Embed Size (px)
Citation preview

JOURNAL OF CLINICAL MICROBIOLOGY, Feb. 1992, p. 401-4060095-1137/92/020401-06$02.00/0Copyright X 1992, American Society for Microbiology
Cross-Infection Risks Associated with Current Procedures for UsingHigh-Speed Dental Handpieces
DAVID L. LEWIS'* AND ROBERT K. BOE2Faculty ofEcology, University of Georgia, Athens, Georgia 30602,1 and 4721 Chamblee-Dunwoody Road, Building 400,
Dunwoody, Georgia 303382Received 31 October 1991/Accepted 2 December 1991
When a dye solution used to simulate patient material was either injected into high-speed dental handpiece(drill) waterlines or applied to the equipment externally, internal air turbine chambers became contaminated.These chambers served as a reservoir of the material, which was slowly dislodged by air expelled duringsubsequent handpiece operation and which was diluted by water spray used for cooling the drilling surface.Considering the fact that patient materials could reside in internal parts of the equipment that are not usuallydisinfected and that the material may be subsequently sprayed into cuts and abrasions in the oral cavity, thecommon approach to reprocessing handpieces (external wiping in combination with flushing) may poseunacceptably high risks to those individuals treated soon after infected patients. Therefore, unless reliable dataon cross-infection frequencies are obtained and prove it unnecessary, heat-treating high-speed handpiecesbetween each patient should be considered an essential component of standard procedures whenever universalprecautions are practiced in dentistry.
Epidemiological studies in dentistry have historically fo-cused on practices operated by dentists infected with hepa-titis B virus (HBV) or human immunodeficiency virus (HIV)(4, 9, 12, 13, 19, 24). The risk of dentist-to-patient transmis-sion of such blood-borne diseases appears to be extremelysmall. Infected dentists, however, may only rarely be mem-bers of patient-to-patient cross-infection clusters; therefore,historical studies involving infected dentists cannot be usedto accurately assess the extent of cross-infection problems indentistry. Because dentistry potentially exposes much of thepopulation to blood-to-blood contact with infected patientsand because of the current lack of data on the risks ofcross-infection, a careful evaluation of the likelihood thatdental equipment may transmit infections is needed.
Unless adequately disinfected, a wide variety of dentalequipment may pose unacceptable risks of cross-infection.Handpieces and their attachments, including prophyanglesattached to slow-speed motors for cleaning and polishingteeth, and high-speed motors and their burs used for drillingare particularly prone to patient contamination. This studyfocuses on one potential source of infection, the high-speedhandpiece, which has been referred to as the "weak link inthe chain of sterility" (20). Better infection-control measuresthan chemical treatment alone are currently available forhandpieces and their attachments to provide a greater assur-ance that they do not contribute to the spread of diseases.These measures include either autoclaving or dry heattreatment in conjunction with cleaning and chemical disin-fection. However, achieving adequate levels of disinfectionis complicated by a number of factors associated with thehandpiece design. The equipment contains lumens and crev-ices, which collect infective patient materials and are diffi-cult to properly clean and disinfect. Moreover, internalhandpiece components are more prone to malfunction afterfrequent sterilization at high temperatures (29).
Autoclavable handpieces have been manufactured sincethe early 1980's; an American Dental Association survey in
* Corresponding author.
1989 indicated that about half of the dentists practicing in theUnited States possessed autoclavable handpieces (28). How-ever, even though they are widely used, the majority ofgeneral practice dentists do not autoclave them betweeneach patient (3, 5, 11, 14, 15).
Guidelines published by the Centers for Disease Control(CDC) (Atlanta, Ga.) in 1986 suggest that an external treat-ment of dental handpieces with a germicide solution is anacceptable, albeit not the best, form of disinfection (23).However, studies as early as 1977 indicate that germicidetreatment may not adequately disinfect the equipment (21).Additionally, some research has shown that spores insidehigh-speed handpieces may survive autoclaving unless theequipment is also internally treated with chemical disinfec-tants (8). Reliance on American Dental Association andCDC recommendations regarding chemical disinfection inlieu of heat treatment has prevailed throughout the dentalprofession despite the lack of data demonstrating that exter-nal disinfection is effective in controlling cross-infection.Thus, dentists have depended primarily on flushing water-lines to rid internal areas of infectious agents. This approachis supported by CDC guidelines (23), which include a rec-ommendation for holding handpieces over a sink and runningthe equipment before each use in order to discharge patientmaterials. As a further precaution, check valves are recom-mended for older dental units to minimize the amount ofpatient material that might be retracted into waterlines andthen transferred to other patients (2).Much of the concern about the potential for dental hand-
pieces to transmit infections has focused on pathogenicbacteria that may proliferate in waterlines (1, 2, 18, 22). Asis the case with all habitable surfaces in prolonged contactwith contaminated water, waterlines in and leading to high-speed dental handpieces provide an environment that ishighly conducive to biofilm formation. Such attached micro-organisms are unlikely to be readily flushed out and mayentrap and periodically shed pathogens during high-speedhandpiece operation. Viruses, on the other hand, do notreproduce outside of their hosts and therefore cannot prolif-erate in waterlines. Consequently, viral transmission is more
401
Vol. 30, No. 2
on Novem
ber 4, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from
on Novem
ber 4, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from
on Novem
ber 4, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from
on Novem
ber 4, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

402 LEWIS AND BOE
DH1.0 cm
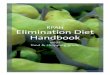
B AOWO ""'AlFIG. 1. Simplified diagram of a high-speed dental handpiece illustrating the chuck insert (CI) for securing the bur (B) driven by air turbines
located in the turbine chamber (TC) of the drill head (DH). Turbines are turned by air entering the high-speed handpiece through the mainair inlet (MAI) and entering the turbine chamber through the main air inlet line (MAIL). Air exits the chamber primarily through the main airoutlet line (MAOL) to the main air outlet (MAO) of the high-speed handpiece. Some turbine air escapes through lumens around the bur andaround the chuck insert. Dye was injected into the water inlet (WI) located near the air inlet (Al). Water and air exiting at the water outlet(WO) and air outlet (AO) cool the bur.
