Embed Size (px)
Citation preview
CroniconO P E N A C C E S S EC DENTAL SCIENCE
Case Report
Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report
Hana Gadalla1* and Bassam M Kinaia2
1Clinical Assistant Professor, Division of Graduate Periodontics, University of Detroit Mercy School of Dentistry, Detroit, MI, USA 2Director and Associate Professor, Division of Graduate Periodontics, University of Detroit Mercy School of Dentistry, Detroit, MI, USA
*Corresponding Author: Hana Gadalla, Clinical Assistant Professor, Division of Graduate Periodontics, University of Detroit Mercy School of Dentistry, Detroit, MI, USA.
Citation: Hana Gadalla and Bassam M Kinaia. “Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report”. EC Dental Science 18.2 (2019): 174-183.
Received: December 18, 2018; Published: January 07, 2019
Abstract
Keywords: Split Ridge Technique; Dental Implant; Esthetic Zone
Introduction
Dental implants are a common treatment for replacement of natural teeth with predictable esthetic results [1,2]. After tooth loss, alveolar ridge resorption occurs resulting in esthetic and functional challenges [3-5]. Average alveolar ridge resorption of 1.5 - 2.0 mm vertically and 40 - 60% horizontally have been reported [6,7]. Such changes, especially in the esthetic zone can be difficult to correct and is dependent on the degree of alveolar ridge deficiency. In an attempt to compensate for such deficiency, a multidisciplinary approach including ridge augmentation and restorative technique is often required [8-10].
Background: Alveolar ridge deficiency is a common occurrence post extraction. Multiple surgical techniques are used to rebuild the alveolar ridge for proper implant placement including the concept of guided tissue regeneration before or at time of implant place-ment. Split ridge procedure is a technique that is used to increase the width of narrow ridge with simultaneous implant placement with high success rates (98 - 100%). Case Report: A 44 year old female presented with missing teeth No. 8, 9 due to trauma for more than 1 years. Upon examination, patient had a thick biotype with horizontal ridge deficiency where implant placement with simultaneous bone grafting was indicated. Clinically, there was approximately 5 - 6 mm of ridge width and 4.74 mm bone width as confirmed by the CBCT. Split ridge procedure was performed using piezosurgery, along with bone expanders and placement of two dental implants combined with bone grafting. Patient follow up for 1 year after implant placement. Results: The bone expansion was successful. The bone width gain was approximately 3 mm, which provided an adequate width to accommodate the dental implants. The two implant s were inserted without complication and the primary stability was achieved at 35 ncm. The two implants were successfully loaded. WES and PES scored were used to objectively examine the soft tissue around implants.Conclusion: The present case demonstrates the effectiveness of split ridge in increase the width of deficient ridge with simultaneous implant placement.
Several guided bone regeneration techniques have been used to rebuild the deficient ridge [11,12]. In order to increase the bone width, height and improve bone quality including guided bone regeneration [13], only ridge bone grafting [11]. However, these procedures revealed several disadvantages, including the necessity of second surgical site [14], graft materials resorption [15,16], delayed implant
175
Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report
Citation: Hana Gadalla and Bassam M Kinaia. “Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report”. EC Dental Science 18.2 (2019): 174-183.
placement 3 - 6 months of healing [17], membrane exposure [18]. These complication may lead to increase the duration and cost of treat-ment [16]. Split ridge technique represented as less invasive alternative approach to treat deficient ridge in bucco-lingual dimension with simultaneous implant placement in short treatment duration [19]. It allows reliable expansion of atrophic ridges, which helps placing im-plant inside the alveolar bone housing with adequate blood supply with success rate (89 - 100%) [20]. Aim of this case report to present case was treated with ridge split technique with simultaneous implant placement in esthetic zone with 1 year follow up.
Methods
Split Ridge Technique is a viable option with horizontal defects ranged from 3 - 5 mm and no need for vertical augmentation. It’s pre-ferred to perform split ridge for narrow ridges minimum of 3 mm. The 3 mm bone will have at least 1 mm of trabecular bone between the two cortical plates [21]. That will ensure housing the implant with good surrounding blood supply [20]. There has been a preference of split ride in maxillary teeth rather than mandibular teeth because of bone quality. Maxillary bone is softer than mandibular Bone. The use of osteotome in split ridge may improve the bone quality around implant and achieve primary stability [22].
