Embed Size (px)
Citation preview

www.EuropeanJournalPain.com
European Journal of Pain 11 (2007) 244–255
Cross-sectional evaluation of patient functioning andhealth-related quality of life in patients with neuropathic pain
under standard care conditions
Rafael Galvez a,*, Carlos Marsal b, Javier Vidal c, Manuel Ruiz d, Javier Rejas e
a Pain and Palliative Care Unit, Hospital Universitario Virgen de las Nieves, Unidad de dolor y Cuidados Paliativos, Avda de las
Fuerzas Armadas, 2, 18014 Granada, Spainb Department of Neurology, Hospital Virgen de la Salud, Toledo, Spain
c Department of Rheumatology, Hospital General Universitario, Guadalajara, Spaind Neurosciences Medical Area, Medical Unit, Pfizer Espana, Madrid, Spain
e Health Outcomes Research Department, Medical Unit, Pfizer Espana, Madrid, Spain
Received 3 October 2005; received in revised form 4 January 2006; accepted 5 February 2006Available online 24 March 2006
Abstract
Aim: The purpose of this cross-sectional evaluation was to determine the impact of neuropathic pain (NeP) on patient functioningand Health-Related Quality of Life (HRQoL) under standard care conditions.Methods: Patients with NeP or neuropathic and nociceptive pain [Mixed Pain (MP)] enrolled in the DONEGA study, a naturalistic,prospective and multi-centre study of the effectiveness of gabapentin under usual care conditions, were included in this cross-sec-tional evaluation before starting study treatments. Participants completed the Short Form-McGill Pain Questionnaire, MOS ShortForm-12 (SF-12), and Sheehan Disability Scale (ShDS). Multivariate analysis and regression models were used to analyze patientdata.Results: A total of 1519 patients [mean ± SD; 56.0 ± 13.7 yrs old (58.8% female)] with NeP or MP were enrolled in the study. Themean pain history was 1.1 ± 2.8 yrs, current pain intensity on a 5-point visual analogue scale was 2.8 ± 1.0 and mean pain in pre-vious week was 71.3 ± 19.0 mm. Pain substantially interfered (i.e., score P 5 on 0–10 scale) with normal work (5.9 ± 3.0), social life(5.7 ± 3.0), and family life (5.3 ± 3.0), producing substantial disability (total ShDS score of 16.9 ± 8.3 pts). Country-standardisedphysical (PCS) and mental health (MCS) component summary scores of SF-12 indicated significant impairment in both domainscompared with the general Spanish population: PCS; �1.13 ± 1.0 SDS (standard deviation score), and MCS; �1.21 ± 0.7 SDS,equivalent to the 15th and 25th percentiles of normative populations, respectively.Conclusions: Under standard care conditions, neuropathic and mixed pain are associated with impaired physical and mental QoL,producing a substantial level of disability in these patients.� 2006 European Federation of Chapters of the International Association for the Study of Pain. Published by Elsevier Ltd. Allrights reserved.
Keywords: Disability; Mixed pain; Neuropathic pain; Real world; Standard care conditions; Quality of life
1090-3801/$32 � 2006 European Federation of Chapters of the International
reserved.
doi:10.1016/j.ejpain.2006.02.002
* Corresponding author. Tel.: +34 958 241100.E-mail address: [email protected] (R. Galvez).
1. Introduction
The International Association for the Study of Pain(IASP) defines neuropathic pain (NeP) as pain initiated
Association for the Study of Pain. Published by Elsevier Ltd. All rights

R. Galvez et al. / European Journal of Pain 11 (2007) 244–255 245
or caused by a primary lesion or dysfunction in the
nervous system. NeP is a common symptom of an het-erogeneous group of disorders that includes diabeticneuropathy, trigeminal neuralgia, post-herpetic neural-gia and spinal cord injury, among others (IASP TaskForce in Taxonomy, 1994; Jensen et al., 2001; Nichol-son, 2003). NeP is a chronic and remarkably commoncondition. According to the study ‘‘Pain in Europe’’(Pain in Europe, 2005), chronic pain is an extensiveproblem affecting 1 out of every 5 individuals (19%,approximately 75 million people). It is generallyacknowledged that NeP is extremely difficult to treat,and the presence of comorbidity is known to have amajor impact on outcome (Nicholson and Verma,2004). Patients with persistent pain experience workdisability and activity limitation with a substantialimpact on their social functioning (Gureje et al.,1998) and are substantially more likely to have associ-ated disorders such as anxiety, depression, poor sleep,and interference with social roles and personal identity(Gureje et al., 1998; McWilliams et al., 2003; Harriset al., 2003). Therefore, neuropathic pain is a signifi-cant problem for both patients and the health caresystem.
The limited information currently available on neu-ropathic pain is consistent with the wider literature onchronic pain and indicates that pain assessment shouldinclude measurement of multiple dimensions of qualityof life and social functioning (Haythornthwaite andBenrud-Larson, 2001). Health-related quality of life(HRQoL) has been found to be severely impaired inpatients with NeP of varied origin (Meyer-Rosberget al., 2001a; Galer et al., 2000), and persistentchronic pain affects both physical and mental well-being (Meyer-Rosberg et al., 2001b). Despite this evi-dence, most experimental trials have primarily focusedon pain relief rather than on the impact of NeP onHRQoL and patient functioning. Therefore, theseissues are under-researched in many health settings,especially under standard patient care conditions.Despite recent European guidelines recommendingassessment of these health areas, clinicians appear topay more attention to psychiatric comorbidities associ-ated with NeP, e.g., depression and anxiety (Hardenand Cohen, 2003; Cruccu et al., 2004). Thus, few stud-ies have evaluated the impact of NeP on patient-reported functioning and well-being, and these havelargely addressed specific diseases, such as diabeticperipheral neuropathy.
The aim of this study was to evaluate the impact of abroad range of neuropathic pain and mixed pain syn-dromes on HRQoL and patient functioning in a cohortof patients referred for pain control under usual specia-lised pain care conditions (Galvez et al., 2004b; Galvezand the Spanish team for Study of Neuropathic Pain,2004a).
