Embed Size (px)
Citation preview
Journal of Affective Disorders 140 (2012) 215–221
Contents lists available at SciVerse ScienceDirect
Journal of Affective Disorders
j ourna l homepage: www.e lsev ie r .com/ locate / jad
Review
Cross validation with the mood disorder questionnaire (MDQ) of aninstrument for the detection of hypomania in Brazil: The 32 item hypomaniasymptom check-list, first Revision (HCI-32-R1)
Inês Alice Teixeira Leão a,b,⁎, José Alberto Del Porto a
a Federal University of São Paulo, Brazilb Military Hospital at Belo Horizonte, Minas Gerais, Brazil
a r t i c l e i n f o
⁎ Corresponding author at: Federal University of SãE-mail address: [email protected] (I.A.T. Leão
0165-0327/$ – see front matter © 2011 Elsevier B.V. Adoi:10.1016/j.jad.2011.12.033
a b s t r a c t
Article history:Received 5 October 2011Received in revised form 27 November 2011Accepted 14 December 2011Available online 28 January 2012
Background: Bipolar disorders are frequently diagnosed and treated as unipolar depressioninitially and accurate diagnosis is often delayed by 8 to 10 years. It has been demonstratedthat the bipolar spectrum disorders are associated with notable disability and that the currentdiagnostic gold standard, the Structured Clinical Interview for DSM-IV (SCID) is not sufficientlysensitive to the diagnosis of hypomania or subthreshold manic states. There is a need for betterand simpler ways to identify these conditions.Methods: Hirschfeld et al. (2000) developed and tested a self-report scale for bipolar disorder:the Mood Disorder Questionnaire (MDQ). Recently, another scale has been developed by Angstto assess hypomanic symptoms and to increase the detection of suspected and of manifest, butundertreated, cases of bipolar disorders.In this Brazilian study, 200 patients with the putative diagnosis of “depression” were inter-viewed using the Structured Clinical Interview for DSM-IV, Axis I Disorders — ClinicianVersion (SCID-CV; First et al., 1997), as modified by Benazzi and Akiskal (2003) to increasethe sensitivity to BP II disorders. Before the interview patients were screened by bothHCI-32-R1 and MDQ and asked to complete them.Results: The HCI-32-R1 showed a sensitivity of 79.8% and a specificity of 60.5% for the cut-off of14. A sensitivity of 68.1% and a specificity of 63% were obtained for the Mood DisorderQuestionnaire for the cut-off of 7.Limitations: Although not showing a good specificity, the MDQ seems to be a useful instrumentfor the screening phase, in which it is important that “cases” are recognized. The HCI-32-R1
does not distinguish between BP I and BP II disorders. The sample size of patients should beincreased in further studies.Conclusions: The HCI-32-R1 demonstrated two main factors identified as “active-elated” hypo-mania and “risk-taking/irritable” hypomania and showed to be a sensitive instrument forhypomanic symptoms. It is a simple and easy-to-use tool for the self-assessment of hypomanicsymptoms and may be a valuable supplement to the clinician's interview.The Mood Disorder Questionnaire is a useful screening instrument for bipolar I, bipolar IIdisorders and other manifestations of bipolar spectrum. As such, this scale might increasethe detection of under-treated cases of bipolar disorders. Further studies are needed to verifythe accuracy of these tools in non-psychiatric settings and in the general population.
© 2011 Elsevier B.V. All rights reserved.
Keywords:QuestionnaireHypomaniaBipolarDepressionValidation
o Paulo, Brazil. Tel.: + 55 31 3222 8207; fax: +55 31 3221 4799.).
ll rights reserved.
216 I.A.T. Leão, J.A. Del Porto / Journal of Affective Disorders 140 (2012) 215–221
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2162. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 216
2.1. Design . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2162.2. Subjects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2162.3. Instruments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2172.4. Procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 217
3. Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2173.1. Description of sample . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2173.2. Accuracy and reliability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2183.3. Factorial analysis or internal structure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 218
4. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 219Role of funding source . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220Conflict of interests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220
1. Introduction
The bipolar spectrum is an important area of recent re-search. Labeled type II and NOS in DSM-IV, recent studieshave begun to elucidate the nature of these conditions, suchas the depressive mixed state (Akiskal and Benazzi, 2003;Brieger et al., 2003), cyclothymia (Akiskal et al., 2003;Perugi et al., 2003), irritable presentations (Benazzi andAkiskal, 2003a), and the so-called bipolar spectrum disorder(Akiskal, 2003; Ghaemi et al., 2002; Hantouche et al., 2003).
It has been demonstrated that these bipolar spectrumconditions are associated with notable disability (Judd andAkiskal, 2003) and that the current diagnostic gold standard,the Structured Clinical Interview for DSM-IV (SCID), is notsufficiently sensitive to diagnose hypomania or subthresholdmanic states (Benazzi and Akiskal, 2003b). There is a need forbetter and simpler ways to identify these conditions.
