Embed Size (px)
Citation preview
Creation of a mechanism for the exchange of knowledge on Clinical Added Value for Orphan Drugs (CAVOD)Meeting EUCERD
October 24th, 2011
Pascale Augé (former Ernst & Young), Head of Tech Transfer & Entrepreneurship, Institut Pasteur

2011 CAVOD StudyPage 2© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
The nine objectives of the study on the creation of a mechanism of exchange of knowledge on CAVOD (1/2)
► 1. To describe the regulatory process followed by an orphan medicine, from Orphan Designation at the European level to reimbursement in the Member State and examine to what extent the information produced by the authorities responsible for Orphan Designation and Marketing Authorization is directly useful for the medicine reimbursement decision process.
► 2. To describe the Health Technology Assessment expertise (focusing on relative efficacy and relative effectiveness) used at national level for this purpose and the level of involvement of existing international Health Technology Assessment networks.
► 3. To describe what expertise is used when the medicine is prescribed to all the targeted population of patients affected by a certain rare disease and how the heterogeneity of a disease expression is appraised (e.g. differences of weight, age, clinical manifestations, history of treatments taken by each patient, differences of social situation, patient ability to comply with the constraints imposed by the treatment, etc.), with the aim to identify the data collection which could be considered as acceptable to establish the relative effectiveness and, based on this data, to generate an assessment of real clinical added value.
► 4. To propose a format for the Common Assessment Report for clinical added value for orphan medicines structured in a usable way for national decision makers, keeping in mind that this Common Assessment Report should be flexible enough to be used for the revision of this report.
2011 CAVOD StudyPage 3© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
The nine objectives of the study on the creation of a mechanism of exchange of knowledge on CAVOD (2/2) ► 5. To define, in consultation with the EC competent Units, the European Union Committee of Experts on Rare
Diseases (EUCERD), EMA, COMP and other EMA Committees (CHMP, CAT and PDCO), which is the most appropriate structure for performing this Task at a coordinated EU level: (a) Which could be the most appropriate mechanism of coordination with the HTA organizations in Europe, the COMP and other EMA committees, in terms of governance and in order to obtain the highest scientific added value? (b) Which could be the most appropriate composition of this mechanism of coordination? (c) What are the financial implications for setting up a new structure or using an existing structure?
► 6. To formulate recommendations for principal Tasks of this mechanism of coordination taking into account that expressed opinions should be in the form of non-binding Common Assessment Reports on the scientific assessment of the relative effectiveness of orphan Medicines approved at the EU level and for the set up of the modus operandi of the dialogue with Member States to facilitate coordination of possible additional national requirements (e.g. registries, real life studies).
► 7. To propose possible articulation between these Common Assessment Reports on the Clinical Added Value of Orphan Medicines and CHMP (Committee for Human Medicinal Products) post-marketing obligations to avoid duplication and make the most of available resources.
► 8. To stick to what can be implemented within the current legislative framework on pharmaceutical products, including the role of EMA.
► 9. To envisage potential enlargement of these assessment and related mechanisms of cooperation to the broader context of HTAs and to all types of medicines, not just orphan medicines.
2011 CAVOD StudyPage 4© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
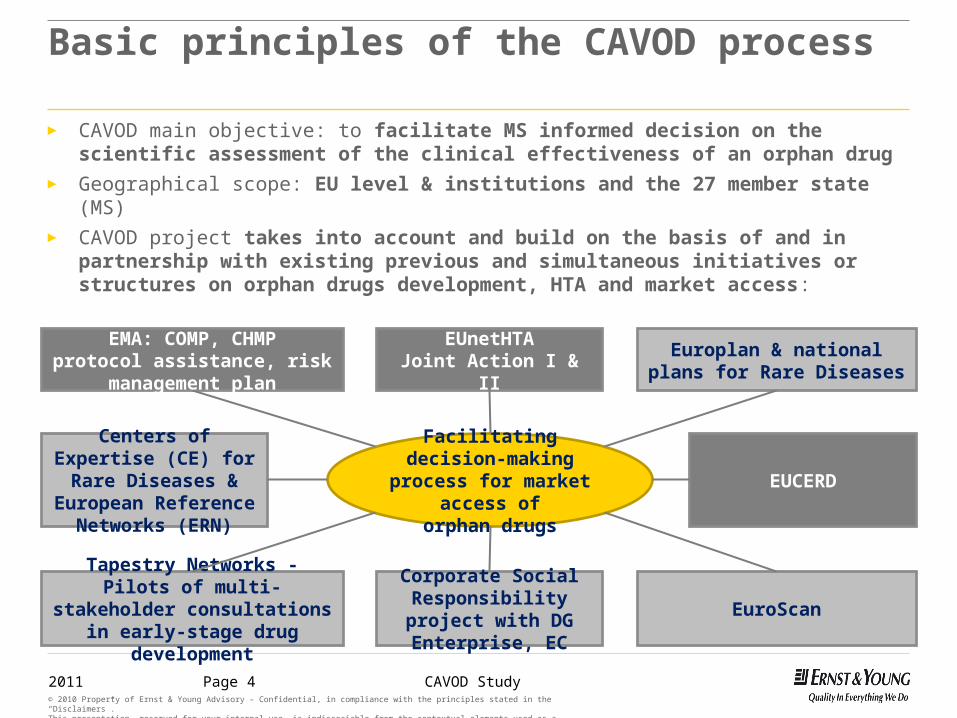
Centers of Expertise (CE) for Rare Diseases & European Reference
Networks (ERN)
Facilitatingdecision-making process
for market access oforphan drugs
EMA: COMP, CHMPprotocol assistance, risk
management plan
Europlan & national plans for Rare Diseases
EUnetHTAJoint Action I & II
EUCERD
Tapestry Networks - Pilots of multi-stakeholder consultations in early-
stage drug developmentEuroScan
Corporate Social Responsibility project with DG Enterprise, EC
Basic principles of the CAVOD process
► CAVOD main objective: to facilitate MS informed decision on the scientific assessment of the clinical effectiveness of an orphan drug
► Geographical scope: EU level & institutions and the 27 member state (MS)► CAVOD project takes into account and build on the basis of and in partnership with
existing previous and simultaneous initiatives or structures on orphan drugs development, HTA and market access:
2011 CAVOD StudyPage 5© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
CAVOD process
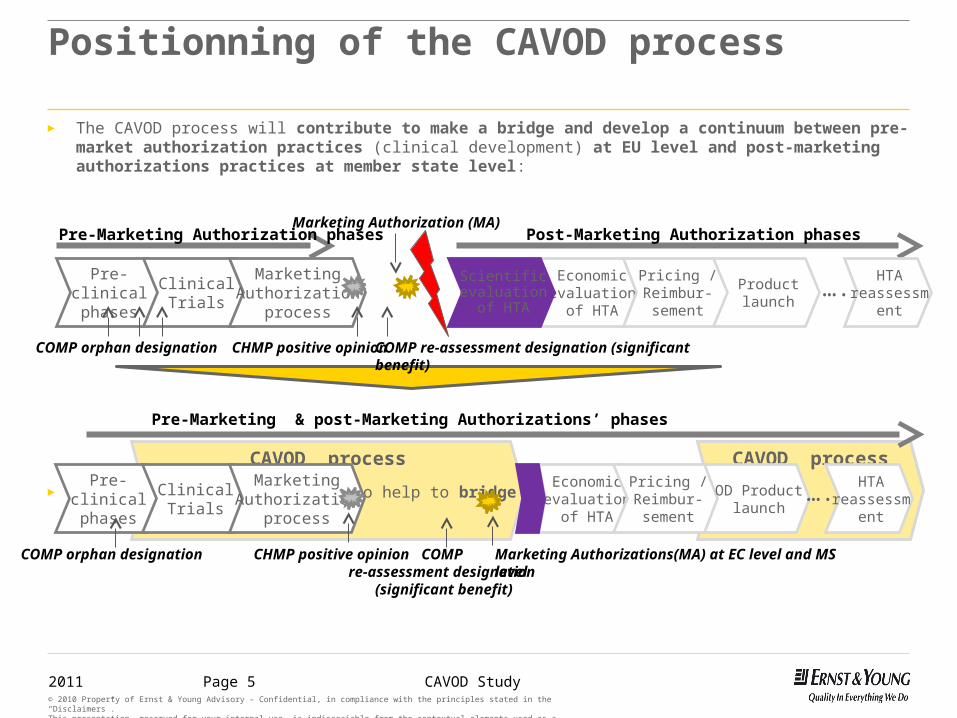
► The CAVOD process will contribute to make a bridge and develop a continuum between pre-market authorization practices (clinical development) at EU level and post-marketing authorizations practices at member state level:
► The CAVOD mechanism should also help to bridge the gap between regulators and HTA bodies
CAVOD process
Positionning of the CAVOD process
Pre-clinical phases
ClinicalTrials
Marketing Authorization
process
Economic evaluation of
HTA
Pricing / Reimbur-sementProduct launch
Marketing Authorization (MA)Post-Marketing Authorization phasesPre-Marketing Authorization phases
Pre-clinical phases
ClinicalTrials
Economic evaluation of
HTA
Pricing / Reimbur-sement
OD Product launch
Pre-Marketing & post-Marketing Authorizations’ phases
Marketing Authorization
process
CHMP positive opinion Marketing Authorizations(MA) at EC level and MS level
CHMP positive opinionCOMP orphan designation COMP re-assessment designation (significant benefit)
Scientific evaluation of
HTA
COMP re-assessment designation
(significant benefit)
COMP orphan designation
HTA reassessment
HTA reassessment
….
