Embed Size (px)
Citation preview

3/24/2018
1
Creating a NeuroNICU:
People, Practices, Possibilities
Kathi Salley-Randall, RN, MSN, CNS, NNP-BCNeuroNICU Program Consultant
• What is a NeuroNICU
• Why the NeuroNICU Trend
• How we created a NeuroNICU
2
Outline
Assessm
ent
Monitoring
Protection
Developm
ent
4 Pillars of Neuro-NICU Care

3/24/2018
2
How do we assess the brain?Pillar #1: Neuro-AssessmentTraining included detailed neonatal neuro exam, Sarnat, and Neonatal Pain, agitation,
and sedation Scale (N‐PASS)
Specialized ImagingMRI/MRS, Ultrasound, CT (for emergencies/trauma), F‐MRI, PETs
Pillar #2: Bedside neuromonitoring devices
Continuous videoEEG (cEEG)
Amplitude integratedEEG (aEEG)
Near infraredSpectroscopy (NIRS)
BRAIN FUNCTION BRAIN PERFUSION

3/24/2018
3
Pillar #3: Neuro-Protection• Initially the term (NP) applied to treatments and cares to prevent injury and cell death
• IVH Prevention• Therapeutic Hypothermia• Cocktails on Ice
Pillar #4 - Neuro-development
The 4 Pillars of Neuro-Conscious NICU
• Neuro-Assessment– Clinical /pain
assessment– Metabolic– MRI/MRS– Ultrasound– Follow up care
• Neuro-Monitoring– EEG– aEEG– NIRS– Hearing Screen– N-Trainer
• Neuro-Development– Environment – Sleep– Stress/Separation– Positioning– Support during
procedures
• Neuro-Protection– Cooling– Medications– Nutrition– IVH Bundles (Head
position, etc..)
POSSIBILITIES FOR ALL
12

3/24/2018
4
Where are you now?Where are you going?
• Neuro-NICU’s can be a:• QI project• Expanded Program• New unit design/environment• Change in culture
Why is there a NeuroNICU Trend?
• Recognition of improved survival with increased morbidities
• Taking advantage of our local expertise in fetal medicine, neonatal intensive care, neonatal neurology, pediatric neuroradiology, pediatric neurosurgery, and high‐risk infant follow‐up to focus on brain care
• Bringing new care practices and research findings to the bedside
• To improve the short and long term outcomes for infants and their families.
Neonatal Brain Injury• There are a number of causes and
diagnoses
• Outcomes depend on location, timing, extent of injury, interventions

3/24/2018
5
Perinatal-Neonatal Brain Injury
• The incidence of neurological
disabilities related to perinatal brain
injury has not decreased in decades• CP, Cognitive impairment, Epilepsy• Term and preterm infants are affected
Degos V et al. Anesth Analg2008;106:1670-1680
What we still don’t know• On the basis of our follow-up data we feel that the
size of the hemorrhage on ultrasound is by no
means the only guideline to outcome.
• There may well be other factors influencing the
result which we cannot yet diagnose by
ultrasound.
• M. I. Levene - Letter to the Editor, Lancet, 1981
Graphic Credit: Dr. Dieter Wolke, UK
IQ scores at 26 years (n=359)

3/24/2018
6
Graphic Credit: Dr. Dieter Wolke, UK
What we still don’t knowNeither structural brain alterations nor the
medical complications common in the NICU
population fully explain the variation in
long-term neurobehavioral development
Milgrom, 2010
Why is there a NeuroNICU Trend?• Recognition of improved survival with increased morbidities
• Taking advantage of our local expertise in fetal medicine, neonatal intensive care, neonatal neurology, pediatric neuroradiology, pediatric neurosurgery, and high‐risk infant follow‐up to focus on brain care
• Bringing new care practices and research findings to the bedside
• To improve the short and long term outcomes for infants and their families.
Neuro-NICU’s:Getting above the clavicles
• UCSF NeuroIntensive Care Nursery –2007• Phoenix Children’s NeuroNICU – 2009• Johns Hopkins• St. Louis Children’s• Vanderbilt Medical Center• Children’s National Medical Center,
Washington D.C.• Boston Children’s - Peds Neuro ICU
Glass, Bonifacio, Peloquin, Shimotake, et al. Neurocritical Care for Neonates. Neurocrit Care. 2010 June ; 12(3): 421–429. doi:10.1007/s12028-009-9324-7.
Photo credit – www.ucsf.edu
• Lucile Packard Children’s at Stanford• Loma Linda University Children’s
Hospital• Sharp Mary Birch & Rady’s
Children’s – San Diego• Riley Children’s – Indiana• CHOC – Orange, CA• And More…