Recently, Hirschfeld et al. (2000) developed and tested aself-report scale for bipolar disorder: the Mood Disorder Ques-tionnaire (MDQ). The MDQ was shown to have a sensitivity of73% and a specificity of 90%. The MDQ is an internationallyrecognized screening instrument for bipolar disorders;(Hirschfeld et al., 2000, 2003), that seems to be sensitive foridentifying bipolar I disorders but probably less so for bipolarII disorders. (Zimmerman et al., 2004). The Mood DisorderQuestionnaire has been used to screen for bipolar I and II disor-ders in a large general population epidemiology study on theprevalence and burden of illness of bipolar I and II disordersin the community (Hirschfeld et al., 2003).
Angst et al. (2005) first conceptualized the HCI-32. Its pri-mary goal is to identify hypomanic components in patientswith MDD in order to help the clinician to diagnose BPIIand other spectrum disorders (apud Angst et al., 2003) pre-senting in psychiatric and general medical practice. A second-ary goal is the development of a final potentially shortermulti-lingual version with established cut-off scores for hy-pomania. (Angst et al., 2003). Compared to the MDQ, theHCI-32 has been shown to have higher sensitivity but lowerspecificity for bipolar disorders. (Rybakowski et al., 2010;Vieta et al., 2007). The HCL-32-R1 is the revised version ofthe original HCL-32, (Angst et al., 2005) from which one
difficult question (Q4) was omitted without any loss ofinformation.
Hypomania as an element of bipolar II disorder is veryoften not experienced and recognized by the subject as path-ological, therefore not reported to doctors and under-diagnosed in 25 to 50% of depressive patients. Thus an easilyadministered screening instrument for self-assessment maybe useful in clinical practice. The aim of the present study,carried out in a sample of depressed patients attending a psy-chiatric out-patient unit of a general hospital, was to set apreliminary standardization of one Brazilian Portugueseversion of the HCL-32-R1 as a screening instrument for bipo-lar disorders and to compare results with the same sampleusing the Mood Disorder Questionnaire (MDQ).
2. Methods
2.1. Design
The study design consisted in the evaluation of the accu-racy of one Brazilian version of the HCI-32-R1 and of theMDQ, using the Structured Clinical Interview for DSM-IV,Axis I Disorders — Clinician Version (SCID-CV, First etal., 1997) module of affective disorders, as modified byBenazzi and Akiskal (2003b), as the gold standard for thediagnosis.
Prior to the interview all subjects had filled in the Brazil-ian version of the HCI-32-R1 and the MDQ. Written informedconsent was obtained from all study participants. The ques-tionnaires had been translated into Brazilian Portuguese be-fore the start of the research project, had been back-translated into English and approval had been obtainedfrom both authors (Angst and Hirschfeld) of the originalversion.
2.2. Subjects
The patients were included consecutively at the psychiatricclinic, from January 2007 to January 2009. They provided writ-ten consent to participate. Eligible subjects were psychiatricout-patients between 18 and 65 years of age who sought

Table 1Description of samples.
SCID
Scale MDQ or HCI-32 R1 + −+ A B A+B− C D C+D
A+C B+D
AAþC ¼ sensitivity ¼D
BþD ¼ specificity ¼A
AþB ¼ PPP ¼D
CþD ¼ NPP ¼ :
217I.A.T. Leão, J.A. Del Porto / Journal of Affective Disorders 140 (2012) 215–221
psychiatric care or had been referred to psychiatric evaluation.Two hundred patients were randomly selected with the helpof the Epi-Info software. Patients presenting schizophreniaand severe organic diseases were excluded.
2.3. Instruments
The Structured Clinical Interview for DSM-IV Disorders ofAxis I is a semi-structured interview aimed at formulating themain diagnoses covered by Axis-I of DSM IV. In this study weused the Clinician Version as modified by Benazzi and Akis-kal. For the diagnoses of a mood disorder the criteria ofDSM-IV were adhered to, except for BP II, for which one ofthe DSM-IV criteria for hypomania episode was left out: thecriterion for duration. Besides, the SCID-CV skip-out instruc-tion of the stem question about past elevated or irritablemood was not followed, as a negative answer would notallow the assessment of the other past hypomanic behavior.This was done mainly to permit probing for past overactivebehavior (increased goal-directed activity), when the answerto the stem question on mood was negative.
The DSM-IV 4 days minimum duration of hypomania forBP II diagnosis was not followed, because this cut-off is notbased on data (Dunner, 1998) Instead, at least 2 days of hy-pomania were required for the diagnosis of BP II.