2. Material and methods
2.1. Study population
The impact of neuropathic pain (NeP) on patientfunctioning and health-related quality of life (HRQoL)was analyzed in a sample of male and female patients,18 years of age and older, enrolled in a pragmatic, openlabel, prospective, multi-centre study conducted in spec-ialised pain care settings (pain units, neurology, rheuma-tology, etc.) throughout Spain between 2002 and 2003(the DONEGA study (Galvez et al., 2004b; Galvezand the Spanish team for Study of Neuropathic Pain,2004a)). This study assessed the effectiveness of analge-sic treatment for NeP of broad origins with flexibledoses of gabapentin for 3 months. A cross-sectionalevaluation was performed using baseline sample databefore administration of any study treatment. Inclusioncriteria were: being an outpatient (male or female) agedP18 years; clinical diagnosis of neuropathic pain,capacity to participate in a clinical study, and willing-ness to give written consent to their participation. Exclu-sion criteria were: known hypersensitivity to gabapentinor its excipients, pregnancy or breastfeeding, being hos-pitalised or institutionalised, and inability to completehealth questionnaires. The study was designed to studythe management and treatment of these patients underreal-world conditions of standard medical practice.Table 1 details the main demographic and diagnosticcharacteristics of the study sample.
Sample size estimation was based on the objective offinding significant differences in pain score on the visualanalogue scale (VAS) of the short form of the McGillPain Questionnaire (SF-MPQ) (Melzack, 1987) amongthe overall sample and among subpopulations ofpatients classified according to their underlying pain-associated disease after three months of treatment withflexible doses of gabapentin. Patients were consecutivelyenrolled by non-probabilistic sampling after confirma-tion of patient consent to inclusion in the study and ver-ification of eligibility criteria. Cluster sampling was usedto select participating centres (centres/clinics caring forpatients with pain). Pain specialists at each centre wereselected at random.
2.2. Description of scales
2.2.1. SF-MPQ
Pain assessment using the SF-MPQ was the primaryefficacy parameter of the DONEGA study (Meyer-Ros-berg et al., 2001b). The primary endpoint was thechange in the mean score on the 100-mm line VAS forpain intensity anchored by ‘‘0 mm = no pain and100 mm = worst possible pain’’. The 100-mm line VASfor pain intensity is part of the SF-MPQ. The SF-MPQ also includes a 5-point global rating scale

Table 1Demographic characteristics and baseline scoring in the Short FormMcGill Pain Questionnaire (SF-MPQ), abridged version of the SF-12Quality of Life Questionnaire, and Sheehan Disability Scale (ShDS) ofpatients enrolled in the DONEGA study
na 1509Age (years) 56.9 (13.6)Sex (female) 61.2% (58.6–63.7%)BMI (kg/m2)b 26.8 (4.0)Obese (BMI P30) 18.1% (15.5–20.8%)Time since diagnosis (years) 1.2 (2.8)
Naıve: 28.1% (25.7–30.5%)<1 year: 48.8% (46.1–51.4%)P1 year: 23.2% (20.9–25.4%)
Current analgesic treatment 71.9% (69.5–74.3%)
Pain score (SF-MPQ)Visual analog scale-VAS- (0–100): 71.3 (19.0)Present pain intensity (1–6): 2.8 (1.0)
Sample distribution by pain intensity in VASSevere (>70) 61.2% (58.6–63.7%)Moderate (40–70) 32.6% (30.2–35.1%)Mild (<40) 6.2% ( 5.0–7.6%)
Score in the SF-12 questionnairePhysical component summary (PCS) 37.6 (5.9)Mental component summary (MCS) 46.0 (8.1)SDS-PCSc �1.13 (1.0)SDS-MCS �1.21 (0.7)
Score in the ShDS scale Mean (SD) % markedand/or extremedisabilityd
Total score (3 items; range 0–30): 16.9 ( 8.3) 42.7 (39.8–45.7)Work item (0–10): 5.9 ( 3.0) 50.8 (47.9–53.8)Social life item (0–10): 5.7 ( 3.0) 47.3 (44.4–50.3)Family life item (0–10): 5.3 ( 3.0) 42.2 (39.2–45.1)Perceived stress (0–10): 5.0 ( 3.0) 37.7 (34.8–40.6)Perceived social support (0–100): 65.0 (28.3) 19.4 (17.0–21.7)e
Values given as proportion (95% CI) or mean (standard deviation).a The study enrolled 603 (41.3%) patients with neuropathic pain, 856
(58.7%) with mixed pain (neuropathic and nociceptive pain), and 60patients who were considered non valuable because their type of painwas not identified.
b BMI, body mass index.c SDS, standardised score relative to the Spanish reference
population.d Individual score in each item P 7 or P21 in total score.e Proportion (%) of patients with a score 630% (equivalent to no or
little support).
246 R. Galvez et al. / European Journal of Pain 11 (2007) 244–255
(1 = mild to 5 = excruciating) that was used to assessthe intensity of pain at study recruitment, designatedpresent pain intensity.
2.2.2. Medical outcomes trust short form 12 (SF-12)
HRQoL was assessed by administering the Spanishversion of the SF-12 (Ware et al., 1996; Gandek et al.,1998). This is a generic, self-administered quality of lifetool, with most items scored as yes–no or on 5–6-pointscales. Scores are summarised into two summary com-ponents, Physical and Mental Component Summaries(PCS and MCS), and range from 0 (worst possible qual-
ity of life) to 100 (best possible quality of life). However,for adequate interpretation, standard deviation scores(SDS) were estimated for both physical summary andmental components using the Spanish SF-12 norms forsex and age (Vilagut et al., 2005).
2.2.3. Sheehan disability scale (ShDS)
Patient functioning was assessed using the Spanishversion of the ShDS (Bobes et al., 1999; Sheehanet al., 1996). It assesses patient functional impairmentin three domains: work impairment, social impairment,and impairment of family life/home responsibilities.Two further items gather data on patient-perceivedstress and social support. Baseline assessments weremade of the degree of disability in the work, social lifeand family life domains, and of the levels of stress andsocial support perceived by patients. For better interpre-tation, observed scores were compared with scores of thenormal population studied for cultural and psychomet-ric validation of the Spanish version of ShDS (Bobeset al., 1999). The first four items of the instrument arerated on a Likert type scale (0 = no disability;10 = extreme disability). The fifth item (perceived socialsupport) uses a similar scale but expressed as percent-ages (0% = no support, 100% = ideal support). Thetotal score is the sum of the scores for the first threeitems (work, social life, and family life) and ranges from0 (no disability) to 30 (extreme disability). Items 4 and 5are directly and separately interpreted, although thescore for the fifth item must be inverted.