likely to be of concern when significant amounts of patientmaterials remain in the lumens and crevices of handpiecesand of their attachments, as well as on internal mechanisms.Because many of these sites are isolated from waterlines,flushing should not be expected to rid them of contamina-tion. Considering the nature of the various areas potentiallyserving as fomites, we can separate cross-infection concernsassociated with dental handpieces into two distinct catego-ries: (i) pathogenic bacterial (and possibly fungal) growth inwaterlines and (ii) contamination of lumens, crevices, andairways with patient materials harboring any kinds of patho-gens, including viruses.
This study specifically pertains to the latter category ofproblems. However, when contamination is dislodged fromalmost any area of a high-speed handpiece, it may be dilutedas it becomes incorporated into the air-water spray used tocool the bur during drilling. Therefore, our experimentsincluded addressing the effect of cooling water spray oncontamination dilution rates.
MATERIALS AND METHODS
The amount of time required to expel contamination inwaterlines was calculated by using a dye-extinction curve forapproximately 0.1 ml of commercial food coloring concen-trate solution (Kroger red dye, Cincinnati, Ohio). To assesscontamination problems originating with waterlines, dyeconcentrate solution was injected with a hypodermic syringeinto handpiece waterlines at the handpiece water inlet (Fig.1). In other experiments, high-speed handpieces were ex-posed to the dye solution externally to simulate contamina-tion problems associated with external surfaces of hand-pieces as they operate in the oral cavity. This wasaccomplished by switching the handpiece on and off in 1-sintervals for 25 s and contacting the bur with the surface of
50 ml of dye solution in a tilted 250-ml beaker. Care wastaken not to submerge the handpiece head.Dye was sampled in the water spray ejected from hand-
pieces and the spray was obtained either by running theequipment continuously or by switching air and water flowson and off at 1- to 5-s intervals. Water flow rates wereapproximately 1.0 ml/s. Effluent samples were collectedfrom water spray that had been expelled into glass-stopperedtest tubes for up to 9 min. Sample volumes were amendedwith water to a total volume of 5 ml.
One-milliliter samples of the same dye solution used fortreating handpieces were withdrawn with a 5-ml hypodermicsyringe equipped with a 20-gauge needle. The dye solutionwas then partially ejected from the syringe to ensure that theneedle was completely filled with dye. A silicone rubber bulbcontaining 5 ml of water was then punctured, and the needlewas quickly withdrawn so that the contents were contam-inated in a manner similar to an accidental percutaneousexposure. The needle entered the water contained in thebulb to a distance of about 0.5 cm.Dye concentrations were measured with a Perkin-Elmer
Lambda 4C Spectrophotometer at 210 nm, by using waterfrom dental unit waterlines as reference blanks. Dilutionrates were measured with a minimum of three trials each forthree handpiece models manufactured by Kinetic Instru-ments, Inc. (Bethel, Conn.) and for three models manufac-tured by Midwest Dental Products Corporation (Des Plains,Ill.). Only one model manufactured by Star Dental Products(Lancaster, Pa.) was tested, and dilution rates were mea-sured with it in three trials. Experiments were performed byusing dental units both corrected and uncorrected for waterretraction. Tests were not done to ensure that check valveswere functioning properly at the time the experiments wereconducted. Multiple trials were carried out with each hand-piece to detect any dye washed out of air turbine chambers
J. CLIN. MICROBIOL.
on Novem
ber 4, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

DENTAL HANDPIECE CONTAMINATION 403
'c 6.5,_ 4.5 U U
=- 2.5% 0.5
-1.5 O (a) (b)-3.5-5.5 - .
0 5 10 15 20Time (sec.)
FIG. 2. Initial exponential dilution rates observed after dye wasinjected into handpiece waterline inlets and after effluent sampleswere collected as dye solution was expelled during high-speedhandpiece operation. The ordinate axis is the natural logarithm ofamounts of the dye solution injected into the handpiece remaining in1-s samples of water spray expelled by the high-speed handpiece.Plots (a) and (b) represent data using handpieces from differentmanufacturers, and each point represents a single dye sample takenat time t.
5
o \4\
0
Q EU
0 2 4 6 8 10 12Time (sec.)