After having remembered a period of overactivity, evenwhen at first the answer to the stem mood question hadbeen negative, the subject had the salutary result of greaterease in remembering past hypomanic mood.
The HCI-32-R1 is a self-administered paper and pencil in-ventory made up of a 32 yes/no items used to identify thehypomanic component in patients with depressive episodesin order to help the clinician to diagnose bipolar II andminor bipolar disorders in psychiatric and general medicalpractice (Angst et al., 2005). In order to help diagnose hypo-mania the instrument is designed to assess the personal andsocial role consequences of hypomanic symptoms. It alsotakes into account the subject's current overall affective sta-tus (low–usual–high) as a potentially interfering variable inanswering the questions. Several questions also have thepotential to reveal the extent to which the patient has in-sight into his condition, which is important for treatmentconsiderations.
The Mood Disorder Questionnaire is a self-report invento-ry that screens for bipolar I and II disorders with 13 yes/noitems derived from both DSM-IV criteria and clinicalexperience (Hirschfeld et al., 2000). A positive criteria screenrequires that seven or more items be endorsed, that at leastseveral of the items co-occurred, and that the symptomscaused at least moderate psychosocial impairment. TheMood Disorder Questionnaire was previously validated in agroup of psychiatric out-patients. (Hirschfeld et al., 2000).
2.4. Procedures
For the MDQ and HCI-32-R1, sensitivity and specificity,predictive validity and test–retest reliability were analyzed.The discriminative capacity of both scales for bipolar disorderwas then compared as well internal consistency and concur-rent validity. Except for test–retest reliability, the psycho-metric characteristics of the HCI-32-R1 and MDQ were
derived from the first administration of the questionnaire, in-cluding all the patients who completed the survey. Internalconsistency was evaluated by Cronbach's alpha for the totalscale and each individual item. Concurrent validity was ana-lyzed comparing DSM-IV diagnostic criteria and the scoreobtained on the HCI-32-R1 by means of the Cronbach's coef-ficient. The cut-off points in the Brazilian version of theHCI-32-R1 and MDQ were evaluated by ROC curves.
Sensitivity and specificity were calculated for each possibleMood Disorder Questionnaire symptom cut-off score relative toa SCID diagnosis of bipolar I and II disorders as a diagnostic stan-dard and were plotted as Receiver–Operating–CharacteristicsCurve (ROC).
Sensitivity was the proportion of cases with SCID diag-noses of bipolar I and II disorders correctly diagnosed bythe Mood Disorder Questionnaire, and specificity was theproportion of individuals without bipolar disorder whowere correctly identified as such by the Mood DisorderQuestionnaire.
To study the sensitivity, specificity and efficacy of theHCI-32-R1, the proportion of subjects correctly diagnosedwith BP I and BP II (bipolar spectrum disorders) and the pro-portion of subjects without the disorder identified as such,was calculated. A discriminant analysis was then used to de-scribe the percentage of subjects correctly classified based onthe result obtained on the HCI-32-R1. The interclass correla-tion coefficient was calculated for these populations. The re-sults of the HCI-32-R1 and the MDQ were compared bystudying the internal consistency of the two questionnairesbased on the T-test (Feldt, 1980). A principal componentanalysis to describe the internal structure of the HCI-32-R1
was performed (Table 1).
3. Results
3.1. Description of sample
For the comparison between age and diagnostic Student'st-test was used. In some cases the Mann Whitney test wasused. Eighty per cent of the patients were female, 59.5% pre-sented bipolar spectrum and, among these, almost 39% hadcyclothymic according to the modified SCID.