….

2011 CAVOD StudyPage 6© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
General methodology
► Extensive data collection, via literature, interviews and questionnaires, on the regulatory processes (and particularly those applicable to orphan drugs) in the relevant institutions and national authorities involved in relative effectiveness assessment of drugs at MS level.
► Creating a trusted, solid and long-term relationship between the stakeholders (and in particular between EU and MS level stakeholders) through productive working sessions and workshops to reach a consensus solution that can be implemented in the future.
Stakeholders worked together in a real committed way to develop the new proposal for the CAVOD process
► Defining the process associated with the CAVOD mechanism
► Evaluating the budget impact of this new process for the exchange of knowledge in terms of governance, operational function and decision-making process, in order to evaluate the cost of such mechanism.
► Drafting and finalizing the Final Recommendation report, including a format for the Common Assessment Report, CAR, for the scientific assessment of the relative effectiveness of orphan medicines.

2011 CAVOD StudyPage 7© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
Update on the methodology
► Interviews/meetings with the 9 different types of stakeholders including:► EC/EAHC► EMA (COMP, CHMP, Secretariat)► HTA national authorities in MS► Payers (ESIP)► European networks (EUNetHTA, HTAi, EUCERD)► Patient organizations (EURORDIS…)► Industry organizations (EBE, EFPIA…)► Other initiatives (Orphanet, Swedish Presidency
Initiative, national plan for RD…)► Meeting with stakeholders:
► EUnetHTA (May 2011)► EBE (Feb, May 2011)► EFPIA (May 2011)► EUCERD (Ocotber 2011)
► Questionnaires for the HTA national authorities including, among which:
► HTA bodies► Government healthcare department officers
► Working sessions and workshop:► 1st working session: March 1st
► CAVOD mechanism, model, structure and organization
► 2nd working session: March 31st, ► the relevant process and criteria for the scientific
assessment of CAVOD
► 3rd workshop: May 27th, ► final workshop coupled with EURORDIS Round Table of
Companies (ERTC) on the “Mechanisms for the Implementation of the Clinical Added Value (Relative Efficacy or Relative Effectiveness) of Orphan Drugs, so called CAVOD”
2011 CAVOD StudyPage 8© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
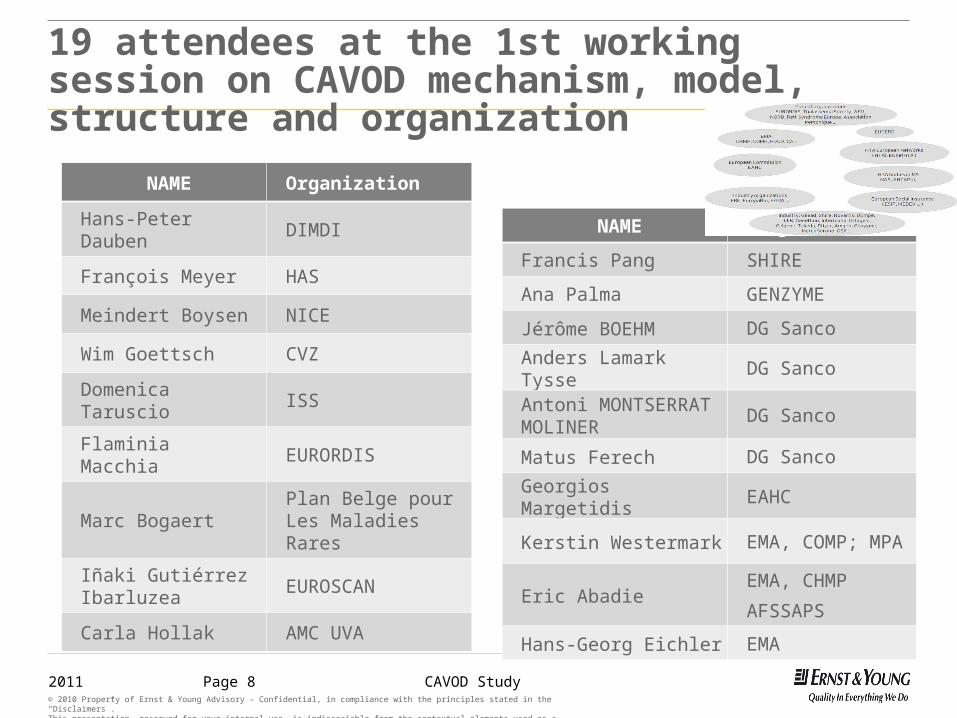
19 attendees at the 1st working session on CAVOD mechanism, model, structure and organization
NAME Organization
Hans-Peter Dauben DIMDI
François Meyer HAS
Meindert Boysen NICE
Wim Goettsch CVZ
Domenica Taruscio ISS
Flaminia Macchia EURORDIS
Marc Bogaert Plan Belge pour Les Maladies Rares
Iñaki Gutiérrez Ibarluzea EUROSCAN
Carla Hollak AMC UVA
NAME Organization
Francis Pang SHIRE
Ana Palma GENZYME
Jérôme BOEHM DG Sanco
Anders Lamark Tysse DG Sanco
Antoni MONTSERRAT MOLINER
DG Sanco
Matus Ferech DG Sanco
Georgios Margetidis EAHC
Kerstin Westermark EMA, COMP; MPA
Eric AbadieEMA, CHMP
AFSSAPS
Hans-Georg Eichler EMA
2011 CAVOD StudyPage 9© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
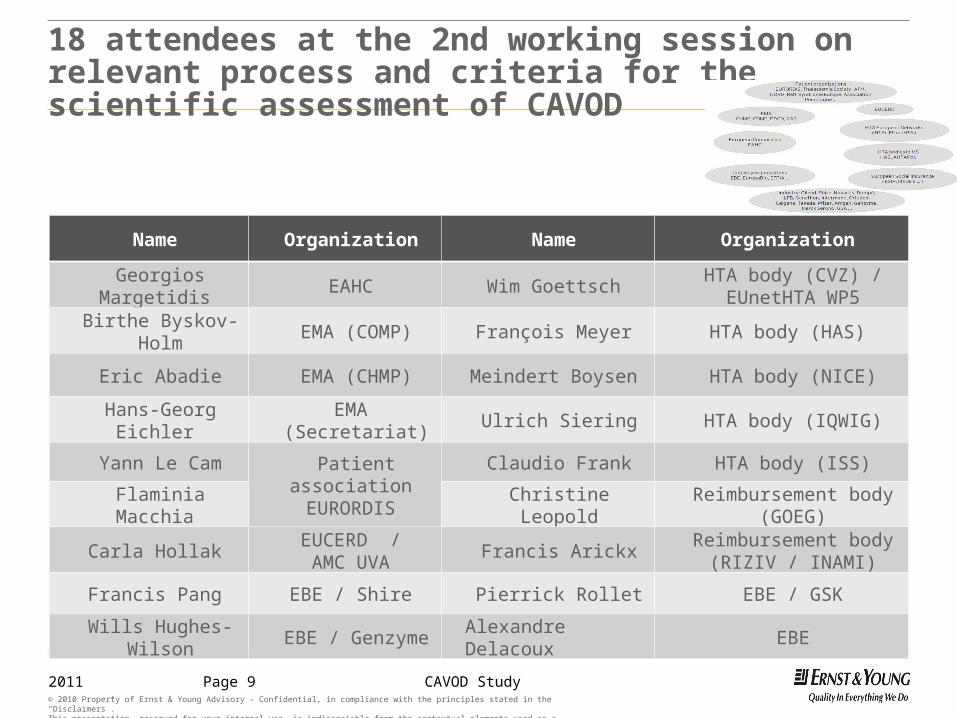
18 attendees at the 2nd working session on relevant process and criteria for the scientific assessment of CAVOD
Name Organization Name Organization
Georgios Margetidis EAHC Wim Goettsch HTA body (CVZ) / EUnetHTA WP5
Birthe Byskov-Holm EMA (COMP) François Meyer HTA body (HAS)
Eric Abadie EMA (CHMP) Meindert Boysen HTA body (NICE)
Hans-Georg Eichler EMA (Secretariat) Ulrich Siering HTA body (IQWIG)
Yann Le Cam Patient association EURORDIS
Claudio Frank HTA body (ISS)
Flaminia Macchia Christine Leopold Reimbursement body (GOEG)
Carla Hollak EUCERD / AMC UVA Francis Arickx Reimbursement body (RIZIV /
INAMI)
Francis Pang EBE / Shire Pierrick Rollet EBE / GSK
Wills Hughes-Wilson EBE / Genzyme Alexandre Delacoux EBE

2011 CAVOD StudyPage 10© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
81 attendees at the final workshop of the Eurordis – Ernst & Young Round Table of Companies (ERTC)“Mechanisms for the Implementation of the Clinical Added-Value (Relative Effectiveness) of Orphan Drugs, CAVOD”
List of participant Name Organisation
Jakub Adamski Ministry of Health Poland
François Anger ADDMEDICA France Francis Arickx National Institute for Health and Disability