Case Presentation
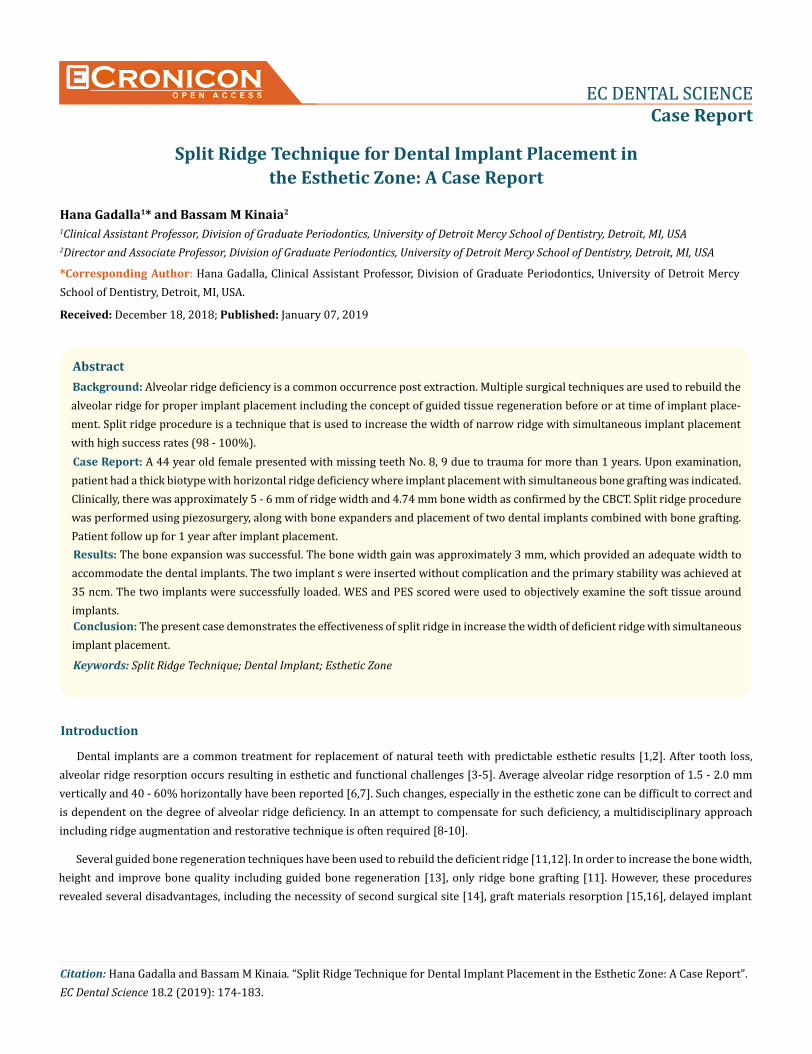
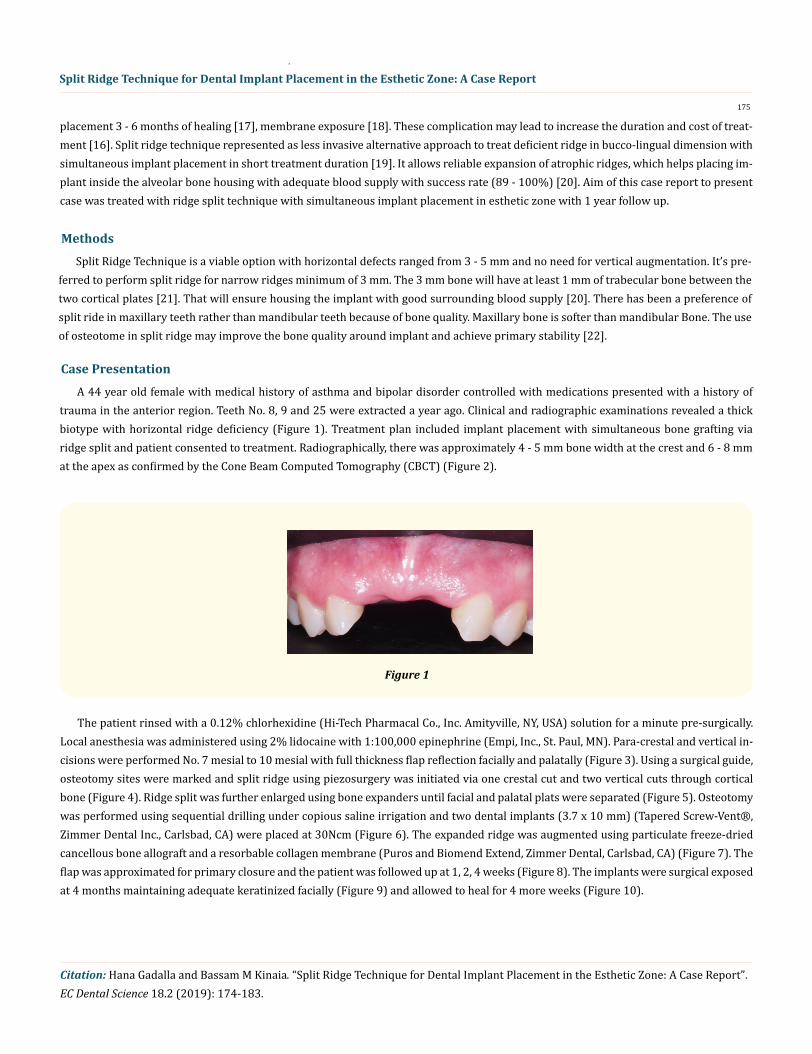
A 44 year old female with medical history of asthma and bipolar disorder controlled with medications presented with a history of trauma in the anterior region. Teeth No. 8, 9 and 25 were extracted a year ago. Clinical and radiographic examinations revealed a thick biotype with horizontal ridge deficiency (Figure 1). Treatment plan included implant placement with simultaneous bone grafting via ridge split and patient consented to treatment. Radiographically, there was approximately 4 - 5 mm bone width at the crest and 6 - 8 mm at the apex as confirmed by the Cone Beam Computed Tomography (CBCT) (Figure 2).