2.3. Statistical methods
Pain intensity was measured by means of the shortform of the McGill pain scale, using a visual analoguescale (VAS) to assess the mean pain intensity in theprevious week, and ordinal VAS to assess present painintensity. Patients were grouped according to their painat study recruitment as follows: patients with mildpain (VAS < 40), moderate pain (VAS 40–69), andsevere pain (VAS P70). Patients were also segmentedas follows: according to their body mass index (BMI)into normal weight (<27), overweight (P27 and <30),and obese (P30) groups; according to time elapsed sincestart of neuropathic or mixed pain, classified as no time(diagnosis at recruitment), less than 1 year, and 1 year ormore; and according to presence or not of current anal-gesic treatment. SDS were obtained using the followingequation: SDS = observed score minus mean score ofnormative group of same sex and age, divided by stan-dard deviation of the normative group. To facilitateinterpretation of the ShDS, patients were also classifiedaccording to the following dysfunction levels for eachscale item: no dysfunction or stress – or no social sup-port (0 score for item); mild dysfunction or stress orlow social support (score of 1, 2, or 3; score of 1–30%

R. Galvez et al. / European Journal of Pain 11 (2007) 244–255 247
for item 5); moderate dysfunction or stress, or moderatesocial support (score 4, 5, or 6; score of 31–60% for item5); marked dysfunction or stress, or marked social sup-port (score 7, 8, or 9; score of 61–99% for item 5); andextreme dysfunction or stress, or high social support(score of 10; score of 100% for item 5).
A descriptive analysis was performed, including cen-tral tendency and dispersion statistics for continuous
variables and frequencies and percentages for categoricalvariables, applying the Kolmogorov–Smirnov test fornormality of distribution. A baseline homogeneity anal-ysis was performed considering: type of pain (Ne orMP); sex; age; pain intensity; body mass index; timesince pain commencement; analgesic treatment; andtype of centre (specialty). This analysis used a Student’st test for independent groups and a parametric androbust analysis of variance (Welch and Brown–Forsytherobust tests) according to the type and distribution ofthe variable. Categorical variables were compared usinga v2 test, Fisher’s exact test or linear v2 statistic for ordi-nal categorical variables. All tests were two-sided, andan alpha error of <0.1 was accepted as significant toreject the homogeneity hypothesis.
Multivariate linear regression models were con-structed using block design with centres grouped by spe-cialty as fixed variable and the other variables by abackward stepwise procedure, with scores for physicaland mental summary components as dependent vari-ables. Variables initially included in the model were typeof pain (Ne or MP), age, sex, time since diagnosis, pres-ence of current analgesic treatment, body mass index,VAS-assessed pain intensity, and type of participatingcentre/specialty. The F probability value was used as cri-terion for excluding variables from the model (inclu-sion < 0.05; exclusion > 0.10), except for the centre/specialty variable, which was maintained constant inthe models. An analysis of covariance (ANCOVA) withspecialty, sex, age, and type of pain as covariates wasused to analyze the physical and mental componentsof quality of life (expressed as SDS) according to themean pain intensity in the previous week, categorisedas mild, moderate, or severe. Bonferroni test was appliedfor statistical comparison between groups. Two-wayanalysis of variance (ANOVA) models (adjusted for spe-cialty, sex, type of pain, body mass index, and presentpain intensity variables) were used to analyze the effectof pooled age and sex or type of pain on the physicaland mental QOL of patients with NeP or MP. Bonfer-roni’s correction was applied to multiple comparisons,and a Levene test was used to verify the assumed homo-scedasticity of variables.
ShDS results were analyzed by ordinal regressionmodels for the total score (sum of items 1– 3), and a sep-arate model for item 4 (perceived stress). Item 5 (socialsupport) was analyzed using a multivariate linear regres-sion model. In all cases, variables initially included in
the model were type of pain, neuropathic or mixed pain,age, sex, time since diagnosis, presence of current anal-gesic treatment, body mass index, VAS-assessed painintensity, and medical specialty. The F probability valuewas used as criterion for excluding variables in themodel (inclusion < 0.05; exclusion > 0.10). An ANOVAmodel for repeated measures was used for within-groupcomparison of the mean scores in items 1–4 of the dis-ability scale, and ANCOVA models were used to com-pare ShDS scores among subgroups, adjusted byspecialty, sex, pain intensity, age and type of pain ascovariates. Bonferroni’s correction was used for multi-ple comparisons, and a Levene test was used to verifythe assumed homoscedasticity of variables.
The DONEGA Study was conducted in compliancewith Spanish legal regulations for observational, post-marketing studies of drugs administered to humansubjects. Approval was requested from three hospitalClinical Research Ethics Committees according to Span-ish regulations on post-marketing studies, and wasgranted before commencement of the study. The studywas also conducted in compliance with the ethical prin-ciples for medical research involving human subjectsstated in the Declaration of Helsinki of the World Med-ical Association and its amendments. The physicians incharge were responsible for patient screening andrecruitment. Data were collected by investigators oncase report forms, monitored centrally to check for miss-ing information or inconsistencies and subsequentlycompiled for analysis. A written informed consent wasobtained from each patient before study entry.
3. Results
A total of 1519 patients [603 patients with neuro-pathic pain (NeP), 856 patients with neuropathic andnociceptive mixed pain (MP), and 60 patients with painof an unknown cause, who were therefore excluded fromevaluation] were enrolled in the study; 61.2% werefemale. All patients were aged over 18 yrs, with a meanage (±standard deviation) of 56.9 ± 13.6 yrs. Mean timeelapsed since diagnosis was 1.1 ± 2.8 yrs. Table 1 showsthe main demographic characteristics of patients, theirscale scores, and their distribution by VAS-assessed painintensity. Current pain intensity on the SF-MPQ ordinalscale was 2.8 ± 1.0 (mean ± standard deviation), andmean VAS-assessed pain in the previous week was71.2 ± 18.9 mm. The underlying diseases and clinicalsyndromes of the NeP and MP patients in the studyare shown in Table 2.