FIG. 3. Slow-elimination dilution rates observed after dye wasinjected into handpiece waterline inlets and after effluent sampleswere collected as dye solution was expelled during high-speedhandpiece operation. The ordinate axis is the logarithm of amountsof the dye concentrate remaining in 1-s samples of water sprayexpelled by the high-speed handpiece. Solid and hollow symbolsindicate duplicate trials using the same handpiece, and each pointrepresents a single dye sample taken at time t. Means ± SD for theslow-elimination rates were 4.4 ± 1.5 (*) and 3.4 ± 1.1 (E) ±l s-1.
after the equipment was disconnected and cleaned. Becausethe amounts of dye collected in air turbine chambers couldinvariably be easily seen with the unaided eye when thechambers were flushed, no effort was made to determine itsconcentrations spectrophotometrically.Dye dilution data were plotted on logarithmic plots to
illustrate that the dilution rates were exponential. Because itwas not usually possible to perform replicate trials usingeven the same handpiece such that starting levels of dyecontamination were the same in different trials, data fromseparate dilution trials could not be averaged and presentedin the same figure. Also, so that any slight differencesobserved in dilution rates among different models would notbe construed to imply that one model may have any signif-icant advantage over another or that any manufacturer'sequipment has advantages over another on the basis of ourtests, equipment models were not identified with their cor-responding data in the presentation of our results.
RESULTS
Dilution rates of dye solution injected into water inlets orapplied externally to high-speed handpieces were biphasic,beginning with rapid, exponential dilution (Fig. 2). This wasfollowed by an almost constant elimination of trace quanti-ties of dye (Fig. 3 and 4), which originated from externalsurfaces and from air turbine areas contaminated by waterspray. The rates of decrease in dye concentrations during thelatter phase were extremely slow, which is consistent with aslow-leaking reservoir of very high dye concentrations rela-tive to those in the expelled cooling water.The source of dye in the slow-elimination phase was
evident because dye solution could be seen collecting onexterior handpiece surfaces and coming out of the top ofhandpiece heads with the unaided eye. Rinsing external dyecontamination from handpieces had no detectable effect onthe amounts of dye expelled during the slow-eliminationphase. Additionally, after disconnecting handpieces, copi-ous quantities of dye were flushed from air turbine chambers
even after the handpieces had been operated 10 min or more.Therefore, air turbine chambers were the primary source ofwater-spray recontamination during the slow-eliminationphase. It was evident that some of the water sprayed aroundburs was either forced into the handpiece heads by waterspray pressure or sucked into turbine chambers, perhapswhen turbines rotated momentarily after the air flow wasswitched off. Air turbine chambers became contaminatedregardless of whether the dental units were corrected withcheck valves to minimize water retraction and regardless of
6
r, S. 5C3CA 4
043
20-¼41
o
U
0 2 4 6 8 10Time (min.)
FIG. 4. Slow-elimination dilution rates obtained after a high-speed handpiece was run with the bur in contact with dye concen-trate solution for 25 s and then 1-s effluent samples were collected asdiluted dye solution was ejected during high-speed handpiece oper-ation. These data are from a high-speed handpiece from a differentmanufacturer than for the handpiece used in Fig. 3, and it wasoperated for longer periods of time. Each point represents a singledye sample taken at time t. The mean + SD for the slow-eliminationrates was 2.8 ± 1.1 j±l s-1.
VOL. 30, 1992
on Novem
ber 4, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

404 LEWIS AND BOE
the method of dye application (injection into waterlines orexternal application).By using the same dye solution used to treat handpieces,
we determined that the mean amount of dye released by a20-gauge needle per single simulated percutaneous exposure(± standard deviation [SD]) was 62.3 ± 21.9 ,ul (12 trials). Bycomparison, 2.7 ± 1.8 ,ul of dye per s (mean ± SD, four trialswith three handpieces from two manufacturers) was expelledin handpiece water spray during the slow-elimination phasefor up to 9 min when dye was either injected into handpiecewaterline inlets or contacted externally (Fig. 3 and 4). Whena minimum of three trials were run for each of 10 handpieces,water flushed from all air turbine chambers after the hand-pieces were disconnected exhibited visible amounts of dyeas it washed out the handpiece air outlet. Therefore, airturbine chambers invariably became contaminated with highconcentrations of dye and acted as reservoirs of contamina-tion, which slowly leaked out during handpiece operation.By disinfecting handpieces both internally and externally,
risks of cross-infection posed by the slow-decontaminationphase could be eliminated. When waterline contaminationextending beyond the handpiece is not a factor, the timerequired to effectively flush handpieces could be basedsolely on contamination levels and on the initial exponentialdilution rates observed with waterlines. On the basis of thisapproach, we calculated the time required to expel contam-ination suspended in waterlines by using the slopes ofnatural logarithmic dye-extinction plots. Because the initialdilution rates were reasonably exponential (r2 = 0.89 + 0.16[mean ± SD] for handpieces from three manufacturers),exponential rate coefficients, k1, were calculated using theequation k1 = [ln (C)I(Co)]It, where C is the dye concentra-tion expelled by the handpiece at time t and CO is the initialdye concentration in discharged water. Values of k1 for thehandpieces were 1.9 ± 1.6 s-1 (mean ± SD) and ranged from-0.89 to -3.8 s-1 for handpieces from three manufacturers.With the following equation, k1 values could be used tocalculate the time required to reduce the concentration ofcontamination by one half (to.5): to05 = 0.693/kl.The time that must be exceeded to flush a waterline of
freely suspended material (X,) could be determined using thefollowing equation: X, = ln [(B,)I(B0)]1k1, where Bo is theinitial concentration of the contaminant and B, is one celldivided by the total volume of water contained in the line. If,for example, 0.05 ml of fluid containing 50 cells/ml wasretracted into the volume of water contained in the hand-piece (0.094 ml), it would require 1.03 s to flush the hand-piece (determined on the basis of a k1 value of 0.89 s-1).To illustrate the importance of using an appropriate dilu-
tion rate expression, we determined the amount of timerequired to flush the handpiece when exponential dilution isdisregarded. This was calculated as the volume of watercontained in the handpiece (0.094 ml) divided by the waterflow rate (1.1 ml/s), which equaled 0.085 s. Consequently, ittook 12 times longer to effectively flush the level of contam-ination in the above example than was expected solely on thebasis of the water flow rate and the volume of water itcontained. This difference seems insignificant, yet the timerequired to flush a line under exponential dilution is greatlyinfluenced by the value of Bo. If, for example, the dentistdrilled into a pocket of bacterial infection and the shortwaterline inside the handpiece became contaminated to alevel of 10,000 cells per ml, it would take over 90 timeslonger to flush the line than would be expected from thewater flow rate and the volume of water. Extrapolating thisrelationship to a 3-m length of waterline in which this high
level of contamination may occur through continual retrac-tion or bacterial growth, it would take over 3 min tocompletely flush the suspended contamination from theequipment.