Figure 1
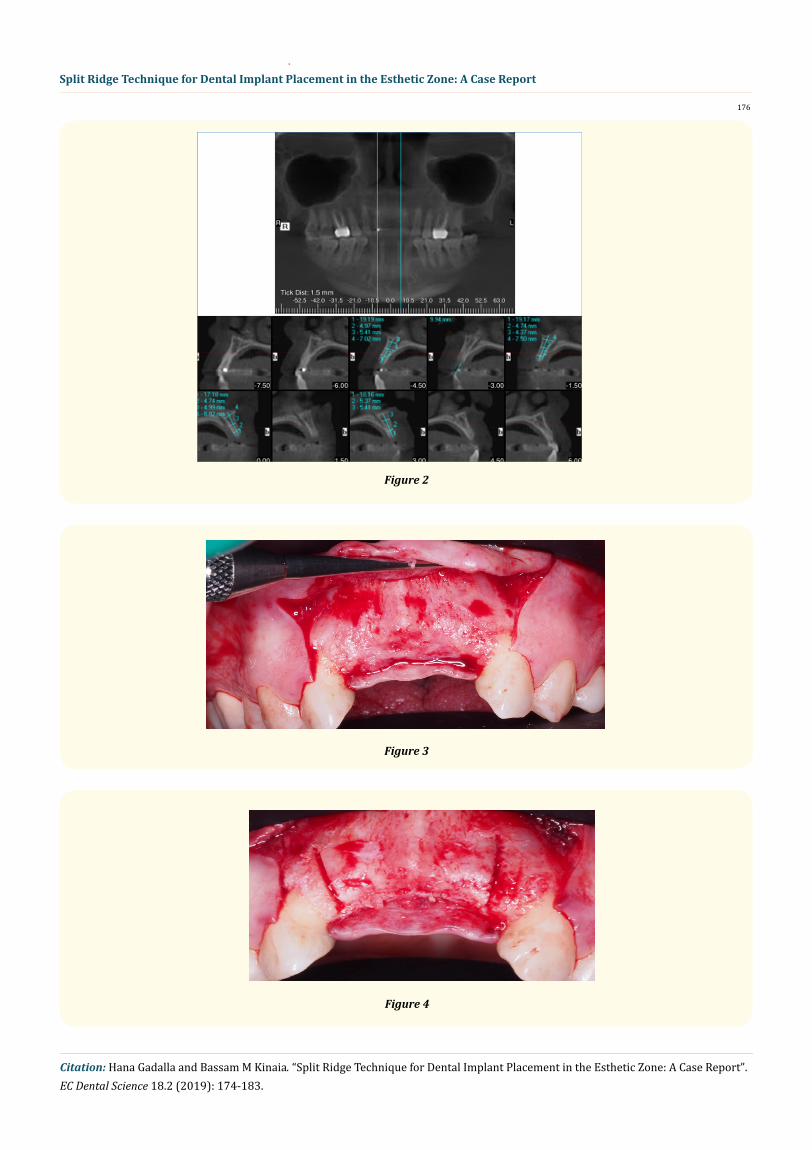
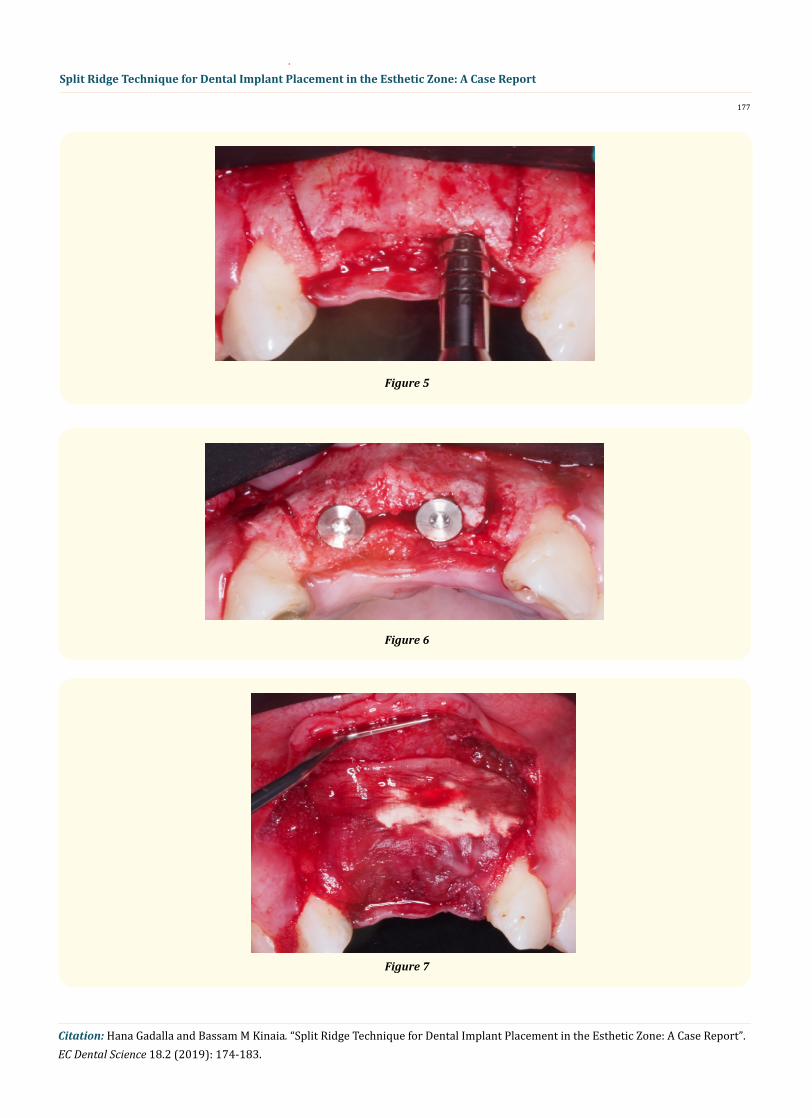
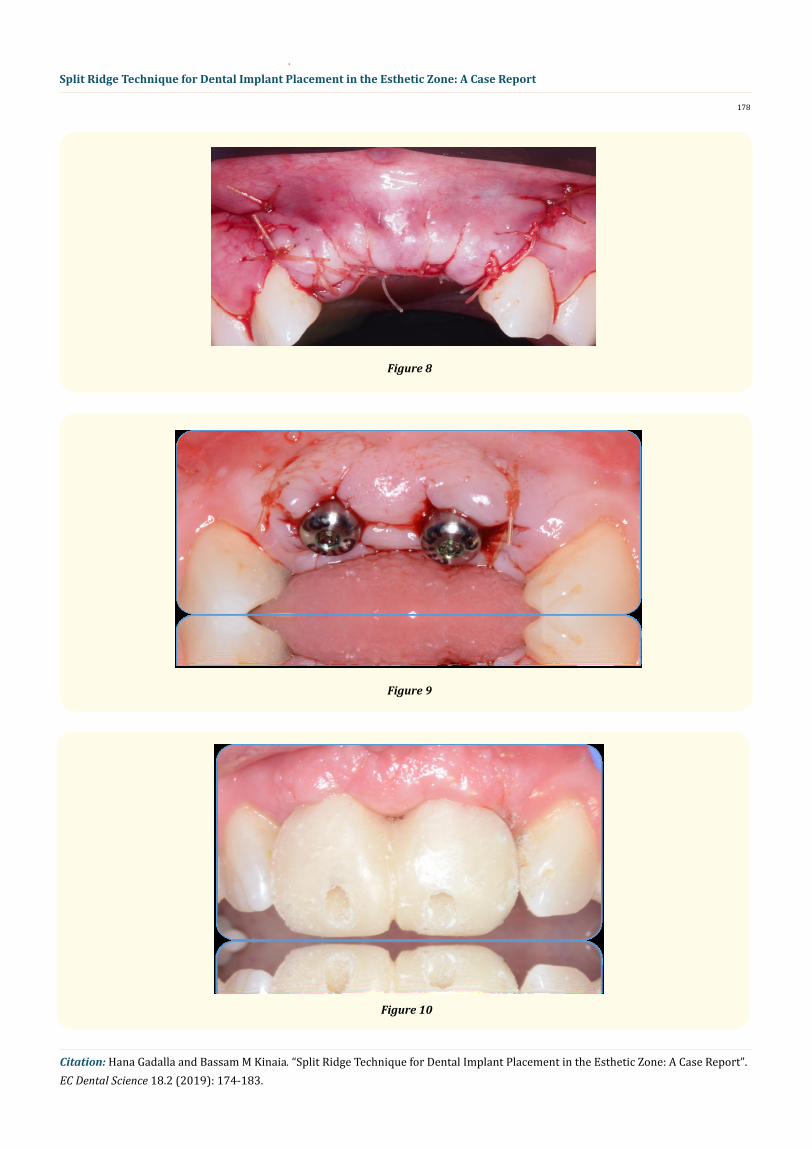
The patient rinsed with a 0.12% chlorhexidine (Hi-Tech Pharmacal Co., Inc. Amityville, NY, USA) solution for a minute pre-surgically. Local anesthesia was administered using 2% lidocaine with 1:100,000 epinephrine (Empi, Inc., St. Paul, MN). Para-crestal and vertical in-cisions were performed No. 7 mesial to 10 mesial with full thickness flap reflection facially and palatally (Figure 3). Using a surgical guide, osteotomy sites were marked and split ridge using piezosurgery was initiated via one crestal cut and two vertical cuts through cortical bone (Figure 4). Ridge