Insurance Belgium Pascale Augé Ernst & Young France Fabrizia Bignami EURORDIS France Karin Blumer Novartis International AG Switzerland Anne-Mary Bodin EURORDIS France Jill Bonjean EURORDIS France Meindert Boysen Centre for Health Technology Evaluation,
NICE United Kingdom Giorgio Buseghin Chiesi Farmaceutici S.p.A. Italy
David Caponera Aegerion Pharmaceuticals, Inc. USA
Germano Carganico Rare Partners Srl Italy
François Cornu Aegerion Pharmaceuticals, Inc. France
Alvarez, Cuervo Virginia Pharma Mar, S.A. Spain
Stéphanie Daireaux Ernst & Young France
Dorica Dan Romanian National Alliance for Rare Diseases Romania
Hans-Peter Dauben DIMDI Germany
Ri De Ridder National Institute for Health and Disability Insurance Belgium
Emma Eatwell Genzyme Belgium
Hans-Georg Eichler European Medicines Agency (EMA) United Kingdom
Jennifer Farrugia Ministry of Health Care & the Elderly Pharmaceutical Policy & Monitoring, Directorate of Malta
Katia Finck Shire Pharmaceuticals, HGT France
Juan-Manuel Fontanet Universitat Autònoma de Barcelona Spain
Sylvain Forget Swedish Orphan - Biovitrum France
Marie-Christine Fortun Orphan Europe (Recordati group) France
Gatermann Ruediger CSL Behring Germany
Pamela Gavin National Organization for Rare Disorders (NORD) USA
Ruben Giorgino Helsinn Health Care Switzerland
Josie Godfrey National Specialised Commissioning Team, NHS United Kingdom
Alicia Granados Genzyme Spain
Lesley Greene COMP, EMA United Kingdom
Laura Gutierrez Celgene International Switzerland
Iñaki Gutiérrez Ibarluzea Basque Office for Health Technology Assessment Basque Country
Pertti Happonen Finnish Medicines Agency Finland
Adam Heathfield Pfizer United Kingdom
Thierry Heinrich Talecris Germany
Stéphanie Hoffmann Enobia Pharma Belgium
Birthe Holm COMP, EMA Denmark
Wills Hughes-Wilson Genzyme Belgium
Ulrike Jägle Novartis International AG Switzerland
Mohit Jain Talecris Germany
Ana Jerónimo INFARMED Portugual
Anna Korecka-Polak Agency for Health Technology Assessment in Poland Poland
Kateřina Kubáčková University Hospital Motol Czech Republic
Lucie Kutikova Amgen Europe Switzerland Yann Le Cam EURORDIS France Patrick Le Courtois European Medicines Agency (EMA) UK Lugdivine Le Dez Alexion Pharma Belgium Sprl Belgium Christine Leopold Austrian Health Institute Austria Kevin Loth Celgene International Switzerland Flaminia Macchia EURORDIS Belgium Georgios Margetidis The Public Health Executive Agency
Luxembourg Maria Mavris EURORDIS France Joan Mendivil Bayer Hispania, S.L. Spain Isabelle Mercier Millenium: The Takeda Oncology company
USA François Meyer Haute Autorité de Santé (HAS) France Fredrik Moen AstraZeneca Belgium Elena Molina Vázquez Swedish Orphan Biovitrum S.L. Spain
Antoni Montserrat European Commission/ DG Health and Consumers Luxembourg
Jean Mossman Mark Krueger & Associates, Inc. USA Hicham Naim Ernst & Young Switzerland Alan Newlands Clovis Oncology United Kingdom Gérard Nguyen Rett Syndrome Europe France Célia Oculi Ernst & Young France Francis Pang Shire Pharmaceuticals, HGT United
Kingdom Samantha Parker Orphan Europe (Recordati group) France Elisabeth Paternostre Sanofi-Aventis R&D France Fabien Peuvrelle Celgene International Switzerland Robert Pleticha EURORDIS France Massimo Radaelli ARIAD Pharmaceuticals, Inc. USA Pierrick Rollet GSK rare diseases United Kingdom Alric Ruether Institute for Quality and Efficiency in
Health Care Germany Peter Saltonstall National Organization for Rare Disorders
(NORD) USA Laura Sampietro Colom HTAi Spain Ad Schuurman Department of the Dutch Health Care
Insurance Board Netherlands Sylvie St-Laurent Pfizer France Jan-Maarten Ten Brundle Baxter World Trade Belgium Geraint Thomas GlaxoSmithKline United Kingdom Josep Torrent-Farnell COMP, EMA Spain Anders-Lamark Tysse European Commission- DG SANCO
Belgium Jutta Ulbrich Bayer Schering Pharma AG Germany Kerstin Westermark COMP, EMA Sweden Martine Zimmermann Alexion Europe France

2011 CAVOD StudyPage 11© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
Definitions of clinical added value: relative efficacy / relative effectiveness (1)
► Relative efficacy is the extent to which an intervention does more good than harm under ideal circumstances, compared to one or more alternative interventions
► Relative effectiveness can be defined as the extent to which an intervention does more good than harm compared to one or more intervention alternatives for achieving the desired results when provided under the usual circumstances of health care practice.