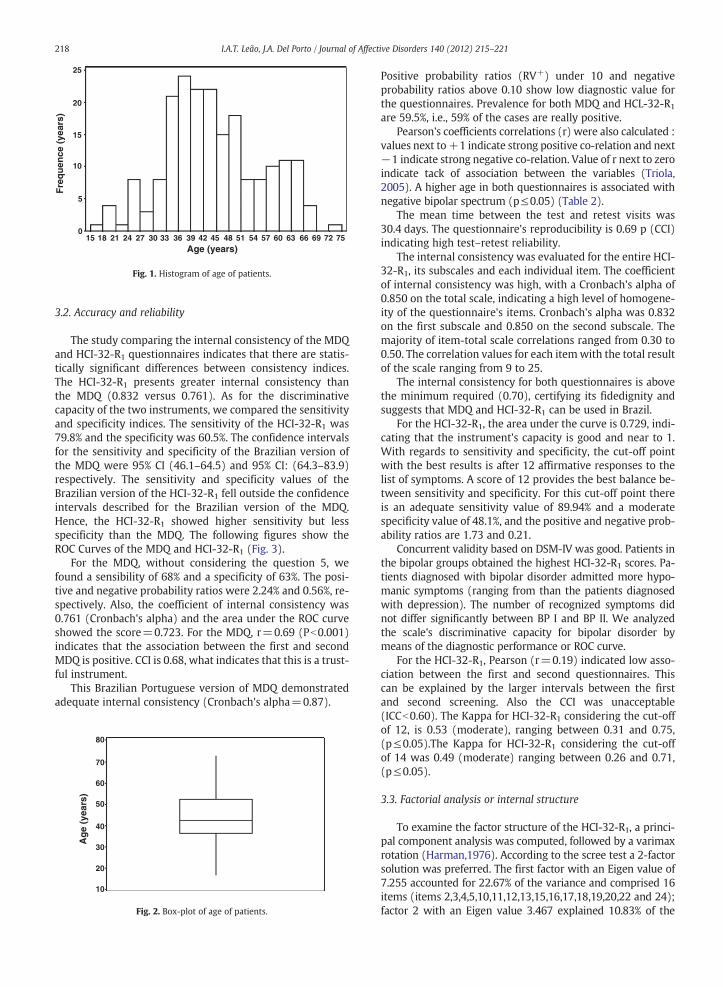
Mostly patients were around 44 (33–45), ranging a mini-mum age of 16 and maximal of 73 (see Figs. 1 and 2).
Fre
qu
ence
(ye
ars)
Age (years)
25
20
15
10
5
015 18 21 24 27 30 33 36 39 42 45 48 51 54 57 60 63 66 69 72 75
Fig. 1. Histogram of age of patients.
218 I.A.T. Leão, J.A. Del Porto / Journal of Affective Disorders 140 (2012) 215–221
3.2. Accuracy and reliability
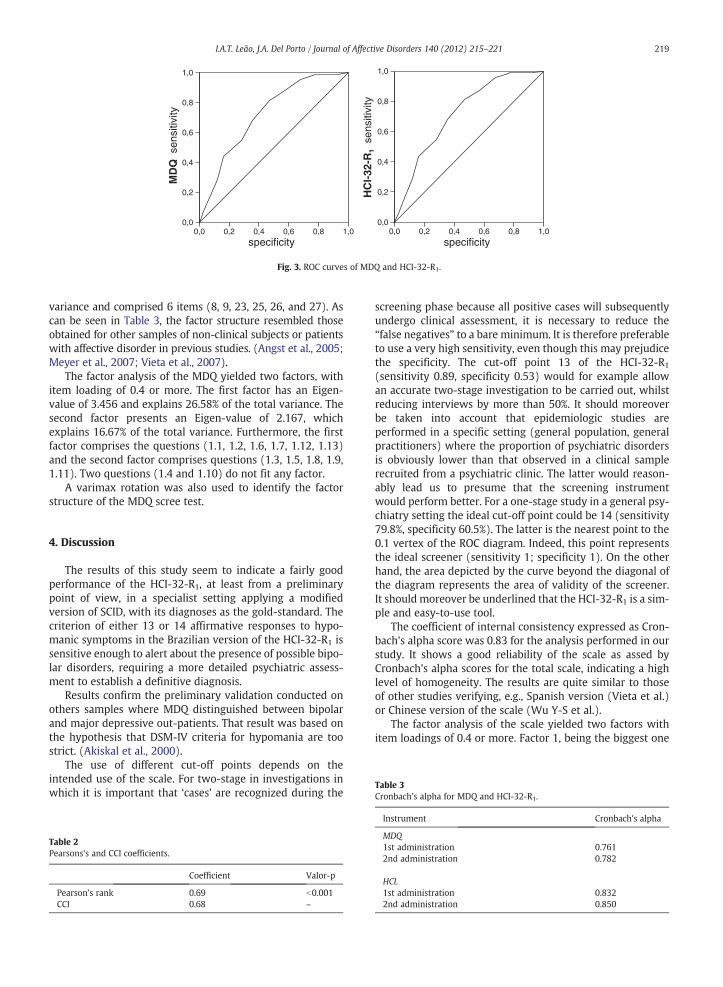
The study comparing the internal consistency of the MDQand HCI-32-R1 questionnaires indicates that there are statis-tically significant differences between consistency indices.The HCI-32-R1 presents greater internal consistency thanthe MDQ (0.832 versus 0.761). As for the discriminativecapacity of the two instruments, we compared the sensitivityand specificity indices. The sensitivity of the HCI-32-R1 was79.8% and the specificity was 60.5%. The confidence intervalsfor the sensitivity and specificity of the Brazilian version ofthe MDQ were 95% CI (46.1–64.5) and 95% CI: (64.3–83.9)respectively. The sensitivity and specificity values of theBrazilian version of the HCI-32-R1 fell outside the confidenceintervals described for the Brazilian version of the MDQ.Hence, the HCI-32-R1 showed higher sensitivity but lessspecificity than the MDQ. The following figures show theROC Curves of the MDQ and HCI-32-R1 (Fig. 3).