split was further enlarged using bone expanders until facial and palatal plats were separated (Figure 5). Osteotomy was performed using sequential drilling under copious saline irrigation and two dental implants (3.7 x 10 mm) (Tapered Screw-Vent®, Zimmer Dental Inc., Carlsbad, CA) were placed at 30Ncm (Figure 6). The expanded ridge was augmented using particulate freeze-dried cancellous bone allograft and a resorbable collagen membrane (Puros and Biomend Extend, Zimmer Dental, Carlsbad, CA) (Figure 7). The flap was approximated for primary closure and the patient was followed up at 1, 2, 4 weeks (Figure 8). The implants were surgical exposed at 4 months maintaining adequate keratinized facially (Figure 9) and allowed to heal for 4 more weeks (Figure 10).
176
Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report
Citation: Hana Gadalla and Bassam M Kinaia. “Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report”. EC Dental Science 18.2 (2019): 174-183.
Figure 2
Figure 3
Figure 4
177
Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report
Citation: Hana Gadalla and Bassam M Kinaia. “Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report”. EC Dental Science 18.2 (2019): 174-183.
Figure 5
Figure 6
Figure 7
178
Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report
Citation: Hana Gadalla and Bassam M Kinaia. “Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report”. EC Dental Science 18.2 (2019): 174-183.
Figure 8
Figure 9
Figure 10
179
Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report
Citation: Hana Gadalla and Bassam M Kinaia. “Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report”. EC Dental Science 18.2 (2019): 174-183.
Restorative treatment
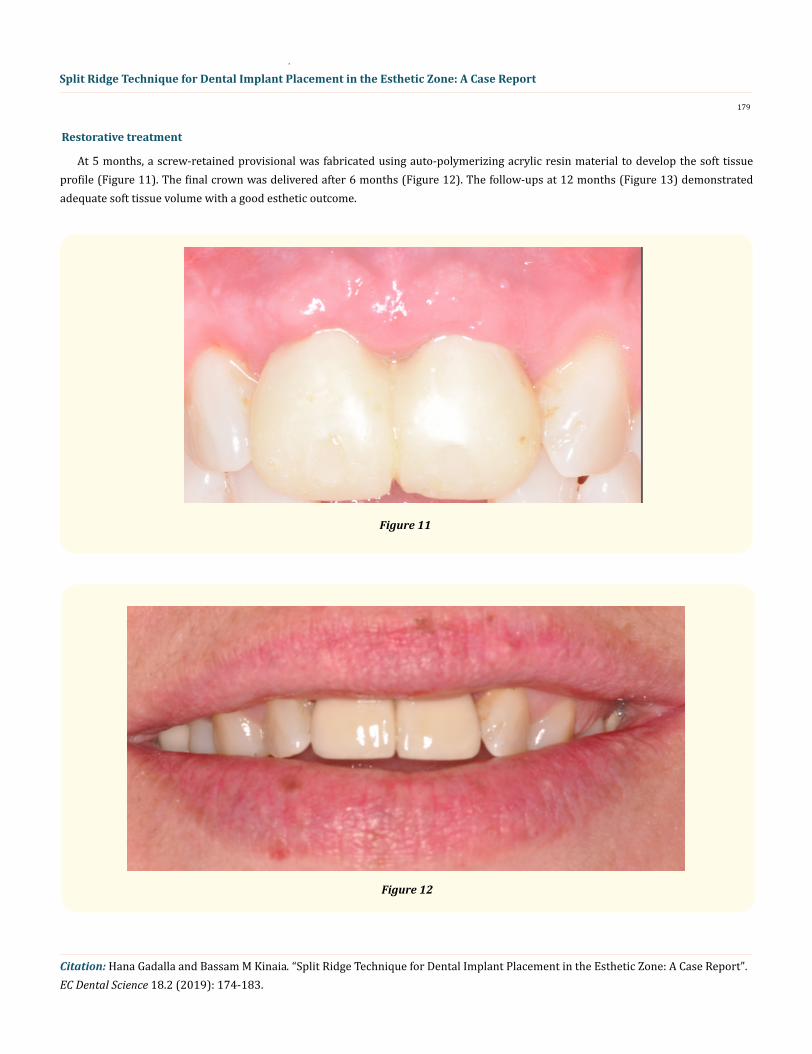
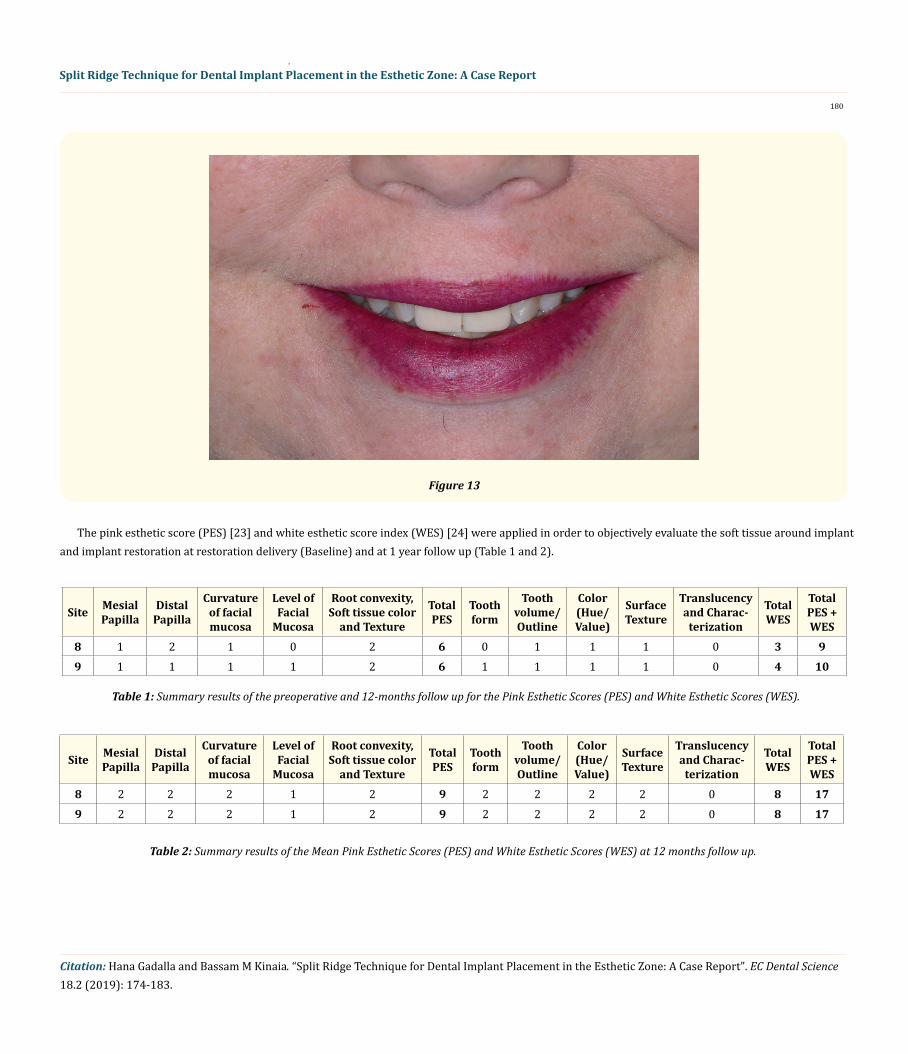
At 5 months, a screw-retained provisional was fabricated using auto-polymerizing acrylic resin material to develop the soft tissue profile (Figure 11). The final crown was delivered after 6 months (Figure 12). The follow-ups at 12 months (Figure 13) demonstrated adequate soft tissue volume with a good esthetic outcome.