3.1. Health-related quality of life (MOS-SF-12)
The patients had mean scores of 37.6 ± 5.9 for thephysical component summary and 46.0 ± 8.1 for the

Table 2Observed frequencies and percent distribution of underlying causes of neuropathic pain or neuropathic and nociceptive mixed pain (Values are givenas frequency (proportion) [95% confidence interval])a
Neuropathic pain (n = 603) Mixed pain (n = 856)
Diabetic neuropathy 66 (10.9%) [8.5–13.4%] Radiculopathy 245 (28.6%) [25.6–31.6%]Trigeminal neuralgia 58 (9.6%) [7.4–12.3%] Lumbar pain 193 (22.5%) [19.7–25.3%]CRPSb 77 (12.8%) [10.1–15.4%] Slipped disk 147 (17.2%) [14.6–19.7%]Post-herpetic neuropathy 89 (14.8%) [11.9–17.6%] Spinal canal stenosis 68 (7.9%) [6.2–10.0%]Entrapment syndromesc 115 (19.1%) [15.9–22.2%] Spondylosis 56 (6.5%) [5.0–8.4%]Central post-stroke pain 22 (3.6%) [2.3–5.5%] Surgical trauma 45 (5.3%) [3.9–7.0%]Phantom limb pain 16 (2.7%) [1.5–4.3%] Spondylolisthesis 17 (2.0%) [1.0–2.9%]Peripheral neuropathies and other neuralgiasd 160 (26.5%) [23.0–30.1%] Musculoskeletal and rheumatologic causese 87 (10.2%) [8.4–12.4%]
a Among the 1519 patients enrolled in the DONEGA study, the type of pain was not identified in 60 patient, who were therefore considered nonvaluable.
b CRPS, complex regional pain syndrome.c Includes carpal tunnel syndrome.d Includes neuralgia of glosofaringeo, metabolic and toxic peripheral neuropathies, mielitis, tumours, etc.e Includes causes with a frequency <2% (osteoporosis, arthritis and osteoarthritis, bone fracture, spondylitis, etc.).
248 R. Galvez et al. / European Journal of Pain 11 (2007) 244–255
mental component summary of MOS-SF-12, valuesbelow the 15th and 25th percentiles, respectively, ofSpanish norms for this instrument (Table 1); the meanstandardised scores were �1.13 ± 0.98 and �1.21 ±0.68 points, respectively. Table 3 lists the variables iden-tified as predictors in the multivariate regression modelsfor the physical and mental components; age and sexwere the variables with greatest relative weight in bothmodels.
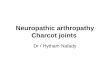
Figs. 1–3 show the main quality of life resultsexpressed as SDS with respect to Spanish populationnorms. Both physical and mental scores were stronglyand significantly related to patient age, with higherscores for older patients (Fig. 1), and this relationship
Table 3Multivariate linear regression models showing the significant b-coefficientcomponent expressed as standardised score (SDS) relative to the Spanish refand nociceptive) pain
Variable Coefficient b (95% CI)
Physical component
Constant �4.70 (�5.07 to �4.33)Age (years) 0.05 (0.04–0.05)BMI (kg/m2) 0.01 (0.00–0.02)Sexa 0.44 (0.36–0.52)Center �0.01 (�0.03 to 0.00)Type of painb 0.24 (0.16–0.32)Present pain intensityc �0.04 (�0.08 to 0.00)R2 corrected = 0.506; ANOVA, F = 216.73 (p < 0.0001)
Mental component
Constant �2.99 (�3.21 to �2.76)Age (years) 0.01 (0.01–0.02)Sexa 0.71 (0.65–0.78)Center �0.02 (�0.04 to �0.01)Type of painb 0.24 (0.17–0.31)R2 corrected = 0.329; ANOVA, F = 130.21 (p < 0.0001)
BMI, body mass index.The center variable was kept fixed in both models and variables with a sign
a Male = 1, Female = 2.b Neuropathic = 1, Mixed (neuropathic and nociceptive) = 0.c 1 = no pain, 2 = mild, 3 = bothersome, 4 = severe, 5 = terrible.
was more marked in the physical component model.Younger age groups had significantly lower standar-dised scores (very different from scores of the normativepopulation) compared with older age groups, whosescores approached mean values in the general popula-tion. After adjusting for type of specialty, present painintensity and type of pain (Fig. 2), the score in bothphysical and mental components of the quality of lifequestionnaire was significantly lower in male thanfemale patients all other age groups except the youngest(18–24 yrs). Patients with moderate mean pain intensity(by SF-MPQ) in the previous week had a significantlylower SDS in both quality of life components versuspatients with severe pain (p = 0.006 for physical
s of variables explaining quality of life score [physical and mentalerence population] in patients with neuropathic or mixed (neuropathic
t Significance
�25.08 <0.000132.09 <0.00011.72 0.085
10.79 <0.0001�1.57 0.116
5.81 <0.0001�1.88 0.061
�26.20 <0.000110.09 <0.000120.93 <0.0001�3.00 0.003
6.95 <0.0001
ificance p < 0.1 were included.

-4.00
-3.50
-3.00
-2.50
-2.00
-1.50
-1.00
-0.50
0.00
0.50
1.00
Age (years)
)SD
S( tnenopmoc lacisyhP
-4.00
-3.50
-3.00
-2.50
-2.00
-1.50
-1.00
-0.50
0.00
0.50
1.00
0 10 20 30 40 50 60 70 80 90 100
0 10 20 30 40 50 60 70 80 90 100
Age (years)
)S
DS( tnen opmoc latne
M
Adjusted SDS [mean + SD (95% CI)] = -1.13 + 0.71 (-1.17 to -1.09)
Adjusted SDS [mean + SD (95% CI)] = -1.21 + 0.42 (-1.22 to -1.20)
Fig. 1. Scatter plot showing the linear relationship between age (years) and quality of life of the patient; physical and mental components, given as astandardised score relative to the reference Spanish population (SDS). SDS score is shown for each patient adjusted for type of neuropathic pain,center, and present pain intensity, age, and sex. SD, standard deviation; 95% CI, 95% confidence interval.
R. Galvez et al. / European Journal of Pain 11 (2007) 244–255 249
component and p = 0.020 for mental component) ormild pain (p = 0.026 and p = 0.037, respectively, Fig. 3).
3.2. Sheehan disability scale (ShDS)
The youngest age group (18–24 yrs) had a highermean ShDS compared with older patients, althoughthe difference was only close-to-significant (p < 0.1),with a high degree of similarity among scores of theother age groups. Mean total disability scores were21.4 (17.2–25.7) [mean (95% CI)], 15.9 (13.7–18.0),
18.2 (16.7–19.5), 17.2 (16.2–18.1), 16.7 (15.7–17.6),16.4 (15.5–17.4), and 16.3 (14.8–17.8) for age strata of18–24 , 25–34, 35–44, 45–54, 55–64, 65–74, and P75years, respectively. A similar pattern was observed inthe results for both perceived stress and social support,with the youngest age group showing a non-significantlyhigher score than the other age groups and no differ-ences among the latter.