Efficacy… Relative efficacy Relative effectiveness
Time of positive opinion
of CHMP (T0)
T0 +T (3/5 years)
(1) Definitions aligned with : EUnetHTA JA WP5: REA of Pharmaceuticals, Draft Background review, April 2011High Level Pharmaceutical Forum, Core principles on relative effectiveness, Dec 2010
►In certain HTA practices, the terms « Clinical effectiveness » are also used►Within rare diseases and in particular ultra-rare diseases, comparators may particularly be complex to handle
2011 CAVOD StudyPage 12© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
►Avoid duplications at EU level
►Open, rigorous and transparent system
►Flexible system
►Quick operational implementation
►Build on an existing system/initiative
► Preferred option: EUnetHTA
► 2 additional options (hCMD- EMA or EUCERD-EAHC)
► Contribution of stakeholders in a real open and committed way
►A process and not a new structure
►Run pilots as early as 2012
Basic fundamentals Scope & mandate of CAVOD mechanism (1/2)
2011 CAVOD StudyPage 13© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
►CAVOD process associated with EUnetHTA current & future initiatives as the rare diseases arm, so called EUnetHTA-CAVOD.
►Central role shall be to:► Exchange valuable and trustable information on rare diseases and drugs► Develop and make available methodology and tools for scientific HTA assessment adapted for OD► Proceed to the EUnetHTA-CAVOD assessment according to necessary time-points► Organize continuous evidence collection for OD as post-marketing activities
►Secondary role shall be to:►Act as a “knowledge center” and collect all possible information on rare diseases and healthcare solutions► Contribute to developing a continuum between pre-market and post-marketing authorizations ►Be the first operational implementation phase of a process delivering at EU level relative effectiveness assessment dedicated to rare diseases
► A sub-group of EUnetHTA in charge of OD with a general function of linking with existing initiatives, projects, bodies & institutions for all matters relating to OD and dedicated HTA (EMA, national HTA bodies, EUCERD, MEDEV, PPRI, PHIS, HTAi, INATHTA, EURORDIS… )
Basic fundamentals Scope & mandate of CAVOD process (2/2)

2011 CAVOD StudyPage 14© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
The approach of the EUnetHTA-CAVOD process: « à la carte » system adapted for the various HTA bodies’ needs
Additional evidence generation
EUnetHTA-CAVOD analysis
Methodology / Toolkit dedicated to
orphan drugs
Information exchange
► the “information exchange” primary layer would support member states in giving them the opportunity to access the most complete information on the orphan drug, the targeted pathology, the epidemiology (associated with EUnetHTA JA WP6 and EMA (SAWP, CHMP, COMP))
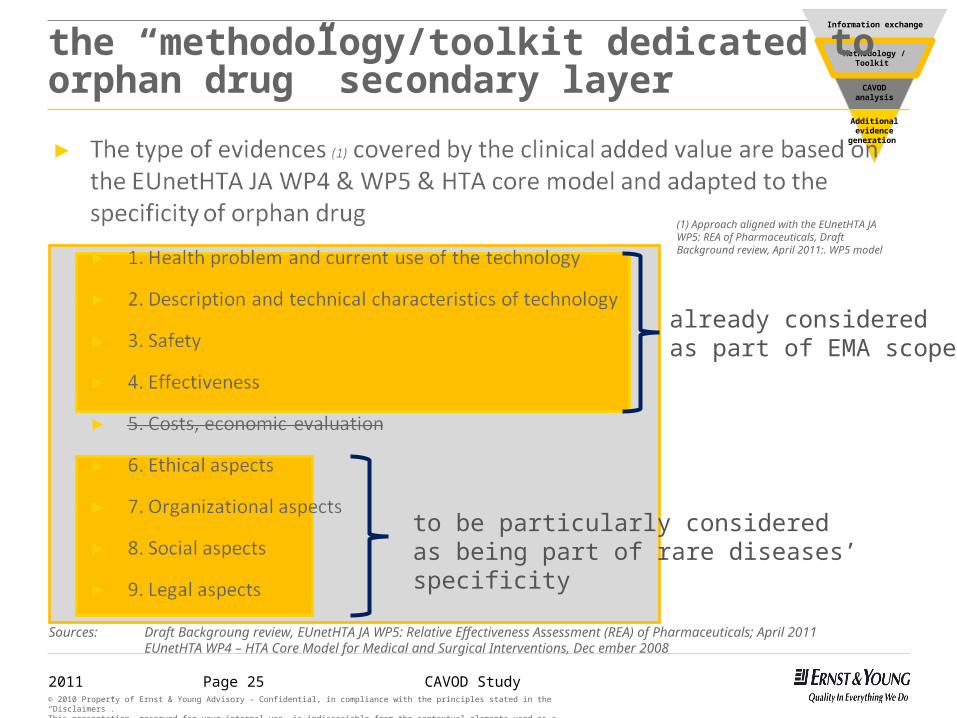
► the “methodology/toolkit dedicated to orphan drug” secondary layer would support member states in giving a methodological support specific to orphan drug in order to run their own assessment (associated with EUnetHTA JA WP4 )
► the “EUnetHTA-CAVOD analysis” layer would propose reports focused on relative effectiveness to MS which do not have the time and/or resource to run their own assessment and report (associated with EUnetHTA JA WP5)
► the “additional evidence generation” layer, would aim at proposing recommendations for post-marketing evidence generation addressing uncertainties based on National and European shared views (associated with EUnetHTA JA WP7 and EMA (CHMP))
► A four-layer approach was proposed following interviews with key stakeholders in order to better fit with the needs of the different national authorities involved in health technology assessment (HTA) processes:
2011 CAVOD StudyPage 15© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
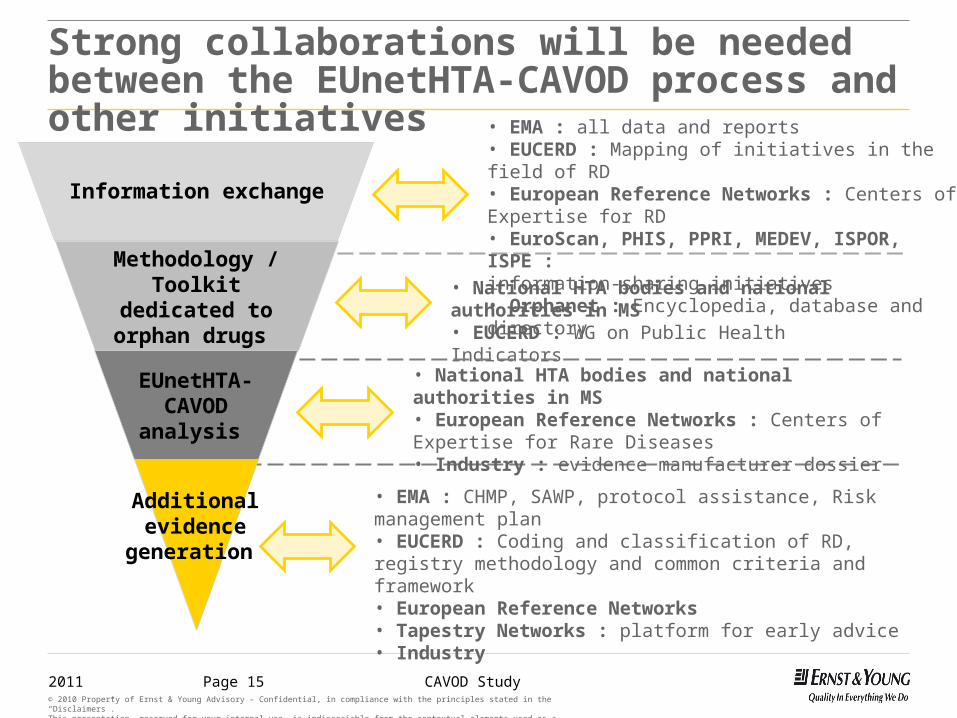