DISCUSSION
The mathematical model we presented for predictingdilution rates is applicable to all situations, except whenparticulates adhere to surfaces and are not freely expelledwith fluid. Both slow elimination of contamination fromhandpiece heads and biofilm growth could greatly extend thetime required to completely rid handpieces of suspendeddebris. However, the mathematical model shows that sev-eral minutes of flushing is sufficient for removing even veryhigh concentrations of freely suspended materials when thesource of contamination is confined to the handpiece, al-though the material was not removed nearly so rapidly asone might expect solely on the basis of water flows andvolumes.
Previous studies with dye and bacterial suspensions byCrawford and Broderius (6, 7) did not detect recontamina-tion of the handpiece water spray by air turbine chambers.However, the researchers did not flush the air turbinechambers to detect contamination in that particular area, andtheir method of elucidating the presence of dye in waterlines(placing approximately 0.5 ml of water on white paper)would not detect the low dye concentrations measuredphotometrically in our samples of waterline effluent. Casesof cross-infection will often involve amounts of material notvisible to the unaided eye. Therefore, fully assessing cross-infection mechanisms with dye studies requires consideringeven infinitesimal quantities of the dye tracer.As in the studies by Crawford and Broderius, we have
used bacterial suspensions in conjunction with dye tracers(15). We sometimes failed to detect bacteria inside equip-ment when liquid disinfectant was applied to the equipmentexternally. However, we attributed the absence of bacterialgrowth in samples taken from internal components of exter-nally disinfected handpieces either to the presence of smallamounts of disinfectant carried over to the growth media orto superficial disinfection of microbial aggregates by tracesof disinfectants that may have entered the equipment. In anycase, the difficulties involved in sterilizing microbially con-taminated aggregates with liquid disinfectants are wellknown and provide an ample basis for an argument againstassuming that nonculturability of test microbes in someexperiments means that surface treatment of the equipmenteffectively sterilizes it internally.Because of concentration and temperature gradients, mi-
crobial aggregates may be sterilized only on the surface byany technique designed to either sterilize or disinfect them.Additionally, the same diffusion gradients that protect aggre-gate interior microbes from exposure to biocidal solutionsalso limit their contact with nutrient solutions (16, 17).Consequently, surface-sterilized aggregates can mistakenlyappear to be dead when plated on nutrient agar or suspendedin a nutrient solution. However, when surface-sterilizedaggregates are broken apart by a high-speed handpiece'smoving parts, their viable interiors could be liberated andcause infection. Because misleading efficacy tests of disin-fection or sterilization procedures could result from surfacesterilization of aggregated materials, disinfection efficacytests should always include a postdisinfection step in whichaggregates in grooves and crevices of the equipment are
J. CLIN. MICROBIOL.
on Novem
ber 4, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

DENTAL HANDPIECE CONTAMINATION 405
broken apart by sonication or by mechanical means and thentested to reveal any viable contents.Our experiments indicated that the amount of contamina-
tion escaping handpieces per minute, for periods of timeextending well beyond the brief flushing normally adminis-tered to rid the equipment of internal contamination, wasequivalent to the total volume of fluid injected in multiplesimulated 20-gauge-needle percutaneous exposures. Formany dental procedures, such as minor restorations, riskspresented by patient material-contaminated cooling watermight be similar to risks involved with certain infectionspassed by unprotected oral intercourse; i.e., microbes eithermay be directly taken up through mucosal membranes or
may enter small cuts and abrasions. This is not to say thatthe amount of microbial exposure is the same in both cases,
just that the mode of infection would be the same. However,when the bur is operated invasively to the mucosa or to toothpulp, the effect is more analogous to percutaneous exposurewith a needle. Mechanical pressure applied to a syringeplunger drives fluid out of a needle and into a wound as itpenetrates percutaneously. Likewise, a high-pressure flowof water directed at the cutting edge of a bur drives fluid intovascular systems as the bur cuts through mucosa or pulp.Use of a high-speed handpiece for sectioning teeth duringextraction or for performing root canals is an example ofsuch an invasive procedure. It is in such highly invasiveprocedures that HBV transmission in dentistry has beencorrelated most frequently (12, 13, 24), and most of theconcern of cross-infection should be placed on them. How-ever, with the substantial amounts of blood commonlyproduced even with prophylaxis treatments, the distinctionbetween invasive and noninvasive procedures in dentistry isnot so clear as it is in other fields of medicine.