Approximately 43% of patients had marked and/orextreme disability (score P 21), with a relatively homo-geneous distribution in the degree of disability for each

-5
-4
-3
-2
-1
0
1
-5
-4
-3
-2
-1
0
1
18 -24 25 -34 35 -44 45 -54 55 - 64 65 -74 >75-
***
***
***
*** ***
***
-3
-2.5
-2
-1.5
-1
-0.5
0
0.5
-3
-2.5
-2
-1.5
-1
-0.5
0
0.5
18-24
******
******
-
***
***
)SDS(tnenop
moclacisyhP
Age groups (years)
Age groups (years)
)SDS(tnenop
moclatneM
25-34 35-44 45-54 55-64 65-74 >75
Fig. 2. Linear relationship between age (by subgroups), patient quality of life, physical and mental components [given as a standardised score relativeto the reference Spanish population (SDS)], and sex [female (¤), male (h)]. SDS score is given as a marginal mean (95% CI) estimated by leastsquares and adjusted for center, present pain intensity, and the type of neuropathic pain (in the physical component, adjustment is also made for thebody mass index). *** p < 0.001 with Bonferroni correction for multiple comparisons.
250 R. Galvez et al. / European Journal of Pain 11 (2007) 244–255
item in the questionnaire (Table 1); 51% showed markedor extreme disability for work (score P 7), 47% amarked or extreme disability for social life (score P 7),and 42% had the same degree of disability for family life(score P 7). Thirty-eight percent of subjects reportedmarked or extreme stress (score P 7), and 19% reportedreceiving no or little social support (score P 30). Dis-ability was significantly more marked for work thanfor other disability areas assessed by the questionnaire(p < 0.0001, Table 1).
After adjustment for confounding variables, the menshowed significantly greater family disability and per-ceived stress compared with the women (p < 0.05 andp < 0.01, respectively; Table 4) regardless of type of pain,pain severity or patient age, despite the significantlygreater social support received by the men than by thewomen (p < 0.05). Although the level of social support
reported by MP and NeP patients was similar, regardlessof sex, age, or pain severity, the former patients showed asignificantly greater disability than the latter in the totalscale score and in each of the individual scale items(p < 0.001 in all cases). Perceived stress was also signifi-cantly higher in MP patients (p < 0.001, Table 4). Thedisability scale scores of patients with NeP were substan-tially higher than those of the normative scores, indicat-ing their greater disability compared with thepopulation without neuropathic pain.
Disability (overall and per item) and perceived stresswere significantly associated with pain intensity at thetime of scale administration, regardless of the type ofpain, sex, or age of patients (p < 0.001 in all cases; Table4). The association was strongest for patients with terri-ble or severe pain, although those with bothersome painalso showed higher disability scores than did patients

Fig. 3. Physical and mental components of patient quality of life [given as a standardised score relative to the reference Spanish population (SDS)],by mean pain intensity in the previous week, categorised as mild, moderate, and severe. SDS score is given as a marginal mean (95% CI) estimated byleast squares and adjusted for center, sex, age, and type of neuropathic pain.
Table 4Scores in the Sheehan disability scale (ShDS) observed at baseline in patients recruited in the DONEGA study, broken down by subgroups accordingto sex, type of pain (neuropathic pain or neuropathic and nociceptive mixed pain) and age stratum
Subgroup Sheehan disability scale
Item 1(work)
Item 2(social life)
Item 3(family life)
Total score(3 items)
Item 4(perceived stress)
Item 5(social support)
Sex
Men (n = 557) 6.0 (5.7–6.2) 5.6 (5.3–5.8) 5.0 (4.7–5.3) 16.5 (15.8–17.3) 4.7 (4.4–4.9) 68.1 (65.2–70.9)e
Women (n = 877) 6.0 (5.8–6.2) 5.8 (5.5–6.0) 5.5 (5.3–5.7)d 17.3 (16.7–17.9) 5.3 (5.0–5.5)c 63.6 (61.4–65.8)
Type of pain
NPa(n = 603) 5.5 (5.2–5.7) 5.2 (4.9–5.5) 5.0 (4.7–5.2) 15.6 (14.9–16.3) 4.6 (4.3–4.9) 64.9 (62.2–67.6)Mixedb(n = 856) 6.4 (6.1–6.6)c 6.1 (5.8–6.3)c 5.6 (5.4–5.8)c 18.0 (17.4–18.6)c 5.4 (5.1–5.6)c 65.6 (63.3–68.0)
Present pain intensity in SF-MPQ F = 20.4(p < 0.001)
F = 20.3(p < 0.001)
F = 28.6(p < 0.001)
F = 27.1(p < 0.001)
F = 21.6(p < 0.001)
F = 1.4(p = 0.229)
No pain (n = 72) 5.3 (4.5–6.1) 5.3 (4.5–6.1) 4.7 (3.9–5.4) 15.2 (13.0–17.4) 5.3 (4.5–6.1) 66.2 (58.0–74.4)Mild (n = 394) 5.2 (4.8–5.5) 4.8 (4.5–5.2) 4.3 (3.9–4.6) 14.3 (13.3–15.2) 4.1 (3.7–4.4) 65.0 (61.5–68.5)Bothersome (n = 710) 5.9 (5.6–6.1) 5.6 (5.4–5.9) 5.3 (5.1–5.6) 16.8 (16.2–17.5) 5.0 (4.7–5.2) 64.2 (61.7–66.7)Severe (n = 172) 7.3 (6.8–7.8) 7.1 (6.7–7.6) 6.9 (6.4–7.4) 21.3 (20.0–22.7) 6.4 (5.9–6.9) 66.5 (61.5–71.5)Terrible (n = 86) 8.3 (7.5–9.0) 7.7 (6.9–8.4) 7.8 (7.1–8.5) 23.7 (21.7–25.8) 7.2 (6.5–8.0) 73.6 (66.0–81.2)
Values are given as mean (95% CI). Non-significant differences except as noted.SF-MPQ = Short-Form McGill Pain Questionnaire.Mean values calculated by least squares and adjusted for age, participating center, mean pain intensity in the previous week, sex, and type of pain.
a NP, neuropathic pain alone.b Mixed = Neuropathic + inflammatory pain, 95%. CI = 95% confidence interval.c p < 0.001.d p < 0.01.e p < 0.05 between groups in each category.
R. Galvez et al. / European Journal of Pain 11 (2007) 244–255 251
reporting no or mild pain, with significant or close-to-significant differences (Table 4). The association of dis-ability with pain intensity was independent of the socialsupport received, with very similar levels of social sup-port reported by the different pain intensity subgroups.
