Embed Size (px)
Citation preview

Crohn’s Disease Presenting as Intestinal Parasites “I got worms…”
Poster by Jared Halterman, Kade Rasmussen DO, and Joseph Dougherty DO
A 14 year-old male with abdominal pain and vomiting for three days was transferred from a rural ER to the emergency department at a tertiary children’s care center with the diagnosis of parasitic worm infection of the small bowel. The patient had initially presented to the transferring facility the previous day. Based on physical exam he was diagnosed with gastroenteritis and discharged home. He returned the next day with worsening symptoms. Labs and CT scan of the abdomen were performed, leading to diagnosis and transfer.
Pertinent medical and social histories were negative except for a recent trip to Puerto Rico two months prior. On exam vitals were within normal limits, membranes were slightly dry. There was periumbilical tenderness with rebound and guarding. Discs with CT imaging accompanied the patient and were reread by pediatric specialists. Impression was as follows;
“Dilated loops of small bowel at the level of the terminal ileum with wall thickening, multiple ovoid shaped densities with peripheral lucency/gas in the distal small bowel, probable resulting in obstruction at the level of the terminal ileum/ileocecal valve. These intralumenal densities could represent parasitic disease or represent retained ingested material. The colon is collapsed and there is free fluid in the abdomen and pelvis. There are multiple mesenteric nodes which may be reactive.”
In the ED the patient received pain medications, IV fluids and an NG tube placed. Patient was taken by surgery for an exploratory lap, the end result of which was ileocecectomy with anastamosis. Pathology of the removed segment showed full thickness colitis with granulation tissue, and retained vegetable material. Final diagnosis was new onset Crohn’s Disease leading to small bowel obstruction.
References:1 Griffiths, AM, Hugot, JP. Crohn Disease. In: Pediatric Gastrointestinal Disease: Pathopsychology, Diagnosis, Management, 4th ed, Walker, WA, Goulet, O, Kleinman, RE, et al (Eds), BC Decker, Ontario, 2004. p. 789.2 Galbraith SS, Drolet BA, Kugathasan S, et al. Asymptomatic inflammatory bowel disease presenting with mucocutaneous findings. Pediatrics 2005; 116:e439.3 http://www.cdc.gov/ibd/4 http://www.mayoclinic.com/health/crohns-disease/DS00104
Crohn's Disease (CD) is an inflammatory, immune-mediated condition which may affect any portion of the GI tract from the mouth to the anus, most commonly the ileum and cecum (50%). Pathophysiology is not clearly defined, but likely involves both genetic and environmental factors. Incidence is 5-10 cases per 100,000 with app 25% occurring children younger than 18.
Presentation is variable and often nonspecific. In children intestinal symptoms include growth failure, weight loss, diarrhea, abdominal pain, abdominal mass, bowel obstruction, rectal bleeding. Extraintestinal manifestations include fever, arthralgias, uveitis, anemia, clubbing, oral ulcers. Diagnosis typically involves extensive workup to rule out other diseases.
Incorrect initial diagnosis is not uncommon due to the variability in early symptoms, though possible parasitic infestation is presumed to be a less common presentation. That we are aware, our patient denied typical previous signs or symptoms before presenting with SBO secondary to terminaI iliel inflammation requiring ileocecectomy.
Treatment is based on symptoms and consist of diet control, anti-inflammatory medications (sulfasalazine, corticosteroids), immunosupressents (azathioprine), antibiotics when necessary, anti-diarrheals or laxatives, pain control and surgery as a last resort.
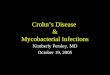
Terminal Ileum w/ granulation tissue, gross and on microscopy
Cobblestoning inflammation