In a study of 2,006 percutaneous HIV exposures among
1,962 health care workers (10), a total of six seroconversionswere observed. This represents an infection rate of 0.32%per exposed person. The risk of contracting HBV, on theother hand, is within the range of 10 to 35% (10). Therefore,if the risks posed by invasive procedures with contaminatedhigh-speed handpieces are comparable to risks of percuta-neous exposures with needles, several individuals per thou-sand patients treated with invasive procedures soon afterHIV-infected patients are treated could become infected ifthe equipment is not adequately disinfected between eachpatient. An even larger number of patients could be infectedwith HBV under these circumstances.Not all of the contaminated water spray from a high-speed
handpiece would be taken up internally as is the case withfluids left in needle punctures. The overall risks of infectionfor these two types of exposures, however, may be some-
what comparable since the spray may deliver the equivalentfluid volumes of several percutaneous exposures per minute(determined on the basis of our results) and an invasivedental procedure with a high-speed handpiece may last for 30min or longer. Moreover, a needle prick injects materialrather passively compared with a high-pressure jet of water
directed into a sizable, bleeding wound where a tooth isbeing extracted or the pulp invaded. Admittedly, percutane-ous exposure with a needle is not a perfect model forinvasive drilling, perhaps not even a good enough one to
reasonably state whether it over- or underestimates risks ofinvasive dental procedures. Nevertheless, it provides theonly benchmark currently available by which we could even
begin to assess the possible risks for the transmission of HIVand other diseases via invasive procedures performed withcontaminated high-speed dental handpieces.
Considering the facts that material from previous patientscan reside in parts of the equipment that are not usuallydisinfected and that the material may be subsequentlysprayed into cuts and abrasions in the oral cavity, thecommon approach to reprocessing handpieces is inadequate.This concern is ameliorated somewhat because of the rela-tively low incidence of some of the infections of primaryconcern (HBV and HIV), which tends to make the overallrisks of cross-infection for these diseases low at present.However, patient material ejected from handpieces is likelyto pose unacceptably high risks to those particular individ-uals treated soon after infected patients, and common sensewould dictate that risks posed by handpieces should beregarded no differently than other contaminated equipment,such as explorers and scalers, for which the CDC and othershave recommended only heat sterilization.These studies, along with others we cited, suggest that a
significant cross-infection potential exists with high-speedhandpieces whenever they are only externally disinfected.However, to date, not one case of dental equipment medi-ated cross-infection has been confirmed and reported in themedical literature. Either the conclusions of studies indicat-ing the cross-infection potential have been overstated or thecurrent system for detecting and reporting cross-infection indentistry is largely ineffective. Indeed, there is no specificsurveillance system for detecting individuals who may havecontracted any disease from infected dental patients treatedpreviously to them. Moreover, because of the current wide-spread assumption that HBV and HIV transmission throughdentistry is extremely rare, there is little to no incentive forgovernmental agencies to investigate possible cross-infec-tion clusters, especially whenever those clusters include (asthey almost invariably will) individuals with one or morerecognized risk factors. Additionally, because patient cross-infection clusters may only rarely include an infected den-tist, historical studies involving HBV- and HIV-infecteddentists cannot be expected to indicate frequencies of cross-infection. Therefore, we should consider that the currentabsence of reported cross-infection cases in dentistry may bedue more to the lack of an adequate means of detection thanto the universal application of an adequately high level ofinfection control throughout the profession.Only epidemiological studies can ascertain the actual
frequencies at which diseases are transmitted in practice.Appropriate cross-infection studies in dentistry could beaccomplished either (i) by following the rates of seroconver-sions among many hundreds or thousands of patients treatedshortly after infected patients or (ii) by investigating clustersof infected patients. In the latter studies, patients sharingepidemiologically linked microbial strains would conclu-sively represent cross-infection in cases in which the dentistis not infected and in which the patients cannot be epidemi-ologically linked outside the dental practice. Studies by theCDC linking HIV infections in five patients to an infecteddentist in a Florida practice (25-27) represent the first timethat DNA sequencing has been used to elucidate sharedinfections among dental patients. HIV infections are rela-tively rare among the population as a whole, and the rates atwhich the virus undergoes nucleotide sequence changes as itis passed from one patient to the next are very high. Thus,notwithstanding the fact that the HIV studies we proposewould be both expensive and difficult, HIV appears topresent us with an unusual opportunity to ascertain cross-infection frequencies in the practice of medicine. Unlessreliable data on cross-infection frequencies are obtained andprove it unnecessary, thoroughly cleaning and heat-treating
VOL. 30, 1992
on Novem
ber 4, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

406 LEWIS AND BOE
high-speed handpieces between each patient should be con-sidered an essential component of standard procedureswhenever universal precautions are practiced in dentistry. Ifthese steps are taken, the potential for cross-infecting pa-tients with high-speed handpieces will be essentially elimi-nated.