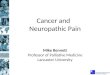
Disability significantly increased with higher meanpain intensity in the previous week (Fig. 4) in both
NeP and MP patients, mainly among those with severepain. In MP patients, total and per item disability scoreswere significantly higher among patients who rated painintensity in the previous week as moderate or severe.Perceived stress also increased with pain intensity, andthis increase was significantly higher in MP than inNeP patients in the subgroups with moderate [4.9

0
5
10
15
20
25
30
100,0 <p
100,0 <p
***
***
10,0 <p
10,0 <p
0
2
4
6
8
10
100,0 <p
100,0 <p
***
***
10,0 <p
50,0 <p
†
0
2
4
6
8
0
2
4
6
8
1010
100,0 <p
100,0 <p
***
***
100,0 <p
*
0
2
4
6
8
0
2
4
6
8
1010
100,0 <p
100,0 <p
†***
1,0 <p
100,0 <p
Tot
al S
DS
(3 it
ems)
ytisnetniniaP
dliM etaredoM ereveS
SDS
– So
cial
life
ytisnetni niaP
dliM etaredoM ereveS
SDS
– W
ork
ytisnetniniaP
dliM etaredoM ereveS
SDS
– F
amily
life
ytisnetniniaP
dliM etaredoM ereveS
Fig. 4. Total and per item score in Sheehan Disability Scale (ShDS) by type of pain [neuropathic (n) or mixed, neuropathic and nociceptive (d)] andpain intensity in the previous week [mild (<40), moderate (P40 and <70) and severe (P70)]. Score is given as a marginal mean (95% CI) estimated byleast squares and adjusted for center, present pain intensity, age, and sex. +p < 0.1; * p < 0.05; *** p < 0.001 between groups with Bonferronicorrection for multiple comparisons. Within-group significance level is inserted in the plot.
252 R. Galvez et al. / European Journal of Pain 11 (2007) 244–255
(4.5–5.4) vs. 3.9 (3.4–4.3); p < 0.001] and severe [5.6(5.3–5.9) vs. 5.0 (4.7–5.4); p < 0.05] intensity. In con-trast, there were no differences in social support levelaccording to either type of pain or pain intensity.
Fig. 5 shows the relationship between physical or men-tal quality of life (expressed as standardised score relativeto Spanish population norms) and the degree of disabilityas rated by the ShDS questionnaire, with patients distrib-uted by type of pain. Scores of patients with MP weremore divergent from those of the Spanish normative pop-ulation and were significantly lower than those of NePpatients, especially when the disability was moderate-to-extreme. However, no linear association was observedbetween quality of life summary component scores andthe severity of disability. Patients with moderate disabil-ity showed the worst (poorest) quality of life scores, withno differences among the other severity groups.
4. Discussion
The DONEGA study (Galvez et al., 2004b; Galvezand the Spanish team for Study of Neuropathic Pain,
2004a) enrolled a consecutive sample of patients withneuropathic or mixed pain undergoing treatment understandard clinical practice. As a result, the series can beconsidered representative of patients with the underlyingdiseases most commonly associated with NeP and toMP who are treated in specialised care centres in Spain.
4.1. Health-related quality of life
Patients with persistent pain experience work disabil-ity and activity limitation with a substantial impact ontheir social functioning and roles (Nicholson andVerma, 2004; Gureje et al., 1998; McWilliams et al.,2003; Harris et al., 2003). In addition to disability, theseconditions are associated with a poor HRQoL in boththe physical and mental dimensions spheres (Galeret al., 2000; Meyer-Rosberg et al., 2001b; Schmader,2002; Mauskopf et al., 1994). After adjusting for con-founding variables and using standardised scores withrespect to the normative population, the results of thisstudy show that NeP or MP is associated with impairedHRQoL, and that this impairment is substantiallygreater in young male patients and in most patients

-2
-1
0
-2
-1.5
-1
-0.5
0
0.5
* * ** *
+
-2
-1
0
-2
-1.5
-1
-0.5
0
0.5
* * ** **
*
)SDS(
tnenopmoclacisyh
P
Groups by disability
No Moderate Extrem Mild Marked
)SDS(
tnen opmoclatne
M
Groups by disability
No Moderate Extrem Mild Marked
Fig. 5. Relationship between patient quality of life, physical and mental components [given as a standardised score relative to the reference Spanishpopulation (SDS)], and the degree of disability according to Sheehan Disability Scale [no disability (total score, 0–2 points) , mild (3–9 points),moderate (10–18 points), marked (19–27 points), and extreme disability (28–30 points)], broken down by type of pain; neuropathic (n) or mixed pain(d). SDS score is given as a marginal mean (95% CI) estimated by least squares and adjusted for center, pain intensity (present and in the past week),age, sex, previous analgesic treatment, and time since diagnosis. *** p < 0.001; ** p < 0.01; * p < 0.05; +p < 0.1 with Bonferroni correction for between-group multiple comparisons.
R. Galvez et al. / European Journal of Pain 11 (2007) 244–255 253
with MP. Meyer-Rosberg et al. used SF-36 (Meyer-Rosberg et al., 2001a,b) and found an impairedHRQoL in patients with NeP, fully consistent withthe present findings using the abridged version of thesame instrument (SF-12). Rowbotham et al. (1998),Backonja et al. (1998), Dworkin et al. (2003) and Riceand Maton (2001) also demonstrated the poor qualityof life of NeP patients with diabetic neuropathy orpost-herpetic neuralgia, although always in a clinicaltrial setting, and Benbow et al. (1998) reported thatscores for most dimensions of the Nottingham HealthProfile were significantly worse among patients withNeP of diabetic origin than among diabetics withoutNeP or age- and sex-matched controls. Gore et al.(2004) recently used version 2 of SF-12 in diabeticpatients with NeP, reporting results that were identicalresults to those observed by Benbow et al. and verysimilar to the present findings, although they did notuse standardised scores in relation to a normativepopulation.
The present study demonstrated the poor quality oflife of patients with NeP treated under standard medicalpractice conditions in comparison with their referencepopulation, regardless of the underlying cause of theirpain, confirming that quality of life improvement is animportant treatment goal. Thus, therapy selected forthese patients should be adequately tolerated as well asdelivering effective pain relief (Kalso et al., 1995). Thepatients studied cannot have received optimal treatmentor their NeP was refractory to available treatments,since their pain persisted and led to an impairedHRQoL. As stated by Harden et al., our understandingof NeP has substantially improved in recent years butthe adequate management of NeP remains a challengeto the medical community (Harden and Cohen, 2003).