For the MDQ, without considering the question 5, wefound a sensibility of 68% and a specificity of 63%. The posi-tive and negative probability ratios were 2.24% and 0.56%, re-spectively. Also, the coefficient of internal consistency was0.761 (Cronbach's alpha) and the area under the ROC curveshowed the score=0.723. For the MDQ, r=0.69 (Pb0.001)indicates that the association between the first and secondMDQ is positive. CCI is 0.68, what indicates that this is a trust-ful instrument.
This Brazilian Portuguese version of MDQ demonstratedadequate internal consistency (Cronbach's alpha=0.87).
Ag
e (y
ears
)
80
70
60
50
40
30
20
10
Fig. 2. Box-plot of age of patients.
Positive probability ratios (RV+) under 10 and negativeprobability ratios above 0.10 show low diagnostic value forthe questionnaires. Prevalence for both MDQ and HCL-32-R1
are 59.5%, i.e., 59% of the cases are really positive.Pearson's coefficients correlations (r) were also calculated :
values next to+1 indicate strong positive co-relation and next−1 indicate strong negative co-relation. Value of r next to zeroindicate tack of association between the variables (Triola,2005). A higher age in both questionnaires is associated withnegative bipolar spectrum (p≤0.05) (Table 2).
The mean time between the test and retest visits was30.4 days. The questionnaire's reproducibility is 0.69 p (CCI)indicating high test–retest reliability.
The internal consistency was evaluated for the entire HCI-32-R1, its subscales and each individual item. The coefficientof internal consistency was high, with a Cronbach's alpha of0.850 on the total scale, indicating a high level of homogene-ity of the questionnaire's items. Cronbach's alpha was 0.832on the first subscale and 0.850 on the second subscale. Themajority of item-total scale correlations ranged from 0.30 to0.50. The correlation values for each itemwith the total resultof the scale ranging from 9 to 25.
The internal consistency for both questionnaires is abovethe minimum required (0.70), certifying its fidedignity andsuggests that MDQ and HCI-32-R1 can be used in Brazil.
For the HCI-32-R1, the area under the curve is 0.729, indi-cating that the instrument's capacity is good and near to 1.With regards to sensitivity and specificity, the cut-off pointwith the best results is after 12 affirmative responses to thelist of symptoms. A score of 12 provides the best balance be-tween sensitivity and specificity. For this cut-off point thereis an adequate sensitivity value of 89.94% and a moderatespecificity value of 48.1%, and the positive and negative prob-ability ratios are 1.73 and 0.21.
Concurrent validity based on DSM-IV was good. Patients inthe bipolar groups obtained the highest HCI-32-R1 scores. Pa-tients diagnosed with bipolar disorder admitted more hypo-manic symptoms (ranging from than the patients diagnosedwith depression). The number of recognized symptoms didnot differ significantly between BP I and BP II. We analyzedthe scale's discriminative capacity for bipolar disorder bymeans of the diagnostic performance or ROC curve.
For the HCI-32-R1, Pearson (r=0.19) indicated low asso-ciation between the first and second questionnaires. Thiscan be explained by the larger intervals between the firstand second screening. Also the CCI was unacceptable(ICCb0.60). The Kappa for HCI-32-R1 considering the cut-offof 12, is 0.53 (moderate), ranging between 0.31 and 0.75,(p≤0.05).The Kappa for HCI-32-R1 considering the cut-offof 14 was 0.49 (moderate) ranging between 0.26 and 0.71,(p≤0.05).
3.3. Factorial analysis or internal structure
To examine the factor structure of the HCI-32-R1, a princi-pal component analysis was computed, followed by a varimaxrotation (Harman,1976). According to the scree test a 2-factorsolution was preferred. The first factor with an Eigen value of7.255 accounted for 22.67% of the variance and comprised 16items (items 2,3,4,5,10,11,12,13,15,16,17,18,19,20,22 and 24);factor 2 with an Eigen value 3.467 explained 10.83% of the
0,0
0,2
0,4
0,6
0,8
1,0
0,0 0,2 0,4 0,6 0,8 1,0 0,0 0,2 0,4 0,6 0,8 1,00,0
0,2
0,4
0,6
0,8
1,0
MD
Q s
ensi
tivity
specificity specificity
HC
I-32
-R1
sen
sitiv
ity
Fig. 3. ROC curves of MDQ and HCI-32-R1.
219I.A.T. Leão, J.A. Del Porto / Journal of Affective Disorders 140 (2012) 215–221
variance and comprised 6 items (8, 9, 23, 25, 26, and 27). Ascan be seen in Table 3, the factor structure resembled thoseobtained for other samples of non-clinical subjects or patientswith affective disorder in previous studies. (Angst et al., 2005;Meyer et al., 2007; Vieta et al., 2007).