ACKNOWLEDGMENTS
We gratefully acknowledge the support of J. Benjamin Patrick,Athens, Ga., for the use of treatment rooms and equipment and ofGene E. Michaels, University of Georgia, for laboratory space andequipment. Numerous leading researchers, technical experts, andpracticing dental professionals provided invaluable assistance. Thesuggestions of John Young, University of Texas Dental School, SanAntonio, Tex., and James Crawford, University of North CarolinaDental School, Chapel Hill, N.C., were drawn upon especiallyheavily. Also, Jack Smith, Amdent Corporation, Waxahachie, Tex.,was particularly helpful.
REFERENCES1. Abel, L. C., R. L. Miller, R. E. Micik, and G. Ryge. 1971.
Studies on dental aerobiology. IV. Bacterial contamination ofwater delivered by dental units. J. Dent. Res. 50:1567-1569.
2. Bagga, B. S. R., R. A. Murphy, A. W. Anderson, and I.Punwani. 1984. Contamination of dental unit cooling water withoral microorganisms and its prevention. J. Am. Dent. Assoc.109:712-716.
3. Christensen, G. J. 1991. Infection control: some significantloopholes. J. Am. Dent. Assoc. 122:99-100.
4. Comer, R. W., D. R. Myers, C. D. Steadman, M. J. Carter, J. P.Rissing, and F. J. Tedesco. 1991. Management considerations foran HIV positive dental student. J. Dent. Educ. 55:187-191.
5. Cottone, J. A., and J. A. Molinari. 1991. State-of-the-art infec-tion control in dentistry. J. Am. Dent. Assoc. 122:33-41.
6. Crawford, J. J., and C. Broderius. 1988. Control of cross-infection risks in the dental operatory: prevention of waterretraction by bur cooling spray systems. J. Am. Dent. Assoc.116:685-687.
7. Crawford, J. J., and C. Broderius. 1990. Evaluation of a dentalunit designed to prevent retraction of oral fluids. QuintessenceInt. 21:47-51.
8. Edwardsson, S., G. Svensater, and D. Birkhed. 1983. Steamsterilization of air turbine dental handpieces. Acta Odontol.Scand. 41:321-326.
9. Feldman, R. E., and E. R. Schiff. 1975. Hepatitis in dentalprofessionals. JAMA 232:1228-1230.
10. Gerberding, J. L. 1991. Reducing occupational risk of HIVinfection. Hosp. Pract. 26:103-118.
11. Gragg, P. P., J. M. Young, and J. A. Cottone. Handpiecesterilization: establishing an office protocol. Gen. Dent., inpress.
12. Kane, M. A., and L. A. Lettau. 1985. Transmission of HBV fromdental personnel to patients. J. Am. Dent. Assoc. 110:634-636.
13. Lewin, M. L., W. C. Maddrey, J. R. Wands, and A. I. Mende-loff. 1974. Hepatitis B transmission by dentists. JAMA 228:1139-1140.
14. Lewis, D. L. 1990. Risk of infection from dental handpieces.ASM News 56:625. (Letter.)
15. Lewis, D. L. 1991. Infection control in dental handpieces. ASMNews 57:393. (Letter.)
16. Lewis, D. L., and D. K. Gattie. 1990. Effects of cellularaggregation on the ecology of microorganisms. ASM News56:263-268.
17. Lewis, D. L., and D. K. Gattie. 1991. The ecology of quiescentmicrobes. ASM News 57:27-32.
18. Martin, M. V. 1987. The significance of the bacterial contami-nation of dental unit water systems. Br. Dent. J. 163:152-154.
19. Mosley, J. W., V. M. Edwards, G. Casey, A. G. Redeker, and E.White. 1975. Hepatitis B virus infection in dentists. N. Engl. J.Med. 293:729-734.
20. Neugeboren, N., R. J. Nisengard, E. H. Beutner, and G. W.Ferguson. 1972. Control of cross-contamination. J. Am. Dent.Assoc. 85:123-127.
21. Pelzner, R. B., D. Kempler, M. M. Stark, P. R. Barkin, and D.A. Graham. 1977. Laser evaluation of handpiece contamination.J. Dent. Res. 56:1629-1634.
22. Scheid, R. C., C. K. Kim, J. S. Bright, M. S. Whitely, and S.Rosen. 1982. Reduction of microbes in handpieces by flushingbefore use. J. Am. Dent. Assoc. 105:658-660.
23. U.S. Department of Health and Human Services. 1986. Recom-mended infection-control practices for dentistry. Morbid. Mor-tal. Weekly Rep. 35:237-242.
24. U.S. Department of Health and Human Services. 1987. Outbreakof hepatitis B associated with an oral surgeon-New Hamp-shire. Morbid. Mortal. Weekly Rep. 36:132-133.
25. U.S. Department of Health and Human Services. 1990. Possibletransmission of human immunodeficiency virus to a patientduring an invasive dental procedure. Morbid. Mortal. WeeklyRep. 39:489-493.
26. U.S. Department of Health and Human Services. 1991. Update:transmission of HIV infection during an invasive dental proce-dure-Florida. Morbid. Mortal. Weekly Rep. 40:21-27, 33.