Figure 11
Figure 12
Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report
180
Citation: Hana Gadalla and Bassam M Kinaia. “Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report”. EC Dental Science 18.2 (2019): 174-183.
The pink esthetic score (PES) [23] and white esthetic score index (WES) [24] were applied in order to objectively evaluate the soft tissue around implant and implant restoration at restoration delivery (Baseline) and at 1 year follow up (Table 1 and 2).
Figure 13
Site Mesial Papilla
Distal Papilla
Curvature of facial mucosa
Level of Facial
Mucosa
Root convexity, Soft tissue color
and Texture
Total PES
Tooth form
Tooth volume/Outline
Color (Hue/Value)
Surface Texture
Translucency and Charac-
terization
Total WES
Total PES + WES
8 1 2 1 0 2 6 0 1 1 1 0 3 99 1 1 1 1 2 6 1 1 1 1 0 4 10
Table 1: Summary results of the preoperative and 12-months follow up for the Pink Esthetic Scores (PES) and White Esthetic Scores (WES).
Site Mesial Papilla
Distal Papilla
Curvature of facial mucosa
Level of Facial
Mucosa
Root convexity, Soft tissue color
and Texture
Total PES
Tooth form
Tooth volume/Outline
Color (Hue/Value)
Surface Texture
Translucency and Charac-
terization
Total WES
Total PES + WES
8 2 2 2 1 2 9 2 2 2 2 0 8 179 2 2 2 1 2 9 2 2 2 2 0 8 17
Table 2: Summary results of the Mean Pink Esthetic Scores (PES) and White Esthetic Scores (WES) at 12 months follow up.
181
Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report
Citation: Hana Gadalla and Bassam M Kinaia. “Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report”. EC Dental Science 18.2 (2019): 174-183.
Results
The bone expansion was successful. The bone width gain was approximately 3 mm, which provided an adequate width to accommo-date the dental implants. The two implant s were inserted without complication and the primary stability was achieved at 35 ncm. The two implants were successfully loaded.
Discussion
The present case report examined the amount of increase of labiolingual width of a narrow ridge with simultaneous implant place-ment following split ridge procedure in anterior maxilla. This technique allows dental implant placement in areas involving insufficient bone width by moving the labial external cortical plate labially [25]. There are many advantages to this procedure. First, it eliminates the need for second surgical site to harvest the bone graft like intra-oral or Extra-oral site, therefore reduced the patient morbidity [14]. Also, Chiapasco 2009 reported that it allows reliable expansion of atrophic ridges that permit immediate implant placement an inside alveolar bony housing with adequate blood supply and High success rates (98 - 100%) [20]. Also, this technique is more suitable in maxilla rather than mandible because of thinner cortical plates and softer medullary bone [26].
Conclusion This case demonstrates the effectiveness of split ridge in increase the width of deficient ridge with simultaneous implant placement.
Bibliography
1. Schmitt A and Zarb GA. “The longitudinal clinical effectiveness of osseointegrated dental implants for single-tooth replacement”. International Journal of Prosthodontics 6.2 (1993): 197-202.
2. Henry PJ., et al. “Osseointegrated implants for single-tooth replacement: A prospective 5-year multicenter study”. International Jour-nal of Oral and Maxillofacial Implants 11.4 (1996): 450-455.
3. Schropp L., et al. “Bone healing following immediate versus delayed placement of titanium implants into extraction sockets: A pro-spective clinical study”. International Journal of Oral and Maxillofacial Implants 18.2 (2003): 189-199.
4. Araujo MG., et al. “Ridge alterations following implant placement in fresh extraction sockets: An experimental study in the dog”. Jour-nal of Clinical Periodontology 32.6 (2005): 645-652.
5. Amler MH., et al. “Histological and histochemical investigation of human alveolar socket healing in undisturbed extraction wounds”. Journal of the American Dental Association 61 (1960): 32-44.
6. Van der Weijden F., et al. “Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review”. Journal of Clinical Periodontology 36.12 (2009): 1048-1058.
7. Schropp L., et al. “Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study”. International Journal of Periodontics and Restorative Dentistry 23.4 (2003): 313-323.
8. Seibert JS. “Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. part I. technique and wound healing”. Compendium of Continuing Education in Dentistry 4.5 (1983): 437-453.
9. Allen EP., et al. “Improved technique for localized ridge augmentation. A report of 21 cases”. Journal of Periodontology 56.4 (1985): 195-199.