4.2. Disability
Pain is associated with a very high disability rate, asshown in this study, significantly affecting the three

254 R. Galvez et al. / European Journal of Pain 11 (2007) 244–255
domains evaluated by the Sheehan scale (work, family,and social life), and it causes substantial patient-per-ceived stress. Thus, almost half of the patients in our ser-ies had marked or extreme disability according to theabove scale, as found by authors of the Spanish valida-tion of the Sheehan scale. Our result contrasts with thealmost complete absence of disability among the healthysubjects assessed in the validation study and is similar tothe finding of impaired occupational, social, and familyactivities in around half of their patients with social pho-bia (Sheehan et al., 1996).
A higher disability rate was observed among patientswith MP versus those with NeP alone, and patients withmultiple conditions usually show greater decreases infunctioning and well-being versus those with a single con-dition (Stewart et al., 1989). Disability was clearly associ-ated with pain intensity, so that patients with severe painover the previous week, whether mixed or neuropathic,showed significantly higher scores in the disability scale.Irrespective of type of pain and social support received,disability linearly increased with present pain intensity.On the other hand, the men reported greater social sup-port than did the women, while the women experienceda more marked level of stress and disability in family lifeas a result of their pain. These findings may be attribut-able to the specific roles of men and women still prevail-ing in the Spanish Society. Surprisingly, although the agewas related to quality of life, it was not associated withdegree of disability. This appears to be because painwas the main cause of disability, regardless of other fac-tors, as confirmed by the relationship found between painintensity and degree of disability.
No studies could be found that assess disability inpatients with NeP or MP using the Sheehan scale, ham-pering comparison of our results with the disabilityfound in other types of patient, such as those with psychi-atric disorders (Leon et al., 1997; Kennedy et al., 2002).Nevertheless, the marked severity of the disability of ourseries is consistent with numerous many reports in the lit-erature of decreased function associated with chronicpain (Harden and Cole, 1998; Kanazi et al., 2000; Sulli-van et al., 2005; Nicholson, 2003). Thus, enhancing dailyfunctioning and well-being is an increasingly advocatedgoal in the treatment of patients with chronic conditions,especially pain, which accounts for a substantial part ofhealthcare expenditure (Berger et al., 2004).
4.3. Limitations
The main limitation of this cross-sectional evaluationis that the study was not originally designed to assess theimpact of NeP or MP on patient functioning orHRQoL. This was a secondary objective of the evalua-tion of gabapentin effectiveness in pain relief and otherhealth outcomes under standard clinical practice condi-tions. However, the study offered a representative range
of underlying diseases and participating centres/special-ties as well as assessing patients under standard clinicalpractice conditions, for the first time in such a large sam-ple of patients.
A further possible limitation is that quality of life wasmeasured using a generic questionnaire, rather than aspecific questionnaire for pain or neuropathic pain. Onthe other hand, most authors measuring the quality oflife in patients with neuropathic pain have used genericquality of life instruments such as the SF-36, SF-12, orthe Nottingham Health Profile, which has shown accept-able psychometric properties for use in patients withneuropathic pain (Meyer-Rosberg et al., 2001b; Mau-skopf et al., 1994; Backonja et al., 1998; Hamza et al.,2000). In the present study, reliability and validity ofthe SF-12 questionnaire were found to be acceptable(Rejas et al., 2005), supporting the use of this instrumentin this type of patient.
The Sheehan disability scale was initially developed toassess functional impairment in patients with mental dis-orders such as anxiety, phobia, or depression. However,neither the author of the instrument nor people responsi-ble for validation of its Spanish version have ever contra-indicated its use in other disease settings, and patientswith neuropathic pain have associated mental disorders,including anxiety and depression (Nicholson and Verma,2004; McWilliams et al., 2003; Harris et al., 2003; Ben-bow et al., 1998). To our knowledge, this is the first appli-cation of this scale to examine functioning in patientswith neuropathic or mixed pain in our health setting,making the results of special interest, although furtherresearch is required to support our findings.
Taking the above limitations into account, it can beconcluded that patients with neuropathic or mixed painshow a poor physical and mental HRQoL under condi-tions of standard clinical practice in comparison with thegeneral population, and suffer a high severity of social,family, and occupational disability. Being young and maleand presence of mixed pain are associated with poorerquality of life and disability scores. Severe pain, low overallhealth rating, increased work disability, and poor familyand social functionality, together with a significant impacton quality of life, represent a substantial burden forpatients with NeP or MP syndromes. Therefore, a primarygoal of the health care for these patients is optimisation oftheir daily life functions, well-being and quality of life.
Acknowledgements
Authors wish to thank all investigators participatingin the DONEGA study for their participation in the datacollection and analysis and Dr Teresa Leon of the Med-ical Unit of Pfizer Espana, for her support in the designand scientific supervision of the research. This study wassupported by an unrestricted grant from Pfizer Espana.

R. Galvez et al. / European Journal of Pain 11 (2007) 244–255 255
References
Backonja M, Beydoun A, Edwards KR, Schwartz SL, Fonseca V, HesM, et al. Gabapentin for the symptomatic treatment of painfulneuropathy in patients with diabetes mellitus: a randomizedcontrolled trial. JAMA 1998;280:1831–6.
Benbow SJ, Wallymahmed ME, MacFarlane IA. Diabetic peripheralneuropathy and quality of life. QJM 1998;91:733–7.
Berger A, Dukes EM, Oster G. Clinical characteristics and economiccosts of patients with painful neuropathic disorders. J Pain2004;5:143–9.
Bobes J, Badıa X, Luque A, Garcıa M, Gonzalez MP, Dal-Re R yel Grupo de Validacion en Espanol de los Cuestionarios deEvaluacion de la Fobia Social. Validacion de las versiones enespanol de los cuestionarios Liebowitz Social Anxiety Scale,Social Anxiety and Distress Scale, y Sheehan Disability Inven-tory para la evaluacion de la fobia social. Med Clin (Barc)1999;112:530–8.
Cruccu G, Anand P, Attal N, Garcıa-Larrea L, Haanpaa M, Jorum E,et al. EFNS guidelines on neuropathic pain assessment. Eur JNeurol 2004;11:153–62.
Dworkin RH, Corbin AE, Young Jr JP, Sharma U, LaMoreaux L,Bockbrader H, et al. Pregabalin for the treatment of postherpeticneuralgia: a randomized, placebo-controlled trial. Neurology2003;60:1274–83.