The factor analysis of the MDQ yielded two factors, withitem loading of 0.4 or more. The first factor has an Eigen-value of 3.456 and explains 26.58% of the total variance. Thesecond factor presents an Eigen-value of 2.167, whichexplains 16.67% of the total variance. Furthermore, the firstfactor comprises the questions (1.1, 1.2, 1.6, 1.7, 1.12, 1.13)and the second factor comprises questions (1.3, 1.5, 1.8, 1.9,1.11). Two questions (1.4 and 1.10) do not fit any factor.
A varimax rotation was also used to identify the factorstructure of the MDQ scree test.
Table 3Cronbach's alpha for MDQ and HCI-32-R1.
4. Discussion
The results of this study seem to indicate a fairly goodperformance of the HCI-32-R1, at least from a preliminarypoint of view, in a specialist setting applying a modifiedversion of SCID, with its diagnoses as the gold-standard. Thecriterion of either 13 or 14 affirmative responses to hypo-manic symptoms in the Brazilian version of the HCI-32-R1 issensitive enough to alert about the presence of possible bipo-lar disorders, requiring a more detailed psychiatric assess-ment to establish a definitive diagnosis.
Results confirm the preliminary validation conducted onothers samples where MDQ distinguished between bipolarand major depressive out-patients. That result was based onthe hypothesis that DSM-IV criteria for hypomania are toostrict. (Akiskal et al., 2000).
The use of different cut-off points depends on theintended use of the scale. For two-stage in investigations inwhich it is important that ‘cases’ are recognized during the
Table 2Pearsons's and CCI coefficients.
Coefficient Valor-p
Pearson's rank 0.69 b0.001CCI 0.68 –
screening phase because all positive cases will subsequentlyundergo clinical assessment, it is necessary to reduce the“false negatives” to a bare minimum. It is therefore preferableto use a very high sensitivity, even though this may prejudicethe specificity. The cut-off point 13 of the HCI-32-R1
(sensitivity 0.89, specificity 0.53) would for example allowan accurate two-stage investigation to be carried out, whilstreducing interviews by more than 50%. It should moreoverbe taken into account that epidemiologic studies areperformed in a specific setting (general population, generalpractitioners) where the proportion of psychiatric disordersis obviously lower than that observed in a clinical samplerecruited from a psychiatric clinic. The latter would reason-ably lead us to presume that the screening instrumentwould perform better. For a one-stage study in a general psy-chiatry setting the ideal cut-off point could be 14 (sensitivity79.8%, specificity 60.5%). The latter is the nearest point to the0.1 vertex of the ROC diagram. Indeed, this point representsthe ideal screener (sensitivity 1; specificity 1). On the otherhand, the area depicted by the curve beyond the diagonal ofthe diagram represents the area of validity of the screener.It should moreover be underlined that the HCI-32-R1 is a sim-ple and easy-to-use tool.
The coefficient of internal consistency expressed as Cron-bach's alpha score was 0.83 for the analysis performed in ourstudy. It shows a good reliability of the scale as assed byCronbach's alpha scores for the total scale, indicating a highlevel of homogeneity. The results are quite similar to thoseof other studies verifying, e.g., Spanish version (Vieta et al.)or Chinese version of the scale (Wu Y-S et al.).
The factor analysis of the scale yielded two factors withitem loadings of 0.4 or more. Factor 1, being the biggest one
Instrument Cronbach's alpha
MDQ1st administration 0.7612nd administration 0.782
HCL1st administration 0.8322nd administration 0.850

220 I.A.T. Leão, J.A. Del Porto / Journal of Affective Disorders 140 (2012) 215–221
and explaining more them half of the total variance, com-prised sixteen items connected with elevated mood and in-creased activity. Factor 2 included six items connected withirritability and risk-taking behavior. As in precedent studies(Angst et al., 2010; Rybakowski et al., 2010; Vieta et al.,2007; Wu et al., 2008) one of the two factors would be an in-dicator of hypomanic symptoms related to energy-activity(increase in activity, energy, social contacts, verbal fluency,communication with others and self-confidence) and theother would be related to disinhibition, self-control and at-tention capacity (irritability, distractibility, mental controldifficulties, risk behavior, being unpleasant to others and ex-cessive spending). This dual structure of hypomania with“classic” driven euphoria and irritable risk taking expressionswas previously described by using a preliminary version ofHypomania Checklist as “dark” and “sunny” expressions ofsoft bipolarity (Akiskal et al., 2003; Hantouche et al., 2003).