3/24/2018
7
The Neuro-Conscious NICU Team
• Nursing• Identification of Risk• Triage patient,
staffing, equipment• Clinical Assessment• Apply equipment
• Neurology• Mechanism of injury• Coordinate application
and interpretation of EEG/aEEG
• Manage seizure
• Neonatology• Stabilize infant• Attention to
physiology and diagnosis
• Advanced Life Support
• Family & Follow Up• Prognosis• Long-term continuity• Support
The Neuro NICU is multi-disciplinary
Child Neurology
Developmental Behavioral Pediatrics/High Risk Infant follow‐up Clinic
DevelopmentalTeam
Pediatric Neurosurgery
Child Psychiatry
Neonatology
Neuroradiology
Why is there a NeuroNICU Trend?• Recognition of improved survival with increased morbidities
• Taking advantage of our local expertise in fetal medicine, neonatal intensive care, neonatal neurology, pediatric neuroradiology, pediatric neurosurgery, and high‐risk infant follow‐up to focus on brain care
• Bringing new care practices and research findings to the bedside
• To improve the short and long term outcomes for infants and their families.
HOW TO CREATE A NEURO-NICU?
28
Photo credit: @kyletdaddio - Twitter

3/24/2018
8
ONE UNIT’S JOURNEY
29
The LPCH Journey• 2012:
• Written proposal and budget submitted,
• Funding approved for equipment, training, and support staff
• Decision to make “virtual” unit within the unit
• Meetings with related departments to share vision
• Develop and trend “top 10” list
Who could BE Served
• Term Infants• HIE• Induced
Hypothermia• Seizures• Meningitis• Stroke• Cerebral Vascular
Malformations• ECMO• Metabolic Disease
• Preterm infants• Developmental
Care• Neuro-Protective
Interventions• Seizures• IVH, PVL
Who will BE served at LPCHTHE TOP 10 LISTS FOR LPCH
HIE/CoolingSeizures
ECMO/pre‐ECMOSevere 3‐4 IVH/hydrocephalus
Critical/unstablePremie ≤ 28 weeksCNS anomaliesMetabolic
Cyanotic CHDCNS infection

3/24/2018
9
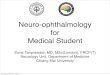
CRITERIA 1/14 1/24 1/28 2/5 2/12
HIE/Cooling 1 2 1 0 0SZS 2 1 1 0 1
ECMO/pre‐ECMO 2 1 0 0 1Severe 3‐4
IVH/hydrocephalus 0 0 0 0 0Critical/unstable 4 2 2 2 2Premie ≤ 28 weeks 1 1 2 0 2CNS anomalies 1 0 0 0 0
Metabolic 0 1 1 0 0Cyanotic CHD 1 2 1 3 1
CNS inf 0 0 0 0 0
_______ _______ _______ _______ _______Total NNICU 12 10 8 5 7
Total, Criteria 1‐5 9 6 4 2 4Total NICU census 34 37 31 23 26
NNICU/NICU 35.3% 27.0% 25.8% 21.7% 26.9% 34
Top 12 priority diagnoses for Neuro NICU
Priority Diagnosis Priority Diagnosis
1 HIE/cooling 7 Metabolic disease
2 Seizures 8CNS anomalies or Primary neurologic disorders
3 ECMO/pre‐ECMO 9 Cyanotic CHD4 Critical/unstable 10 CNS infection5 Preemie <29 weeks 11 Symptomatic PDA
6Grade III/IV or hydrocephalus
12 ALTE
The LPCH Journey• 2013:
• aEEG Nurse Training – application• aEEG MD Training – interpretation
• 3-Day NeuroNICU Training Courses, including hypothermia, NIRS and aEEG;
• Nurse Staffing Organized
• April - Opening of the NeuroNICU
• Start NeuroNICU Database