Galer BS, Henderson J, Perander J, Jensen MP. Course of symptomsand quality of life measurement in complex regional painsyndrome: a pilot survey. J Pain Symptom Manage2000;20:286–92.
Galvez R, the Spanish team for Study of Neuropathic Pain. Pharma-coepidemiologic and multidisciplinary study of gabapentin inneuropathic pain. Neuropathic Pain. Changing Paradigms inDiagnosis and Treatment. An International Congress of NeuPSIG.Madrid; 2004a [abstract].
Galvez R, Ribera MV, Rejas J, Masramon X, Ruiz M. Chronicneuropathic pain (NeP) impact on patient quality of life anddisability: results from the DONEGA study. Value Health2004;7:794 [abstract PNL23].
Gandek B, Ware J, Aaronson N, Apolone G, Bjorner J, Brazier J,et al. Cross-validation of item selection and scoring for the SF-12health survey in nine countries: result from the IQUOLA project. JClin Epidemiol 1998;51:1171–8.
Gore M, Brandenburg N, Dukes E, Hoffman D, Zinder-Chavis A, taiK. Pain severity in diabetic peripheral neuropathy (DPN) impactspatients functioning, symptom levels of anxiety and depression,and sleep. J Pain 2004;5(Suppl. 1):112.
Gureje O, von Korff M, Simon GE, Gater R. Persistent pain and well-being: a World Health Organization study in primary care. JAMA1998;280:147–51.
Hamza MA, White PF, Craig WF, Ghoname ES, Admed HE, ProctorTJ, et al. Percutaneous electrical nerve stimulation: a novelanalgesic therapy for diabetic neuropathic pain. Diabetes Care2000;23:365–70.
Harden N, Cohen M. Unmet needs in the management of neuropathicpain. J Pain Symptom Manage 2003;25:S12–7.
Harden RN, Cole PA. New developments in rehabilitationof neuropathic pain syndromes. Neurol Clin 1998;16:937–50.
Harris S, Morley S, Barton SB. Role loss and emotional adjustment inchronic pain. Pain 2003;105:363–70.
Haythornthwaite JA, Benrud-Larson LM. Psychological assessmentand treatment of patients with neuropathic pain. Curr PainHeadache Rep 2001;5:124–9.
IASP Task Force in Taxonomy. Pain Terms: A Current List withDefinitions and Notes on Usage. In: Merksey H, Bogduk N,editors. Classification of chronic pain syndromes and definitions of
pain terms. Second Edition. Seattle, Washington: IASP Press; 1994.p. 206–13.
Jensen TS, Gottrup H, Sindrup SH, Bach FW. The clinical picture ofneuropathic pain. Eur J Pharmacol 2001;429:1–11.
Kalso E, Tasmuth T, Neuvonen PJ. Amitryptiline effectively relievesneuropathic pain following treatment of breast cancer. Pain1995;64:293–302.
Kanazi GE, Johnson RW, Dworkin RH. Treatment of postherpeticneuralgia: an update. Drugs 2000;59:1113–26.
Kennedy BL, Lin Y, Schwab JJ. Work, social, and family disabilitiesof subjects with anxiety and depression. South Med J2002;95:1424–7.
Leon AC, Olfson M, Portera L, Farber L, Sheehan DV. Assessingpsychiatric impairment in primary care with the Sheehan DisabilityScale. Int J Psychiat Med 1997;27:93–105.
Mauskopf J, Austin R, Dix L, Berzon R. The Nottingham healthprofile as a measure of quality of life in zoster patients: convergentand discriminant validity. Qual Life Res 1994;3:431–5.
McWilliams LA, Cox BJ, Enns MW. Mood and anxiety disordersassociated with chronic pain: an examination in a nationallyrepresentative sample. Pain 2003;106:127–33.
Melzack R. The short-form McGill pain questionnaire. Pain1987;30:191–7.
Meyer-Rosberg K, Burckhardt CS, Huizar K, Kvarnstrom A, Nordf-ors LO, Kristofferson A. A comparison of the SF-36 andNottingham Health Profile in patients with chronic neuropathicpain. Eur J Pain 2001;5:391–403.
Meyer-Rosberg K, Kvarnstrom A, Kinnman E, Gordh T, NordforsLO, Kristofferson A. Peripheral neuropatic pain: a multidimen-sional burden for patients. Eur J Pain 2001;5:379–89.
Nicholson B, Verma S. Comorbidiries in chronic neuropathic pain.Pain Med 2004;5:S9–S27.
Nicholson BD. Diagnosis and management of neuropathic pain: abalanced approach to treatment. J Am Acad Nurse Pract2003;15:S3–9.
Rejas J, Masramon X, Ruiz M. The MOS-short-form-12 (SF-12) as ameasure of health-related quality of life in Neuropathic Pain (NeP)patients: reliability, concurrent and discriminant validity. ValueHealth 2005;8:A142 [abstract].
Rice AS, Maton S. Postherpetic Neuralgia Study Group. Gabapentinin postherpetic neuralgia: a randomised, double blind, placebocontrolled study. Pain 2001;94:215–24.
Rowbotham M, Harden N, Stacey B, Berstein P, Magnus-Miller L.Gabapentin for the treatment of postherpetic neuralgia: a ran-domized controlled trial. JAMA 1998;280:1837–42.
Schmader KE. Epidemiology and impact on quality of life ofpostherpetic neuralgia and painful diabetic neuropathy. Clin JPain 2002;18:350–4.
Sheehan DV, Harnett-Sheehan K, Raj BA. The measurement ofdisability. Int Clin Psychopharmacol 1996;11:S89–95.
Stewart AL, Greenfield S, Hays RD, Wells K, Rogers WH, Berry SD,et al. Functional status and well-being of patients with chronicconditions. Results from the medical outcomes study. JAMA1989;262:907–13.
Sullivan MJ, Lynch ME, Clark AJ. Dimensions of catastrophicthinking associated with pain experience and disability in patientswith neuropathic pain conditions. Pain 2005;113:310–5.
The Pain in Europe: a report. En URL: http://www.painineurope.com(accessed on April 26th, 2005).
Vilagut G, Ferrer M, Rajmil L, Rebollo P, Permanyer-Miralda G,Quintana JM, et al. Alonso J por los investigadores de la Red-IRYSS. El cuestionario de salud SF-36 espanol: una decada deexperiencia y nuevos desarrollos. Gac Sanit 2005;19:135–50.
Ware Jr JE, Kosinski M, Keller SD. A 12-item short-form healthsurvey: construction of scales and preliminary tests of reliabilityand validity. Med Care 1996;34:220–33.