Neither factor enables us to distinguish subtypes of bipo-lar disorder. We confirm the existence of these two factors,higher scores in themwould be indicative of suffering a bipo-lar disorder.
In summary, the HCI-32-R1 has been shown to be a usefulinstrument for the detection of hypomania in patients withaffective disorders, thus leading to better detection of bipo-larity than with the MDQ. A key aspect of appropriate man-agement of bipolar disorders, this questionnaire representsa potential improvement in clinicians' ability to detect andcorrectly treat bipolar disorder, and in some aspects suchas internal consistency, obtain better results than theMDQ. The lower specificity of the MDQ could be explainedby the fact that it does not include many items. The hypo-manic or sub-hypomanic episodes that characterize type IIand NOS can be especially difficult for patients to recognizesince they do not, by definition, cause significant impair-ment. The sensitivity of the scale may be due to its focuson change in energy and drive during hypomanic periodsrather than an emphasis on patients' self-report of moodsymptoms.
Interestingly enough, a high percentage of depressed pa-tients had a HCI-32-R1 score of 14 or above, indicating eithersome false positives or, alternatively, as postulated by Akiskalet al. (2003) that “soft” hypomania may be present even inclinically indisputable “unipolar” patients.
The high prevalence (59.5%) of bipolar spectrum foundamong depressive patients interviewed through the modifiedSCID is very similar to that found by Angst et al. (2005).
More studies in different clinical and epidemiological set-tings are needed.
Role of funding sourceThere were no research funds.
Conflict of interestsThe author Inês Alice Teixeira Leão has no conflict of interest. This au-
thor declares that she has no competing interests.Prof. Del Porto is member of the international board of the Lundbeck In-
stitute, speaker for AstraZeneca, Bristol, GSK, Pfizer, Abbott, Lilly, Lundbeck,Servier and Clinical researcher for Servier.
AcknowledgmentsCel. Dr. Domingos Sávio Lage Guerra.
References
Akiskal, H.S., 2003. Validating “hard” and “soft” phenotypes within the bipo-lar spectrum: continuity and discontinuity. Journal of Affective Disorders73, 1–5 Hantouche, E.G.
Akiskal, H.S., Benazzi, F., 2003. Family history validation of the bipolar natureof depressive mixed states. J. Affect. Disord. 73, 113–122.
Akiskal, H.S., Bourgeois, M.L., Angst, J., Post, R., Moller, H., Hirschfeld, R.,2000. Re-evaluating the prevalence of and diagnostic composition with-in the broad clinical spectrum of bipolar disorders. Journal of AffectiveDisorders 1 (Suppl. 59), S5–S30.
Akiskal, H.S., Hantouche, E.G., Allilaire, J.F., 2003. Bipolar II with and withoutcyclothymic temperament: “dark” and “sunny” expressions of soft bipo-larity. Journal of Affective Disorders 73, 49–57.
Angst, J., Gamma, A., Benazzi, F., Ajdacic, V., Eich, D., Rössler, W., 2003. Diagnosticissues in bipolar disorder. EuropeanNeuropsychopharmacology13, S43–S50.
Angst, J., Adolfsson, R., Benazzi, F., Gamma, A., Hantouche, E., Meyer, T.D.,Skeppar, P., Vieta, E., Scott, J., 2005. The HCI-32 towards a self-assessement tool for hypomanic symptoms in out patients. Journal ofAffective Disorders 88, 217–233.
Angst, J., Meyer, T.D., Adolfsson, R., Skeppar, P., Carta, M., Benazzi, F., Lu, R.B.,Wu, Y.H., Yang, H.C., Yuan, C.M., Morselli, P., Brieger, P., Katzmann, J.,Teixeira Leão, I.A., Del Porto, J.A., Hupfeld Moreno, D., Moreno, R.A.,Soares, O.T., Vieta, E., Gamma, A., 2010. Hypomania: a transcultural per-spective. World Psychiatry 9 (1), 41–49 February.
Benazzi, F., Akiskal, H.S., 2003b. Refining the evaluation of bipolar II: beyondthe strict SCID-CV guidelines for hypomania. Journal of Affective Disor-ders 73, 33–38.
Benazzi, F., Akiskal, H.S., 2003a. The dual factor structure of self-rated MDQhypomanic: energized-activity versus irritable-thought racing. Journalof Affective Disorders 73, 34–64.
Brieger, P., Roettig, S., Ehrt, U., Wenzel, A., Blöink, R., Marneros, A., 2003.TEMPS — a scale in "mixed" and "pure" manic episodes: new date andmethodological considerations on the relevance of joint anxious — de-pressive temperament traits. J. Affect. Disord. 73, 99–104.
Dunner, D.L., 1998. Diagnostic revisions for DSM-IV. On:. In: Goodnick, P.L.(Ed.), Mania, Clinical and Research Perspectives. American PsychiatricPress, Washington, DC, pp. 3–10.