3/24/2018
10
The LPCH Journey• 2014
• Annual course continues
• Annual “skills” day for aEEG, NIRS, Cooling, Developmental Care
• Add additional NNP hours for bedside coverage
• Research:• CA Transport Cooling Trial – Servo vs Passive Cooling• Electrode Impedance QI project• Completed Optimized Cooling Trial• Late Hypothermia Enrollment
The LPCH Journey• 2015
• Annual course + skills day continue
• Add additional NNP hours for bedside coverage
• Add aEEG documentation to nurse charting
• aEEG Quiz for MD’s
• Summer Case Study Series (bedside)
The LPCH Journey• 2016
• Annual course + skills day continue
• Hire part-time NeuroNICU Nurse Educator
• Annual aEEG + NIRS Quiz for MD’s
• Research• HEAL (High-Dose Epo Trial)• Premature Infant Cooling Trial• Transfusion of Prematurity + NIRS
The LPCH Journey• 2017
• Annual course + skills day continue
• Annual aEEG + NIRS Quiz for MD’s
• Clinical Improvement Project = Seizures• Treatment Algorithm• Bedside Review of aEEG/Communication Audit

3/24/2018
11
The LPCH JourneyProgram Stats:• 1 year anniversary – 226 patients
• 2 year anniversary – 260 patients
• 3 year anniversary – 370 patients
• 4 year anniversary – 494 patients
• Total 1,350 infants
Clinical service• Specialized care by Neuro NICU trained RN team (n=90)
• Daily joint rounds with Neurology service
• On-site NNP or educator 5 days a week
• EPIC enhancements: Neuro NICU tab, dot phrases for neuro exam and aEEGinterpretation, order sets for hypothermia and seizures
• Neuro NICU database in REDCap for research, QA/QI, and program planning
Education• Annual didactic training (2-Day Course) –Open to the public – Next Sept 26-27, 2018
• Annual “skills day” for NeuroNICU nurses on aEEG, NIRS, cooling an developmental care
• Annual online review quiz for Medical Providers on aEEG, NIRS
• Weekly “5 Minute Friday Lectures”
Where are you now?Where are you going?
• Neuro-NICU’s can be a:• QI project• Expanded Program• New unit design/environment• Change in culture

3/24/2018
12
Neuro-NICU Pillars
• Neuro-Assessment– Clinical /pain
assessment– Metabolic– MRI/MRS– Ultrasound– Follow up care
• Neuro-Monitoring– EEG– aEEG– NIRS– Hearing Screen– N-Trainer
• Neuro-Development– Environment – Sleep– Stress/Separation– Positioning– Support during
procedures
• Neuro-Protection– Cooling– Medications– Nutrition– IVH Bundles (Head
position, etc..)
Framework of NICU Care
Practice Personnel
Research/QI Equipment
Final Thoughts• Brain injury is a reality of many infants in the NICU.
• The brain is the organ that has the greatest impact on long term quality of life and function.
• We have the opportunity to improve the quality of life of high-risk infants, and the quality of care provided through the expansion of new technologies, therapies, and practices.
• www.synapsecare.com• Free webinars on various NeuroNICU topics• Upcoming hypothermia training course• Monthly developmental care book club• Monthly aEEG Q&A call – review cases + hot
topics
• Annual NeuroNICU Nurse Training Course – Feb 2019 in San Diego, CA
48
Resources

THE CONFERENCE
February 3-5, 2019Neuro NICU Nurse Training
San Diego, CA
www.synapsecare.com#onenurse

register now at: www.synapsecare.com
Some featured topics:• Advanced NeuroExam
• HIE updates
• Trauma Informed Care
• Pain in the Brain
• Using aEEG
• Touch & Massage
• Caregiver Fatigue
• Music Therapy
The ONE Conference will focus on the four pillars of Neuro NICU nursing care:
Neuro-assessment, Neuro-monitoring, Neuro-development, and Neuro-protection
Download our FREE NeuroNICU Program & Practice QuickStartwww.quickstart.synapse.com
San Diego, CAKona Kai Resort & Spa
SPEAKERS INCLUDE:
Marsha Campbell-Yeo
Mary Coughlin
Lauren Heimall
Kathi Randall
Rachelle Sey
Jayne Solomon
Shannon Tinkler
Michelle Waddell
Kara Ann Waitzman
and more!

3/24/2018
13
• Innovative Care of the Newborn Brain
• Stanford University• 2 day Course• September 26-27, 2018• ONLINE REGISTRATION:
• tinyurl.com/neuronicu-sept
49
Resources