Strong collaborations will be needed between the EUnetHTA-CAVOD process and other initiatives
• National HTA bodies and national authorities in MS• EUCERD : WG on Public Health Indicators
• EMA : all data and reports• EUCERD : Mapping of initiatives in the field of RD• European Reference Networks : Centers of Expertise for RD• EuroScan, PHIS, PPRI, MEDEV, ISPOR, ISPE :information-sharing initiatives• Orphanet : Encyclopedia, database and directory
• National HTA bodies and national authorities in MS• European Reference Networks : Centers of Expertise for Rare Diseases• Industry : evidence manufacturer dossier
• EMA : CHMP, SAWP, protocol assistance, Risk management plan• EUCERD : Coding and classification of RD, registry methodology and common criteria and framework • European Reference Networks • Tapestry Networks : platform for early advice • Industry
Additional evidence
generation
EUnetHTA-CAVOD analysis
Methodology / Toolkit dedicated to
orphan drugs
Information exchange
2011 CAVOD StudyPage 16© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
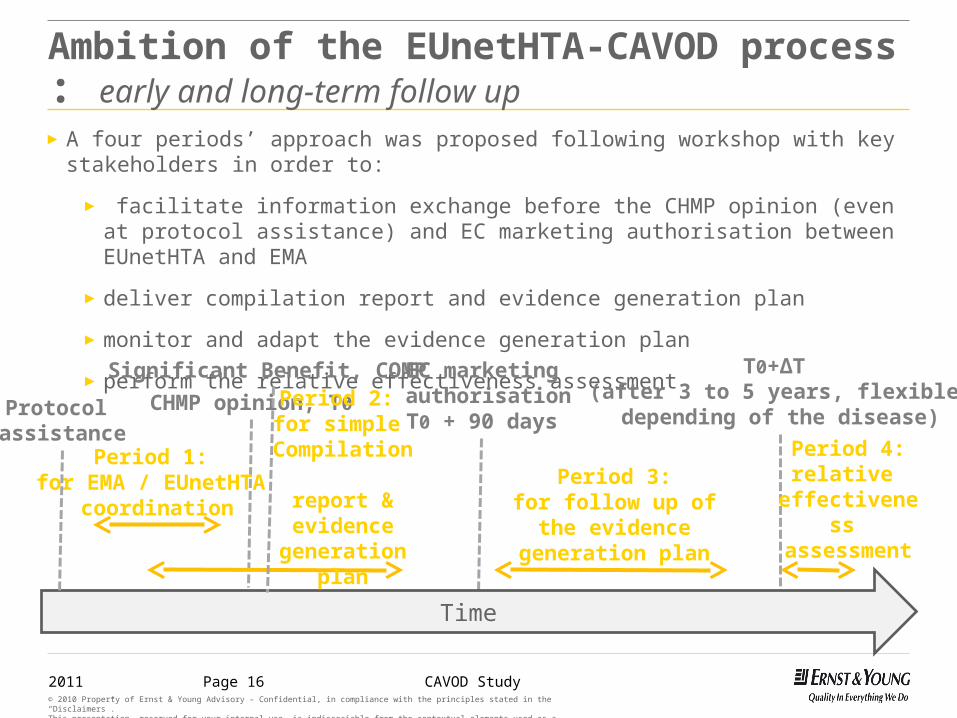
Ambition of the EUnetHTA-CAVOD process : early and long-term follow up
► A four periods’ approach was proposed following workshop with key stakeholders in order to:
► facilitate information exchange before the CHMP opinion (even at protocol assistance) and EC marketing authorisation between EUnetHTA and EMA
► deliver compilation report and evidence generation plan
► monitor and adapt the evidence generation plan
► perform the relative effectiveness assessment
Time
CHMP opinion, T0
EC marketing authorisationT0 + 90 days
T0+ΔT (after 3 to 5 years, flexible depending of the disease)
Period 1: for EMA / EUnetHTA
coordination
Period 2: for simple
Compilation report & evidence
generation plan
Period 3:for follow up of the
evidence generation plan
Period 4:relative
effectiveness assessment
Protocol assistance
Significant Benefit, COMP

2011 CAVOD StudyPage 17© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
Time
Principle of EUnetHTA-CAVOD process, early and long-term process along the life cycle of an orphan drug
2011 CAVOD StudyPage 18© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
Interaction process to bridge the gap between pre- & post-marketing practices
► One or more representative(s) of EUnetHTA-CAVOD as permanent participant to COMP and associated COMP working groups
► One or more representative(s) of EUnetHTA-CAVOD as non-permanent participant to SAWP, PDCO, CAT, CHMP (on an adhoc basis)
► One/two representative(s) of COMP as permanent participant to EUnetHTA-CAVOD work (EUnetHTA assembly when rare diseases are concerned)
► One representative of SAWP, PDCO, CAT, CHMP as non-permanent participant to EUnetHTA-CAVOD work (on an adhoc basis)
► One representative of rare diseases’ patient organisation (EURORDIS) as permanent participant to EUnetHTA-CAVOD work
► One representative of rare disease specific patient organisation as non-permanent participant to EUnetHTA-CAVOD work (on an adhoc basis)
► One representative of manufacturer as non-permanent participant to EUnetHTA-CAVOD work (on an adhoc basis)
2011 CAVOD StudyPage 19© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
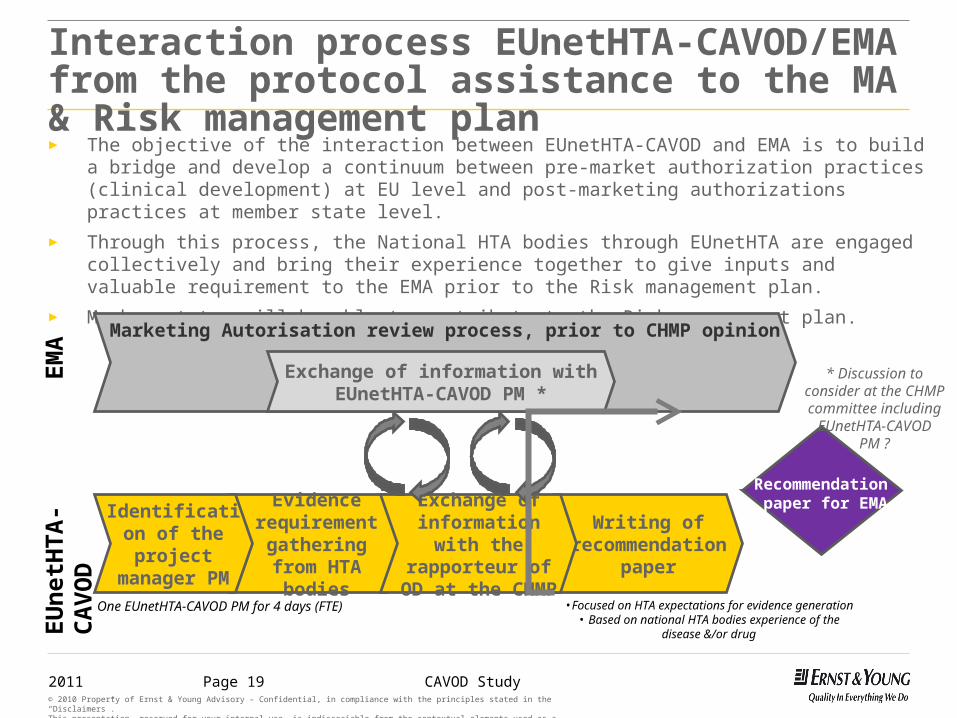
Interaction process EUnetHTA-CAVOD/EMA from the protocol assistance to the MA & Risk management plan► The objective of the interaction between EUnetHTA-CAVOD and EMA is to build a bridge and develop a
continuum between pre-market authorization practices (clinical development) at EU level and post-marketing authorizations practices at member state level.
► Through this process, the National HTA bodies through EUnetHTA are engaged collectively and bring their experience together to give inputs and valuable requirement to the EMA prior to the Risk management plan.
► Member states will be able to contribute to the Risk management plan.