Feldt, L.S., 1980. A test of the hypothesis that Cronbach's Alfa reliabilitycoefficient is the same for two tests administered to the same sample.Psychometria 45, 99–105.
First, M.C., Spitzer, R.L., Gibbon, M., Williams, J.B.W., 1997. Structured ClinicalInterview for DSM-IV Axis I Disorders — Clinician Version (SCID-CV).American Psychiatric Press, Washington, DC.
Ghaemi, S.N., Ko, J.Y., Goodwin, F.K., 2002. “Cade's discase” and beyond:misdiagnosis, antidepressant use, and a proposed definition for bipolarspectrum disorder. Canadian Journal of Psychiatry 47, 125–134.
Hantouche, E.G., Angst, J., Akiskal, H.S., 2003. Factor structure of hypomanic,interrelationsships with cyclothymic and the soft bipolar spectrum.Journal of Affective Disorders 73 (1–2), 39–47.
Harman, H.R., 1976. Modern Factor Analysis. University of Chicago Press.Hirschfeld, R., Willians, J., Spitzer, R., Calabrese, J., Flynn, L., Reck, P., Lewis, L.,
McElroy, S., Post, R., Rapport, D., Russel, J., Sachs, G., Zajecka, J., 2000.Development and validation of a screening instrument for bipolar spec-trum disorder: the mood disorder questionnaire. The American Journalof Psychiatry 157, 1873–1875.
Hirschfeld, R.M.A., Calabrese, J.R., Weissmann, M.M., Reed, M., Davier, M.A.,Faye, M.A., Keck Jr., F.E., Lewis, L., Mc Elroy, S.L., MC Nulty, J.F., Wagner,K.D., 2003. Screening for bipolar disorder in the Community. The Journalof Clinical Psychiatry 64 (1), 53–59.
Judd, L., Akiskal, H., 2003. The prevalence and disability of bipolar spectrumdisorders in the US population: re-analysis of the ECA database takinginto account subthseshold cases. Journal of Affective Disorders 73,123–131.
Meyer, T.D., Adolfsson, R., Angst, J., 2007. The Hypomania Checklist(HCL-32): its factorial structure and association to indices of impairmentin German and Swedish nonclinical samples. Comprehensive Psychiatry48 (1), 79–87.
Perugi, G., Toni, C., Travierso, M.C., Akiskal, H.S., 2003. The role of cyclothy-mia in atypical depression: toward a data-based reconceptualization ofthe borderline-bipolar II connection. Journal of Affective Disorders 73,87–98.
Rybakowski, J., Angst, J., Dudek, D., et al., 2010. Polish version of theHypomania Checklist (HCI-32) scale: the results in treatment-resistantdepression. European Archives of Psychiatry and Clinical Neuroscience260 (2), 139–144.
Triola, Mario F, 2005. Introdução à estatística. 9 ed. LTC, Rio de Janeiro.Vieta, E., Sanchez-Moreno, J., Bulbena, A., Chamorro, L., Ramos, J.L., Artal, J.,
Perez, F., Oliveras, M.A., Valle, J., Lauerta, J., Angst, J., 2007. for the
221I.A.T. Leão, J.A. Del Porto / Journal of Affective Disorders 140 (2012) 215–221
EDHIPO (hypomania detection study) Cross validation with the mooddisorder questionnaire (MDQ) of an instrument for the detection ofhypomania in Spanish: the 32 item hypomania symptom checklist(HCI-32). Journal of Affective Disorders 101, 43–55.
Wu, Y.-S., Angst, J., Ou, C.-S., Chen, H.-C., Lu, R.-B., 2008. Validation of theChinese version of the Hypomania Cheklist (HCI-32-R1) as an instrument
for detecting hypo (mania) in patients with mood disorders. Journal ofAffective Disorders 106, 133–143.
Zimmerman, M., Pasternak, M.A., Chelminsk, I., Salomon, D.A., 2004. Usingquestionnaires to screen for psychiatric disorders: a comment on thestudy of screening for bipolar disorder in the community. The Journalof Clinical Psychiatry 45 (5) 605/610.


















![P2020 QorIQ Integrated Processor Hardware[1] ma [8] mcke [2] mck [3] mdm [7] lgpl [3] mdq [41] mdq [61] mdm [5] mdqs [5] mdq [60] lad [13] mdq [56] lwe [1] lad [15] lad [11] lclk [1]](https://img.pdfslide.us/doc/110x75/6006250dd91d683d27518c79/p2020-qoriq-integrated-processor-1-ma-8-mcke-2-mck-3-mdm-7-lgpl-3-mdq.jpg)