27. U.S. Department of Health and Human Services. 1991. Update:transmission of HIV infection during an invasive dental proce-dure-Florida. Morbid. Mortal. Weekly Rep. 40:377-381.
28. Verrusio, A. C., E. A. Neidle, K. D. Nash, S. Silverman, A. M.Horowitz, and K. S. Wagner. 1989. The dentist and infectiousdiseases: a national survey of attitudes and behavior. J. Am.Dent. Assoc. 118:553-562.
29. Wirthlin, M. R., Jr., I. L. Shklair, R. A. Northerner, S. W.Shelton, and G. L. Bailey. 1981. The performance of autoclavedhigh-speed dental handpieces. J. Am. Dent. Assoc. 103:584-587.
J. CLIN. MICROBIOL.
on Novem
ber 4, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

JOURNAL OF CLINICAL MICROBIOLOGY, July 1992, p. 1902-19030095-1137/92/071902-02$02.00/0
Letters to the EditorCross-Infection Risks Associated with High-Speed Dental Drills
The article on the possible risks of disease transmissionvia high-speed dental drills by Lewis and Boe (8) hascommanded the attention of the dental community. Theauthors theorize that certain dental instruments may be asignificant factor in patient-to-patient conveyance of disease.
Valuable insights into this hypothetical problem can begained by studying hepatitis B virus (HBV). HBV is aprevalent, highly contagious blood-borne virus which hasbeen assiduously monitored for decades. As such, the occu-pational transmission in the health care setting has been wellestablished.A thorough review of the literature on HBV fails to reveal
a single documented case of patient-to-patient (i.e., via acontaminated instrument) transmission in all of dentistry ormedicine. Although several hundred cases of patients whohave been infected by highly contagious dentists and medicalsurgeons have been documented, studies in both the UnitedStates (1) and Great Britain (11) indicate that such transmis-sions are rare. In noting, therefore, that instrument trans-mission of HBV is without precedent, we have reasonableassurance that the risks of such is inconsequential.
Dentistry's exemplary record of preventing patient-to-patient transmission of the highly contagious HBV shouldgive ample indication that the risks of transmitting less-contagious diseases approach the meaningless. With regardto the specific comparison of HBV to human immunodefi-ciency virus (HIV) (Isn't HIV the cause of our anxiety?), itmust be noted that prospective studies of accidental intra-venous needle-stick seroconversions show that HBV is 100times more contagious than HIV (4). HBV is also much moreresistant to heat and germicidal agents, and HBV maintainsthe capacity to infect via contaminated surfaces hundreds oftimes longer.However, even with such a tremendous disparity in infec-
tivity, there are those who maintain that Dr. David Acerunprecedentedly transmitted HIV to his dental patientsthrough contaminated instruments, and they maintain thathe repeated the unprecedented act five times. They incom-prehensibly maintain that he transmitted his own viral strainfrom one patient to another via this unprecedented route.Such scenarios are scientifically defenseless. Acer had anestimated dozen or so HIV-infected patients in his practice.As such, the cross-contamination hypothesis would be muchmore compelling if the viral DNA had been different from hisown. But the DNA strains of the infected patients were
remarkably similar to Acer's, while being distinctly differentfrom those of eight HIV-positive controls who were ran-
domly selected from the area in which Acer practiced. Theeight controls were also distinctly different from each other.This suggests that no particular HIV strain predominates inthat geographic area, and it demonstrates that there was no
other viral strain comparable to Acer's (5).Numerous studies reveal that barriers lack demonstrable
benefits for both practitioners (6, 10, 12) and patients (7)vis-a-vis highly contagious carriers of HBV. Additionally,there are studies which show that highly contagious carrierstransmit disease in spite of judicious efforts, including thosemaintained in the fastidiously controlled environment of thehospital operation room (3, 7, 14). There are also studies
which show that infectious diseases are punctuated by highlycontagious carriers who exemplify the extremes for infectiv-ity (3, 9, 13, 14). In view of the Centers for Disease Control'sdata indicating that Acer was using reasonable infectioncontrols (5) (which is corroborated by his patients and staff[2]) and in view of the above-referenced studies, the logicalconclusion is that Acer, as the most viable source of highlyinfectious microbes, unwittingly transmitted HIV to hispatients while performing invasive procedures. This mode oftransmission has concrete precedent with regard to blood-borne viruses; the instrument transmission hypothesis hasnone. It would seem beyond debate that the small occupa-tional risk of HIV transmission is one posed by the highlycontagious human incubator and not by an instrument whichwas used on another patient.
REFERENCES1. Ahtone, J., and R. Goodman. 1983. Hepatitis B and dental
personnel. J. Am. Dent. Assoc. 106:219-222.2. Atlanta Constitution. 1991. Fri. Aug. 30, A-8.3. Berkelman, R., et al. 1982. Streptococcal wound infections
caused by a vaginal carrier. JAMA 247:2680-2682.4. Centers for Disease Control. 1991. Estimates of endemic trans-
mission of HBV and HIV. Given to attendees at January 30,1991 meeting, Atlanta.
5. Centers for Disease Control. 1991. Update: transmission of HIVinfection during an invasive dental procedure-Florida. Morbid.Mortal. Weekly Rep. 40:21-27.