Evidence requirement
gathering from HTA bodies
Writing of recommendation
paper
Identification of the project
manager PM
EUne
tHTA
-CAV
OD
Exchange of information with the rapporteur of OD at
the CHMP
Marketing Autorisation review process, prior to CHMP opinion
Exchange of information with EUnetHTA-CAVOD PM *
One EUnetHTA-CAVOD PM for 4 days (FTE)
EMA
•Focused on HTA expectations for evidence generation• Based on national HTA bodies experience of the disease
&/or drug
Recommendation paper for EMA
* Discussion to consider at the CHMP committee
including EUnetHTA-CAVOD PM ?

2011 CAVOD StudyPage 20© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
Compilation report at T0: Factual presentation of all available information in a meaningful way► The objective of the compilation report is to have a common format, which offers a factual
presentation of all available information in a meaningful way and to make the most of stakeholders’ knowledge.
► This will be useful :► To avoid duplication of work between HTA agencies► To support in their assessment MS which have not enough time/resources ► To increase transparency by providing a EU central report
► At T0 , CAVOD may focus on domains 1&2 and 6 to 9 when possible as there is often a limited amount of information for domains 3&4
Evidence requirement Organisation
• Manufacturer report (optional)• EMA data and documents developed under
the scope of OD analyses by the COMP, CHMP, CAT, PDCO
• Clinical trials’ dossier• Non EU information on the drug itself or on
available alternative therapies• Natural history of the disease• Clinical nature and impact of the diseases• Current management of the disease and
therapy limitations • Patient & clinical experts perspective • Compassionate use information, …
Compilation Report• Template elaborated
by the EUnetHTA-CAVOD scientific secretariat • Implementation of a pilot with an orphan drug to be selected• Keep flexibility
• Quality control role• Dissemination
EUnetHTA-CAVOD scientific secretariat• Gathering the data within CAVOD partners• Additional bibliography search• Report drafting and writing• 1 analyst (FTE) for 2 months
EUnetHTA-CAVOD assembly:• focused on quality control
Timing• 60-90 days, prior to MA from EC
Involvement of the MA holder
2011 CAVOD StudyPage 21© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
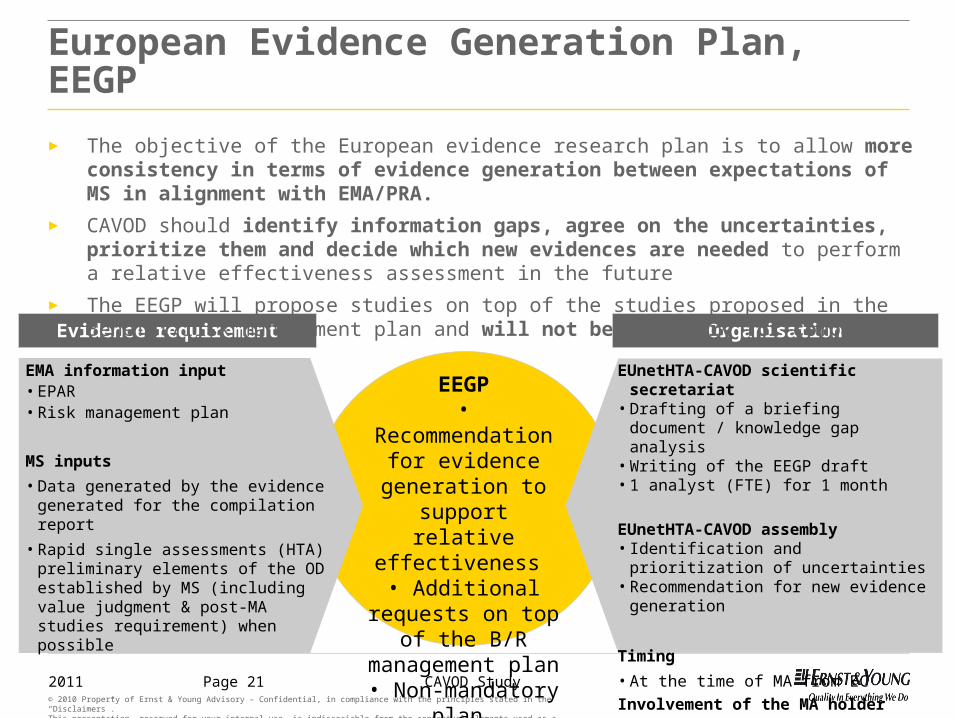
European Evidence Generation Plan, EEGP
Evidence requirement Organisation
EMA information input• EPAR• Risk management plan
MS inputs• Data generated by the evidence generated
for the compilation report• Rapid single assessments (HTA) preliminary
elements of the OD established by MS (including value judgment & post-MA studies requirement) when possible
EUnetHTA-CAVOD scientific secretariat• Drafting of a briefing document / knowledge
gap analysis• Writing of the EEGP draft• 1 analyst (FTE) for 1 month
EUnetHTA-CAVOD assembly• Identification and prioritization of uncertainties• Recommendation for new evidence generation
Timing• At the time of MA from ECInvolvement of the MA holder
EEGP• Recommendation for evidence generation to
support relative effectiveness
• Additional requests on top of the B/R management plan
• Non-mandatory plan
► The objective of the European evidence research plan is to allow more consistency in terms of evidence generation between expectations of MS in alignment with EMA/PRA.
► CAVOD should identify information gaps, agree on the uncertainties, prioritize them and decide which new evidences are needed to perform a relative effectiveness assessment in the future
► The EEGP will propose studies on top of the studies proposed in the Benefit/risk management plan and will not be mandatory for companies
2011 CAVOD StudyPage 22© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
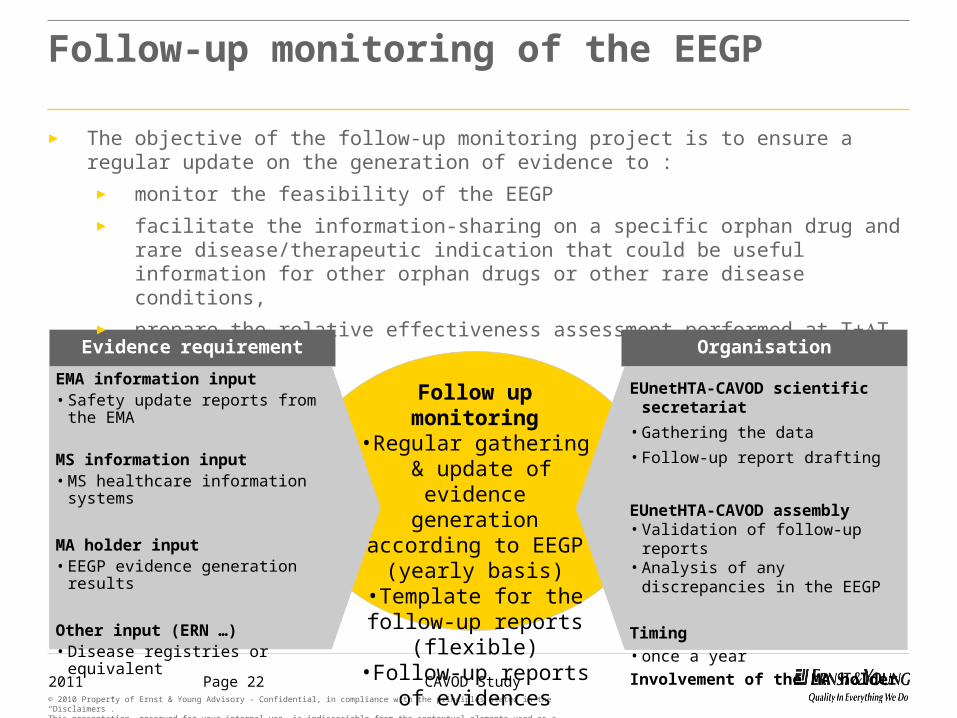
Follow-up monitoring of the EEGP
Evidence requirement Organisation
EMA information input• Safety update reports from the EMA
MS information input• MS healthcare information systems
MA holder input• EEGP evidence generation results
Other input (ERN …)• Disease registries or equivalent
EUnetHTA-CAVOD scientific secretariat• Gathering the data• Follow-up report drafting
EUnetHTA-CAVOD assembly• Validation of follow-up reports• Analysis of any discrepancies in the EEGP
Timing• once a yearInvolvement of the MA holder
Follow up monitoring•Regular gathering & update of evidence
