure & pacingThere
are often particular activities that are challenging, painful and
sometimes avoidedfor fear of causing damage or harm. With new
knowledge of pain and confidence tomove you can gradually re-engage
with some of these activities. Pacing means that youset a baseline
and work towards your goals, see the Pain Management page for
moreinformation.Brain-Focused StrategiesModern neuroscience has
delivered us new ways of approaching pain though ourunderstanding
of the brain when we are in pain, in particular chronic or
persisting pain.We can target the adaptations and changes that have
been found via particular types ofsensory and motor training. For
example, the graded motor imagery program and tactilediscrimination
training.Mindfulness & focused attention trainingTo gain
control over your attention and emotional regulation; there has
been a spotlightplaced upon these techniques in recent years due to
their effectiveness in stress andpain. We teach and practice
mindfulness and other cognitive methods as a way ofreducing the
emotional aspects of pain, to directly tackle stress and to
optimiseperformance. Click here for an example of one of the
mindfulness techniques.Imagery & visualisationMotor imagery is
used as part of the graded motor imagery programme and as a
standalone brain focused training. When we think about movement,
the same areas of thebrain are active as when we actually move.
Using this physiology within the corticalnetwork allows us to
re-train normal movement (how the brain plans and then
executesprecise and well controlled actions) at the early stages of
rehabilitation. Visualisation isa way of changing the body
physiology in a positive manner thereby benefiting thephysical
self, mood and creating a positive context for rehabilitation.When
it All Gets Too MuchThe suicide rate among RSD/CRPS sufferers is
extremely high due to the intensity ofthe never-ending pain, sleep
deprivation, frustration, social isolation, misunderstanding,and
lack of support from medical professionals, family and friends. If
you are a patientsuffering from depression and contemplating
suicide, please, please get help SuicidePrevention / Depression
Support: UK: Samaritans (National and local): 08457 90 90 90 or
[email protected] UK: Painline: 0845 603 1593 US: Hopeline (Suicide
Prevention): 1-800-SUICIDE (1-800-784-2433) US: Suicide Hotline:
1-800-273-Talk (1-800-8255) US: Directory of Local Helplines /
CentersFeeling suicidal is not a character defect, and it doesnt
mean that you are crazy, orweak, or flawed. It only means that you
have more pain than you can cope with rightnow. Please read this
fantastic guide before you do anything that will leave
everyonewondering if there was something that they could do. No
matter how you feel in thismoment, and no matter how impossible it
may seem, things can and do improve.Life with severe, constant pain
is hard, very hard. There will be times when what isalready
excruciating flares up to being beyond comprehension in terms of
pain (I knowIm often astonished at just how limitless the variety
and intensity of pain can be), and itis these times where you must
take extra special care of yourself and mind.Read Techniques to
Help Depression for help with depression. More will be
addedregularly.Know that youre not alone; the human mind can
sometimes be your own worst enemy,especially when bottling up how
youre feeling both physically and mentally. Considerjoining a
community who knows how youre feeling and speak with members who
havefirst-hand experience with depression stemming from
RSD/CRPS.