6. Feldman, R. 1975. Hepatitis in dental personnel. JAMA 232:1228-1230.
7. Heptonstall, J. 1991. Outbreaks of hepatitis B virus infectionassociated with infected surgical staff. CDR 1:81-85.
8. Lewis, D. L., and R. K. Boe. 1992. Cross-infection risks asso-ciated with current procedures for using high-speed dentalhandpieces. J. Clin. Microbiol. 30:401-406.
9. Nakashima, A., et al. 1984. Epidemic bullous impetigo in anursery due to a nasal carrier of staphylococcus aureus. Infect.Control 5:326-331.
10. Nobel, M., et al. 1991. Hepatitis B and HIV infections in dentalprofessionals: effectiveness of infection control procedures. J.Can. Dent. Assoc. 57:55-58.
11. Palakoff, S. 1986. Acute hepatitis B in patients in Britain relatedto previous operations and dental treatment. Br. Med. J. 293:33-36.
12. Reingold, A., and M. Kane. 1988. Failure of gloves and otherprotective devices to prevent transmission of hepatitis B virusto oral surgeons. JAMA 259:2558-2560.
13. Roderick, S., et al. 1982. Intraoral and pulmonary tuberculosisfollowing dental treatment. Lancet i:842-844.
14. Welch, J., et al. 1989. Hepatitis B infection after gynaecologicalsurgery. Lancet i:205-206.
Stephen D. Carter6267 Memorial DriveStone Mountain, Georgia 30083
The article by Lewis and Boe on cross-infection risksassociated with use of dental handpieces is a seeminglywell-written study; however, its conclusions are based on a
pyramid of multilevel assumptions for which there is littleevidence of actual occurrence in dental patient populations.The authors' statement "despite the lack of data demon-
strating that external disinfection is effective in controlling
1902
Vol. 30, No. 7

LETTERS TO THE EDITOR 1903
cross-infection . . ." is poorly worded for a scientific article.The real issue is whether there are any data showing thatexternal disinfection is ineffective in controlling cross-infec-tion of handpieces.Though there is a substantial body of evidence implicating
needles in dental disease transmission, there are no docu-mented reports implicating traditionally disinfected dentalhandpieces. This absence of cases demonstrates that thisproblem is rare to nonexistent and that externally disinfectedhandpieces pose no significant problem in cross-contamina-tion in vivo.
Internal cleaning and/or autoclaving is destructive to theequipment and environment (through increased use of chlo-rofluorocarbon lubricants), reduces productivity, and in-creases the cost of providing and receiving dental treatmentwhile affording no measurable benefit to the patient or staff.Because of these disadvantages and the improbability of thetheoretical risks posed in the article, it is advisable that ourlimited resources be allocated to other, more productivepreventative measures.
E. J. Neiburger1000 North Ave.Suite 102Waukegan, Illinois 60085
Author's ReplyConsidering what would be required to prove a case of
patient-to-patient cross-infection in dentistry, it's not sur-prising that none are documented, even for HBV. Legally, itwould be almost impossible to have patients treated beforethe infected individual in question identified and tested to seewhether any were HBV carriers. Even if that were done itwould be scientifically impossible to determine that an HBVinfection originated with a particular patient and was ac-quired by another patient through a particular piece of dentalequipment.
It is widely accepted that contaminated needles can trans-mit HBV and HIV. Therefore, needles used to deliveranesthetics are suspected whenever there is any indicationof cross-infection. Air-driven high-speed handpieces andprophylaxis angles carry much more patient material than isharbored by needles. However, on the basis of the amount ofmaterial we can detect coming back out of this equipment
during reuse, it appears that frequencies of cross-infectionmay be comparable to those observed with needle sticks;i.e., large clusters of infected patients may not be produced.Documented clusters of HBV-infected dental patients havemost likely involved a more efficient mode of transmission.Nevertheless, the widespread operation of an inefficientmechanism may lead to a larger number of infected individ-uals in the population than is produced by the rare occur-rence of a more efficient mechanism.DNA sequences in the Acer cases suggest that HIV
infections there were associated with the dental practice, butlittle if anything more can be concluded. Stretching that datato conclude such things as patients were infected by thedentist rather than by other patients is scientifically unsup-portable. Regardless of what may have happened in the Acercases, we know that certain types of dental equipmentcollect visible amounts of blood and tissue inside and thatthis material comes back out when the equipment is reused.It cannot be that 150,000 dentists in this country are treatingmillions of patients with such equipment and only externallydisinfecting it in most cases and that virtually no one is beinginfected even with HBV. Considering the fact that noprospective epidemiological studies of cross-infection havebeen done in dentistry, the absence of documented casesshould not be used to assure patients that cross-infectionrisks are rare to nonexistent for any infectious agent. Addi-tionally, this should not prevent us from establishing auniversal standard that dental equipment contaminated in-ternally with blood and tissue must be cleaned and heattreated between patients. Centers for Disease Control guide-lines recommend that this equipment be autoclaved betweeneach patient, and many dentists have been doing so foryears.
REFERENCE
1. Palca, J. 1992. The case of the Florida dentist. Science 255:392-394.
David L. LewisGraduate FacultyFaculty of EcologyUniversity of GeorgiaAthens, Georgia 30602
VOL. 30, 1992