Innovative Care of the Newborn Brain
Our Invited Guest Faculty
September 26-27, 2018 Join us for a 2-day Neuro-NICU training course. In addition to our local experts in neonatology, neurology, developmental pediatrics and high-risk infant follow up care, we have several inter-national experts joining us to provide a range of break-out sessions for beginners and advanced users of therapeutic hypothermia, aEEG and NIRS. This is a conference not to be missed!
Lina Chalak MD, MS Epi Associate Professor in Pediatrics & Attending Neonatologist UT Southwestern Medical Center Dallas, TX - USA
Dr Lina Chalak’s clinical and translational research expertise is related to neonatal brain injury, HIE identification and therapies, as well as the use of NIRS to evaluate neurovascular unit and cerebral auto-regulation.
Lena Hellström-Westas MD, PhD Professor of Perinatal Medicine Senior Consulting Neonatologist Uppsala University Hospital Uppsala, Sweden
Dr. Lena Hellström-Westas is one of the pioneering clinical researchers on amplitude-integrated EEG monitoring with a focus on early prediction of outcome in asphyxiated infants and preterm infants, seizure detection, sleep and pain assessments.
Marianne Thoresen MD, PhD Professor of Neonatal Neuroscience, University of Bristol, UK & Professor of Physiology, University of Oslo, Norway
Dr. Marianne Thoresen is considered one of the world’s leading experts on both the basic science and clinical use of neonatal hypothermia and other neuroprotective strategies. She has been cooling neonates since 1998 and played an important role in implementing hypothermia throughout the UK.

Course Description This course has been designed to bring you an intense focus on one organ system, the neonatal brain and nervous system; the organ system that is ultimately responsible for our quality of life. We will take you on a journey from fetal life, through specialized care in the NICU, and finally beyond the doors of the NICU, to the infant’s real home.
Date & Time
September 26 & 27, 2018 0800 to 1700
Location Frances C. Arrillaga Alumni Center 326 Galvez Street—Stanford University Registration $400 until June 1st, 2018 $450 after June1st; $500 at the door Registration Fee Includes: Printed Sylla-
bus, Parking, Lunch and Light Snacks
Refund Policy 50% refunds will be given for cancellations re-
ceived in writing by August 30th, 2018 Agenda + Registration https://tinyurl.com/neuronicu-sept
Course Objectives 1. Identify risk factors, incidence and common
causes; describe the pathophysiology, di-agnostic work-up, two potential medical treatments, procedures, referrals; and list two nursing interventions or care considera-tions, for infants with the following condi-tions: • Hypoxic Ischemic Encephalopathy • CNS Malformations • Seizures • ELBW Infants
Full list of objectives and course schedule can be found online at: https://tinyurl.com/neuronicu-sept
Contact Information: Shannon Tinkler—NeuroNICU Educator Email: [email protected] Krisa Van Meurs—NeuroNICU Medical Director Email: [email protected]
0810: Why a NeuroNICU? - The LPCH story up until now— Kathi Salley Randall
0830: Fetal and neonatal brain development: Timing, significance, and out-comes—Courtney Wusthoff, MD, MS Epi
0915: Neurological Examination of the Newborn - Courtney Wusthoff, MD, MS Epi
1030: IVH and white matter injuries: Under-standing the pathophysiology, and risks for the small and big baby -Valerie Chock, MD, MS Epi
1115: HIE – Insult, impact, & interventions Krisa Van Meurs, MD
1145: Systemic Implications of Hypothermia Bedside Management Pearls Sonia L. Bonifacio, MD
1300: Mild HIE: Should we cool? Lina Chalak, MD, MS Epi
1330: The past and future of neonatal neuroprotection—Marianne Thoresen, MD, PhD
1430: Short-Term and Early Neurodevelopmen-tal Outcomes of Extremely Preterm Infants—Susan R. Hintz, MD MS Epi
1530: 5 Ways to Offer Neuro-Protective Care in the NICU—Kathi Salley Randall
1600: Psychological Support in the NICU to ef-fect short and long-term neonatal outcomes—Dr. Richard Shaw
0815: aEEG in Every Day Practice Lena Hellström-Westas , MD, PhD
0900: NIRS in the NICU—Now and the Future Directions—Lina Chalak, MD, MS Epi
0945: Diagnosis and management of neonatal seizures Courtney Wusthoff, MD, MS Epi
1130: Comfort Care vs Critical Care Diana Kobayashi, NNP
1300: BREAK-OUT SESSIONS— Beginner & Advanced aEEG/NIRS/Cooling Cases
1500: Looking back to look forward: The parent’s perspective of life in the NICU and beyond LPCH Family-Centered Care Department
1045: Pain and the preterm brain— Lena Hellström-Westas , MD, PhD
Wed, September 26 Thurs, September 27
Nursing CE Credits This course is pending approval for Nursing Continuing Edu-cation by California Board of Registered Nursing Provider Number CEP 15417 for 14 contact hours. No CME credits