182
Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report
Citation: Hana Gadalla and Bassam M Kinaia. “Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report”. EC Dental Science 18.2 (2019): 174-183.
10. Hannon SM., et al. “Selective use of gingival-toned ceramics: Case reports”. Quintessence International 25.4 (1994): 233-238.
11. Chiapasco M., et al. “Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants”. Clinical Oral Implants Research 17.2 (2006): 136-159.
12. Jensen SS and Terheyden H. “Bone augmentation procedures in localized defects in the alveolar ridge: Clinical results with different bone grafts and bone-substitute materials”. International Journal of Oral and Maxillofacial Implants 24 (2009): 218-236.
13. Castillo R. “Horizontal ridge augmentation before placing implants using a double-bone, double resorbable membrane technique: Two clinical cases”. European Journal of Esthetic Dentistry 5.4 (2010): 340-356.
14. Hammerle CH., et al. “A systematic review of the survival of implants in bone sites augmented with barrier membranes (guided bone regeneration) in partially edentulous patients”. Journal of Clinical Periodontology 29.3 (2002): 226-233.
15. Ignatius AA., et al. “A composite polymer/tricalcium phosphate membrane for guided bone regeneration in maxillofacial surgery”. Journal of Biomedical Materials Research Part A 58.5 (2001): 564-569.
16. Chiapasco M., et al. “Clinical outcome of autogenous bone blocks or guided bone regeneration with e-PTFE membranes for the recon-struction of narrow edentulous ridges”. Clinical Oral Implants Research 10.4 (1999): 278-288.
17. Blus C and Szmukler-Moncler S. “Split-crest and immediate implant placement with ultra-sonic bone surgery: A 3-year life-table analysis with 230 treated sites”. Clinical Oral Implants Research 17.6 (2006): 700-707.
18. Nevins M and Mellonig JT. “Enhancement of the damaged edentulous ridge to receive dental implants: A combination of allograft and the GORE-TEX membrane”. International Journal of Periodontics and Restorative Dentistry 12.2 (1992): 96-111.
19. Simion M., et al. “Jawbone enlargement using immediate implant placement associated with a split-crest technique and guided tissue regeneration”. International Journal of Periodontics and Restorative Dentistry 12.6 (1992): 462-473.
20. Chiapasco M., et al. “Bone augmentation procedures in implant dentistry”. International Journal of Oral and Maxillofacial Implants 24 (2009): 237-259.
21. Khairnar MS., et al. “Modified ridge splitting and bone expansion osteotomy for placement of dental implant in esthetic zone”. Con-temporary Clinical Dentistry 5.1 (2014): 110-114.
22. Summers RB. “A new concept in maxillary implant surgery: The osteotome technique”. Compendium 15 (1994): 152, 154, 156, 158, 162.
23. Furhauser R., et al. “Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score”. Clinical Oral Implants Research 16.6 (2005): 639-644.
24. Belser UC., et al. “Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: A cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores”. Journal of Peri-odontology 80.1 (2009): 140-151.
25. Simion M., et al. “Qualitative and quantitative comparative study on different filling materials used in bone tissue regeneration: A controlled clinical study”. International Journal of Periodontics and Restorative Dentistry 14.3 (1994): 198-215.
183
Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report
Citation: Hana Gadalla and Bassam M Kinaia. “Split Ridge Technique for Dental Implant Placement in the Esthetic Zone: A Case Report”. EC Dental Science 18.2 (2019): 174-183.
Volume 18 Issue 2 February 2019© All rights reserved by Hana Gadalla and Bassam M Kinaia.
26. Misch CM. “Implant site development using ridge splitting techniques”. Oral and Maxillofacial Surgery Clinics of North America 16.1 (2004): 65,74, vi.
27. Milinkovic I and Cordaro L. “Are there specific indications for the different alveolar bone augmentation procedures for implant place-ment? A systematic review”. International Journal of Oral and Maxillofacial Surgery 43.5 (2014): 606-625.
28. Ella B., et al. “Mandibular ridge expansion using a horizontal bone-splitting technique and synthetic bone substitute: An alternative to bone block grafting?” International Journal of Oral and Maxillofacial Implants 29.1 (2014): 135-140.











![Cronicon DENTAL SCIENCE OPEN ACCESS · When compared with the general population it was found that the dentists and dental staff have higher chances of respiratory infec-tions [4]](https://img.pdfslide.us/doc/110x75/5f808e398bdfb254e72ebad0/cronicon-dental-science-open-access-when-compared-with-the-general-population-it.jpg)