generation according to EEGP (yearly basis)
•Template for the follow-up reports (flexible)
•Follow-up reports of evidences
► The objective of the follow-up monitoring project is to ensure a regular update on the generation of evidence to :
► monitor the feasibility of the EEGP► facilitate the information-sharing on a specific orphan drug and rare disease/therapeutic
indication that could be useful information for other orphan drugs or other rare disease conditions,
► prepare the relative effectiveness assessment performed at T+T
2011 CAVOD StudyPage 23© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
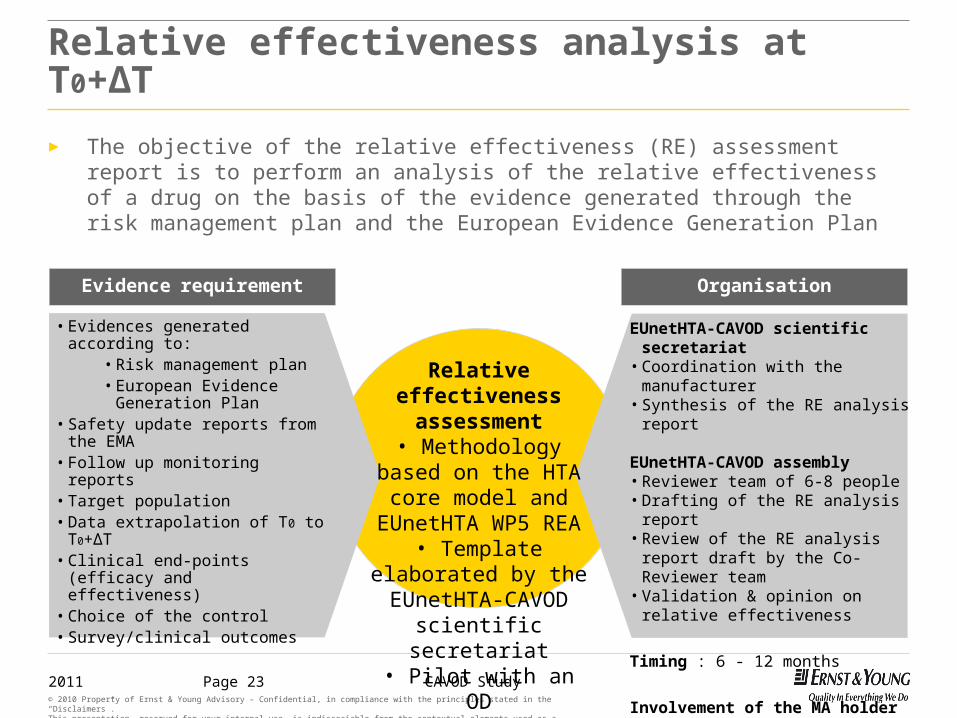
Relative effectiveness analysis at T0+ΔT
Evidence requirement Organisation
• Evidences generated according to:• Risk management plan• European Evidence Generation
Plan• Safety update reports from the EMA• Follow up monitoring reports• Target population• Data extrapolation of T0 to T0+ΔT• Clinical end-points (efficacy and
effectiveness)• Choice of the control• Survey/clinical outcomes
EUnetHTA-CAVOD scientific secretariat• Coordination with the manufacturer• Synthesis of the RE analysis report
EUnetHTA-CAVOD assembly• Reviewer team of 6-8 people• Drafting of the RE analysis report• Review of the RE analysis report draft by
the Co-Reviewer team• Validation & opinion on relative
effectiveness
Timing : 6 - 12 months
Involvement of the MA holder
Relative effectiveness assessment
• Methodology based on the HTA core model and
EUnetHTA WP5 REA• Template elaborated
by the EUnetHTA-CAVOD scientific secretariat• Pilot with an OD
► The objective of the relative effectiveness (RE) assessment report is to perform an analysis of the relative effectiveness of a drug on the basis of the evidence generated through the risk management plan and the European Evidence Generation Plan
2011 CAVOD StudyPage 24© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
Additional evidence
generation
CAVOD analysis
Methodology / Toolkit
Information exchange
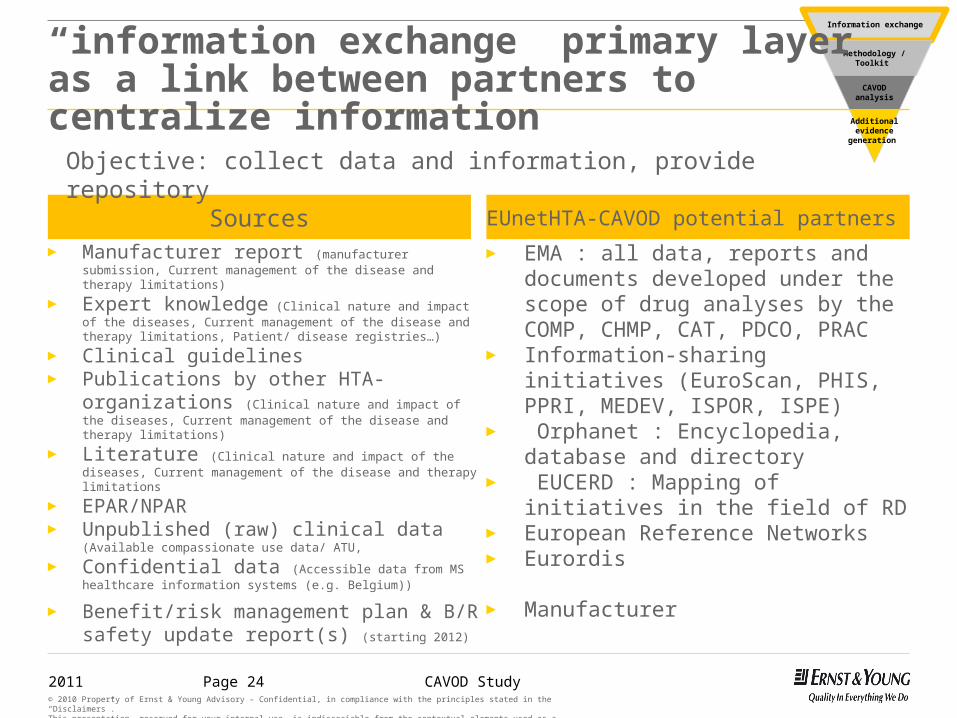
“information exchange” primary layer as a link between partners to centralize information
Sources► Manufacturer report (manufacturer submission, Current
management of the disease and therapy limitations)
► Expert knowledge (Clinical nature and impact of the diseases, Current management of the disease and therapy limitations, Patient/ disease registries…)
► Clinical guidelines► Publications by other HTA-organizations (Clinical
nature and impact of the diseases, Current management of the disease and therapy limitations)
► Literature (Clinical nature and impact of the diseases, Current management of the disease and therapy limitations
► EPAR/NPAR► Unpublished (raw) clinical data (Available
compassionate use data/ ATU,
► Confidential data (Accessible data from MS healthcare information systems (e.g. Belgium))
► Benefit/risk management plan & B/R safety update report(s) (starting 2012)
EUnetHTA-CAVOD potential partners ► EMA : all data, reports and documents
developed under the scope of drug analyses by the COMP, CHMP, CAT, PDCO, PRAC
► Information-sharing initiatives (EuroScan, PHIS, PPRI, MEDEV, ISPOR, ISPE)
► Orphanet : Encyclopedia, database and directory
► EUCERD : Mapping of initiatives in the field of RD
► European Reference Networks► Eurordis
► Manufacturer
Objective: collect data and information, provide repository
2011 CAVOD StudyPage 25© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
Additional evidence
generation
CAVOD analysis
Methodology / Toolkit
Information exchange
the “methodology/toolkit dedicated to orphan drug” secondary layer
Sources: Draft Backgroung review, EUnetHTA JA WP5: Relative Effectiveness Assessment (REA) of Pharmaceuticals; April 2011EUnetHTA WP4 – HTA Core Model for Medical and Surgical Interventions, Dec ember 2008
(1) Approach aligned with the EUnetHTA JA WP5: REA of Pharmaceuticals, Draft Background review, April 2011:. WP5 model
to be particularly considered as being part of rare diseases’ specificity
already considered as part of EMA scope
2011 CAVOD StudyPage 26© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
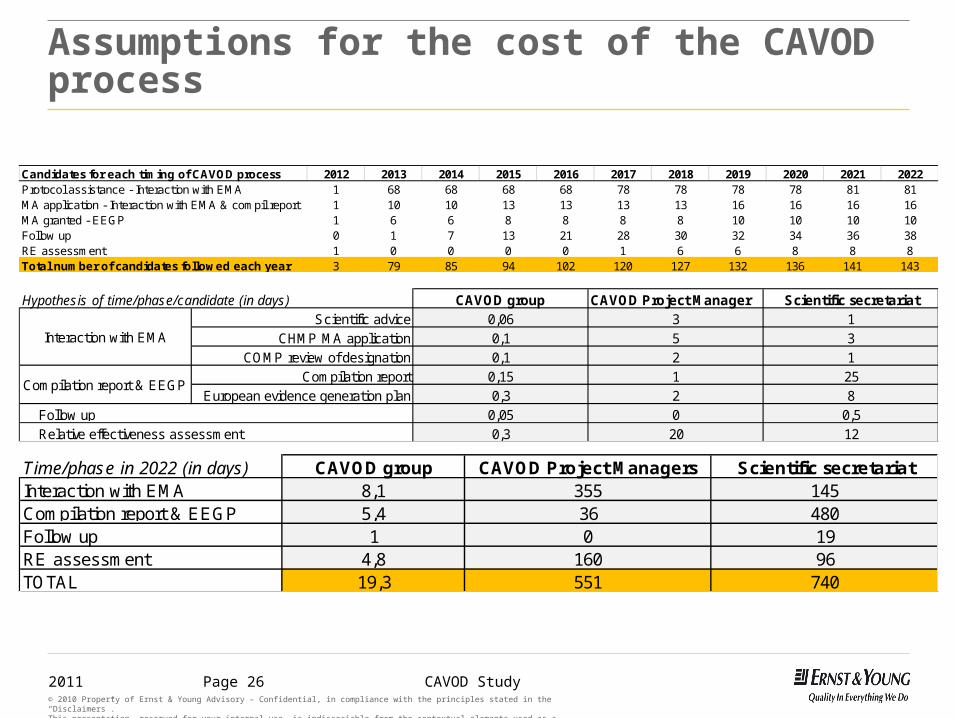
Assumptions for the cost of the CAVOD process
Candidates for each timing of CAVOD process 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022Protocol assistance - Interaction with EMA 1 68 68 68 68 78 78 78 78 81 81MA application - Interaction with EMA & compil report 1 10 10 13 13 13 13 16 16 16 16MA granted - EEGP 1 6 6 8 8 8 8 10 10 10 10Follow up 0 1 7 13 21 28 30 32 34 36 38RE assessment 1 0 0 0 0 1 6 6 8 8 8Total number of candidates followed each year 3 79 85 94 102 120 127 132 136 141 143
Hypothesis of time/phase/candidate (in days) CAVOD group CAVOD Project Manager Scientific secretariatScientific advice 0,06 3 1
CHMP MA application 0,1 5 3COMP review of designation 0,1 2 1
Compilation report 0,15 1 25European evidence generation plan 0,3 2 8
0,05 0 0,50,3 20 12
Interaction with EMA
Compilation report & EEGP
Relative effectiveness assessment Follow up
Time/phase in 2022 (in days) CAVOD group CAVOD Project Managers Scientific secretariatInteraction with EMA 8,1 355 145Compilation report & EEGP 5,4 36 480Follow up 1 0 19RE assessment 4,8 160 96TOTAL 19,3 551 740

2011 CAVOD StudyPage 27© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
Three scenarios & three different direct costs with the EUnetHTA option presenting the highest cost synergies
Direct costs borne by CAVOD for each scenario from 2012 to 2022
Distribution of direct costs borne by CAVOD for each scenario in 2022
Other ?
EU
netH
TA
EUCERD- EAHC
CMD - EMA
0 €
500 000 €
1 000 000 €
1 500 000 €
2 000 000 €
2 500 000 €
3 000 000 €
3 500 000 €
2012 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022
Scenario 1 - EUnetHTA Scenario 2 - CMDh like Scenario 3 - EAHC
196 837 € 380 119 €157 300 €800 998 €
921 998 €376 297 €
537 567 €
537 567 €800 000 €
800 000 €
268 783 €
459 579 €
352 066 €
0 €
500 000 €
1 000 000 €
1 500 000 €
2 000 000 €
2 500 000 €
3 000 000 €
3 500 000 €
Scenario 1 -EUnetHTA
Scenario 2 - CMDh like
Scenario 3 - EAHC hosting
Surveillance committee
Administrative functions
External experts for RE assessment
Scientific secretariat
Project Manager - interaction with EMA
Principal group meetings
Scenarios Scenario 1 Scenario 2 Scenario 3
Budget 2022 without synergies
2,9 m€ 3,3 m€ 3,1 m€
Budget 2022 with synergies
1 m€ 2,6 m€ 3 m€
2011 CAVOD StudyPage 28© 2010 Property of Ernst & Young Advisory – Confidential, in compliance with the principles stated in the “Disclaimers”. This presentation, reserved for your internal use, is indissociable from the contextual elements used as a basis for its elaboration and from the spoken comments accompanying it.
Four pilots to set up & run in 2012 requiring the support of key stakeholders (EUnetHTA, EMA, MAH…)► First Pilot to set up the process for the interaction and information exchange between EUnetHTA and EMA prior to
the CHMP opinion,
► Second Pilot to run the CAVOD compilation report based on an OMP under final review by the CHMP for the marketing authorisation,
► Third Pilot on the development of the European evidence generation plan with an OMP under reception of a positive opinion of the CHMP including the Risk management plan
► Fourth Pilot to perform a EUnetHTA-CAVOD relative effectiveness assessment with one orphan drug that is already on the market in certain countries and that is about to be reviewed by one member state
► As part of these 4 pilots,
► EUnetHTA-CAVOD shall have to delegate representatives at the SAWP, the CHMP, prepare the designation of project manager within its current member representative
► EMA shall have to open its committees and working groups and in particular the CHMP and the SAWP to EUnetHTA-CAVOD representatives and delegate COMP and CHMP representatives to EUnetHTA,
► Manufacturing holders shall support the CAVOD process through the selection of four OMPs designated product ready to enter the adhoc period of the CAVOD process,
► EUnetHTA shall have to set up the EUnetHTA scientific secretariat dedicated to CAVOD and further develop the information exchange center as well as adapt the methodological aspects;
► EMA shall have to open its data and internal reports related to selected molecule to EUnetHTA-CAVOD representatives
► EUCERD shall share with EUnetHTA-CAVOD all information on RD and registry set up
Contacts: Ernst & Young Advisory, Paris, France
Tour Ernst & YoungFaubourg de l'Arche92031 Paris-La Défense CedexFRANCE







![Welcome [] · 2018. 10. 1. · Dr Miriam Schmidts, Institute of Child Health 12:30 pm What can an Alliance of Patients and Professionals Achieve? Vicki Hedley, EUCERD & University](https://img.pdfslide.us/doc/110x75/612f04dc1ecc515869432d58/welcome-2018-10-1-dr-miriam-schmidts-institute-of-child-health-1230-pm.jpg)





















